
Abstract
The aim of this study was to investigate women’s intention to use long-acting reversible contraception using two established models of health behaviour: the theory of planned behaviour and the health belief model. A questionnaire was completed by a convenience sample of 128 women attending a community sexual health clinic. The independent variables were constructs of theory of planned behaviour (attitude, subjective norm and perceived behavioural control) and health belief model (perceived susceptibility, perceived severity, perceived benefits, perceived barriers, health motivation and cues to action). The dependent variable was intention to use long-acting reversible contraception. The theory of planned behaviour and the health belief model accounted for 75% of the variance in intention to use. Perceived behavioural control, perceived barriers and health motivation predict the use of long-acting reversible contraception. Public health information for women considering using long-acting reversible contraception should be based around addressing the perceived barriers and promoting long-acting reversible contraception as a reliable contraceptive method.
Keywords
Introduction
It has been estimated that approximately 30% of all conceptions in the United Kingdom are unintended1,2 although some authors put the figure as high as 50%.3–5 Frost and colleagues 6 attributed 52% of unintended conceptions to women who were not using a method of contraception at the time of conception. A further 43% of unintended conceptions were with women who were using contraception but were using the contraceptive method either inconsistently or incorrectly at the time of conception.
The World Health Organization Medical Eligibility Criteria (WHOMEC) is primarily intended for use in developing countries where the risks associated with pregnancy are often extremely high, but it is the intention of WHO that the guidance be adapted for use in different settings in which the risk benefit ratio of contraceptive methods may differ. The US Medical Eligibility Criteria (USMEC) and UK Medical Eligibility Criteria (UKMEC) are two examples where the WHOMEC has been adapted to be applied to the different countries/settings. There are no significant differences between WHOMEC, USMEC and UKMEC as they are evidence-based recommendations on who can use contraception safely. In addition, the United Kingdom follows National Institute for Health and Care Excellence (NICE) guideline 30 for contraceptive use, which promotes the use of long-acting reversible contraception (LARC). 1
LARC does not rely upon a daily concordance and thus has been nicknamed the ‘fit and forget’ methods of contraception. 7 These are more adequately explained as a contraceptive method which requires one or less administration per cycle or month. There are four types of LARC licensed for use in the United Kingdom (copper intrauterine devices, progestogen-only intrauterine systems, progestogen-only injectable contraceptives and progestogen-only subdermal implants); however, uptake for LARC has been low accounting for only 12% of all contraceptives prescribed. 1
The theory of planned behaviour (TPB) and the health belief model (HBM) are socio-cognitive models of behaviour change which have been widely used in research on health-related behaviours and intentions. The HBM predicts intention to engage in positive health-related actions in terms of susceptibility to, and severity of, a negative health outcome and the benefits of, and barriers to, taking action. 8 The TPB describes the predictors of behaviours in terms of attitudes, expectations of significant others and perceived behavioural control. 8 Many researchers have argued that these models should be utilised in unison when investigating positive health behaviours as the belief-based HBM model variables can be used to interpret the attitudinal TPB measures. 8 A study of the literature suggests that there is a dearth of research that empirically compares different health psychology models; 9 however, there is evidence that more recently this is changing with more researchers finding value in this type of research.8,9 A few studies have used the HBM and the TPB together to examine health and health-related behaviours;8–13 however, as yet this has not been done in the contraception field; this article will begin to address this issue. Studies comparing the two theoretical models have explored behaviours such as testicular self-examination, 11 examining intentions and uptake of the human papillomavirus vaccination, 9 uptake of cervical screening 13 and cycle helmet use. 12 These studies show that a comparison between the two models is not clear-cut and that more research is needed to both compare the models and utilise the comparisons across different health behaviours.
The aim of this study was to utilise two models of health behaviour to explore the beliefs and attitudes that predict intention to use LARC and whether or not a woman is currently using LARC.
Materials and methods
Participants
A convenience sample was recruited over 6 weeks from eight community contraception and sexual health clinics in South East Wales collectively servicing approximately 144 clients per week. The clinics were for women who were at risk of pregnancy but did not want to get pregnant at that time and were seeking to use contraception. A total of 128 female participants took part in the study (mean age: 26.12 years, standard deviation (SD): 7.91). See Table 1 for demographic details. The study was only conducted in English and participants were not screened for literacy.
Descriptive statistics for participants.

SD: standard deviation; LARC: long-acting reversible contraception.
