
Abstract
Rural breast cancer survivors experience gaps in post-treatment education and support. We report the development and delivery of Reach Out to Rural Breast Cancer Survivors Program. Community-based participatory research and multi-level assessment were used to (a) engage rural community leaders, survivors, and providers; (b) analyze and report results of discussion groups to understand survivorship concerns and preferences; (c) integrate discussion group findings to develop, tailor, and deliver Reach Out; and (d) evaluate Reach Out with regard to satisfaction and helpfulness. In total, 16 rural breast cancer survivors participated in discussion groups. Four major concerns were identified through content analysis: lost in transition, self-management in survivorship, preference for support, and cancer surveillance. Major concerns and survivor preferences were integrated into Reach Out. A 15-item evaluation survey was used to assess the acceptability and helpfulness of Reach Out. In all, 72 participants attended three Reach Out programs; 96% completed evaluations of acceptability and helpfulness. In all, 68 were breast cancer survivors (99%), 88.4% were interested in the information; 91% indicated that personal objectives were met. Content about maintaining health, lymphedema management, and sexuality were ranked as most helpful. Rural survivorship concerns were similar to non-rural survivors, the major difference being access to services. In conclusion, multi-level assessment and community engagement were keys to understand rural survivorship and to develop and deliver content that attended to rural breast cancer survivors’ preferences.
Keywords
Background
Of the 14 million cancer survivors in the United States, over 3 million are female breast cancer, making them the largest group of survivors. 1 In the state of Alabama, breast cancer is the most commonly diagnosed cancer in women and the second leading cause of death, and more than 3400 new breast cancer cases are diagnosed annually. 2 Alabama is located in the southern region of the United States. It is predominantly a rural state with 54 of 67 counties (81%) designated as rural. 3 In all, 22 Alabama counties have breast cancer incidence rates (124.4–152.1 per 100,000) higher than the US average (123.0 per 100,000). 2 Rural Alabama residents are poor on numerous health and socioeconomic indicators such as low education, high unemployment, lack of insurance, poverty, and limited access to health care when compared to the residents of urban counties.4–8
Rural breast cancer survivors (BCS) face unique challenges that impact their quality of life.5,6,9 Rural BCS experience higher traveling time, lower access to health care and support service, and higher distress during and after cancer-related treatments, and overall lower quality of life when compared to their urban counterparts. 9 Azuero et al. 10 found that rural BCS were a higher risk for comorbid conditions (e.g. obesity and cardiovascular disease) and experience negative late effects (e.g. depression, pain, and sleep problems). In this same study, investigators also found that older rural BCS who suffered from obesity, low economic status, and low social support were more likely to experience challenges to their survivorship care in regard to their physical and psychosocial well-being.
Rural BCS encounter obstacles at numerous points across the cancer care continuum. 11 A recent review indicated that rural BCS continue to report psychosocial distress, depression, lack of social support, and poor access to cancer surveillance. 11 Accessibility and transportation concerns are additional obstacles to survivorship care. The review highlighted the urgency for tailored interventions to improve the survivorship experience of rural BCS.
Community-based participatory research (CBPR) has been a successful framework for engaging communities and researchers as partners in a variety of ways. Examples include the conduct of needs assessments, development of effective interventions to improve health outcomes for at-risk communities, and a method to decrease cancer disparities.12–16 A CBPR framework can help facilitate collaboration across different groups working toward a mutual goal and supports access to difficult to reach populations.13,14 Furthermore, CBPR supports capacity-building within communities and fosters positive relationships between the community and academic partners. 17
Angell et al. 18 reported that community involvement was essential to develop relevant interventions with rural BCS. More recently, multi-level engagement helps build CBPR capacity. 19 Multi-level engagement involves gathering stakeholders such as patients, providers, and institutions working together to develop sustainable patient-centered programs and models.19,20 Here, we report the (a) process of multi-level engagement of rural community leaders, BCS, and oncology providers; (b) analysis and results of rural BCS discussion groups to better understand survivorship concerns and preferences; (c) integration of discussion group findings to develop, tailor, and deliver a rural breast cancer survivorship program called Reach Out; and (d) analysis and results of Reach Out in terms of satisfaction with and helpfulness of the Reach Out program. Since multi-level engagement is a process, the authors report two separate, but related results. The stepwise process of multi-level assessment is depicted in Figure 1.
