
Abstract
There is considerable interest and enthusiasm within the clinical gynecologic oncology community regarding the potential for poly (ADP-ribose) polymerase inhibitors to play a critically relevant role in the management of epithelial ovarian cancer and particularly (although not exclusively) in the setting of known mutations in the BRCA gene. This review will briefly highlight the biological rational for the use of poly (ADP-ribose) polymerase inhibitors in this malignancy, followed by summary of currently available clinical data supporting the delivery of agents approved by the US Food and Drug Administration for non-investigative use.
Keywords
There is considerable interest and enthusiasm within the clinical gynecologic oncology community regarding the potential for poly (ADP-ribose) polymerase (PARP) inhibitors to play a critically relevant role in the management of epithelial ovarian cancer and particularly (although not exclusively) in the setting of known mutations in the BRCA genes. This review will briefly highlight the biological rational for the use of PARP inhibitors in this malignancy, followed by summary of currently available clinical data supporting the delivery of agents approved by the US Food and Drug Administration for non-investigative use.
Biological relevance of PARP inhibition in epithelial ovarian cancer
The ability of cells to repair DNA damage occurring either during the normal replication process or induced by external exposures (e.g. carcinogens) is an absolutely essential component of cellular survival. 1 The inability to repair such damage can lead to a variety of serious consequences, including cell death or the development of a malignancy.
As a result, it should not come as a surprise that cells possess a variety of pathways whose biological purpose is to repair different types of damage to its DNA. One of the critical mechanisms responsible for repair of double-stranded DNA breaks is controlled by the BRCA genes. The process of repairing double-stranded DNA is known as homologous recombination repair.
In the absence of the “normal” (wild-type) BRCA gene (e.g. BRCA1 or BRCA2 mutations), a second mechanism, controlled by PARP, becomes essential in the repair of DNA damage. Impressive pre-clinical data have revealed that in the presence of a BRCA mutation, inhibition of the function of PARP through exposure to an agent which inhibits PARP activity results in high degrees of cell death, while critically the addition of such a drug has minimal impact on cell survival in the presence of a wild-type BRCA gene.
It should be noted that other mutations in epithelial ovarian cancer patients have been found to result in the functional absence of BRCA activity even in the presence of a germline wild-type BRCA gene (a situation labeled, “BRCA-ness”), and mutations in BRCA have been found to be present solely in the tumor DNA (somatic mutation) while simultaneously absent in the germline of individual patients. 2
Olaparib
The initial experience with the use of PARP inhibitors in epithelial ovarian cancer management was with the drug olaparib. In phase 1 study of the agent that enriched the study population to include individuals with documented BRCA mutations (for the reasons cited above), radiographic partial or complete responses were observed in 9 of 19 patients with such mutations (8 with epithelial ovarian cancer) but in no individuals with wild-type germline BRCA (Table 1). 3 In addition, while a number of side effects were encountered, the drug was overall reasonably well-tolerated, and importantly, there was no evidence of an increase in the severity of side effects in individuals with a germline BRCA mutation.
Clinical activity of olaparib, rucaparib, and niraparib in recurrent epithelial ovarian cancer.
