
Abstract
Objective:
To examine the prevalence of psychological symptoms of the coronavirus disease 2019 outbreak among pregnant women and its association with gestational age and post-traumatic stress disorder symptoms.
Methods:
A cross-sectional study was conducted between June and November 2020 to assess the impact of the COVID-19 pandemic on mental health in pregnancy using the Impact of Event Scale-Revised. Pregnant women 18 years and older were recruited from antenatal and obstetrics clinics in Jordan. A total of 481 pregnant women participated in an online survey developed on Google Forms. A self-administered structured questionnaire was used to collect sociodemographic data, mental health information, and lifestyle changes. The Impact of Event Scale-Revised, the Perceived Support Scale, and the Mental Health Lifestyle Scale were administered. Variables related to sociodemographic information and dietary behavior and perception during the COVID-19 pandemic were also assessed.
Results:
The results showed that 58.6% of pregnant women reported the presence of post-traumatic stress disorder symptoms and women in the second trimester were more likely to show post-traumatic stress disorder symptoms compared with the first and third trimesters (p = 0.001). Moreover, a higher level of education, employment, poor dietary habits, and changes due to the pandemic were significantly associated with the Impact of Event Scale-Revised score and the presence of post-traumatic stress disorder symptoms.
Conclusion:
The COVID-19 pandemic was associated with high rates of psychological distress among pregnant women. Identifying mothers at risk of post-traumatic stress disorder symptoms may help improve maternity services and prevent adverse child outcomes.
Keywords
Introduction
Coronavirus disease (COVID-19) emerged by the end of 2019 as a highly infectious disease spreading exponentially worldwide. 1 This pandemic resulted in an unprecedented global public health threat and required hospitalization for a large number of moderate to severe cases. Hence, it inevitably overwhelmed health sectors in most countries worldwide. 2 By 1 June 2022, and over after 2 years of the virus’ emergence, there are 530 million confirmed cases and over 6.2 deaths worldwide. 3 In response to the pandemic, governments were obliged to initiate several immediate intervention measures that led to severe social and economic repercussions.
The Hashemite Kingdom of Jordan, a country in the Middle East region, initiated its first national response to COVID-19 on 27 February 2020, by prohibiting non-Jordanian passengers from high-risk countries to enter the country. As the number of reported cases increased; educational institutes, tourist sites, and restaurants were closed, and all public events were prohibited. Moreover, borders were closed and travel between governorates in Jordan was suspended. On 20 March, Jordan declared a state of emergency and initiated a nationwide lockdown. 4 Up to the 7 June 2022, a total of 1,697,271 cases and 14,068 deaths were reported in Jordan according to the World Health Organization (WHO). 3
The strict measures of home isolation, quarantine, social distancing, the uncertainty of the future, and overall movement restriction resulted in drastic modifications of the usual routine and impacted the mental health of the general population.5–7 The psychological impact and coping mechanisms for such outbreaks have been previously studied amid the severe acute respiratory syndrome (SARS) outbreak. A high rate of psychiatric and post-traumatic illnesses was reported 8 and the negative mental impact was primarily observed among females and those who were less educated. 9 Similarly, elevated levels of anxiety and depression were indicated during the COVID-19 pandemic, 10 and a moderate to severe negative impact on mental health was reported among the general population.11,12 In particular, women had higher post-traumatic stress symptoms and more prominent negative psychological impact during the COVID-19 pandemic. 13
Pregnancy is a period of physical, psychological, hormonal, and social changes, thus there is an increased risk of emotional distress and psychological issues during this stage of a woman’s life. 14 There is an increased level of concern regarding the mental health of pregnant women as they are more prone to having psychiatric disorders of which depression is the most common. 15 According to the WHO, 10% of pregnant women worldwide experience a mental disorder and the percentage is higher in developing countries with a prevalence of 15.6%. 16 Researchers propose that mental disorders prevalence may increase significantly during the COVID-19 pandemic as psychological distress increases in cases of stressful life events and disease outbreaks. 17
Given the mental and physical changes during pregnancy, pregnant women are more likely to be affected by the spread of the virus making them more vulnerable than the general population. 18 Several studies that investigated the psychological impact on pregnant women found a moderate to severe stressful influence in this vulnerable group.19,20 Moreover, it has been suggested that the COVID-19 pandemic had aggravated anxiety among pregnant women.21,22 Numerous factors increase the level of concern and anxiety among pregnant women in this unprecedented context. These include changes in their birth plans where intended family members may not be present to provide support during childbirth. Others include the anxiety of antenatal care follow up due to infection risk. 21 Furthermore, the increasing number of confirmed COVID-19 cases worldwide and information from media about the pandemic may further worsen stress and anxiety levels.
