
Abstract
Background:
The COVID-19 pandemic caused significant socioeconomic and healthcare disruptions in Canada. COVID-19 healthcare policies and local infection rates varied considerably across Canada’s geographically diverse, multijurisdictional healthcare system. Emergence of highly transmissible COVID-19 variants and widespread COVID-19 vaccination mandates in Fall 2021 further impacted life in Canada. The experiences of pregnant people, in particular, were challenged by COVID-19 outbreaks, Canadian hospital policies, and local public health restrictions.
Objective:
This study explored experiences of Canadian perinatal care in the context of the COVID-19 pandemic.
Design:
Online, cross-sectional survey with qualitative analysis.
Methods:
Individuals pregnant after January 1, 2020 who received perinatal care in Canada participated in our Pandemic Pregnancy Experiences eSurvey, September 1, 2021 to February 1, 2022. Open-ended survey responses were qualitatively evaluated by thematic and content analysis. Codes were identified both deductively and inductively, categorized using principles of woman-centered care, and developed into major and minor themes.
Results:
Prenatal care and COVID-19 vaccination experiences were evaluated from 362 participants, with 234 participants also elaborating on their labor and delivery (L&D) care. Major themes organized by woman-centered care category as follows: Choice of Healthcare Provider (good quality healthcare provider, barriers to provider of choice), Autonomy-Healthcare (autonomy empowered, autonomy impacted), Choice of Delivery Place (wanted hospital birth, got hospital birth), Choice of Support Companion(s) (no support companion for prenatal appointments, hospital restrictions L&D support companion(s)), and, Autonomy-COVID-19 Vaccination (vaccinated while pregnant/breastfeeding).
Conclusions:
Pregnancy and birth experiences were generally positive; however, both COVID-19 and existing constraints of provincial/territorial healthcare systems impacted Canadian perinatal experiences. Limited choice of healthcare provider type and access to prenatal and L&D support companion(s) affected perinatal care satisfaction.
Plain language summary
Given the widespread impact of the pandemic on Canadian society, this study explored women’s experiences of Canadian perinatal healthcare. Study participants identified both regional health care system limitations together with COVID-19 hospital policies as adversely impacted their pregnancy experiences.
Introduction
Pregnancy experiences are shaped by socioeconomic status (SES) factors, parity, reproductive and general health history, and healthcare providers.1,2 Although many pregnancies are unplanned, for those individuals who plan pregnancy and birth, their self-determination often informs future healthcare decision-making, and ultimately, parenting choices. Retrospective attitudes about birth experience are greatly influenced by perceptions of control and empowerment in the context of reproductive healthcare decision-making. 1 Woman-centered care models promote shared decision-making to empower patients and foster autonomy through informed choice, continuity of care, and effective provider communication skills.1,3,4 Autonomy in childbirth is further represented by individual choices in the medical and/or non-medical management of pain, such as changes in body position and breathing techniques,1,5 birth companion(s) of choice,6 –9 and delivery location of choice.5,10
In 2020, the emergence of COVID-19 as a global pandemic significantly reduced in-person access to reproductive healthcare services in many countries.11 –13 Canada’s sociopolitical response to the pandemic included travel restrictions, mandatory geographical quarantines, curfews, closures of schools, universities, and most “non-essential” businesses.14,15 Early in the pandemic, pregnancy risks of COVID-19 were not well understood, despite infectious respiratory pathogens, including SARS-CoV-1 and influenza viruses, well-established as reproductive hazards. 16 By mid-2021, as COVID-19 caused severe illness and associated complications for pregnant people, priority vaccinations were recommended by Canada 17 and the United States. 18 Although studies have described the impacts of the early waves of the pandemic on Canadian perinatal care experiences,12,19 mental health and coping strategies,20,21 and clinical outcomes, 22 societal pandemic responses continued to evolve and shape reproductive healthcare in Canada. Summer and fall 2021 in Canada were characterized by waves of Delta and Omicron SARS-CoV-2 variants, with COVID-19 vaccination mandated by many employment sectors. 15 Vaccination was required to access transportation, dining, entertainment, and recreational venues. 15 It is essential to understand how COVID-19 and related Canadian public health measures impacted pregnancy experiences. We therefore conducted a quantitative national survey (Pandemic Pregnancy e-Survey) to explore the Canadian healthcare experiences of individuals pregnant at any time during the pandemic. Our aim of this current study was to capture the pandemic pregnancy experiences of our participants in their own words by the qualitative analysis of their open-text survey responses. The inclusion of pandemic primigravid respondents together with multigravid individuals, pregnant both before and during the pandemic, allowed for a comparative analysis. Our findings build on existing research by offering a uniquely Canadian perspective on pregnancy experiences during the first 2 years of the pandemic, framed using a woman-centered care lens.