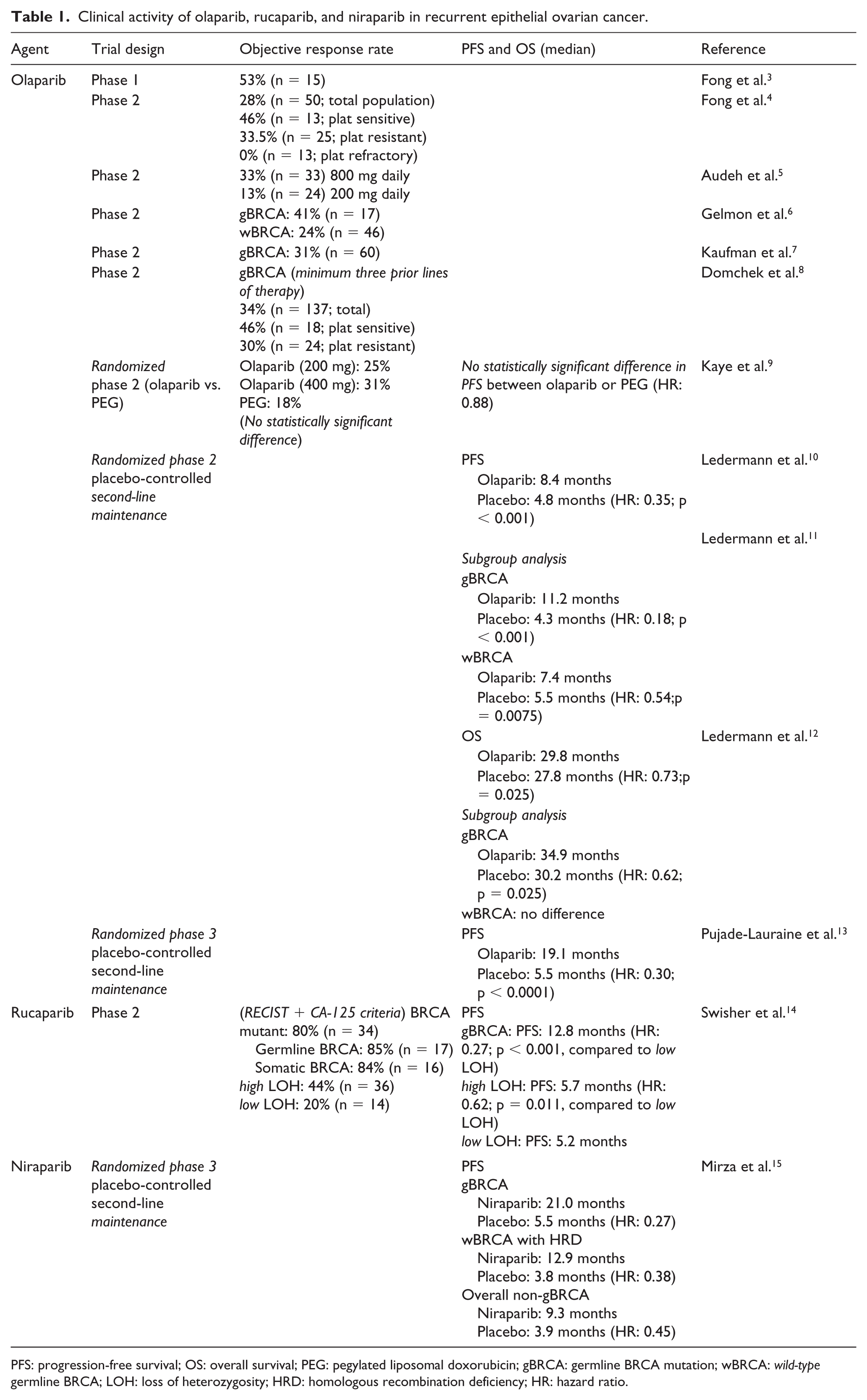
PFS: progression-free survival; OS: overall survival; PEG: pegylated liposomal doxorubicin; gBRCA: germline BRCA mutation; wBRCA: wild-type germline BRCA; LOH: loss of heterozygosity; HRD: homologous recombination deficiency; HR: hazard ratio.
A number of non-randomized single-agent phase 2 trial experiences with single-agent olaparib in previously treated BRCA mutation-positive epithelial ovarian cancer have been reported which confirm the relatively high objective response rate of the drug in this clinical setting (Table 1).
In one study involving patients with both platinum-sensitive recurrent disease (recurrence ⩾6 months following the last dose of platinum-based therapy) and platinum-resistant disease (no response or progression <6 months after the last dose of platinum-based therapy), 40% of 50 evaluable patients achieved an objective response. 4 The median duration of response in this trial was 28 weeks. In addition, and of relevance to the future use of PARP inhibitors in epithelial ovarian cancer, the study demonstrated a higher clinical benefit rate to olaparib in women with platinum-sensitive versus platinum-resistant cancers. The major side effects observed were fatigue and mild gastrointestinal symptoms.