Studies have shown that gestational age may be related to the extent of risk perception and anxiety. However, contradicting data are available in the literature in that regard. Nonetheless, additional precautions must be rooted for when it comes to pregnant women owing to their weakened immune system and their susceptibility to prenatal anxiety, stress, and depression. 23 In addition to stress, malnutrition and physical inactivity could also influence immune and central nervous system (CNS) functions in the mother and her fetus, thus raising the risk for neurodevelopmental and mental disorders. 24
Limited research on the consequences of this pandemic among Arab pregnant women is available. Therefore, this study aimed to examine the prevalence of psychological symptoms of the COVID-19 outbreak among pregnant women in Jordan and investigate associations between gestational age and post-traumatic stress disorder (PTSD) symptoms amid the pandemic. The authors hypothesized that social and mental practices, lifestyle behaviors, and gestational age are associated with PTSD symptoms among pregnant women.
Methodology
Study design and participants
This cross-sectional research was conducted between June and November 2020 in Jordan to assess the impact of the COVID-19 pandemic on mental health. The inclusion criteria were pregnant women who were ⩾18 years and residing in Jordan. Participants were recruited from antenatal and obstetrics clinics. Pregnant women with a previous history of chronic diseases, preterm delivery, and abortion were excluded from this study.
The sample size was calculated using G*Power software (version 3.1.9.2) for the nonparametric one-way analysis of variance (ANOVA) with three groups. The calculation revealed the need for a sample size of 348 participants (a minimum of 116 participants in each trimester) to detect a medium effect size (0.25) with a significance level set at p < 0.05 and power as 0.99. A total of 481 pregnant women participated in the study.
The questionnaire was developed using Google Document Forms in both English and Arabic languages. Before launching the online survey, a pilot test was conducted on 30 pregnant women to ensure clarity and cultural appropriateness. Data from the pilot test were not included in the final analysis of the study. A uniform resource locator (URL) link was generated and disseminated among pregnant women from antenatal and obstetrics clinics in Jordan (a total of 20 clinics in the three main regions of the country: North, Central, and South). An information sheet about the study and its objective was offered on the first page of the online survey. Women who read the information and provide an electronic consent were able to proceed with answering and submitting the survey. Participants were allowed to exit the questionnaire at any point and data were collected anonymously. No incentives were provided for participation or for the completion of the survey. The study protocol was approved by the Hashemite University Institutional Review Board (16/11/2000951). An electronic informed consent was obtained from all participants.
Data collection
A self-administered structured questionnaire was used to collect sociodemographic data, mental health information, and lifestyle changes. Sociodemographic data included age, the governorate of residence, educational level, employment status, work/study from home, pregnancy trimester, and self-reported weight and height. The psychological impact of COVID-19 was assessed using the Impact of Event Scale-Revised (IES-R), 25 the social and family support impact was evaluated using questions from the Perceived Support Scale (PSS), 9 lifestyle changes were assessed using the Mental Health Lifestyle Scale (MHLSS). 9 The full questionnaire is provided as a supplementary file.