Research design
The research was cross sectional in design. The data analysis used was a multiple regression, the dependent variable was intention to use LARC and the independent variables were the constructs of HBM (perceived susceptibility, perceived severity, perceived benefits, perceived barriers, health motivation and cues to action), TPB (attitude, subjective norm and perceived behavioural control) and the construct of self-efficacy. The secondary analysis completed was a logistical regression using all the variables from HBM, TPB and self-efficacy as independent variables with the dependent variable being whether the participant is an existing user or a non-user of LARC. An a priori power analysis was completed using an anticipated effect size (f2) of 0.15, an alpha of 0.05 and power of 0.8 with 10 predictor variables set the sample size needed as 118 participants.
Measures
The measure used was a 59-item questionnaire constructed around the use of contraception. Participants were asked to provide some basic demographic information, such as, age, relationship status and did they have any children. They were also asked behavioural information regarding their contraceptive use. The measures used for the concepts of HBM and TPB as well as self-efficacy and intention to use LARC have been used previously8,9,11,13–19 and were adapted for pregnancy and LARC use. See Table 2 for details.
Concepts of the Health Belief Model (HBM), Theory of Planed Behaviour (TPB), self-efficacy and intention to use LARC explored by the research questionnaire.
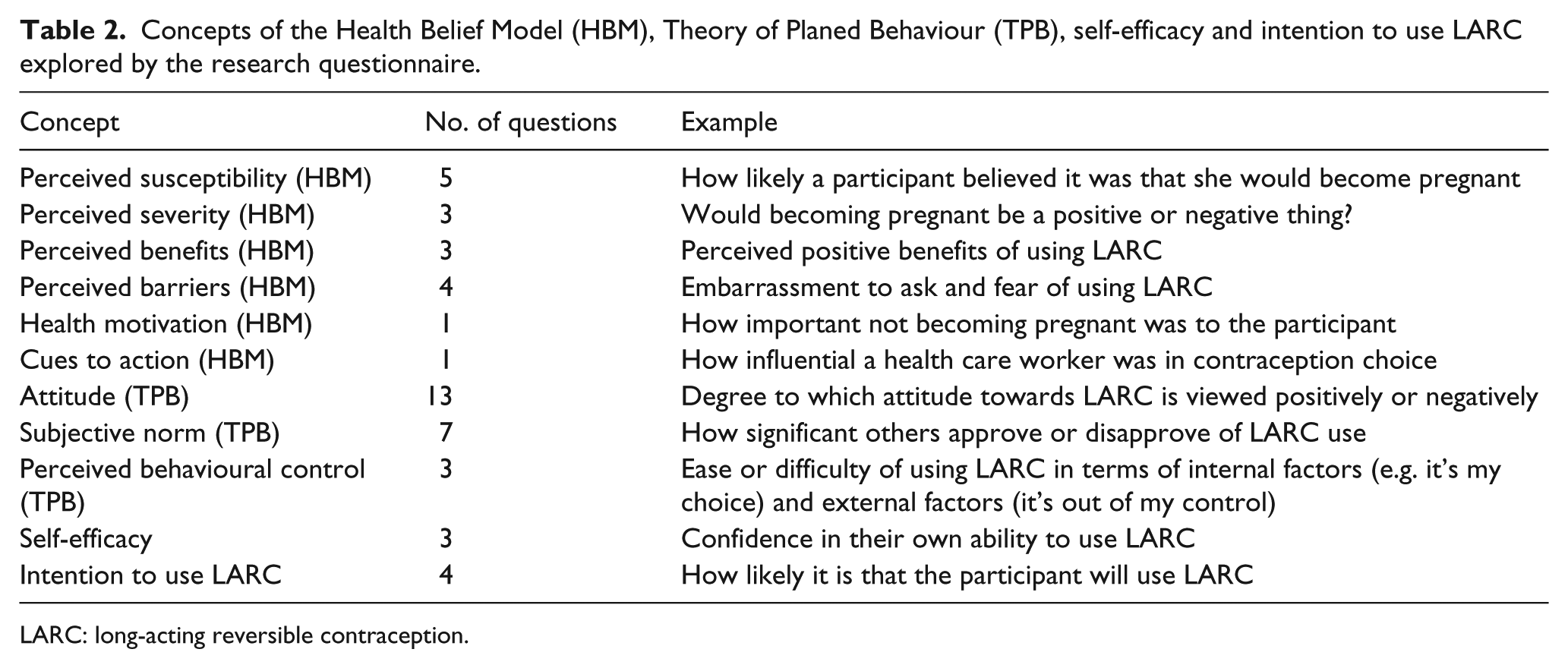
LARC: long-acting reversible contraception.