Methods
Participants
Respondents to the Pandemic Pregnancy eSurvey were invited to elaborate their experiences in open-ended survey questions. Individuals who were pregnant after January 1, 2020, aged 18–45 years, and who received perinatal healthcare in Canada were eligible to participate in this component of the survey analysis. Participants with no English literacy, who were not pregnant during the pandemic, or who received perinatal care outside of Canada were excluded from the study. The sample was further restricted for this analysis to those who provided at least one written response to any of the open-ended questions described below.
Data collection
An online, cross-sectional survey (Survey Monkey™, San Mateo, CA, USA) was designed to examine experiences of pregnancy care in Canada, including reproductive decision-making, both before and after the emergence of the pandemic. Specific to this analysis, participants were asked to provide demographic information including reproductive history, COVID-19 infection and COVID-19 vaccination history, and estimates of COVID-19 infection rates for regions where they received prenatal and labor and delivery (L&D) care. Survey questions were developed using a woman-centered care lens, with emphasis on choice, autonomy and informed consent.1,3 Open-ended survey questions (Box 1) enabled participants to expand on their perinatal care experiences and to provide any final comments. Respondents were recruited through social media, Facebook advertisements, and community groups from September 1, 2021 to February 1, 2022. Dates and times of survey initiation and completion were monitored regularly, ensuring no fraudulent patterns of participation.
Open-ended survey questions.

Note that these questions did not appear sequentially in the original survey.
Data analysis
Survey responses were extracted and cleaned to remove unconsented, missing/incomplete demographics data. We received a total of 1062 consented responses. Respondents who were not pregnant after January 2020 (in response to a pre-pandemic secondary survey component), did not receive perinatal care in Canada, or who did not answer any open-ended questions (Box 1) were excluded, such that 700 were eliminated from this sample. “Primigravid” participants reported their first pregnancy during COVID-19, whereas “multigravid” respondents indicated pregnancies both before January 1, 2020 and during the pandemic. Coding of open-ended responses was organized using NVIVO™ (Release 1.7.1 (1534); QSR International, Denver, CO, United States) as part of thematic 23 and content analysis. 24 Although we did not interview or interact with participants during data collection, we acknowledge that our respective positionalities as female, health sciences researchers may have influenced our interpretation of the data, and therefore we implemented a systematic and transparent coding process.23,24 One researcher (KPP) initially coded open-text responses, with a second researcher (SS-C) reviewing the coding strategy. Coding was framed by woman-centered care categories and survey questions and we incorporated an inductive approach wherein codes were developed from recurrent concepts or ideas in the data. Both deductive and inductive-developed codes were subsequently organized into categories (choice—healthcare provider, delivery place, support companion(s), autonomy—healthcare, vaccination), informed by principles of woman-centered care.1,3 Major themes were dominant topics, whereas subthemes described a subtopic of a major theme. Minor themes reflected divergent topics expressed by a minority of participants. As data analysis was conducted after survey completion, with no opportunity to explore or clarify participants’ brief open-ended text responses, we relied on the relative prevalence of major themes within our sample rather than traditional thematic saturation as an indicator of the appropriateness and quality of our sample. 25 Throughout, spelling, punctuation, and syntax errors in participant quotes are denoted “sic,” with abbreviations/corrections added for reader comprehension. Methodology, analysis, and presentation of our findings are consistent with Standards for Reporting Qualitative Research (Supplemental Material). 26
Results
Demographics
The sample was comprised of 362 respondents, including 195 primigravid and 163 multigravid respondents (Table 1). Although we recognize that non-binary genders can have pregnancy and birth experiences, the sample uniformly identified as “women”, was mainly Caucasian, with relatively high SES. A small proportion (~2.5%) of respondents indicated multiple pregnancy experiences during the pandemic, with pregnancy loss reported by about 6.4% of the sample. Most respondents were vaccinated against COVID-19 (Table 2), with almost half of the sample vaccinated during pregnancy, and about 20% while breastfeeding. Only 11% of women indicated previous COVID-19 infection, and of these, 61% were infected during pregnancy. Respondents received prenatal and L&D care in regions predominantly described as having moderate to high COVID-19 infection rates.