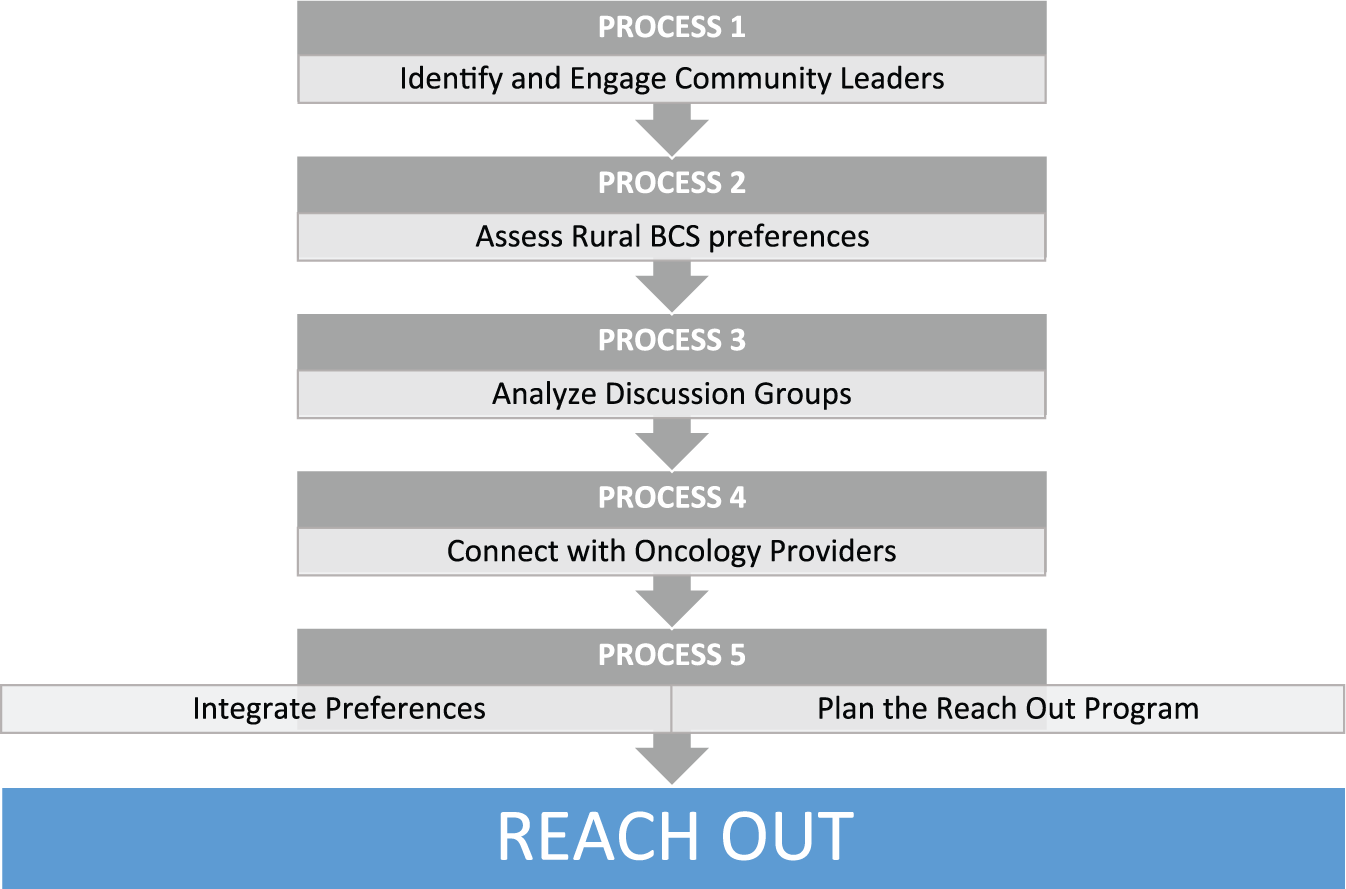
Multi-level assessment of rural BCS.
Materials and methods
The investigators received approval from the Institutional Review Board at the University of Alabama at Birmingham (Protocol #X110406004) to conduct the group discussions.
