
Abstract
Different treatment options are available for patients with gynecological cancers. Imaging plays an important role in assessment of patients with common cancers involving uterine body, cervix and ovaries, from detection to evaluation of the extent of disease. The purpose of this review is to highlight the role of cross-sectional imaging techniques in treatment stratification and overall management of patients with endometrial, cervical and ovarian cancers. Several imaging techniques used are described, including ultrasound, computed tomography (CT), MRI and PET/CT. Specific imaging appearances of the most common uterine, cervical and ovarian cancers are discussed. Imaging findings corresponding to the 2009 revised International Federation of Gynecology and Obstetrics (FIGO) staging of gynecologic malignancies are also described. In the multidisciplinary evaluation of patients with gynecologic malignancies, the role of the radiologist has become central for accurate diagnosis and evaluation of extent of disease to achieve better treatment selection and planning.
Background
Imaging plays an important role in the pretreatment evaluation of patients with common gynecologic malignancies. Comprehensive imaging of the female pelvis can be achieved using a combination of ultrasound (US), computed tomography (CT), MRI and [18F]-fluoro-2-deoxy-d-glucose (FDG)-PET/CT. US is usually the first imaging modality used to evaluate a variety of gynecological symptoms such as postmenopausal vaginal bleeding and pelvic pain suspected to be ovarian in origin. The most important role for MRI is evaluation of local extent of disease in uterine and cervical malignancies [1,2] and it is a problem-solving modality in patients with complex adnexal masses. CT is the modality of choice for staging patients with ovarian cancer. It is also used to stage advanced endometrial and cervical cancer [1]. FDG-PET/CT is gaining popularity for staging owing to its ability to depict functional (e.g., glucose metabolism) in addition to structural tumor features [3]. This review will focus on the role of imaging in the pretreatment evaluation of endometrial, cervical and ovarian cancers, describing the characteristic imaging features of these tumors and their relevance to treatment selection and planning.
Imaging techniques: technical requirements
US
US is the primary imaging modality for the initial evaluation of the female pelvis. US is performed initially via a transabdominal approach with a 3.5–5 MHz curvilinear probe; a full bladder is required to provide a sonic window for the transmission of US from skin to pelvic organs. Transvaginal (TV) US is used for a more detailed assessment of the endometrium and the ovaries. TV US is performed using a 5–8 MHz transducer and requires an empty bladder to reduce the distance between probe and pelvic organs. Color power and spectral Doppler are techniques used to evaluate vascularity. US also has an important role in guiding diagnostic procedures (biopsy). Disadvantages of US include reduced image quality in obese patients, and a degree of interoperator variability.
CT
For evaluation of gynecologic cancers, contrast-enhanced CT of the abdomen and pelvis is performed in the portal venous phase, 70 s following an injection of intravenous contrast medium. Oral contrast medium is utilized to opacify the small bowel, which allows easier detection of bowel serosal deposits. The use of 3D reconstructions in sagittal and coronal plane is crucial in the evaluation of metastatic peritoneal disease in ovarian cancers. CT presents many advantages compared to other imaging modalities, including ready availability, short image acquisition times, large field of view, high spatial resolution and ability to rapidly perform multiplanar reconstructions. In addition, CT-guided biopsy is a safe and useful procedure. Disadvantages include the use of ionizing radiation – especially for young patients – degradation of image quality with metallic implants, such as a hip prosthesis, and the morbidity associated with possible adverse reaction to iodinated contrast agents.
MRI
Patients are asked to fast for 4–6 h prior to MRI examination in order to limit motion artifacts from bowel peristalsis (antiperistaltic agents, e.g., hyoscine or glucagon may also be used). Patients are also asked to void before the examination, as a full bladder may cause motion artifacts. Images are acquired in the supine position using a pelvic surface array multichannel coil. Vaginal opacification with gel may be used in cases where vaginal invasion is suspected. The basic imaging protocol for gynecologic MRI includes: T1-weighted images (T1WI) of the pelvis in the axial plane and T2-weighted images (T2WI) in the axial and sagittal planes. Fat-saturation T1WI are used to differentiate fat from hemorrhage. High resolution, small field of view, axial oblique (short axis) T2-weighted fast spin-echo images taken parallel to the short axis of the uterine corpus are essential to accurately evaluate the depth of myometrial invasion in endometrial carcinoma (Figure 1) [4]. In patients with cervical cancer, high-resolution small field of view axial oblique (short axis) T2-weighted fast spin-echo images taken parallel to the short axis of the cervix are essential to accurately evaluate the depth of cervical stroma and parametrial/paracervix fat tissue invasion (Figure 1) [5]. Dynamic multiphase contrast-enhanced MRI, using 3D gradient echo T1WI after intravenous gadolinium administration, is performed typically before and at 2–3 timepoints after gadolinium injection (e.g., 1, 2 and 3–5 minutes). Diffusion-weighted MRI (DW-MRI) is now incorporated in most standard MRI staging protocols. DW-MRI should be performed at two or more b-values, which include a low b-value (0–100 s/mm2) and a high b-value (750–1000 s/mm2). Advantages of MRI include superior soft-tissue contrast and absence of ionizing radiation.

PET
PET/CT is a functional imaging modality that uses a short-lived radionuclide, FDG. FDG is a glucose analogue, which is taken up by metabolically active cells, such as tumor cells, and subsequently detected by PET imaging. To provide anatomical localization of the abnormal tracer uptake, PET imaging is combined with low-dose CT. Patients are asked to fast for at least 6 h prior to the PET/CT in order to keep serum glucose and insulin levels low. If insulin levels are too high, FDG can be taken up by skeletal muscle, potentially leading to a nondiagnostic study. After intravenous injection of 300–700 MBq of FDG, the patient is required to rest in a warm room for 1 h, to prevent uptake in muscles and brown fat. FDG is excreted by the kidneys and therefore the patient should empty their bladder prior to imaging, to reduce urinary FDG obscuring tracer uptake in the rest of the pelvis. In addition to the qualitative assessment of FDG-PET/CT, measurement of standardized uptake value and other volume-based quantitative parameters derived from FDG-PET/CT such as metabolic tumor volume and total lesion glycolysis may provide additional prognostic information in gynecological cancers. False-positive findings relating to a physiological radiotracer uptake may be seen in the endometrium, ovarian follicles and corpus luteum cysts in premenopausal patients. FDG tracer uptake may also be seen in fibroids and inflammatory processes within the pelvis.