Demographics.

SD: standard deviation.
Indigenous respondents identified as First Nations (8), First Nations/Métis (1), First Nations/Black (1), Métis (11), prefer not to answer (1).
Immigrant participants were born in Netherlands, United States, England, Yugoslavia, Indian, Germany, and Philippines.
Visibile minority participants identified as Arab (2), Black (3), Chinese (1), Filipino (1), Latin American (3), South Asian (4), South Asian/biracial (1), Mixed race (2), and Prefer not to answer (2).
Four participants did not provide pregnancy history.
Information reported in open-ended questions.
Pandemic pregnancies includes reported pregnancy losses.
COVID-19 experiences.

L&D: labor and delivery.
Missing responses.
COVID-19 conditions: COVID-19 hot-spot—frequent or lengthy local lockdowns, regular outbreaks, and restaurants/gyms mostly closed; moderate COVID-19 infection rates—occasional local lockdowns, some outbreaks, and restaurants/gyms sometimes closed; low COVID-19 infection rates—lockdown only because of province, infrequent outbreaks, restaurants/gyms mostly open; what pandemic?—no COVID-19, life has been pretty normal, no lockdowns, no outbreaks, all businesses open.
Woman-centered care: major themes
Major themes, with accompanying subthemes, and minor themes were organized into categories to align with principles of woman-centered care.1,3 Overarching categories included: Choice of healthcare provider, Autonomy-healthcare, Choice of delivery place, Choice of support companion(s), and Autonomy-COVID-19 vaccination. Table 3 summarizes major/minor and subthemes for each category.
Themes organized by woman-centered care categories.

Choice of healthcare provider
Respondents characterized providers as generally supportive and attentive, captured as the major theme good quality healthcare providers (Table 4). Participants recognized efforts of their healthcare teams, including obstetricians and nurses, with many reporting excellent birth experiences. Midwifery care was idealized by many respondents, often contrasted with perceptions of poor-quality care provided by physicians.
Choice of healthcare provider.
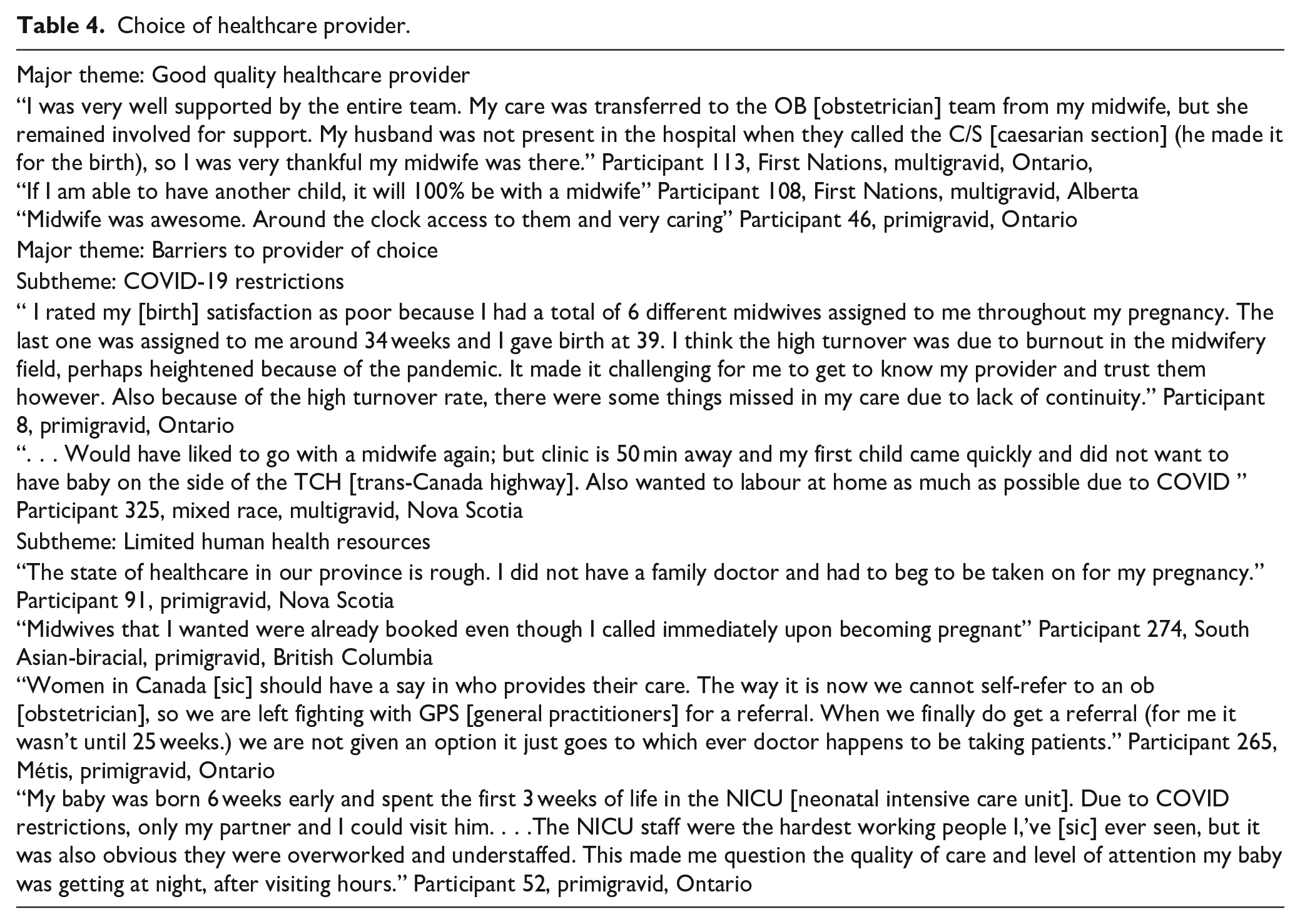