Process 1: identify and engage rural community leaders
In this article, a community is defined as a county. We identified four community health leaders in four rural counties located in Northeast Alabama. Rural counties were selected based on health indicators and breast cancer disparities. Residents in rural counties have higher poverty levels (22%–24%) compared with the state average (19%). 7 About 21% of rural residents are uninsured compared to the state average of 14%. 8 Breast cancer incidence rates (127.7 compared to 119.5 per 100,000 state) and mortality rates are likewise elevated in these rural counties compared to the state rate average (27.9 compared to 22.6 deaths per 100,000 state). 2 We queried the four community health leaders about their needs for breast cancer survivorship education and their interest in working together to deliver survivorship education. We sought community leaders who had experience in cancer care, were working within a health care or community system with patients and families, and would be willing and able to contact BCS and providers for the focus group or interview. Three community leaders in rural Northeast Alabama counties expressed interest, one in each county.
The community leaders agreed to contact rural BCS to elicit interest in participating in a group discussion. They provided rural BCS with the names of two authors (S.G.-C. and N.A.) and their telephone number to call for more information. Community leaders also contacted and provided names of oncology professionals within their community who expressed interest in discussing needs of survivors in their community. In addition, community leaders identified and/or provided a comfortable meeting space to conduct the discussion groups.
Process 2: assess rural BCS preferences
The purpose of the discussion groups was to learn more about rural women’s experiences in survivorship, how well they were managing, types of supports needed and availability, and concerns about cancer surveillance. The information and preferences gleaned from the assessment were used to formulate the content and style of the proposed Reach Out program.
A total of 28 rural BCS expressed interest in participating and provided a contact telephone number. S.G.-C. or N.A. made a follow-up call to answer questions, provide more in-depth information, and check eligibility. In total, 18 rural BCS were eligible and agreed to participate. Two days before the discussion group date, N.A. contacted the individual participants to remind them about the discussion group. In all, 16 rural BCS participated in one of the three discussion groups. They provided written informed consent prior to the start of the discussion. Two authors (S.G.-C. and N.A.) conducted the discussion group with S.G.-C. serving as the moderator. Using focus group techniques described by Krueger, 21 S.G.-C. gave a brief and warm welcome, an overview of the purpose of the meeting, ground rules for discussion, and then opened with the first of four open-ended questions: (a) Tell us about your concerns as a rural BCS; (b) Tell us about how you are managing in survivorship; (c) What kinds of support do you need, what supports are available, and what do you prefer? and (d) Tell us about your cancer surveillance and regular health checkups. Wherever necessary, S.G.-C. used pauses and probes to further stimulate discussion during the discussion.
N.A. served as the assistant moderator. She focused on active listening, took notes of the discussion, observed participant non-verbal responses, and monitored the recorder. The discussion groups lasted between 60 and 90 min and were audio-recorded. At the conclusion, S.G.-C. and N.A. summarized the discussion, asked whether the participants had additional comments or concerns, and provided a telephone number to call for further comments. S.G.-C. thanked them for participation, and N.A. provided a US$25 cash incentive for participation.
Process 3: analyze discussion group
Demographic data were obtained from the 16 rural BCS participants. They had a mean age of 66 years (range: 54–74 years), all were Caucasian non-Hispanic; the majority were married, and 75% were retired. About 37% had high school education or less, and 38% reported annual incomes below US$50,000. In all, 62% were between less than 1 year and up to 5 years since diagnosis. Participants traveled an average of 36 min for provider visits (range:<20–135 min).
The discussion groups were professionally transcribed. Transcripts were uploaded into NVivo® software 22 for analysis. S.G.-C. and N.A. each read the entire transcribed data. They used content analysis to review responses based on the four questions. 21 For each question, the participants’ actual words were documented, and the intended meanings of the words were explored. The context of responses, such as time in which the concern occurred, and the intensity of the responses were noted.
Results of group discussions
The authors generated 22 general themes related to major concerns of rural BCS: three themes related to feeling lost in transition in cancer survivorship; nine themes related to rural BCS self-management concerns in survivorship; five themes concerned survivorship support needed; and four themes related to concerns about cancer surveillance. Table 1 illustrates the major themes and related concerns with selected quotes.
Rural breast cancer survivor’ concerns and selected quotes.

DEXA: dual-energy X-ray absorptiometry.