IES-R Scoring
The IES-R is a 22-item questionnaire 25 that has been used recently to measure mental health symptoms experienced by the general population during the COVID-19 pandemic.26–28 Participants were asked to rate the items based on how distressing they were for them concerning the COVID-19 pandemic in the past 7 days. The response options for each question were scored based on a 5-point Likert-type scale, 0 = not at all and 4 = extremely. A total score was then generated ranging from 0 to 88. The total IES-R score was considered normal (IES-R ⩽ 22); or indicative of PTSD (IES-R > 22). Three subscale scores were also calculated measuring intrusion (8 items), avoidance (8 items), and hyperarousal (6 items).
Indicators of negative mental health impact
This section included six validated questions about negative mental health effects caused by the COVID-19 pandemic. 9 Participants were asked if they felt horrified, apprehensive, or helpless due to COVID-19 the pandemic. Participants were also asked if they were experiencing increased stress from work, financial status, and staying at home during the current pandemic. The response options were much decreased, decreased, same as before, increased, and much increased. For the purpose of the study analysis, the responses from each question were transformed into a dichotomous response and classified into either changed or unchanged.
Social and family support
This part contained questions from the PSS assessing the influence of the COVID-19 pandemic on the support received from family or friends in the past month. 9 It contained five questions: support from family members, support from friends, sharing feelings with a family member, sharing feelings when in blue, and caring for family members’ feelings. The response options were much decreased, decreased, same as before, increased, and much increased. For the purpose of the study analysis, the responses from each question were transformed into a dichotomous response and classified into either changed or unchanged.
Mental health-related lifestyle changes
Questions from the MHLSS 9 were included to rate the frequency of mental health-related lifestyle changes that might have disturbed participants during the COVID-19 pandemic. This section included four items; attention to mental health, spending enough time to rest, relax, and exercise. The response options were much increased, increased, same as before, decreased, and much decreased. For the purpose of the study analysis, the responses from each question were transformed into a dichotomous response and classified into either changed or unchanged.
Dietary behavior and perception
This section included a total of 13 items regarding dietary behavior and perception during the COVID-19 pandemic. Questions were adapted from previously published research on dietary habits during the COVID-19 pandemic.29,30 First item inquired whether participants were consuming any type of supplement as an immune-boosting method. Items 2–6 inquired about the nature of most meals consumed during the pandemic (homemade, frozen food, fast food, restaurants, healthy food). The last seven items inquired about what the participants perceived as an immune-boosting method such as eating a balanced diet, taking supplements, engaging in physical activity, drinking adequate fluids, consuming herbs or spices, proper sleep, and stress management.
Statistical analysis
Statistical analysis was carried out using SPSS version 26.0 (IBM, Chicago, IL, USA). Normality of data was tested using Kolmogorov–Smirnov test. All data were presented with the use of frequency and percentages for the categorical variables and median and interquartile range (IQR) for the continuous variables. Comparisons were performed using the chi-square test (χ2) for categorical variables and the Kruskal–Wallis H test for continuous variables. All statistical tests were carried out using two-sided tests. Two multivariate regression tests were carried out to assess the effect of possible confounding factors on the presence of PTSD symptoms and the total IES-R score. The first was a generalized linear model based on a Poisson distribution and considered the IES-R score as a continuous variable. The second was a logistic regression and used a binary coding of the IES-R score into 0 for lack of PTSD symptoms (IES-R score of less than or equal to 22) and 1 for the presence of PTSD symptoms (IES-R score greater than 22). The variables included in the final multivariate regression tests were selected with the use of a univariate general linear model, with the use of a cut-off value of p < 0.20 to be included. Statistical significance was obtained with a p value
Results
Table 1 shows the sociodemographic characteristics of the 481 pregnant women who participated in this study. Overall, the majority of participants were in the age group 26–35 years (59.3%), living in the central region of the country (67.8%), in their third trimester into pregnancy (39.1%), overweight (43.0%), well-educated (64.5%, bachelor’s degree or higher), unemployed (55.3%), sleep deprived (53.8%), and did not work from home (75.1%).
Sociodemographic characteristics of pregnant women participants (n = 481).