A second major theme, barriers to provider of choice, encompassed limited access to family physicians, lack of choice in the selection of obstetricians, and waitlists for midwifery access, with some regions lacking midwifery care entirely. Barriers to provider choice was further described by two subthemes, COVID-19 restrictions and limited human health resources. Both primigravid and multigravid respondents identified the first subtheme, COVID-19 restrictions, as barriers that prevented their access to doulas as L&D support companions. As described by this low-income, multigravid, Saskatchewan participant:
“We wanted a doula and she wasn’t allowed in. I feel as though her presence would have prevented the C-section” Participant 303.
A second subtheme, limited human health resources, was also recognized by participants as elements of systemic barriers to provider of choice. Respondents perceived that nurse staffing issues further contributed to a lack of continuity of provider care. Although the pandemic was perceived to have caused this limited availability of healthcare providers, participants also recognized ongoing healthcare system deficiencies specific to certain geographical regions. A primigravid, Ontario participant commented,
“Registered to get a midwife but was waitlisted. This is surprising. I contacted them in my sixth week of pregnancy in December and they were already full for August. May speak to the need for midwifery” Participant 196
Autonomy-healthcare
Perceptions of empowerment fostered either by participants’ prenatal/L&D teams, or by the experience of birth itself, were captured as a major theme—autonomy empowered (Table 5). Midwives were generally perceived as more empathetic and respectful, recognized as encouraging greater agency and informed decision-making compared to physicians. Many primigravid respondents expected proactive, transparent information sharing by healthcare providers to foster informed decision-making.
“I have developed a deep appreciation for midwifery care, as nothing has been forced upon me but rather options given. Their informed based approach is the epitome of female health care and respect. I feel so lucky to have had the choice to deal with midwives over doctors for primary care.” Participant 114, Primigravid, Ontario
Autonomy-healthcare.