A phase 2 trial exploring the optimal dose of olaparib revealed a higher objective response rate (33%; n = 33 patients) following treatment with a 400 mg twice daily dose of the agent compared to a 100 mg twice daily administration (13%; n = 24 patients). 5
In another study involving both high-grade serous or poorly differentiated epithelial ovarian cancer and triple-negative breast cancer, among the 63 women with epithelial ovarian cancer and measurable target lesions, an objective response of 41% (7 of 17) was observed in individuals with a documented BRCA1 or BRCA2 mutation and in 24% of patients (11 of 46) with no mutation. 6 The major side effects observed in the ovarian cancer patient population who participated in this trial were fatigue, nausea, vomiting, and decreased appetite.
In a trial which included multiple tumor types where patients were known to have a BRCA mutation, 31% of 60 women with epithelial ovarian cancer achieved an objective response. 7 The most common toxicities noted in this trial included fatigue and emesis. Grade 3 or 4 anemia was observed in 17% of the treated population.
Finally, in an evaluation of the efficacy of single olaparib in a population of epithelial ovarian cancer patients with a germline BRCA mutation who had received a minimum of three prior treatment regimens, an overall objective response rate of 34% (n = 137) was observed. 8 Within the platinum-sensitive (n = 39) and platinum-resistant (n = 81) groups, the objective response rates were 46% and 30%, respectively. The median duration of response (approximately 8 months) did not differ between these two populations.
A three-arm randomized phase 2 trial has also been reported which compared the clinical utility of two doses of single-agent olaparib to single-agent pegylated liposomal doxorubicin in the management of recurrent ovarian cancer in women with a documented germline BRCA mutation. 9 Even recognizing the limited size of this study (total of 97 patients), there was no statistically significant difference in either the objective response rate or progression-free survival (PFS) between the olaparib versus pegylated liposomal doxorubicin-treated patients, a perhaps somewhat surprising result (Table 1).
However, further analysis of this study led to the conclusion that while the observed outcome in the olaparib arms was as potentially anticipated, patients receiving pegylated liposomal doxorubicin in the trial experienced a superior outcome compared to that previously reported in similar ovarian cancer populations unselected for germline BRCA status. Of interest, a provocative retrospective analysis of the impact of this agent in a group of patients with or without a germline BRCA mutation confirmed the observation that PFS appears to be improved in epithelial ovarian cancer patients possessing this molecular abnormality and receiving treatment with pegylated liposomal doxorubicin. 16
Single-agent olaparib has also been explored as a “maintenance strategy” in high-grade serous ovarian cancer following the attainment of an objective response or “stable disease state” to second-line platinum-based chemotherapy. 10 In a randomized double-blind placebo-controlled phase 2 study (n = 265 patients), the delivery of olaparib in this maintenance setting resulted in a highly statistically significant improvement in PFS (median 8.4 months versus 4.8 months) following the completion of chemotherapy (hazard ratio (HR): 0.35; p < 0.001; Table 1).
While patients in this trial were not prospectively randomized based on their germline BRCA (wild type or mutation), the large majority of women (96%) had their mutation status subsequently analyzed. 11 In the population with a documented BRCA mutation, the PFS was almost three times longer (median 11.2 months versus 4.3 months; HR: 0.18; p < 0.001) following olaparib maintenance. 11 Furthermore, although of smaller magnitude, patients with wild-type BRCA also experienced an improvement in PFS with olaparib therapy compared to the placebo control (median 7.3 months versus 5.5 months; HR: 0.54; p = 0.0075). 11
The impact on overall survival (OS) associated with olaparib in this study was recently reported. 12 For the entire population, there was a median 2-month improvement observed (29.8 months versus 27.8 months; HR: 0.73; p = 0.025). However, for the group of individuals with a germline BRCA mutation, the median survival difference was 4.7 months (34.9 months versus 30.2 months; HR: 0.62; p = 0.025) with no difference observed in OS for the wild-type BRCA population.
Finally, the preliminary results of a randomized phase 3 trial examining second-line maintenance therapy in a patient population similar to that just described has been reported. 13 The outcome appears comparable to those observed in the randomized phase 2 study with a substantial improvement demonstrated in PFS (median 19.1 months versus 5.5 months; HR: 0.30) associated with maintenance olaparib in this setting.