Problems and concerns most important to rural BCS were similar to those reported by urban BCS.23,24 Physical side effects such as lymphedema, bone health, pain, fatigue, depression, hair lost, sexuality, hot flashes, and menopause were commonly identified concerns. For example, one survivor voiced her apprehension about sexual dysfunction stating, “I have bad vaginal dryness and intercourse just hurt me, and I thought something was wrong.” Another said that fatigue was so real that “If I listened to my body, I never would get up.” Lymphedema was another area of distress, particularly among rural BCS who carry the burden of heavy physical activities, “I was a Creeler, picking up yarn all the time in a carpet mill and running a machine. My arm just would get to big … But that doesn’t stop me from gardening and riding my lawn mower.”
Feeling lost in transition with fears of recurrence and the unknown were also expressed by survivors as illustrated with this quote, “I’d wake up at three in the morning and think how I am going to live and I’m going to die from this.” They expressed different types of supports needed including support from other survivors, family, spiritual, telephone, and community, as described in the quote “I really think county needs a better support system for breast cancer because when I had breast cancer, nobody came to my room and talked to me.” They also expressed the need of written information to better understand options, “If there could be some type of brochure that would tell what options are to a newly diagnosed breast cancer person.” Cancer surveillance and primary care activities were also important, as found in the quote, “I always get blood work done the week before I go to see him (oncologist). But I’ve had bone scans and chest x-rays and PET scan.”
The major concerns and related ones of feeling lost in transition, self-management, supports needed, and concerns about surveillance were remarkably similar to urban BCS. The major difference, however, was the availability and access on a regular basis to survivorship services. In addition, rural BCS preferred some type of face-to-face interaction. They indicated that they could not easily trust someone who they did not know face to face as illustrated in this quote: “I would like to see her first, for some reason. I want to feel comfortable first before I talk to her.” When asked about the top priorities for survivorship education, they identified fatigue, lymphedema, and sexuality. Furthermore, they desired more information in health-promoting activities including nutrition. The qualitative findings were subsequently incorporated into the Reach Out education and support program.
Process 4: connect with oncology providers
The purpose of connecting with oncology providers was to gain insights into their perspective of survivorship services. Five oncology providers (i.e. physicians, nurse, genetics counselor, and a breast cancer advocate) agreed to an informal meeting with the academic team (S.G.-C. and K.M.). The oncology provider group were not the individual community leaders. We met with them individually and queried them about their views on the types of community and/or institutional support needed, patient access to cancer surveillance, and their preference for types of education and support services. Given the informal nature of the meeting, S.G.-C. and K.M. jotted down notes rather than using audiotape. All oncology providers resided in their respective community for 5–8 years. No other demographic data were collected. In general, they concurred with rural BCS that organized survivorship support services were needed but not readily available in their county. Travel to an urban center to access survivorship services was not a reasonable alternative. They suggested a toll-free telephone call-in service as alternative for support. However, this suggestion differed from the survivors who expressed preference face-to-face survivorship services.
Process 5: integrate preferences and plan the Reach Out program
The authors met with community leaders in each of the three counties to integrate the preferences and needs expressed by rural BCS in planning the Reach Out program. Community leaders agreed to a face-to-face program expressed by survivors. They reasoned that the nature of close social interactions in their rural counties, and the need to address a variety of physical, psychosocial, and surveillance concerns could be addressed in one program. They also suggested that a luncheon and seminar format would best meet their survivors’ social and educational needs. Community partners chose the venue for program delivery, took responsibility for advertising the date and time of the program, announced the events to their networks, and registered the participants.
The authors developed the Reach Out educational format based on the rural BCS discussion findings, along with the community leaders and oncology providers’ suggestions. The format for the program consisted of lively lecture, question and answer, general discussion, peer support, and supplemented by written handouts. Reach Out format was a 2-h program starting with a welcome luncheon followed by lecture, discussion, peer support, and program evaluation. The educational format incorporated survivor preferences for self-management in fatigue, pain, depression, lymphedema, bone health, sexual function, and hot flashes and menopausal symptom management. Practical self-management tips on how to locate local resources such as a nutritionist or lymphedema specialist were integrated into the program. Specific tips to address sexuality and intimacy issues were included as were practical tips such as where to find over the counter lubricants. Other resources and supports included those available through the local chapter of the American Cancer Society and the Susan G. Komen affiliate.