For some participants, a second major theme, autonomy impacted, reflected negative perinatal experiences, particularly due to poor healthcare providers. The subtheme, provider as information gatekeeper, indicated healthcare providers who were dismissive, failed to respond to questions, explain procedures or medications. These experiences were particularly disconcerting for primigravid respondents:
“I did feel like the next steps in the process were rarely explained unless I probed my OB [obstetrician]. I felt largely in the dark most of the way and would have liked to have had more information of what would have been to come in the following trimesters.” Participant 80, Black, primigravid, Ontario
A second subtheme, lack of choice/informed consent characterized both primigravid and multigravid participants’ experiences with pressure from L&D providers, attempts to elicit consent while simultaneously performing procedures, not allowing adequate time for informed decision-making or failing to obtain consent for medications prior to administration:
“I had to ask for them to explain procedures. They never asked permission for students to touch me or stitch me up they just did. I was NOT ok with that.” Participant 243, primigravid, Alberta “The surgeon asked me, when I was already in the OR [operating room] right before the urgent csection [sic], if I was planning to have more kids and would he be performing a tubal ligation as well. That question really threw me off. I wished someone had talked to me about this before I was on the surgical table. I might have actually decided yes, but the way the question was delivered I had no time to consider it.” Participant 30, multigravid, Ontario
Choice of delivery place
When asked to consider whether their L&D location was impacted by COVID-19 or other circumstances, most respondents wanted hospital birth, got hospital birth (major theme; Table 6). The subtheme, hospital safest/only choice, indicated that L&D location was informed by many factors (e.g. proximity to home, prior experience, planned Cesarian section, high risk pregnancies) other than COVID-19 for most of the women in our sample:
“Pandemic was declared the same week I gave birth, it was all so new. Hospital was safest for baby and mom” Participant 46, primigravid, Ontario
Choice of delivery place.

SES: socioeconomic status—combination of highest educational attainment and household income; L&D: labor and delivery.
A second subtheme, limited community L&D options, referred to the lack of birthing centers or options for midwifery-attended births in rural/remote and Atlantic regions of Canada; considered to be greater barriers to choice than COVID-19. Northern Canadian residents described impacts of mandatory COVID-19 quarantine periods, relocation to L&D settings weeks prior to delivery, and associated financial burden.
“I live in a remote location which requires pregnant persons to fly at 36 weeks, stay at a hotel and wait until baby arrives. This definitely adds to the stress and fear of catching COVID due to travel, or my baby getting COVID but unfortunately without adequate medical care in some of the territories the decision to travel while pregnant is out of our hands. I also had to travel at 22 weeks for an ultrasound because they are not offered in my community” Participant 327, primigravid, multiple pandemic pregnancies, Nunavut “It [choice of delivery location] was impacted by lack of care in my community. We have to travel a minimum of 4 hours in order to give birth. . . . I was given 2 days notice that I needed to relocate 4 hours away for 8 weeks to receive care. I wasn’t allowed to come home in that time. I needed to stay in the city where I was paying for a second place to live. just so I could receive proper medical care. I had an emergency c section and was discharged 24 hours later, and told I could drive the 4 hours home. . . .We are seriously lacking adequate medical care in Northern Ontario. Something [sic] needs to change. .” Participant 265, Métis, primigravid, Ontario “No birthing centres and no doulas/midwife around Moncton [New Brunswick city]. Only place is hospitals really.” Participant 19, multigravid, low SES, New Brunswick
Choice of support companion(s)
The major theme, no support companion for prenatal appointments (Table 7) was further nuanced as two subthemes emotionally difficult and concerns that partner missing pregnancy experience.
“Not having partner allowed in during . . . Prenatal visits was emotionally negative” Participant 162, multigravid, Manitoba “I had to attend all prenatal appointments alone. It was both mine and my husbands first pregnancy and he was unable to be present for anything—ultrasounds, heartbeat, questions.” Participant 98, primigravid, low SES, Ontario
Choice of support companion(s).

L&D: labor and delivery.
Primigravid: respondents categorized “primigravid” if first pregnancy experience was during pandemic, regardless of subsequent pregnancies.
A minor theme, COVID-19 exacerbated experience of pregnancy loss, reflected participants’ distressing experiences without support companion(s) present.
“I had a miscarriage in May/June 2021 (before current pregnancy). I found that it was so hard going to ultrasounds alone and receiving bad news, as well as not being able to see my doctor in person. I was also admitted to the hospital with an infection post-miscarriage and it was even more stressful with the COVID restrictions. COVID impacted the quality of care I received and made a pregnancy loss even harder to cope with.” Participant 4, primigravid, Ontario
A second major theme, hospital restrictions L&D support companion(s) represented frustrations with policies limiting visitors typically to a single individual who could only be present once active labor was confirmed, such that early stages of labor were often unaccompanied.
