
Abstract
Background:
Technology-based health interventions present innovative and scalable approaches to enhance cancer care. These interventions have potential to support psychosocial well-being, which is often challenged following a cancer diagnosis and throughout survivorship. Such innovations also enable nurses to extend psychosocial support beyond traditional clinical settings and align with health policy efforts to integrate digital supportive care into routine oncology services.
Aims:
To evaluate the effectiveness of technology-based psychosocial education interventions for cancer patients.
Methods:
Six databases (CINAHL, Cochrane Library, Embase, Medline [Ovid], PubMed and Web of Science) were searched from inception to 29 April 2025. The Cochrane Risk-of-Bias Tool (RoB 2) was used to assess the methodological quality of included studies. Standardised mean differences (SMDs) were calculated to synthesise outcomes measured using varied tools.
Results:
Fourteen studies met the inclusion criteria, including 1509 participants. Technology-based psychosocial education interventions significantly reduced fear of cancer recurrence (SMD = −0.21; 95% CI: −0.42 to −0.01; I² = 4.7%; p = 0.04). Non-significant pooled estimates were observed for reduced psychological distress (SMD = −0.23; 95% CI: −0.61 to 0.15; I² = 76.1%; p = 0.23) and improved quality of life (SMD = 0.21; 95% CI: −0.02 to 0.45; I² = 20.0%; p = 0.08).
Conclusion:
Technology-based psychosocial education interventions show promise in reducing fear of cancer recurrence and may support broader psychosocial outcomes. These interventions are scalable and suitable for diverse clinical settings, supporting nurse-led psychosocial education, remote patient follow-up and the integration of digital supportive care within oncology service delivery.
Introduction
Cancer remains one of the most pressing global health challenges. It is a leading cause of death worldwide and significantly contributes to reduced life expectancy across various countries (Bray et al., 2021). An estimated 20 million new cancer cases and 10 million cancer-related deaths occur annually. Alarmingly, the number of new cancer cases is projected to rise significantly by 2050 (Bray et al., 2024; Ferlay et al., 2021). According to Global Cancer Observatory (GLOBOCAN), the global incidence and mortality of 36 different cancers have been estimated across 185 countries (Obafemi and Umahi-Ottah, 2023). Cancer patients often face a range of challenges that stem not only from the disease itself but also from the side effects of treatments. These challenges may be physical, emotional, interpersonal, existential or spiritual and can persist in both the short and long term (Benedict et al., 2022). A cancer diagnosis can profoundly disrupt every aspect of a person’s life past, present and future as they undergo ongoing therapy, treatment and recovery (Grassi et al., 2017). Consequently, both the physical and psychosocial well-being of individuals are significantly affected by the disease and its treatments (Cigdem and Zeynep, 2017).
Given the rising incidence of cancer and its profound impact on patients’ lives, there is a pressing need to implement more effective, innovative and supportive health management strategies (Marthick et al., 2021). In response to this need, technology-based health interventions offer promising avenues for enhancing clinical care and advancing research (Sharma et al., 2018). Technologies such as internet-based applications, digital games, virtual reality and robotics have increasingly been used in cancer prevention, treatment and health maintenance (Kip et al., 2021). Technology-based psychosocial education represents a targeted strategy that uses digital tools such as websites, mobile apps or video counselling to deliver mental health support, skill building, health education, psychosocial support and the strengthening of self-care (Arpaci et al., 2023; Koyu and Kilicarslan, 2025). By increasing accessibility and reducing geographical and logistical barriers, these interventions can extend psychosocial services to patients who may otherwise face limited access to supportive care (Koyu and Kilicarslan, 2025; Simon et al., 2023). Within nursing practice, such digital approaches can support the delivery of person-centred psychosocial care by enabling nurses to provide education, ongoing support and self-management guidance beyond traditional clinical encounters. Furthermore, integrating technology-based psychosocial education into routine oncology practice may enhance patient engagement, promote adaptive coping strategies and ultimately improve overall quality of life (Bergerot et al., 2024; Penedo et al., 2020).
Recent review studies have focused on the effectiveness of technology-based psychosocial interventions for cancer patients. These interventions have shown significant potential in reducing anger, anxiety and depression, particularly in paediatric oncology populations (Ozturk and Toruner, 2022). Telemedicine, in particular, has emerged as a valuable tool in oncology care, with promising outcomes related to quality of life, anxiety, depression and overall distress (Caminiti et al., 2023). In addition, technology-assisted interventions have been found effective for childhood, adolescent and young adult cancer survivors, positively influencing various domains of survivorship (Zhang et al., 2022). Psychological interventions delivered through digital platforms may also alleviate symptoms such as anxiety, depression, sleep disturbances and fatigue, ultimately enhancing quality of life among survivors (Dong et al., 2025). However, findings on mobile health or ‘mHealth’-based psychosocial interventions for breast cancer patient-caregiver dyads remain inconclusive (Benedict et al., 2022).