Endometrial cancer
Epidemiology, risk factors & diagnosis
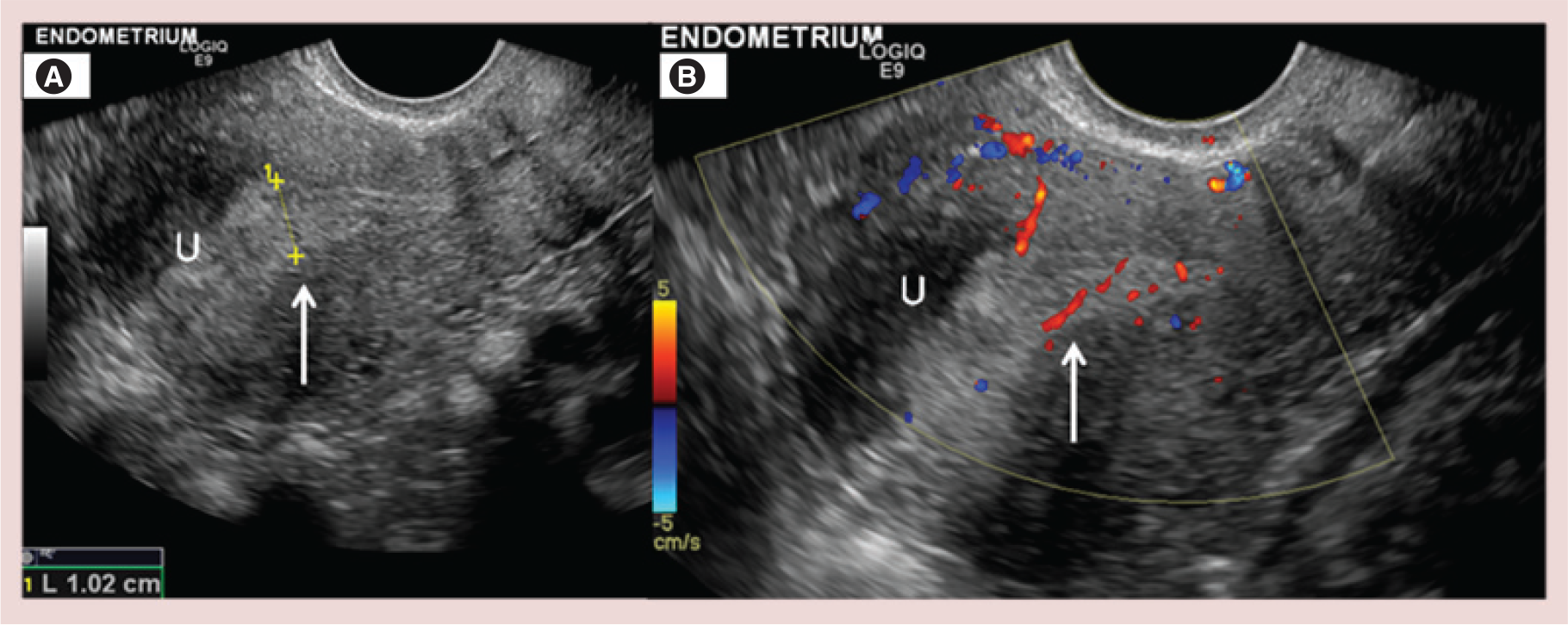
Endometrial carcinoma is the commonest gynecological malignancy in industrialized countries. More than 90% of cases occur in postmenopausal women over the age of 50 years old. Risk factors include conditions leading to increased estrogenic exposure, such as hormonal replacement therapy, obesity, tamoxifen use, early menarche, late menopause, nulliparity, history of polycystic ovary disease and hereditary nonpolyposis colorectal cancer (also known as Lynch syndrome). Endometrial carcinomas are divided into two histological subtypes. The most common histology is endometrioid adenocarcinoma (type 1), further subdivided in grade 1 (well differentiated) to grade 3 (poorly differentiated). Type 2 endometrial carcinomas include serous papillary and clear cell adenocarcinomas. Serous papillary, clear cell carcinomas and grade 3 endometrioid adenocarcinomas demonstrate more aggressive biology and with high probability of locally advanced or distant disease at presentation. Postmenopausal vaginal bleeding represents the early symptom in endometrial carcinoma. TV US is the initial imaging modality of choice to evaluate the endometrium in patients presenting with bleeding [6–9]. In postmenopausal women there is atrophy of the endometrium, which appears on TV US as a thin, regular double-layer echogenic line <5 mm in width [10]. An endometrial thickness <5 mm has a high negative predictive value for the presence of endometrial pathology [8,11,12]. On US, the presence of endometrial heterogeneity, focal or diffuse endometrial thickening >5 mm in the setting of postmenopausal bleeding should be considered suspicious (Figure 2). Definitive diagnosis of endometrial cancer is made by endometrial biopsy or dilation and curettage.
Staging & the role of imaging
Staging of endometrial carcinoma is most commonly performed using the International Federation of Gynecology and Obstetrics (FIGO) surgical-pathological staging system, revised in 2009 (Table 1) [13]. FIGO staging comprises a total abdominal hysterectomy, bilateral salpingo-oophorectomy, peritoneal washings and retroperitoneal lymph node dissection. Prognostic features that predict disease beyond the uterus include tumor histology and grade, presence of lymphovascular space invasion, deep myometrial invasion and cervical involvement. Imaging is not included in FIGO staging, but MRI and CT can provide relevant information prior to surgery [14]. When the extent of disease seen on imaging is combined with tumor biopsy histology and grade, an accurate assessment of risk stratification and prognosis can be obtained prior to surgery.
The revised FIGO staging (2009) of endometrial carcinoma.
FIGO: International Federation of Gynecology and Obstetrics.
Reproduced with permission from [13].
TV US
US has a role in centers with no access to MRI (Figure 2). TV US can assess myometrial invasion in stage I disease. Myometrial invasion is documented when the endometrial mass disrupts the subendometrial halo and/or invades the subjacent myometrium. TV US has been reported to have a sensitivity of 77–100%, a specificity of 65–93%, and an overall accuracy of 60–76% in assessing the degree of myometrial invasion [15]. Assessment of myometrial invasion is more difficult when the myometrium is thinned (postmenopausal) or distorted by fibroids [16]. Objective US measurement techniques (tumor/uterine anteroposterior diameter ratio and minimal tumor-free margin/uterine anteroposterior diameter ratio) have been recently validated as useful tools for evaluating myometrial invasion [17]. When performed by expert operators, TV US has been demonstrated to be a feasible, inexpensive imaging modality with a diagnostic accuracy comparable to that of contrast-enhanced MRI for the preoperative assessment of cervical involvement by endometrial cancer [18]. However, the role of US in predicting the presence of lymph node metastasis remains limited [19].
MRI
MRI is the imaging modality of choice for local staging of endometrial cancer. The European Society for Urogenital Imaging (ESUR) recommends MRI for staging of high-grade endometrioid adenocarcinomas (type I histology) and serous papillary and clear cell adenocarcinomas (type II histology) [20], while the National Cancer Institute in France has incorporated MRI into the preoperative assessment of all patients with endometrial carcinoma [21]. When reporting staging MRI, important factors such as tumor grade and histology should be considered, as grade 3 endometrioid adenocarcinoma, serous papillary and clear cell carcinomas demonstrate more aggressive behaviors with an high pretest probability of advanced disease (stage IB or greater) and/or peritoneal spread at presentation [22].
The normal zonal uterine anatomy is well demonstrated on T2WI, typically revealing high signal intensity endometrium, surrounded by the low signal intensity of the junctional zone (inner myometrium) and finally surrounded by the intermediate signal intensity of the outer myometrium (Figure 1). Endometrial cancer is usually isointense to the myometrium on T1WI and of lower signal intensity than the endometrium on T2WI. On dynamic multiphase contrast-enhanced 3D T1WI, the tumor enhances homogeneously, more slowly and less avidly than the adjacent myometrium (Figure 3). On diffusion-weighted imaging (DWI), the tumor is of high signal intensity (Figure 3) with corresponding low signal intensity on the apparent diffusion coefficient (ADC) maps.