Rucaparib
A second PARP inhibitor, rucaparib, has recently been shown to be clinically active in the second-line treatment of epithelial ovarian cancer. In an international phase 2 trial, 206 patients were treated with the agent, of whom 192 were able to be classified into three predefined “homologous recombination deficiency” (HRD) subgroups. In the BRCA mutation-positive patients (n = 40), a response evaluation criteria in solid tumors (RECIST)-defined objective response rate of 80% was observed.
Table 1 outlines the median PFS in these groups (BRCA mutation positive (n = 40), high “loss of heterozygosity” (n = 82), and low “loss of heterozygosity” (n = 70)). 14
The most common grade 3 (or greater) side effects of rucaparib observed in this trial were anemia and elevations in liver function tests (alanine aminotransferase or aspartate aminotransferase). Nausea was common (75% incidence), but rarely greater than grade 1 or 2 in severity (4% grade 3).
Of note, in a recent press release, the manufacturer of rucaparib has reported the positive results of a phase 3 randomized trial that examined the agent as a second-line maintenance approach in platinum-sensitive recurrent ovarian cancer. The formal presentation of these data at a future oncology meeting and publication of the results in a peer-reviewed manuscript are awaited with interest.
Niraparib
Niraparib was examined in a placebo-controlled phase 3 randomized double-blind trial as a maintenance strategy following the attainment of a response to a second-line platinum-based chemotherapy regimen 15 (Table 1). The trial design was also interesting, in that it included the examination of a novel proprietary molecular biomarker designed to predict for the presence of “HRD” in a setting where there was documented wild-type BRCA. The study revealed a highly statistically significant improvement in PFS for patients receiving niraparib with a germline BRCA mutation (median 21.0 months versus 5.5 months for placebo; HR: 0.27), in women with a proprietary biomarker-defined “positive HRD,” and also in individuals with wild-type BRCA whose cancers were not reported as being “positive” for this biomarker.
The most common grade 3 (or greater) toxicities of niraparib observed in this trial were hematologic effects (thrombocytopenia, anemia, and neutropenia), while nausea was common (74% incidence) in only 3% of cases of grade 3 or 4 severity.
Additional studies exploring the clinical utility of PARP inhibitors in epithelial ovarian cancer
Limited experimental data have provided provocative support for the potential clinical utility of PARP inhibitors in combination with an anti-angiogenic agent in ovarian cancer. 17 Further exploration of this concept is clearly indicated based on the documented utility of both classes of agents in the management of the malignancy.
Based on the utility of single-agent PARP inhibitors as therapy or employed in the maintenance setting, there is an obvious interest to directly combine these drugs with cytotoxic chemotherapy, particularly with a platinum agent. Current experience is limited, but provocative as regards the potential for exhibiting a favorable impact on clinical outcomes. 18 However, existing data also suggest that such combinations will not necessarily be easily developed due to overlapping or even synergistic toxicities (e.g. bone marrow suppression). Again, further examination of this general concept is certainly a relevant clinical question.
Another provocative concept is the potential utility of employing “a PARP inhibitor after a PARP inhibitor,” examining the relevance of treating with a second PARP agent after progression of the first drug. Recognizing that the currently available agents (and several PARP inhibitors in clinical development) likely have somewhat different mechanisms of action (as well as different toxicity profiles), it is reasonable to speculate that resistance to one drug will not necessarily indicate complete resistance to all PARP inhibitors. Exploration of this idea and other novel approaches (e.g. combination with checkpoint inhibitors) in carefully designed clinical trials are appropriate.
While existing data regarding the incidence of myelodysplasia and acute leukemia following delivery of PARP agents (a recognized theoretical risk of an agent inhibiting DNA repair following treatment with cytotoxic drugs) have suggested a low incidence of this serious side effect (<2%), further long-term follow-up of this patient population is required.
It is also reasonable to note that while HRD assays are being developed to help define the clinical utility of PARP agents in ovarian cancer, the various proposed systems identify different targets making it difficult to compare their relative utilities. It will be important for future studies to comparatively evaluate the several proposed platforms.
Finally, a critically important area for investigation is the mechanism of clinical resistance to PARP inhibition, including efforts to document the presence of particular mechanisms in individual patients and the subsequent development of strategies to prevent, reverse, or bypass the interfering molecular process.19,20
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.