Addressing sources of distress experienced by rural BCS that were identified in discussion groups were critical components to include in the Reach Out program. For example, the emotional distress during the transition from active treatment to survivorship as were feelings of being lost and uncertain about the future needed to be acknowledged. Participants shared helpful tips with one another such as being kind to oneself and reaching out to other BCS helped to knit survivors together as a group. Having an open and honest discussion about personal fears of recurrence and experiences of depression also provided rural women with the opportunity to let others know that they were not alone in their fears. These sources of distress and concerns identified through the analysis of the discussion groups were also incorporated into the development and delivery of the Reach Out program.
Results of Reach Out program evaluation
A 15-item evaluation survey was used to assess the acceptability and helpfulness of Reach Out, and preferences for future survivorship programs. The survey contained five questions about general demographics (e.g. age, number of years of survivorship, category of attendees, and existence of support services), eight questions relative to the acceptability and helpfulness of the program, and two questions about preferences for future program delivery. Participants completed the evaluation at the end of the Reach Out program.
A total of 72 participants attended the three Reach Out programs, and 69 (96%) returned their evaluations. Of the completed evaluations, 68 were BCS (99%) and one was a co-survivor. Participants had a mean age of 64.1 years (range: 41–88 years) with a mean of 7.7 years since diagnosis (range: less than 1 year to more than 15 years). Table 2 summarizes the demographics of participants.
Reach Out participants demographics.

BCS: breast cancer survivors.
Because of rounding, not all percentages total 100.
About 72% (n = 50) did not attend support groups. In all, 58% (n = 40) preferred group sessions for receipt of survivorship education. In general, 88.4% were interested in the information presented and 91% felt that their personal objectives were met. Table 3 summarizes the Reach Out program acceptability.
Reach Out program acceptability.

Because of rounding, not all percentages total 100.
Multiple choices.
Participants gave high marks to the tailored content of Reach Out. Content about maintaining health, lymphedema management, and sexuality were the most helpful. Content about emotions and fear of recurrence were not ranked as helpful despite these experiences were identified as a concern in the discussion groups. Overall, rural BCS found the Reach Out content was helpful. The summary is shown in Table 4.
Helpfulness of Reach Out program.
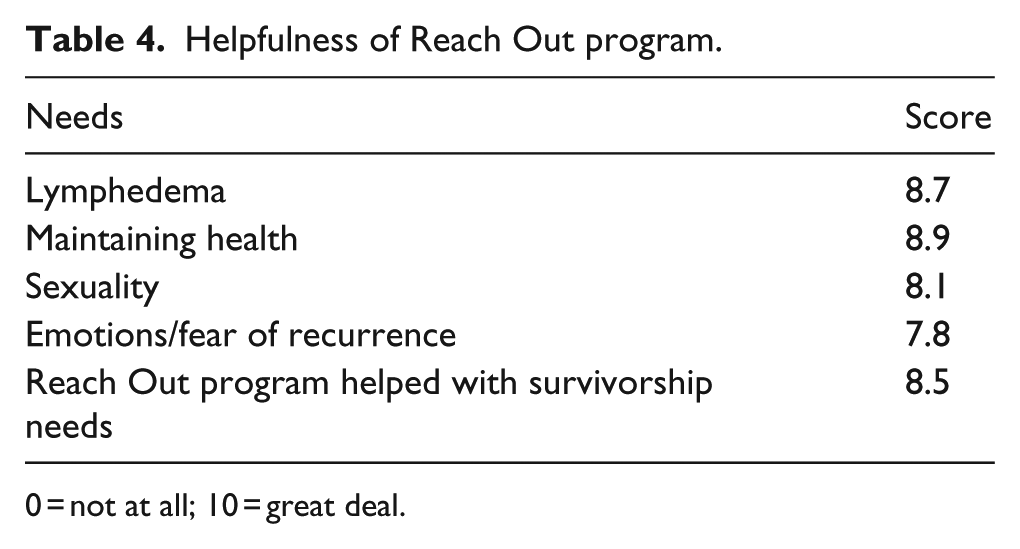
0 = not at all; 10 = great deal.
Discussion
Several lessons learned from Reach Out to Rural Breast Cancer Survivors deserve mention. First, CBPR served as an organizing framework to comprehensively address rural BCS preferences and needs in the community. The CBPR framework allowed for all involved to maintain consistent access across key community leaders, rural BCS, and oncology professions in rural Alabama counties. CBPR also fostered active partnership engagement in developing and delivering a cancer survivorship program based on rural BCS preferences, and community leader and oncology professional perspectives. For instance, the strengths in collaboration and open communication helped reach and promote more local resources for rural BCS.