Stage I
Stage I tumors are confined to the uterine corpus and account for more than 80% of cases. Presence of lymphovascular space invasion on pathology correlates strongly with presence of lymph node metastases. However, it can only be identified within the hysterectomy specimen. Depth of myometrial invasion can be used as a surrogate imaging marker for lymphovascular space invasion and therefore likelihood of nodal metastases [23]. Stage IA includes focal or diffuse endometrium thickening without myometrium invasion or with less than 50% of myometrial depth invasion. Tumor invading more than 50% of myometrium represents stage IB disease (Table 2). High resolution, small field of view, axial oblique T2WI parallel to the short axis of the uterine corpus are essential to evaluate the depth of myometrial invasion (Figures 1 & 3) [4]. Peritumoral inflammation can lead to overestimation of myometrial invasion on MRI. Pitfalls in assessing myometrial invasion also include leiomyomas, adenomyosis, loss of junctional zone definition and myometrial compression by polypoid tumor. The sensitivity and specificity of MRI in assessment of the depth of myometrial invasion vary between 69–94% and 64–100%, respectively [24]. The addition of 3D multiphase contrast-enhanced T1WI and DWI increase the accuracy in determining the depth of myometrial invasion [25]. In particular delayed post-contrast 3D T1W images (2–5 min post gadolinium injection) facilitate evaluation of deep myometrial invasion, providing maximum tumor-to-myometrium contrast. This increases staging accuracy when tumor appears isointense to normal myometrium on T2WI or where tumor extends into the uterine cornu (Figure 4), when it is difficult to accurately evaluate the depth of myometrial invasion on T2WI alone due to myometrial thinning [26]. Studies have shown that the ADC of endometrial cancer is significantly lower than of endometrial polyps and of normal endometrium [27]. Additionally, ADC represents a noninvasive prognostic tool, since lower values are characteristic of high grade endometrial cancers.
Key MRI features according to revised FIGO staging of endometrial carcinoma.
DWI: Diffusion-weighted imaging; FIGO: International Federation of Gynecology and Obstetrics; T1WI: T1-weighted image
T2WI: T2-weighted image.

Stage II
Stage II disease is characterized by direct invasion of the cervical stroma (Tables 1 & Table 2). Invasion of the cervical stroma is associated with a high risk of lymphovascular space invasion, directly correlating with the risk of lymph node metastases. On T2WI, cervical stromal invasion is represented by intermediate to high signal intensity tumor disrupting the normal low signal intensity cervical stroma (Figure 3). Use of dynamic postcontrast T1WI is useful in distinguishing between cervical invasion and polypoidal endometrial tumor protruding into the endocervix. Enhancement of cervical mucosa on postcontrast images, can confidently exclude cervical stroma invasion (Figure 4) [28]. In detecting invasion of the cervical stroma, MRI has an overall accuracy of 90–92% with sensitivity and specificity of 75–80% and 94–96%, respectively [29,30].
Stage III
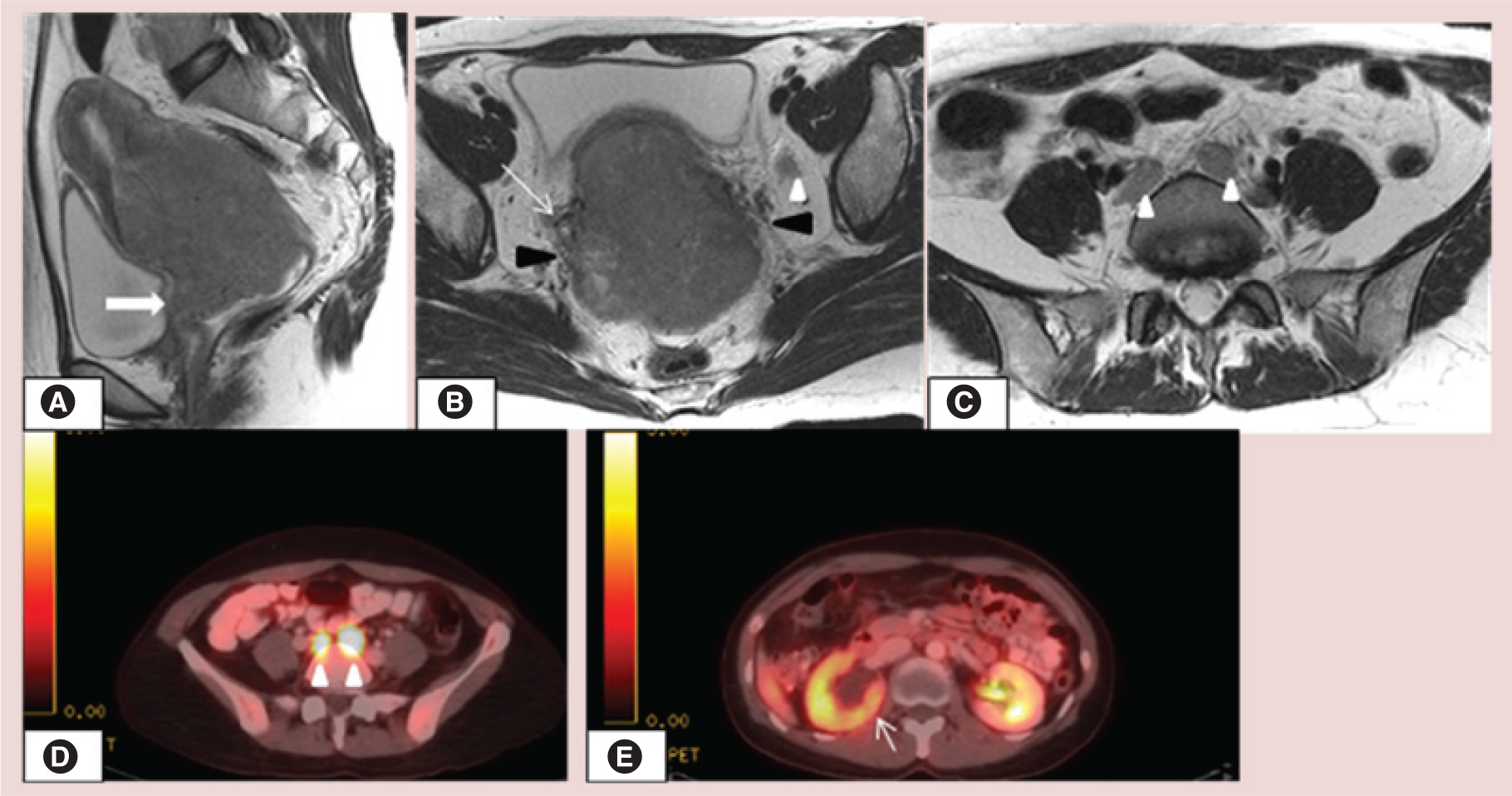
Stage III disease is defined by pelvic spread. Stage IIIA indicates involvement of uterine serosa or adnexa. Serosal involvement is seen as irregular uterine margins on T2WI with disruption of the normal hypointense signal of the serosa and disruption of the normally enhancing rim of the outer myometrium on contrast-enhanced T1WI (Table 2). Tumor may be identified in the adnexa, even without serosal involvement, especially with high grade, clear cell or serous papillary carcinoma. DWI can aid detection in these cases [25]. In stage IIIB disease tumor invades the upper vagina – indicated by segmental loss of the low signal intensity of vaginal wall on T2WI – or invades parametria – indicated by disruption of the low signal intensity cervical stromal ring with nodular and irregular tumor tissue extending into parametrial fat tissue. If parametrial invasion is present, a more radical surgical approach will be required. The presence of enlarged regional and/or para-aortic lymph nodes indicates stage IIIC disease (Figure 5). A short-axis diameter >8–10 mm is typically used to diagnose nodal involvement on MRI, although the sensitivity and specificity for detection may be altered by using locally agreed smaller or larger cutoff sizes [31,32]. Detection of lymph nodes may be increased by using DW-MRI due to the high signal intensity returned from nodes, although correlation with T2WI is always required [33].