As part of the study hypotheses, Table 2 shows an expected association between the presence of PTSD symptoms and gestational age, sociodemographic, lifestyle, and mental variables. Overall, 58.6% of pregnant women reported the presence of PTSD symptoms with the least prevalence during the first trimester (p = 0.001). In general, participants with PTSD symptoms were more likely to have higher level of education (p = 0.008), were employed (p = 0.040), changed seeking support from friends (p = 0.003), changed seeking support from family (p < 0.001), changed sharing feelings with family (p < 0.001), changed sharing feelings with others (p < 0.001), changed caring for family feelings (p < 0.001), changed attention to mental health (p < 0.001), changed time spent to rest (p = 0.006), changed time spent to relax (p = 0.004), changed time spent to exercise (p = 0.002), changed stress from work (p < 0.001), changed financial stress (p = 0.021), changed home stress (p < 0.001), changed horrified feelings from pandemic (p < 0.001), changed apprehensive feeling (p < 0.001), and changed feeling helpless (p < 0.001) in comparison with participants who did not show changes in these practices. In contrast, the presence of PTSD symptoms was not significantly associated with age geographic location, body mass index (BMI), working from home, proper sleep, practicing physical activity, managing stress, eating homemade food, eating frozen food, eating fast food, eating in restaurants, eating healthy food, consuming immune boosters, balanced diet, consuming supplements, drinking water adequately, and using herbs (p > 0.05).
Association of sociodemographic, lifestyle, and dietary variables with the presence of posttraumatic stress disorder symptoms among pregnant women (n = 481).

PTSD: post-traumatic stress disorder; IES-R: Impact of Event Scale-Revised.
As presented in Table 3, the number of pregnant women that showed the presence of PTSD symptoms (IES-R score > 22) was 75 out of 149 (50.3%), 102 out of 144 (70.8%), and 105 out of 188 (55.9%) in the first, second, and third trimesters, respectively (χ2(2) = 13.666; p = 0.001). A Kruskal–Wallis H analysis showed significant differences in IES-R score between the three trimesters of pregnancy (χ2(2) = 15.649; p < 0.001), with a mean rank in IES-R score of 215.37 for the first trimester, 277.61 for the second trimester, and 233.27 for the third trimester. Also, significant differences were detected in intrusion scores between the three trimesters of pregnancy (χ2(2) = 9.928; p = 0.007), with a mean rank intrusion score of 218.18 for the first trimester, 268.83 for the second trimester, and 237.77 for the third trimester. Furthermore, significant differences in avoidance scores were observed among the three trimesters of pregnancy (χ2(2) = 8.096; p = 0.017), with a mean rank avoidance score of 221.30 for the first trimester, 266.68 for the second trimester, and 236.94 for the third trimester. The hyperarousal score was significantly different among the three trimesters of pregnancy (χ2(2) = 14.463; p = 0.001), with a mean rank hyperarousal score of 222.55 for the first trimester, 277.64 for the second trimester, and 227.56 for the third trimester.
Effect and association of pregnancy trimester with the presence of post-traumatic stress disorder and IES-R score during COVID-19 pandemic in Jordan (n = 481).

IES-R: Impact of Event Scale-Revised; χ2: chi-square; IQR: interquartile range.
p Value based on chi-square test.
p Value based on Kruskal–Wallis H test.
Values with different superscript letters are significantly different, based on pairwise comparisons with Bonferroni adjustment (p < 0.05).
Table 4 shows the association of social and demographic confounding factors with the presence of PTSD symptoms. The multivariate regression tests revealed that changes due to the pandemic in sharing feelings with family members, sharing feelings with others, caring about family, spending enough time on mental health, feeling work stress, feeling financial stress, feeling stress from staying at home, feeling apprehensive, and feeling helpless, in addition to the stress regarding education level and trimester into pregnancy were significantly associated with IES-R score and presence of PTSD symptoms.