The question stems used in previous research have been shown to have high internal consistency (all α > 0.74), for measures of testicular self-examination, breast self-examination, dieting behaviour, cervical cancer screening and human papillomavirus vaccination uptake. To verify if this internal consistency was transferrable within this study, a post hoc sample of questionnaires was taken (N = 20) and a Cronbach’s alpha reliability analysis was completed for all of the concepts in Table 2 with the exception of health motivation and cues to action. All multi-item constructs were shown to have internal consistency with all scoring over 0.8. An exception to this was perceived susceptibility which only scored just above 0.5. All scores from the questions were on a unidirectional 7-point Likert-type scale, with 7 denoting a positive review (e.g. strongly agree) of the question and a 1 denoting a negative view (e.g. strongly disagree). All negatively framed questions were reverse scored. A mean score was taken as a composite score for each construct.
Procedure
Women aged between 16 and 45 years old were invited to take part in the study by the clinic clerk as they were being booked in to see a health care professional (either a nurse or doctor). All women were told verbally that taking part was voluntary and anonymous; if women agreed to take part they were given a research packet by the clinic clerk. Within the research packet was a letter inviting the women to take part, a participant information sheet, a consent form, a questionnaire and a self-sealing envelope in which to return the questionnaire. In all, 160 women agreed to take research packets yielding an 80% return rate.
Results
Descriptive statistics
Women who took part in the research were aged between 16 and 45 years (mean: 26.01 years; SD: 7.91), just under half of the women reported being in a relationship (48%) and over half did not report having children (53%). At the time of the study, over 86% reported using contraception. Of the 110 women using a regular method of contraception, 56% were already using LARC, and also the mean score for satisfaction with current contraception was above the median point on the scale (range: +1 to +7) (Table 1).
Linear regression results
A stepwise linear regression analysis (Table 3) was used to predict intention to use LARC (tolerance levels for all coefficients were above 0.2). The independent variables were entered in two steps: first, the predictor variables of TPB and the added variable of self-efficacy; second, the predictor variables of HBM. In this way, it is possible to see the predictive utility of the health models. In step 1, the variables of TPB and self-efficacy explained 50.1% of the variance in intention to use LARC (R2 = 0.501, adjusted R2 = 0.484), F(4,121) = 30.339, p < 0.001, with attitude and subjective norm emerging as significant independent variables. In step 2, there was a significant increment in the amount of variance explained in intention to use LARC (ΔR2 = 0.256), ΔF(6,115) = 20.209, p < 0.001. In this final regression, the variables under consideration accounted for 75.7% of the variance in intention to use LARC (R2 = 0.757, adjusted R2 = 0.736), F(10,115) = 35.820, p < 0.001, with subjective norm, perceived benefits, health motivation and cues to action coming out as significant predictors of intention to use LARC. The beta score for health motivation was negative, indicating that higher motivation to not become pregnant predicted lower intention to use LARC.
Summary of the linear regression analysis for variables predicting intention to use long-acting reversible contraception.
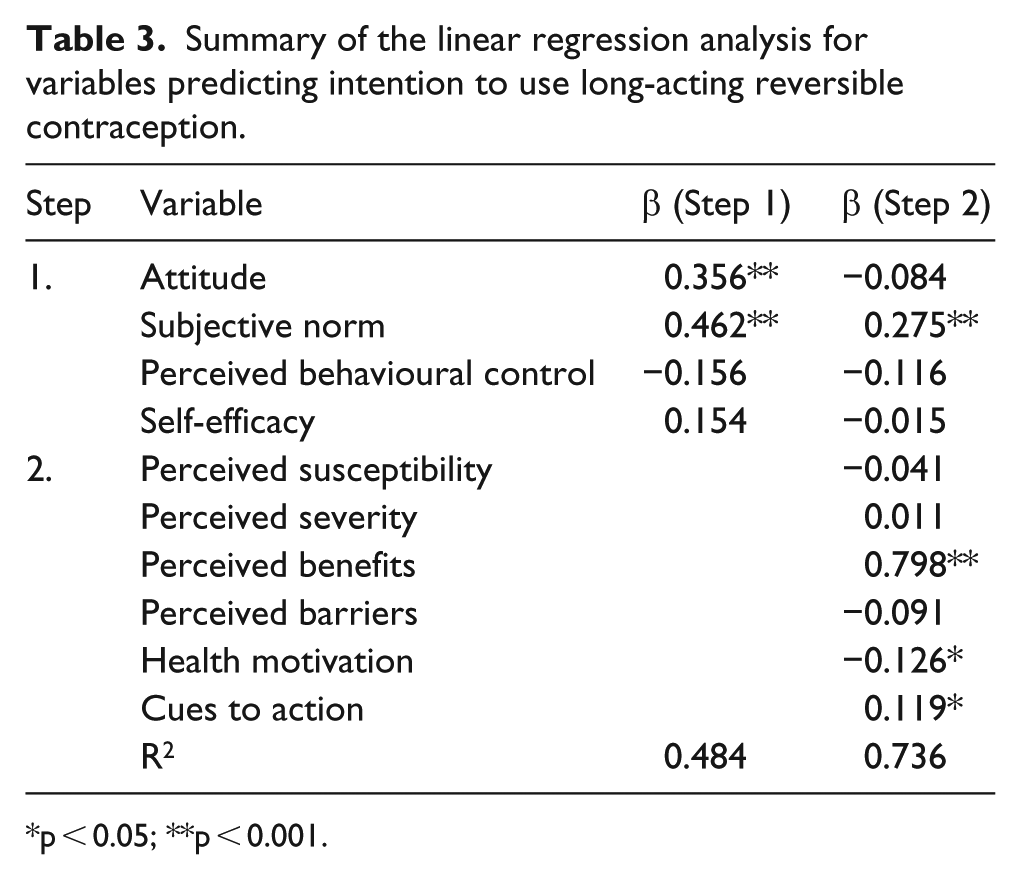
p < 0.05; **p < 0.001.