Stage IV
Stage IV is defined by tumor extension beyond the true pelvis or invasion of bladder or rectal mucosa. On MRI, loss of low signal intensity of the bladder or rectal wall and tumor invading the mucosa is suggestive of stage IVA disease (Table 2). Bladder bullous edema is a frequent sign of tumor in the subserosal or muscular layer, but does not qualify stage IVA disease. In stage IVB disease, distant metastases (including nodal enlargement above renal veins or in the inguinal region), malignant ascites or peritoneal deposits are present. The latter are more common with high grade, clear cell or serous papillary tumors. Distant spread to lung, liver and bone is rare at presentation.
CT
CT is commonly used in the assessment of advanced endometrial disease and in identifying extrauterine spread and enlarged lymph nodes [15]. On contrast-enhanced CT, generally endometrial cancer is characterized by a lower attenuation than myometrium [28]. CT is not sensitive or specific enough to assess the depth of myometrial invasion or cervical stroma involvement [34] owing to the little contrast difference. For detection of deep myometrial invasion, the sensitivity and specificity are 83 and 42%, respectively [34], with an overall staging accuracy of 58–76% [35]. CT can demonstrate invasion to the adjacent organs, such as bladder and rectum. Distant metastases are most often seen in the extrapelvic lymph nodes and peritoneum. Peritoneal metastases on CT appear as peritoneal thickening, or serosal nodular soft-tissue masses, with ascites.
FDG-PET/CT
FDG-PET/CT is useful in assessing nodal disease and distant metastases. Direct comparison of MRI with FDG-PET/CT has demonstrated no statistically significant difference in the detection of lymph node metastases in patients with endometrial cancer [36]. The added value of FDG-PET/CT may be in the detection of distant metastatic deposits, for which it has been found to have sensitivity of 100% and specificity of 94% [36].
Cervical cancer
Epidemiology, risk factors & diagnosis
Cancer of the uterine cervix is the second most common gynecologic malignancy worldwide. The most common histologic type of cervical carcinoma is squamous cell carcinoma (90%) followed by adenocarcinoma (5–10%). Most cervical squamous cell carcinomas grow at the squamocolumnar junction and are related to human papillomavirus infection. Adenocarcinomas arise within the cervical canal. Imaging plays a limited role in diagnosis; cervical cancer may be detected during screening programs, by Pap smear test or by physical examination. Patients may present with abnormal vaginal discharge and bleeding, especially after intercourse.
Staging & the role of imaging
FIGO staging is the most widely used staging system for cervical carcinoma (Table 3) [37]. There are two main treatment options in cervical cancer: radical surgery including trachelectomy and/or radical hysterectomy in early-stage disease (FIGO stages IA, IB1 and IIA1) or primary radiotherapy with concurrent administration of platinum-based chemotherapy for patients with bulky FIGO stage IB2/IIA2 disease (tumors larger than 4 cm) or locally advanced disease (FIGO stage IIB or greater). FIGO staging based on clinical findings (physical exam) is limited. For example, clinical evaluation of tumor size has a reported accuracy of 60%, underestimating tumors with endophytic component [38,39]. Imaging thus complements clinical assessment for more accurate staging, and provides information about other relevant prognostic factors such as lymph node metastases. The presence of metastatic pelvic lymph nodes does not alter the FIGO staging, but is associated with poorer prognosis. Revised FIGO staging (2009) recommended the incorporation of cross-sectional imaging techniques (MRI/CT) in the evaluation and treatment planning for cervical cancer [37].
The revised FIGO staging (2009) of cervical carcinoma.
CIS: Carcinoma in situ; FIGO: International Federation of Gynecology and Obstetrics.
Reproduced with permission from [13].
US
TV and transrectal US are helpful for primary evaluation of tumor size and locoregional extent, but they have a limited role in staging patients with cervical cancer. When performed by an expert operator, TV US has been found to have high accuracy for the assessment of cervical stroma infiltration in the pretreatment assessment of patients with early stage cervical cancer [40]. The limited soft-tissue contrast and the small field of view may lead to a suboptimal evaluation of parametrial invasion (FIGO stage >IIB). However, visualization of the intact or disrupted echogenic cervical stroma on US, use of color Doppler to distinguish infiltrated pericervical ligaments, and a dynamic examination technique can all be helpful for staging patients with cervical cancer. Complications of local-regional invasion may also be identified, including hydronephrosis or distension of the uterine cavity secondary to tumor obstructing the endocervical canal.
MRI
MRI is the best imaging technique for local staging of cervical carcinoma. The normal cervix demonstrates a trilaminar signal intensity pattern on T2WI: high signal intensity (endocervical glands) surrounded by low signal intensity (cervical stroma) and an external rim of intermediate signal intensity (smooth muscle; Figure 1). MRI can accurately determine tumor location (exophytic or endocervical), tumor size, parametrial, pelvic sidewall or adjacent organ invasion and the presence of nodal enlargement [38,39]. MRI is also useful in the pretreatment evaluation of young women with small volume disease who wish to preserve fertility, in whom a conservative surgical procedure can be performed; this involves resection of the cervix together with 2 cm of the parametrium (radical trachelectomy) and lymphadenectomy [41,42]. MRI is mandatory to determine eligibility for trachelectomy in terms of tumor size (<2 cm), cervical length (>2.5 cm), distance tumor-internal uterine ostium (>1 cm) and presence of deep cervical stromal invasion [42,43].
Stage I
Tumors are confined to the cervix (Table 4). In stage IA, disease is microinvasive and cannot be seen on MRI. Stage IB is defined as clinically visible tumor limited to the cervix and is subdivided into IB1 (<4 cm in greatest dimension) and IB2 (>4 cm in greatest dimension). On T2WI, tumor appears as an intermediate signal intensity mass in contrast to the low signal intensity cervical stroma (Figure 6 & 7) [39]. The use of contrast medium increases the contrast between the tumor and normal cervical stroma and can improve detection and localization, especially useful for small tumors. Cervical cancer demonstrates variable enhancement on dynamic multiphase contrast-enhanced T1WI with small tumors enhancing earlier than adjacent cervical stroma and larger tumors demonstrating a variable degree of enhancement (necrosis). In poorly circumscribed lesions, tumor detection may be aided by DWI. Tumors demonstrate high signal intensity on DWI and low signal intensity on the corresponding ADC map. Naganawa et al. reported a mean ADC value of cervical cancer lesions of 1.09 ± 0.20 × 10−3 mm2/s, versus that of normal cervix tissue of 1.79 ± 0.24 × 10−3 [44].