Association of social and demographic confounding variables with the IES-R score and the presence of PTSD symptoms among pregnant women during the COVID-19 pandemic (n = 481).

IES-R: Impact of Event Scale-Revised; CI: confidence interval.
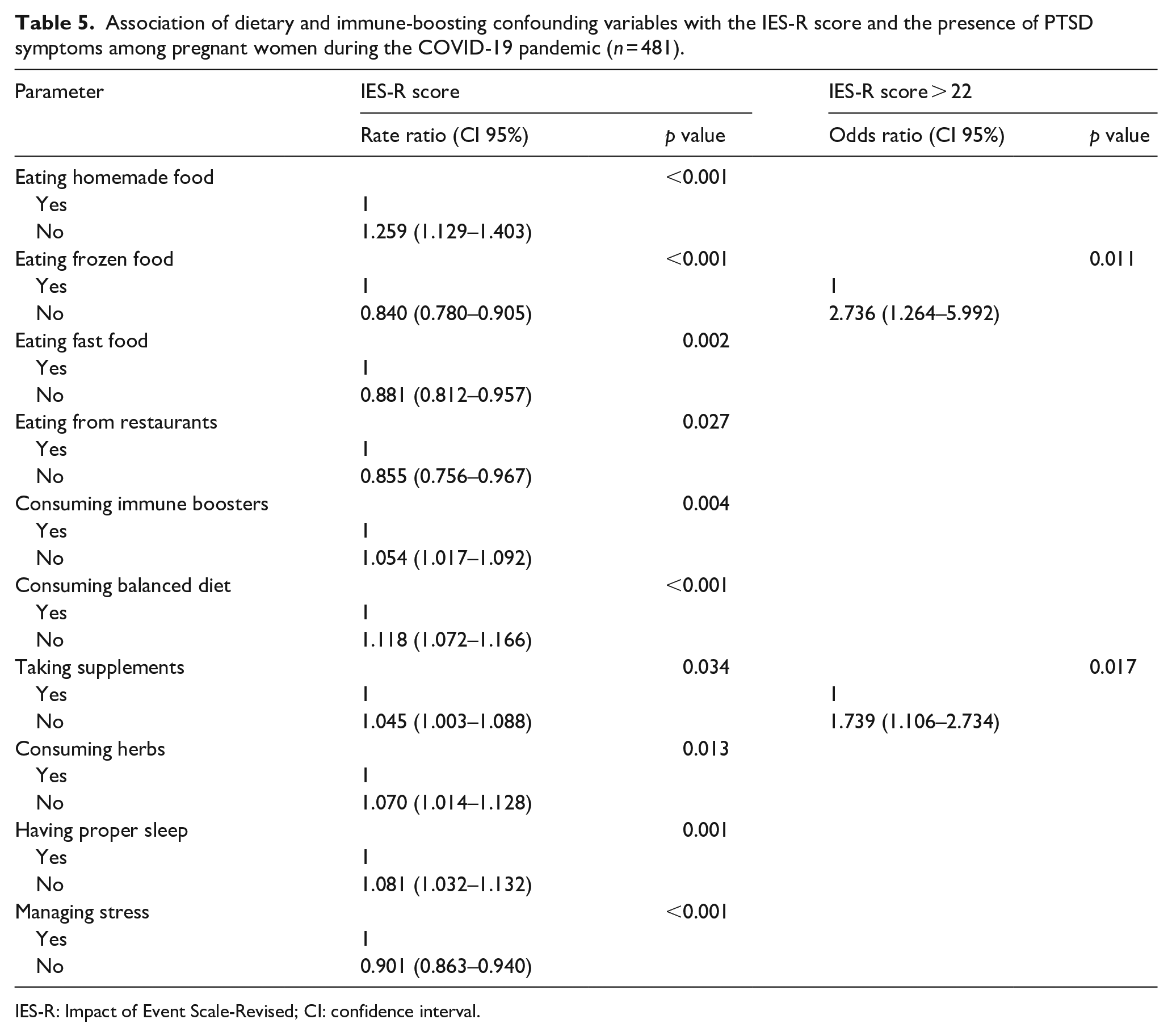
Table 5 shows the assessment of the effect of possible dietary and immune-boosting confounding factors on the presence of PTSD symptoms. The multivariate regression tests revealed that participants who reported no homemade food consumption (p < 0.001), frozen food consumption (p < 0.001), fast food consumption (p = 0.002), and restaurants dining (p = 0.027) were likely to report higher IES-R scores and presence of PTSD symptoms. Also, participants who reported no consumption of immune boosters (5.4%) were more likely to show PTSD symptoms (p = 0.004). Furthermore, participants who did not perceive a relationship between balanced diet (p < 0.001), supplements (p = 0.034), herbs (p = 0.013), and proper sleep (p = 0.001), with immunity, were associated with higher IES-R score and/or presence of PTSD symptoms. In contrast, participants who did perceive a relationship between stress management (p < 0.001) and immunity were associated with higher IES-R score and/or presence of PTSD symptoms.