“My baby was born at 35+1 [35 weeks + 1 day] I had to meet with NICU [neonatal intensive care unit] prior to delivery without my husband due to COVID restrictions. It was an overwhelming and unfortunate situation that would be difficult for any laboring person to go through without their support person.” Participant 358, primigravid, Newfoundland
Autonomy: COVID-19 vaccination
Vaccinated while pregnant/breastfeeding (major theme, Table 8) reflected the experience of most respondents (67.3%; Table 2), with both primigravid and multigravid respondents openly providing the precise timing of their COVID-19 vaccinations/boosters with respect to conception, pregnancy, and breastfeeding.
“I was vaccinated first while breastfeeding (May 2021 and June 2021); I was pregnant (5w) when I received my booster in Dec 2021” Participant 316, multigravid, Manitoba
Autonomy: COVID-19 vaccination.

SES: socioeconomic status—combination of highest educational attainment and household income.
A minority of respondents reported a lack of vaccination choice (minor theme), feeling pressured by healthcare providers, and forced by employers and government mandates to be vaccinated.
“I felt pressured to get the vaccine due to work and risks at my work to my pregnancy. I was concerned about vaccine risks to baby with limited research available. I also had covid in 1st trimester and healed from this and felt antibodies were helpful but still felt pressured to get the vaccine in order to maintain my position at work.” Participant 109, primigravid, Ontario
Some women expressed vaccine safety concerns (minor theme) in terms of potential adverse vaccine affects such as stillbirths, infertility, and menstrual cycle irregularities. These respondents also questioned the scientific validity of the vaccine, its efficacy and the lack of long-term studies.
“It is experimental still and approved of for emergency use only. It’s just coming to light that it affects woman’s cycles and it will probably take years for any longevity studies to come out for other potential harms.” Participant 176, British-immigrant, multigravid, Ontario
Discussion
Prenatal and delivery experiences during the COVID-19 pandemic reflect significant resilience in response to Canadian hospital policies that often impaired patient choices. Most women in our sample described their healthcare providers, particularly midwives, in positive terms, and were able to give birth in their preferred manner, accompanied by a support companion. Within these positive experiences, however, are accounts of healthcare professionals’ dismissive attitudes, failure to explain interventions or provide information, and breaches of patient autonomy, particularly during L&D. The impacts of COVID-19 on women’s experiences were most significant for those with complex perinatal care needs, including pregnancy loss and rural/remote residency.
Perinatal care provider
Provider competency, efficacious practice, and an experience of childbirth that is respectful, culturally appropriate, and individualized are factors that reflect robust perinatal care. Perinatal care provider selection not only determines the quality of perinatal care,13,27 but also will ultimately inform the philosophies of care, and in many cases, the locations for perinatal health services, including L&D. Provincial residence is the most significant factor informing perinatal care provider choice in Canada, followed by patient characteristics including SES, history of pregnancy complications/pregnancy risk, and Indigenous status. 28 Most Canadian births are attended by obstetricians or general practitioners with midwives—regulated in most provinces—comprising only about 6% of perinatal care providers.28,29 Barriers to healthcare provider choice for our respondents included both COVID-19 and systemic healthcare limitations, resulting in challenges to perinatal healthcare access and lack of continuity of care, similar to Canadian experiences of pregnant individuals at the beginning of the pandemic. 19 Deficiencies in the quality of Canadian perinatal healthcare, such as limitations in access to prenatal/postpartum care, breastfeeding support, and discomfort with virtual healthcare, were also reported by women pregnant during the first year of the pandemic.13,21 Our respondents were generally satisfied with their perinatal care providers, although midwifery care was perceived as particularly supportive. Canadian midwifery care fosters uptake of prenatal care, prenatal education, breastfeeding initiation, and maintenance, yielding positive patient experiences both before 30 and during the pandemic. 19 Unfortunately, due in part to a national shortage of midwives, 27 midwifery care is extremely limited in many Canadian communities—a fact recognized by our respondents.