Key MRI features according to revised FIGO staging of cervical carcinoma.
DWI: Diffusion-weighted imaging; FIGO: International Federation of Gynecology and Obstetrics; SI: Signal intensity; T2WI: T2-weighted image.


Stage II
Stage II is defined as tumor growth beyond the cervix but without extension to the pelvic sidewall or the lower third of vagina (Table 4). In stage IIA, there is invasion of the upper two-thirds of the vagina without parametrial invasion. Segmental disruption of the hypointense vaginal wall is demonstrated on T2WI (Figure 8). Large exophytic polypoid cervical tumor may mimic vaginal infiltration, causing widening of the vaginal wall; in this setting low T2 signal intensity of the vaginal wall remains intact. On MRI, stage IIB disease is seen as full-thickness stromal invasion, defined as disruption of the low signal intensity of the stromal ring on T2WI (Figure 9); a spiculated tumor-to-parametrium interface, T2WI intermediate signal intensity soft tissue extending into the fatty parametria (Figure 9) and encasement of the periuterine vessels are additional signs of stage IIB disease [38]. If the intact low signal intensity cervical stromal rim is greater than 3 mm (hypointense rim sign), parametrial invasion can be excluded with specificity of 96–99% and negative predictive value of 94–100% (Figure 7 & 8) [45–47]. Important pitfalls in evaluation of parametrial invasion are related to postbiopsy hemorrhage and large tumors [39,46,48], which can compress and cause stromal edema, obscuring the real tumor boundary. DWI and ADC map can be useful for accurate delineation of parametrial invasion, distinguishing peritumoral edema from tumoral infiltration.


Stage III
Stage III cervical cancer is defined as tumor extension into the lower third of the vagina and/or pelvic side wall (Table 4). In stage IIIA, there is invasion of the lower third of the vagina without extension to the pelvic sidewall. Tumor extending to the pelvic sidewall or causing hydronephrosis (unilateral or bilateral ureter obstruction), is defined as stage IIIB (Figure 10). Tumor visualized within 3 mm of the obturator internus, levator ani, piriformis muscles or iliac vessels is suggestive of stage IIIB disease [46].
Stage IV
Stage IV indicates adjacent organ invasion and/or distant metastatic disease (Table 4). Disruption of low signal intensity bladder or rectal wall by high signal intensity tissue on T2WI with tumor reaching the mucosal surface constitutes stage IVA (Figure 11). The absence of bladder or rectal invasion can be diagnosed with confidence using MRI (reported negative predictive value = 100%) [49]. Tumor invasion along the bladder internal surface (frequently disrupted) can cause T2WI high signal intensity mucosal thickening, known as bullous edema [47]. Direct rectal invasion is uncommon, as the Pouch of Douglas separates the posterior vaginal fornix from the rectum, making the uterosacral ligaments the preferred route for rectal invasion. In stage IVB, distant metastases are present.

CT
CT is often used for staging advanced cervical carcinoma. CT is able to identify extrauterine spread of disease, including enlarged pelvic and/or retroperitoneal lymph nodes, extension to the pelvic side walls and hydronephrosis, fistulation into bladder or into rectum, and the presence of distant parenchymal metastases. CT has limited ability in local staging owing the poor soft-tissue contrast.
Lymph node assessment in cervical cancer
Lymph node status is not part of the FIGO staging system for cervical cancer; however, it has important prognostic implications. Cervical carcinoma typically spreads to the parametrial lymph nodes first, followed by the obturator nodes, the internal and external iliac lymph node chains and paraortic nodes. Early stages IB and IIA survival rates decrease from 85–90% to 50–55%, respectively, in presence of pelvic nodal metastases [48]. Accuracies in detection of nodal involvement have been reported at 83–90% for CT and 86–90% for MRI [50]. Both modalities rely on size criteria, with a nodal short axis diameter >10 mm considered as pathological. For round nodes, 8 mm is typically used as a cutoff value. This leads to a low sensitivity owing to the inability to identify micrometastasis in normal size lymph nodes [51]. Detection of lymph nodes is increased by using DW-MRI due to the high signal intensity returned from nodes, although correlation with T2WI is always required [33]. Pathological nodes may present focal low signal on T1WI and high signal on T2WI areas owing to internal necrosis.
FDG-PET/CT
PET/CT is useful in staging patients with advanced cervical cancer (Figures 10 & 12). PET/CT is accurate in the detection of lymph node metastases, with sensitivities of 75–100% and specificities of 87–100% [52–55], demonstrating abnormal tracer uptake even in normal size nodes. Reinhardt et al. found that in the detection of pathological nodes, sensitivity, specificity and positive predictive value (PPV) were 91%, 100% and 100%, respectively, for FDG-PET, as compared to 73%, 83% and 67%, respectively, for MRI [3]. FDG-PET also improves staging in advanced disease by demonstrating unexpected distant sites of disease (retroperitoneum, supraclavicular nodal metastases) [56]. Maximum primary tumor standardized uptake value and other quantitative metrics that take into account the tracer uptake of the entire lesion such metabolic tumor volume and total lesion glycolysis [57] are promising biomarkers of treatment response and prognosis for patients with cervical cancer.

Ovarian cancer
Epidemiology, risk factors & diagnosis
Ovarian cancer represents the fifth most common cause of cancer death in the female population [58]. It is the most lethal of all gynecological malignancies in developed countries. More than 70% of patients with ovarian cancer are diagnosed at an advanced tumor stage. The 5-year survival rate for women diagnosed with late-stage disease is less than 20% even with extensive surgery and chemotherapy, compared with up to 90% for women diagnosed with early-stage disease [59]. Epithelial ovarian tumors, representing 60% of all ovarian neoplasms and 85% of malignant ovarian neoplasms, are further grouped into subtypes: serous, mucinous, endometrioid, clear cell, transitional cell tumors (Brenner tumors), carcinosarcoma, mixed epithelial tumor and undifferentiated carcinoma. Epithelial tumors can be benign, borderline or malignant (borderline tumors have been introduced as a subgroup identified by all the features of malignant neoplasms but no stromal invasion).
Risk factors for ovarian cancer include genetic predisposition (e.g., BRCA1 or 2 gene mutations), family history of ovarian cancer, previous cancer diagnosis, nulliparity, postmenopausal status and endometriosis. Clear cell and endometrioid carcinomas are highly associated with endometriosis. Imaging is used to detect and characterize adnexal masses and to stage ovarian cancer.