Association of dietary and immune-boosting confounding variables with the IES-R score and the presence of PTSD symptoms among pregnant women during the COVID-19 pandemic (n = 481).
IES-R: Impact of Event Scale-Revised; CI: confidence interval.
Discussion
To the best of our knowledge, this is the first study to examine the prevalence of psychological symptoms related to the COVID-19 outbreak among pregnant women in Jordan and to investigate the associations between gestational age and PTSD symptoms during the pandemic. Interestingly, this study showed that pregnant women in the second trimester of pregnancy were more likely to show PTSD symptoms when compared with the first and third trimesters and that changes due to the pandemic were significantly associated with the IES-R score and the presence of PTSD symptoms.
In this study, more than one-half of the pregnant women reported the presence of PTSD symptoms (IES-R score > 22) during the COVID-19 pandemic. Similarly, a study by Davenport et al. 31 in Canada showed that 40.7% of pregnant women presented high depression scores during the pandemic, and moderate to high anxiety was identified among 72% of the participants. Likewise, a survey among 5866 pregnant and breastfeeding women in Belgium indicated that almost half of them experienced depressive or anxious symptoms during the lockdown period of the COVID-19 pandemic. 32 Another study in Ireland showed that over half of evaluated pregnant women were more concerned about their own health and the health of their unborn babies after the onset of the pandemic compared with before the pandemic. 33 A systematic review investigating the impact of the COVID-19 pandemic on the mental health of pregnant women revealed that social distancing, fear of infection, current economic situation, media pressure, disrupted routines, and the change in family rituals were intensifying factors of psychological distress among pregnant women. 34 The presence of PTSD symptoms among pregnant women was shown to have acute (e.g. preterm delivery) and long-term consequences (e.g. cognitive delays for the offspring) on the psychological and physical health of both mother and baby. 35 Therefore, pregnant women during infectious disease outbreaks could benefit from reliable information and guidance; appropriate support from healthcare professionals; and virtual support groups. 36
Another finding of this study was that pregnant women in the second trimester of pregnancy had a significantly higher IES-R mean score compared with those in their first and third trimesters. Likewise, a study on Chinese pregnant women during the COVID-19 pandemic found that women in their second trimester of pregnancy had the highest IES score. 20 However, a study conducted among women with singleton pregnancies in Italy, suggested that women in their first trimester showed more anxiety compared with those in the second and last trimesters. 19 Other studies from Brazil and Iran indicated a higher negative psychological impact due to the pandemic during the third trimester of pregnancy.14,37 Adrenocortical hormone secretion increases during pregnancy, which makes pregnant women more prone to anxiety and other adverse emotions. 38 Moreover, Silva et al. 14 suggested that mental stress in the second and third trimesters may be due to increased physical discomfort, fear of delivery proximity, and concern for the fetus’ health.