Logistic regression results
A hierarchical logistic regression analysis was used to explore whether the predictor variables of TPB and HBM could predict if a woman was using a LARC (Table 4). The independent variables were added in two steps: first, the variables of TPB (including intention and self-efficacy); second, the variables of HBM. The initial −2 log likelihood value for the constant model was 165.139. The inclusion of the predictor variables of TPB including intention and self-efficacy significantly improved the −2 log likelihood value to 132.781 with, χ2 (5, N = 122) = 32.358, p < 0.001 although only intention emerged as the significant independent predictor. The addition of the predictor variables of HBM also significantly improved the −2 log likelihood value to 112.753 with, χ2 (11, N = 122) = 52.386, p < 0.001, only perceived behavioural control, perceived barriers and health motivation were significant predictor variables. This suggests that as perceived behavioural control, perceived barriers and health motivation increase, the odds of a woman using LARC decreases.
Summary of hierarchical logistic regression analysis for variable predicting long-acting reversible contraception use.
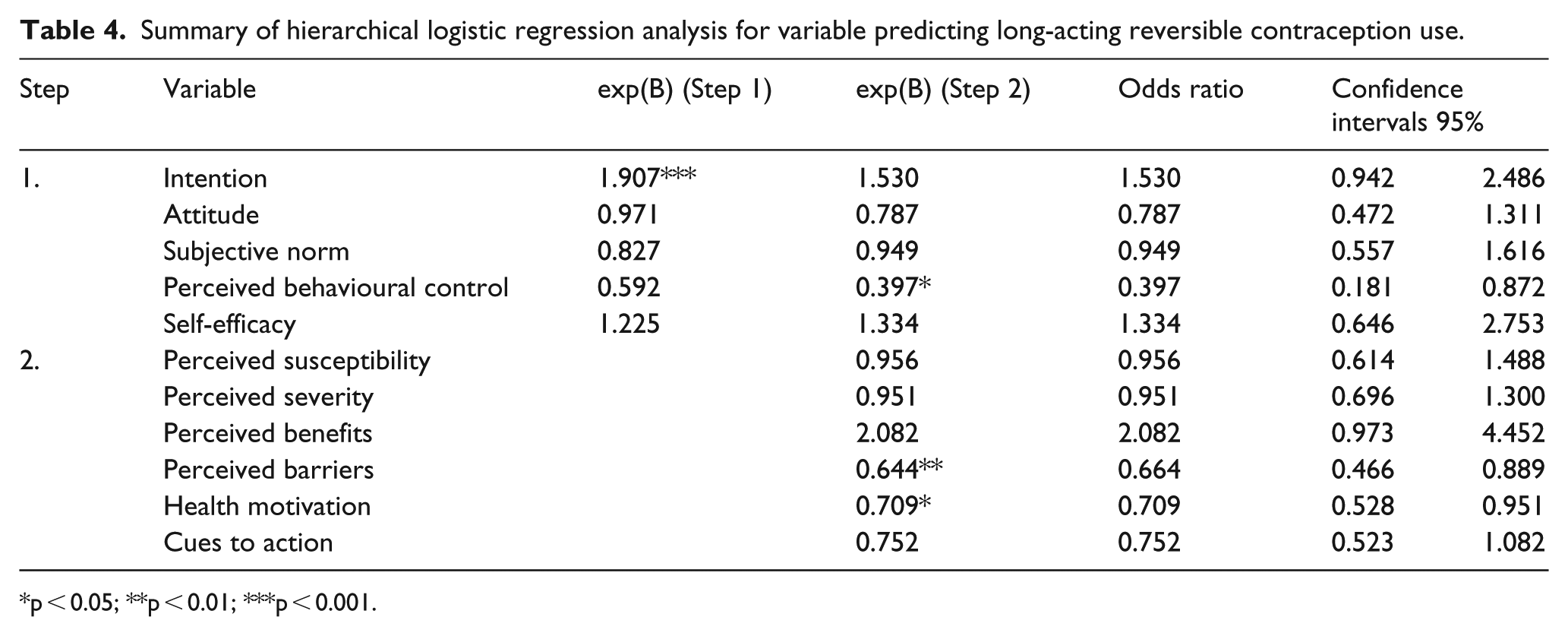
p < 0.05; **p < 0.01; ***p < 0.001.