Staging & the role of imaging
FIGO classification of ovarian cancer is based upon intraoperative findings including histological and cytological assessment (Table 5). The procedures include a comprehensive staging laparotomy with total abdominal hysterectomy, bilateral salpingo-oophorectomy, infracolic omentectomy and lymphadenectomy. Peritoneal cytology and multiple peritoneal biopsies are obtained throughout the pelvis and upper abdomen. Imaging findings are not a formal component of the staging system but they play a significant role in diagnosis and management of patients with suspected ovarian cancer. Imaging is of paramount importance in defining the appropriate management by accurately evaluating the extent of anatomical location of peritoneal spread, which in turn dictates the feasibility of cytoreductive surgery and predicts the likelihood of optimal primary cytoreduction [56,60,61]. Imaging by US and CT is also used to guide ovarian mass/omental biopsy, which is commonly performed in patients where the diagnosis is unclear or prior to neoadjuvant chemotherapy.
FIGO staging of ovarian carcinoma.
FIGO: International Federation of Gynecology and Obstetrics.
Reproduced with permission from [62].
US
US is an excellent modality for identifying ascites, guiding paracentesis as well as omental/peritoneal biopsy. It is clinically useful but has a limited role in staging ovarian cancer owing to a limited field of view of certain portions of the abdomen such as the mesenteric serosal surfaces.
MRI
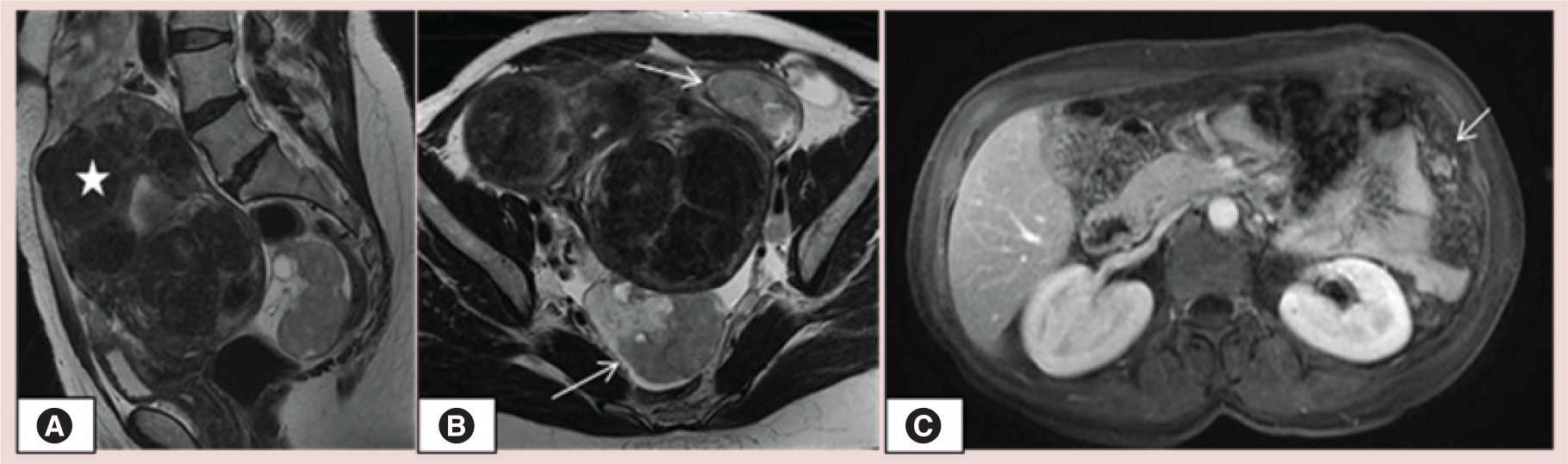
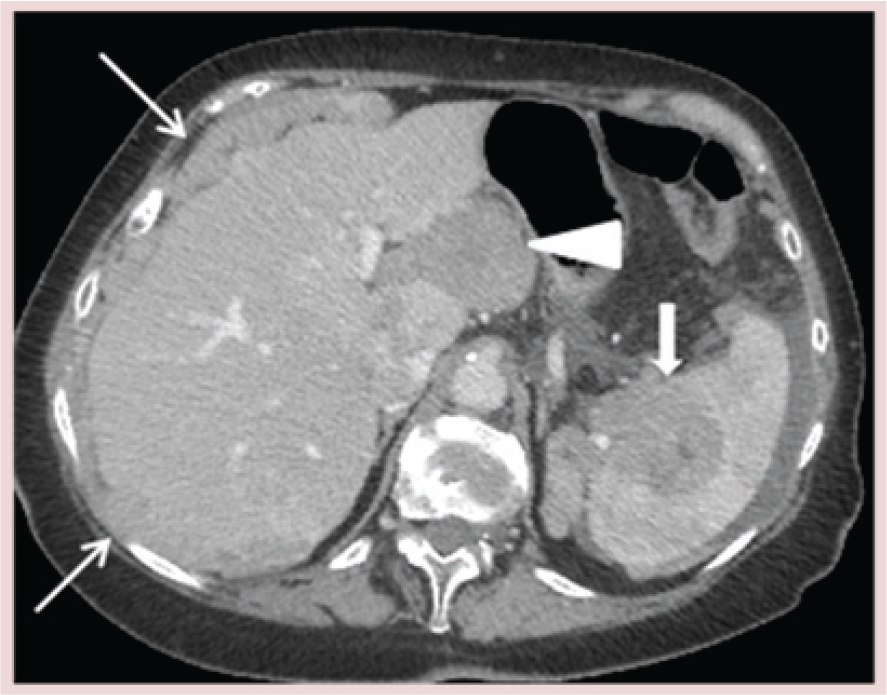
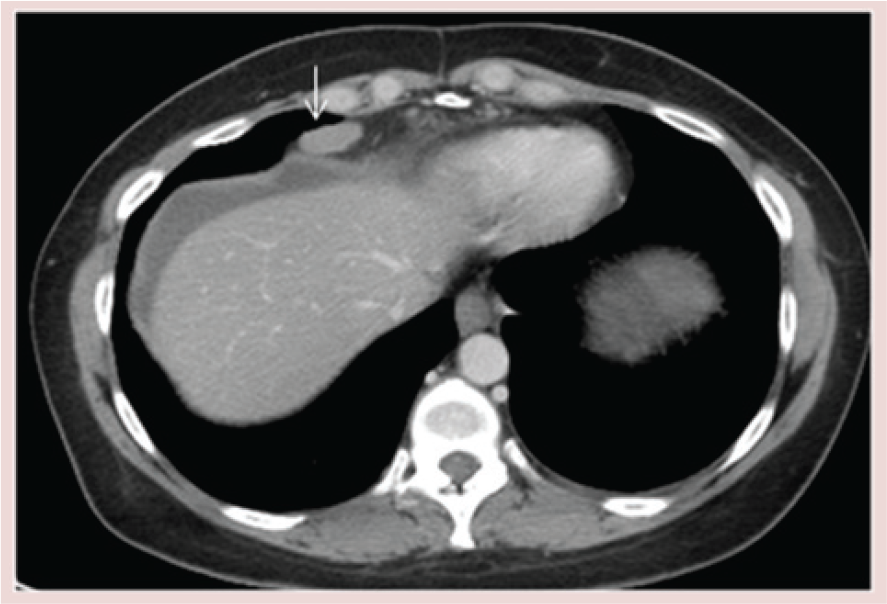
The overall staging accuracy of MRI in patients with ovarian malignancy is 75–78% [63,64]. MRI is recommended as a second-line technique for the staging of ovarian cancer [65] in the pelvis. MRI is best reserved for problem solving and for staging ovarian cancer in patients for whom CT is contraindicated. Multiphase contrast-enhanced MRI has a reported sensitivity of 95% and specificity of 80% for the detection of peritoneal deposits [66]. Contrast enhanced sequences best delineate peritoneal/serosal implants and omental cake (Figure 13). Hepatic capsular implants typically biconvex in shape and indent the liver surface giving it a scalloped appearance. Intraparenchymal hepatic metastases tend to be completely surrounded by liver parechymas and are often ill-defined and circular in shape. Fujii et al. showed that DW-MRI is highly sensitive (90%) and specific (96%) in delineating the extent of peritoneal dissemination. The omental cake and peritoneal deposits retain high signal intensity (Figure 14) [67]. The combination of DW-MRI and gadolinium-enhanced MRI has been reported to improve the accuracy of tumor detection (accuracy of 84–88% compared to 52–72% for gadolinium-enhanced MRI alone and 71–81% for DW-MRI alone) [68].