Autonomy is central to positive experiences of pregnancy and childbirth, which in the context of perinatal care, includes involvement in reproductive decision-making and informed consent.6 –9,13 Although some respondents described their L&D experiences as empowering, the major theme autonomy impacted described incidents wherein providers failed to explain procedures or provide information, and lack of choice/consent, consistent with Canadian 31 and United States32,33 perinatal care experiences prior to the pandemic. Primigravid women in particular expressed frustration with healthcare providers’ dismissiveness and failure to answer questions. Toronto participants, pregnant and postpartum during the first year of pandemic, recommended that healthcare providers improve patient communication, emphasizing clarity and up-to-date explanation of hospital policies. 21 Similarly, women with Canadian birth experiences during the first year of the pandemic experienced reduced prenatal care, reporting that in some cases assertive advocacy was required to access healthcare. 12 A pre-pandemic U.S. study reported that age, being white, and multiparous were among the protective factors against mistreatment during childbirth. 33 Given that our sample was mostly comprised of white women of high SES, we were not able to fully explore perinatal experience of racialized and Indigenous women; however, studies from both Canada 34 and the United States 35 establish pandemic-amplification of existing perinatal healthcare disparities for these populations.
Location of labor and delivery care
Philosophies of perinatal care as medicalized or low intervention/holistic shape provider attitudes about where childbirth should occur in healthcare settings, in communities, or at home, which in turn can influence patient autonomy. Obstetricians and family physicians primarily attend births at hospitals and are generally not favorable toward home birth, whereas midwives offer choice of home birth to about 25%–30% of Canadian patients, in addition to hospital and birthing centers. 36 Canadians1,28,29 and Americans37,38 typically give birth in hospitals, with institutional settings of care associated with decreased patient autonomy and higher odds of mistreatment.32,37 Changes to preferred location of birth due to unanticipated obstetric emergencies or the pandemic can contribute to perceptions of loss of control, lack of involvement in decision-making, and may negatively impact childbirth experiences. 13 Despite the potential for COVID-19 disruptions, most respondents in our study planned for a hospital birth, consistent with similar pandemic birth plans reported by other Canadian,12,19 American,39,40 Australian, 41 and global studies. 42 Women in our sample identified high-risk pregnancies or lack of access to midwifery care, rather than COVID-19, as deterrents to their preferences for home births or birthing centers. A systematic review of perinatal care experiences in multiple countries determined that less than a third of patients contemplated/changed their birth plans or location due to COVID-19. 42 Shifts toward home/community births were typically influenced by fear of contagion, and restrictions to support companions and other institutional policies.39 –42 As many Canadian communities lack childbirth options other than hospital settings, 36 our respondents were resigned that the hospital was the only choice. About 20% of Canadians43,44 lack choice of perinatal care in their rural/remote communities, with relocation in advance of childbirth mandated by Health Canada for northern communities.45,46 Such birth evacuations are particularly traumatic for Indigenous communities, 47 as experienced by at least one Indigenous woman in our sample whose perinatal relocation was further aggravated by COVID-19 community restrictions, reflecting other similar experiences.48 –50 Indigenous scholars recommend return of traditional birth practices to Indigenous communities in Canada, an end to mandatory birth evacuations, and the need to enable Indigenous peoples’ to actively exercise agency in perinatal healthcare decision-making as guided by principles of reconciliation and decolonization.48–51
Support companion(s)
The World Health Organization has long affirmed the right to emotional and social support, commonly identified as a “support companion” or “labor companion” of choice, during childbirth.6 –9 Although the role of support companion(s) is primarily described during childbirth,8,9 the restriction of support companion(s) at prenatal appointments caused significant distress to our respondents and anticipatory fears of giving birth alone. Both primigravid and multigravid respondents expressed sadness that their partners missed these early prenatal appointments and thus, the “experience” of pregnancy consistent with findings from Canada12,13,19,52 and other countries.42,53,54 Participants with historical or pandemic experiences with pregnancy loss described enduring prenatal appointments without support companion(s) as traumatic. Support companion(s) during medical investigations of threatened or confirmed pregnancy loss are recognized to facilitate information processing and decision-making.55,56 Fears of obstetric complications or miscarriage are quite common following adverse pregnancy outcomes, but these concerns appear to have been heightened due to the potential consequences of COVID-19 infection, general pandemic uncertainty and stress, and reduced social support.52,57