This study showed a higher risk of PTSD symptoms in pregnancy among employed pregnant women and those with higher education level. Likewise, the findings of a Pakistani study suggest that pregnant women working outside the household were more anxious and depressed compared with those who were unemployed. 39 The relationship between education level and PTSD due to the COVID-19 pandemic was conflicting in the literature. Some studies suggested that higher levels of education might prepare individuals with better coping strategies when dealing with environmental disasters.40,41 Others implied that highly educated individuals were more stressed as a result of higher self-awareness and a better understanding of the pandemic severity. 42 A study among pregnant women in Turkey, revealed that the presence of COVID-19-related symptoms and educational level were found to predict PTSD symptoms. 43
The findings of this study suggest that the presence of PTSD symptoms was not associated with engagement in physical activity. However, physical activity is recommended as a therapy against the mental and physical consequences of quarantine during the outbreak. 44 Moreover, pregnant women involved in at least 150 min of moderate-intensity physical activity each week during the pandemic had lower scores for both anxiety and depression. 31 Thus, organizing awareness sessions about home exercises and their potential benefits on the mental health are essential. 45
Another important finding of this study demonstrates that the change per se in the perceived family support, along with lifestyle changes, and the negative feelings due to the pandemic were associated with a higher risk of PTSD symptoms. Pregnant women are already going through numerous physical, hormonal, and psychological changes, adding to the experience of a continuous pandemic situation, and the changes in vital support during this period can add to the uncertainty about the future and further exacerbate stress, anxiety, and compromise well-being.46,47
This study shows that better dietary behaviors were negatively correlated with PTSD symptoms. This finding further highlights the perceived benefits of healthy eating habits on the well-being of the mother and her fetus. A study indicated that higher healthy eating index scores were associated with reduced symptoms of anxiety, depression, and stress. 48 Similarly, a study among pregnant women concluded that higher depression scores were associated with lower nutrient indices (potassium, calcium, and iron levels) and lower exercise levels. 49 Moreover, depression and anxiety during pregnancy was negatively associated with healthy behaviors such as taking vitamins and practicing physical activity. 50 Therefore, it is essential to identify psychological risk factors among pregnant women and provide the necessary support. It is essential to develop prevention strategies aimed to promote healthy behaviors in pregnant women.
This study has several strengths, including the sample size and the use of the Impact of Events Scale-Revised (IES-R) questionnaires which facilitates comparing the findings with other studies. Moreover, the use of an online survey permitted data collection from different parts of the country and ensured the anonymity of the participants. However, this study has some limitations. The cross-sectional design of the study does not allow the causal analysis of the psychological impact. Moreover, the self-reporting of the levels of psychological impact among pregnant women. Finally, there was no assessment of the history of mental health or anxiety disorders pre-COVID-19 or the use of psychotherapies among participants.
Conclusion
The findings of this study indicated high rates of psychological distress and PTSD symptoms among pregnant women during the COVID-19 pandemic. This highlights the need for professional mental health support for this vulnerable group. Early detection of psychological distress is fundamental to prevent negative outcomes for women and their fetuses.
Supplemental Material
sj-docx-1-whe-10.1177_17455057221112935 – Supplemental material for Impact of coronavirus 2019 pandemic on post-traumatic stress disorder symptoms among pregnant women in Jordan
Supplemental material, sj-docx-1-whe-10.1177_17455057221112935 for Impact of coronavirus 2019 pandemic on post-traumatic stress disorder symptoms among pregnant women in Jordan by Mo’ath F Bataineh, Maysm N Mohamad, Ayesha S Al Dhaheri, Monketh Rawashdeh, Ali M Al-Nawaiseh, Fida F Asali, Mona Hashim, Amjad Jarrar, Dima O Abu Jamous, Lily Stojanovska, Rameez Al Daour, Sheima T Saleh, Tareq M Osaili and Leila Cheikh Ismail in Women’s Health
Footnotes
Acknowledgements
The authors acknowledge pregnant women for their time and participation and all who contributed to the completion of this study.
Author contribution(s)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
The datasets used and analyzed during this study are available as supplementary material.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.