CT
CT is the primary cross-sectional imaging modality used to stage ovarian cancer. Optimal cytoreductive surgery (residual disease <1 cm) is a strong predictor of survival [69]. Accurate imaging guides the surgeon to areas of disease that may be difficult to identify surgically and describing the volume and extent of disease likely to be optimal resectable disease. Relative criteria for non-optimally resectable disease have been developed [70]. They include lymph node enlargement above the renal hilum, presence of abdominal wall invasion, parenchymal liver metastases, peritoneal implants of >2 cm along the diaphragm, lesser sac, porta hepatis, intersegmental fissure, gall bladder fossa, gastrosplenic, gastrohepatic ligament and root small bowel mesentery. Ascites on CT is easily identified; presence of ascites on CT has a PPV of 72–80% for the presence of peritoneal metastases [71].
Stage I
Stage I ovarian cancer is limited to either one (stage IA) or both (stage IB) ovaries (Table 6); no tumor is present on the ovarian surface and no malignant cells in the ascites or peritoneal washings. In stage IC the tumor is still limited to one or both ovaries but there is a capsular rupture, tumor is present on the ovarian surface, and/or malignant cells are present in the ascites or peritoneal washings (Figure 15).
Key computed tomography imaging features according to FIGO staging of ovarian carcinoma.
CT: Computed tomography; FIGO: International Federation of Gynecology and Obstetrics.

Stage II
Stage II disease is characterized by local extension of tumor confined to the pelvis but with no upper abdominal involvement (Table 6). In stage IIA disease there is extension and/or tumor implants are found in the uterus or fallopian tube(s), but there are no malignant cells in the ascites or peritoneal washings. Stage IIB disease is characterized by extension into and/or implants on other pelvic tissues, with no malignant cells in the ascites or peritoneal washings. On CT, irregularity or obliteration of the fat plane between the uterus and the ovarian mass is indicative of stage IIA disease. Loss of the normal fat plane around the rectum or bladder, less than 3 mm between the tumor and the pelvic sidewall, and/or displacement or encasement of the iliac vessels indicates stage IIB disease (Figure 16) [64].

Stage III
Stage III disease is defined as the presence of extrapelvic peritoneal and/or lymph node metastasis (Table 6). Microscopic extrapelvic peritoneal implants are stage IIIA disease and are not detectable with CT. Stage IIIB, extrapelvic peritoneal implants less than 2 cm and stage IIIC extrapelvic peritoneal implants larger than 2 cm or lymph node metastasis can easily be detected with CT. Approximately 70% of patients have peritoneal metastases at staging laparotomy [72]. CT detection of peritoneal implants depends on several factors including location, presence or absence of surrounding ascites and size. Peritoneal fluid flows from the Pouch of Douglas, along the paracolic gutters to the diaphragm. There is preferential flow along the right paracolic gutter [73]. Thus, the three sites most commonly involved are the right subphrenic space, the greater omentum and the pouch of Douglas [72], and these should be especially scrutinized on CT (Figure 17). CT has a sensitivity of 14–27% for detection of peritoneal implants smaller than 1 cm, especially in the absence of ascites [74,75]. However, the use of coronal and sagittal reformatted images improves sensitivity and allows for better detection of smaller lesions [76]. Omental metastases are characterized as stranding or soft tissue nodules embedded in omental fat or the replacement of the omental fat with thick, nodular tumor (omental cake) along the greater curvature of the stomach, in the gastrosplenic ligament, or anterior to the transverse colon and small bowel in the lower abdomen (Figure 17) [77]. The sensitivity of CT for detection of omental metastasis is reported to be 80–86% [75]. Primary tumor and the metastatic peritoneal deposits can contain microcalcifications; in serous tumors these are known as psammoma bodies, and in mucinous tumors they are known as nonpsammoma calcifications. Both types of tumor calcification can be seen on CT. Mesenteric metastases appear as either round or ill-defined soft tissue masses (Figure 17) surrounded by small-bowel loops and mesenteric fat, or as thickened leaves of the mesentery caused by tumor coating the peritoneal surfaces [78]. Peritoneal metastasis implanted on the liver surface (capsular liver deposits) is the most common type of liver involvement in ovarian cancer. Capsular implants are seen as well-defined, biconvex and peripheral soft-tissue nodules studded along the peritoneal surface of the liver (Figure 18). Sometimes a peritoneal metastasis on the liver or spleen surface can invade into the parenchyma (subcapsular deposits; Figures 14 & 18) [79]. Subcapsular liver deposits cause scalloping of the liver surface with an irregular, enhancing interface between the deposit and the liver parenchyma. Less commonly, direct intrahepatic metastasis can occur by hematogenous dissemination. Intraparenchymal liver lesions are usually less well-defined and circular, and partially or completely surrounded by liver tissue [79]. Tumor extending into the falciform ligament (stage III; Figure 19) can also be mistaken for intraparenchymal disease on axial images, and multiplanar reformatted images can be helpful. Distinction between these different types of liver metastases is important for the selection of an appropriate treatment approach. Subcapsular metastases without parenchymal invasion can be resected directly. However, surgical removal of subcapsular metastases with parenchymal invasion requires liver resection. Information obtained from CT about liver involvement is very useful to the gynecologic surgeon. The presence of multiple perihepatic metastases with parenchymal invasion in multiple regions of both lobes of the liver may preclude surgical resection.