Second, multi-level assessment to engage community leaders, rural BCS, and oncology providers as partners allowed for more robust assessment than would have been obtained by a CBPR framework alone. The variety of formats used for assessment including group discussions, informal interviews, and continuous discussions with community leaders helped to develop, deliver, and evaluate a relevant survivorship program. Multi-level assessment of rural BCS enriched our understanding of the daily lives of rural BCS and was invaluable in integrating survivors’ preferences into the Reach Out program.
Third, our findings support that rural BCS experiences are consistent with other BCS regardless of rural or urban residence.23–27 Rural BCS shared a picture of survivorship regarding the transition from patient to survivor and their specific self-management concerns. These experiences mirrored experiences expressed by BCS who were not rural. The shared concerns affecting quality of life such as fatigue, lymphedema, pain, changes in body image, acceptance of their new self, side effects of medication (i.e. aromatase inhibitors), menopause symptoms, maintaining health issues (cancer surveillance, bone health, and nutrition), emotional issues (depression, anxiety, and fear of recurrence), and sexuality were common across geographic boundaries. Thus, there were more similarities of survivorship experiences whether survivors were rural or urban residents. However, access to survivorship services and resources remained the major difference between rural and non-rural survivors, and continues to present challenges.
Finally, alternative strategies for survivorship support and education delivery are needed to continue to reach rural BCS. In our Reach Out program experience, community leaders stressed the desire for a face-to-face group program. Yet, the continued delivery of support and education using face-to-face formats alone may not be feasible nor sustainable in the long term. Alternatively, when participants were asked whether they would like to receive education and support services through telephone calls, they responded that telephone calls from someone they trusted was acceptable. Previous studies indicate that telephone support combined with written education can be used as a successful alternative to group support.9,28,29
Some potential alternatives to face-to-face education are electronic access and video conferencing. About 17% of Reach Out participants indicated a desire to receive online support. One study on video conferencing in a rural area found that this method could be a reasonable and feasible option to face-to-face education. 30 A second study using electronic access to palliative care education to a rural population also showed promise. 31
Study limitations are noted. First, we note that three group discussions among rural BCS is only a first step toward better understanding of rural survivors’ needs and experiences. Richer details could have been captured with either follow-up assessment or conduct of additional group discussions in other rural communities. Second, evaluations showed that the time allotted for the education component of Reach Out was short leading to insufficient depth. Here too, additional follow-up longitudinally rather than a one-time program would be preferred. Future efforts directed toward sustainability can be built on this program to develop strong survivorship support within the communities. Nevertheless, group discussions, individual interviews, and community engagement for Reach Out was successful in assessing BCS’ needs and delivering survivorship education and support in rural communities.
Conclusion
Rural BCS continue to experience gaps in post-treatment education and support. A CBPR framework that includes community leaders, the intended population of rural BCS, oncology professionals, and academic partners dedicated to improving survivorship care is an excellent starting framework to reach underserved rural BCS. Additional multi-level assessment using a variety of formats such as discussion groups with the population of interest and informal interviews with oncology providers, along with strong community leader collaboration can lead to successful program outcomes with strong potential for sustainability in the future.
Summary points
Rural women face challenges as BCS.
Rural BCS experience gaps in access to survivorship education.
CBPR is an excellent starting framework to reach underserved rural BCS.
Multi-level assessment using a variety of formats such as group discussions and informal interviews along with strong community leader support are vital tools to reach survivors.
Multi-level assessment and engagement are critical to achieve successful program outcomes.
Alternative methods for education and support delivery through electronic access may provide sustainable programs in the future.
Footnotes
Acknowledgements
We are indebted to our rural breast cancer survivors and oncology professionals who participated in the qualitative interviews. We thank Andrea Oliver, Cindy Sparkman, Betty Lou Covington, and Geri Monroe, our community partners who made “Reach Out” a reality. We thank “Reach Out” Nurses: Ann Wooten, Madeline Harris, and Rachel Benz.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical conduct of research
Authors obtained appropriate approval from the University of Alabama at Birmingham Institutional Review Board (Protocol X110406004). In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project was supported by a grant from Susan G. Komen North Central Alabama (LG-2011-AL100-UNAL73-00035). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed. No writing assistance was utilized in the production of this manuscript.