Discussion
The linear regression with both TPB and HBM accounted for 73% of the variance in intention to use LARC. The construct with the strongest predictive power was perceived benefits. The next strongest predictor variable in this model was subjective norm in that the salience of the beliefs of others will increase or decrease a woman’s intention to use LARC. The other variables that predicted intention were cues to action and health motivation. Cues to action was a direct measure of how influential a health professional would be in contraception decision-making. A negative relationship between health motivation to avoid an unintended conception and intention to use LARC is counter-intuitive at first glance. However, this may be explained more realistically as a woman may be motivated to reduce the risk of an unintended conception and may be motivated to use contraception per se but not specifically LARC.
Intention was a significant predictor of whether a woman was using LARC. However, when the variables of HBM were added to the logistic regression, perceived barriers, perceived behavioural control and health motivation predicted not using LARC. Perceived barriers was the strongest predictor variable suggesting that as barriers to using LARC increase (e.g. fear appraisals such as it will hurt and the embarrassment of asking for LARC), the odds of woman using LARC decrease and that reducing barriers to obtaining LARC would potentially increase the uptake.
Increases in health motivation to reduce pregnancy reduced the odds of a woman using LARC. This is counter-intuitive in that higher motivation to reduce the risk of an unintended conception should increase the use of LARC. This similar counter-intuitive relationship is also seen with perceived behavioural control, as this increases as the odds of a woman using LARC decreases. Brown and colleagues 20 state ‘women that choose oral contraception had higher self-directedness scores, perceive themselves as more mature, strong, self-sufficient and trustworthy’. This could explain the negative relationship between perceived behavioural control and intention to use LARC in that, women who score high on perceived behavioural control would see themselves as being able to manage using non-long-acting contraceptive methods in a correct and consistent manner.
The United Kingdom follows NICE guidance 30 which promotes LARC although women’s choice is still paramount; however, using a counselling method such as motivational interviewing which will allow for women to explore the perceived barriers and benefits of the differing methods of contraception. This type of intervention also promotes client self-efficacy and health motivation.
Limitations
The current findings need to be interpreted in the context of a number of limitations. First, cues to action was measured by how influential a health care worker may be in contraceptive choice; however, external influences (outside of the health care setting, such as peers, information found on the Internet) are likely to have more of an impact on contraceptive choice.22 While some of this was captured in the TPB questions about attitudes and subjective norms, it was not specifically questioned in cues to action. Second, participants were not screened for literacy. Third, it should be noted that although intention did predict current LARC use, follow-up studies would be needed to assess the extent to which intention predicted future LARC use.
However, despite these limitations, interventions by health professionals that address the barrier reduction processes and increase processes that influence perceived benefits will be more effective in increasing the uptake of LARC. This has been shown to both reduce unintended conceptions and reduce the economic burden from these on the National Health Service (NHS).
Summary points
It has been estimated that approximately 30%–50% of all conceptions in the United Kingdom are unintended.
LARC does not rely upon a daily concordance and thus has been nicknamed the ‘fit and forget’ method of contraception; however, uptake remains low.
A study of the literature suggests that there is a dearth of research in the past that empirically compares different health psychology models in contraception use.
Constructs of the TPB and the HBM were able to predict intention to use LARC.
As perceived behavioural control, perceived barriers and health motivation increase, the odds of a woman using LARC decrease.
Interventions that will address the barrier reduction processes and increasing processes that influence perceived benefits will be more effective in increasing the uptake of LARC.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical conduct of research
Approval for the study was granted by the South East Wales Research Ethics Committee (Ref: 12/WA/0171).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was undertaken by Aneurin Bevan Health Board who received funding from the Welsh Ministers; the views expressed in the publication are those of the authors and not necessarily those of the Welsh Minister.