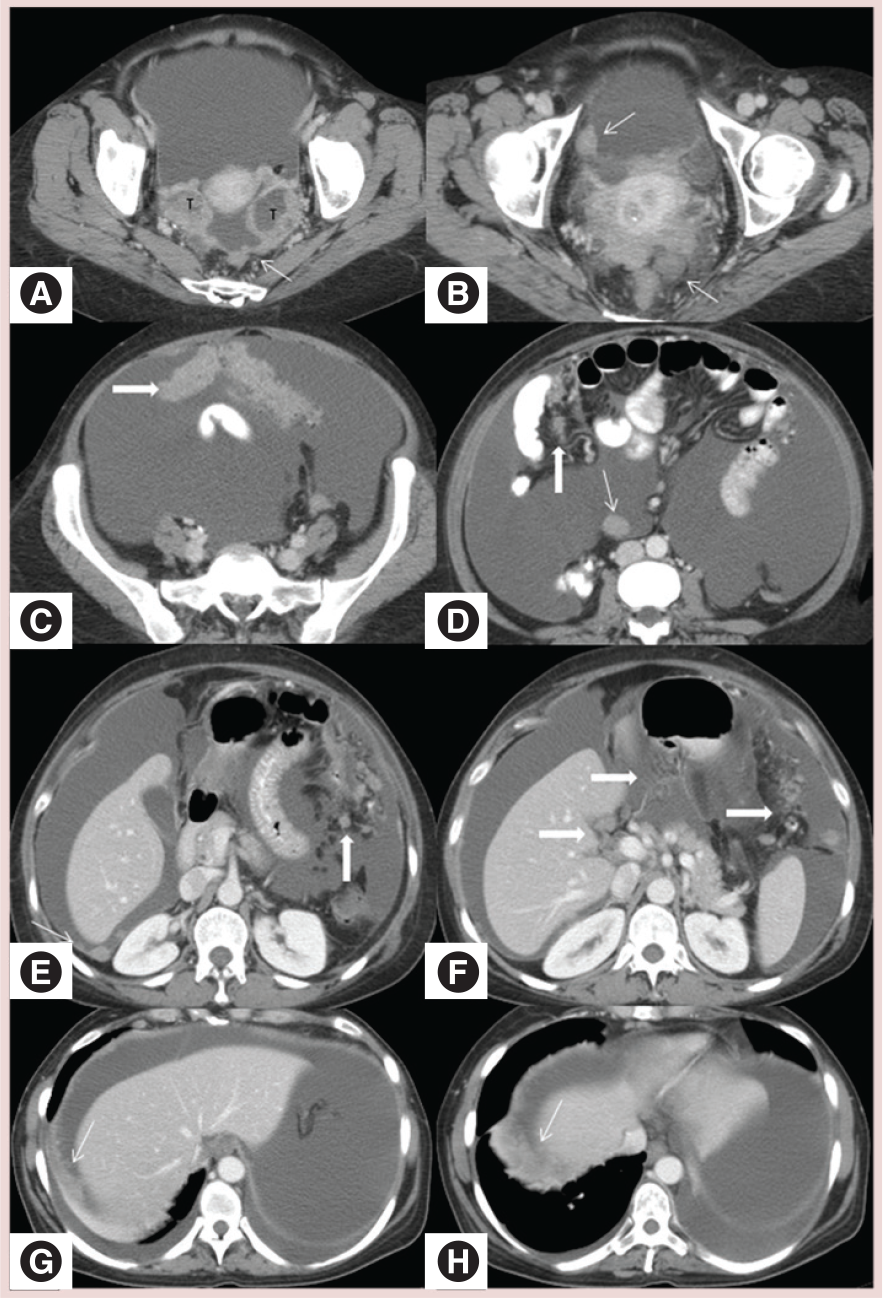

Ovarian cancer can also metastasize through the lymphatic system. Lymph node involvement follows the ovarian veins to the para-aortic and aortocaval nodes at the level of the renal hilum; these are the most common sites for metastatic lymphadenopathy. In general, lymph nodes are defined as enlarged if the short axis diameter is >1 cm; pericardiophrenic nodes are an exception, as they are considered suspicious if greater than 5 mm (Figures 17 & 20). Lymph vessels also pass through the broad ligament and involve the external iliac, hypogastric and obturator nodes. Lymph nodes above the renal hilum and those in the inguinal region represent stage IV disease.
Stage IV
Stage IV disease is defined by distant metastasis beyond the peritoneal cavity, and it occurs via hematogenous spread. Hematogenous metastases are uncommon at the time of diagnosis, but may occur in the solid abdominal organs such as the liver, spleen, kidneys, adrenals, brain and bone. The sensitivity of CT for the detection of extrapelvic disease is approximately 95–100% for liver involvement and 50–60% for nodal involvement [75].
FDG-PET/CT
There is growing evidence that FDG-PET/CT may play a role in preoperative staging of patients with advanced ovarian cancer. FDG-PET/CT has a sensitivity ranging from 62–100% and improves overall diagnostic accuracy compared to CT alone [80,81] because of its ability to characterize metastatic lymph nodes, serosal infiltration along bowel loops and distant metastasis. Lesions <4–6 mm can be difficult to detect owing to the spatial resolution of the gamma camera. A potential source of false-negative findings is mucinous tumor, which is associated with less FDG uptake.
Conclusion
US, CT, MRI and FDG-PET/CT play important roles in the assessment of patients with common gynecological cancers, from the detection to the evaluation of the extent of the disease. Knowledge of the indication for imaging and the modalities used is crucial for pretreatment risk stratification, staging and treatment planning.
Future perspective
The role of the radiologist has become an essential part of the multidisciplinary treatment planning team for patients with gynecologic malignancies. CT and MRI imaging techniques have become an essential tool in guiding presurgical treatment planning, in tailoring treatment options and in pretreatment risk stratification in women with uterine, cervix or ovarian cancer. Imaging techniques providing insights into molecular processes in the tumor microenvironment, such as DW-MRI and PET/CT, are gaining importance in the pretreatment assessment of gynecological malignancies, and their use is likely to expand in the near future.
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Executive summary
In patients with endometrial carcinoma, MRI provides added value as a local staging tool to accurately assess the depth of myometrial invasion and cervical stromal invasion, which correlate with likelihood of lymph node metastases and overall patient survival; in combination with tumor histology and grade, MRI aids the patient's preoperative risk stratification and guides presurgical treatment planning.
MRI plays a paramount role in assessing eligibility for fertility-sparing surgical and medical procedures.
Computed tomography (CT) is used to identify peritoneal disease in serous papillary and clear cell carcinoma of the endometrium, for evaluation of distant metastasis and lymphadenopathy.
MRI is the imaging modality of choice for evaluating tumor location, size and invasion of adjacent structures including the parametria, pelvic side wall and pelvic organs.
The high negative predictive value (94%) for excluding parametrial invasion makes MRI a useful tool for selecting patients who should be treated with surgery.
MRI plays a central role in determining eligibility for fertility-sparing approaches for treatment of cervical cancer (e.g., radical trachelectomy).
[18F]-fluoro-2-deoxy-D-glucose PET is accurate in the detection of lymph node metastases, with a sensitivity of 75–100% and a specificity of 87–100%, demonstrating abnormal tracer uptake even in normal size nodes.
CT is the primary cross-sectional imaging modality used to stage ovarian cancer; the extent and anatomical location of peritoneal spread play a crucial role in the choice between cytoreductive primary surgery versus neoadjuvant chemotherapy.
Diffusion-weighted MRI may play a role in mapping of the extent of the peritoneal disease.
MRI is used as a problem-solving technique and represents the modality of choice for characterization of adnexal lesions.