Beyond their provision of emotional support, support companion(s) may also assist in the physical aspects of L&D including positioning, massage, and encouragement. 58 Support companion presence during L&D is empirically associated with increased spontaneous vaginal birth, shorter labor duration, better Apgar scores and positive birth experience.58,59 In Canada, partners are typically present for L&D, with about one-third of Canadians accompanied by additional support companions such as doulas, extended family members, or friends.1,29 Depending on local COVID-19 infection rates, Canadian hospitals typically limited the number of support companions and generally prohibited visitors.12,60 The majority of our sample were permitted a single support companion for hospital births, permitted hospital access only after progression to active labor with additional support companion(s) restricted, consistent with other Canadian,12,19,52 British, 57 and United States,40,61 studies. As described by our respondents, restrictive hospital policies invariably resulted in women laboring for hours alone, isolated, unable to access doulas, and additional support companion(s). By excluding partners throughout perinatal care, such pandemic policies can be characterized as regressive, preventing gender equality in the form of partner–infant attachment and parental involvement. 52 The exclusion of support companion(s), including Indigenous doulas or “birth helpers,” 50 further challenges the autonomy of Indigenous patients as they navigate Canada’s structurally racist healthcare systems.34,45,47,50
COVID-19 vaccine autonomy
COVID-19 vaccinations and booster schedules were openly described by the majority of our respondents in the context of reproductive phases—during conception, during pregnancy, or while breastfeeding—with a general sense of acceptance. Most respondents received at least one COVID-19 vaccine (~86%), with almost half of vaccinated participants immunized while pregnant, dependent on dose schedule and vaccine availability. Two global meta-analysis studies report COVID-19 vaccine acceptance rates among pregnant women at about 50% with considerable variability depending on country.62,63 In Canada, government and public health agency policies/health promotion resulted in public vaccination rates of about 80% by end of 2021, 15 with vaccine uptake of 57.5%–83.7% among pregnant Canadians by mid-2022.64,65 A small subsample of our respondents perceived the mandatory COVID-19 vaccine policies as a threat to their personal autonomy. Such mandatory COVID-19 vaccine policies were implemented for employees of federal, provincial/territorial, and many municipal government agencies and related public sector employees such as first responders, hospital and education workers in 2021.14,15,66 Vaccine safety concerns were expressed by a minority of our respondents, consistent with previous Canadian studies,64,65 and global meta-analyses.62,63,67,68 One of the more insidious pandemic myths was the suggestion that COVID-19 vaccination caused infertility and other adverse reproductive health outcomes. Such misinformation limited vaccine uptake among pregnant people69,70 and informed vaccine-decision-making for some of our respondents. Ironically, pregnant people were initially excluded from COVID-19 vaccination campaigns due to potential vaccine-induced fetotoxicity. 71 Ultimately, pregnancy was identified as a priority condition for COVID-19 vaccination given the increased morbidity associated with COVID-19 infection and arguments that exclusion on the basis of pregnancy limited personal autonomy and circumvented the process of shared decision-making between patients and providers.72,73
Limitations
Our evaluation of open-ended responses to survey questions has several limitations. The original study design was a cross-sectional, purposive survey, which did not enable in-depth exploration of respondent experiences. Although the sample size is quite large, not all participants answered each question and many survey respondents excluded from this analysis limited their responses to the original closed survey questions. No text or character limitations were imposed however, open-ended responses were typically concise. Nevertheless, the available text was sufficient to convey both positive and negative experiences related to perinatal care in Canada. Finally, the demographics of our sample indicate a predominantly white, high SES sample, individuals likely to have agency and power to negotiate pandemic risks and perinatal healthcare decisions.
Conclusions
Perinatal experiences were challenged by both COVID-19 and existing constraints of Canada’s provincial/territorial healthcare systems. Birth experiences were generally positive; however, choice of perinatal provider type was limited, with respondents identifying significant gaps in access to midwifery care. Negative perinatal care experiences were typically associated with healthcare providers’ lack of information sharing, and in some instances, procedures performed without consent. COVID-19 hospital policies disempowered women of their right to support companions during prenatal appointments, with L&D restricted to a single birth companion. Finally, although most of our respondents were vaccinated, many while pregnant or breastfeeding, a subset expressed concerns about COVID-19 vaccine safety, and perceived government/employer vaccine mandates as coercive.
Supplemental Material
sj-docx-1-whe-10.1177_17455057251331696 – Supplemental material for Experiences of Canadian perinatal care during the COVID-19 pandemic: Analysis of open-ended survey responses
Supplemental material, sj-docx-1-whe-10.1177_17455057251331696 for Experiences of Canadian perinatal care during the COVID-19 pandemic: Analysis of open-ended survey responses by Sigourney Shaw-Churchill and Karen P. Phillips in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.