Although several systematic reviews have explored the impact of technology on the psychosocial well-being of children, adolescents and cancer survivors, research focusing on adult cancer patients remains limited. Moreover, although psychological distress is a critical component of psychosocial well-being, existing literature has largely examined discrete psychological outcomes, such as anxiety and depression, in isolation rather than within a broader psychosocial framework (Roy et al., 2025; Schneiderman et al., 2005). Although important, psychological symptoms represent only one dimension of the cancer experience (Zucca et al., 2012). Psychosocial well-being is inherently multidimensional, encompassing emotional distress, interpersonal relationships, social and role functioning, family dynamics, existential concerns and fear of cancer recurrence, all of which interact to shape overall adjustment and quality of life (Eiroa-Orosa, 2020; Wang and Feng, 2022). A narrow focus on isolated psychological symptoms may therefore underestimate the complexity and cumulative burden of cancer-related challenges. Accordingly, the primary aim of this study was to conduct a meta-analysis of randomised controlled trials to quantify the effectiveness of technology-based psychosocial interventions for individuals diagnosed with cancer. A systematic search and screening process was first undertaken to identify eligible studies, followed by a meta-analytic synthesis of intervention effects. Specifically, this study examined the impact of digital psychosocial interventions across three key domains of psychosocial well-being: fear of cancer recurrence, psychological distress, and quality of life. By synthesising quantitative evidence across these domains, this study provides a clearer understanding of the effectiveness of technology-based psychosocial education interventions and their potential implications for nursing practice and digital supportive care in oncology.
Methods
This systematic review was conducted in accordance with the preferred reporting items for systematic reviews and meta-analyses (PRISMA) 2020 guidelines (Page et al., 2021), see Supplemental Material 1 – PRISMA 2020 Checklist. The study protocol was registered with PROSPERO under the registration number: CRD420251035256.
Literature search for identification of studies
A comprehensive search was performed across six major databases: CINAHL Plus with Full Text, Cochrane Library, Embase, Medline (Ovid), PubMed and Web of Science. The search spanned from each database’s inception up to 29 April 2025. Assistance from a professional librarian ensured the robustness of the search strategy. Search terms were developed using Medical Subject Headings (MeSHs) from CINAHL and PubMed, as well as manually identified keywords from relevant systematic reviews (Low et al., 2024; Ozturk and Toruner, 2022; Zhang et al., 2024b). Key terms included: cancer patients, oncology patients, patients with cancer, malignancy, neoplasm, tumour, carcinoma; and various technology-related terms: mobile phone, smartphone, online, internet, web-based, mHealth, telehealth, mobile application, virtual reality. Additionally, psychosocial and therapeutic intervention terms were included: psychosocial support, psychoeducation, cognitive-behavioural therapy, counselling, mindfulness and acceptance and commitment therapy. Study design-related terms included randomised controlled trial, RCT, randomised control trial and randomisation. To enhance the search coverage, grey literature and reference lists from selected papers were also manually screened after the initial database screening and during the final selection of eligible studies to identify any additional relevant publications. Full details of the search strategy are provided in Supplemental Material 2 – PICO Worksheet and Search Strategy Protocol.
Eligibility criteria
This review focused exclusively on randomised controlled trials involving individuals diagnosed with cancer, regardless of cancer type, stage, age or gender. Studies were eligible irrespective of treatment phase, including patients undergoing active treatment, post-treatment survivorship or long-term follow-up, provided they were not exclusively receiving end-of-life or palliative-only care. Eligible studies examined digital or technology-based interventions, such as internet-based tools, telephone or mobile phone communication, video conferencing, web-based platforms and other forms of digital health technologies. These interventions were compared against control groups that either received standard care or a distinctly different intervention. Studies were excluded if they were review papers, trial protocols or if the full text was not available. Studies were omitted if they did not provide adequate data to calculate pre- and post-intervention means and standard deviations (SDs) for both intervention and control groups.
Study selection
All search results were imported into EndNote 21 for reference management. Duplicate records were removed using the software’s built-in tool. A total of 1883 records were initially identified through searches across the six selected databases. Following the removal of duplicates using EndNote 21, 1310 unique papers remained for title and abstract screening. Two authors independently screened the titles and abstracts to identify potentially relevant studies. Of these, 1272 records were excluded at the title and abstract screening stage for the following reasons: the population did not involve patients with cancer (n = 662); the intervention did not involve technology-based psychosocial education (n = 563); or the study design was not a randomised controlled trial (e.g. review, qualitative study, protocol or observational study; n = 47). Full-text papers of the remaining 38 records were retrieved and assessed independently by the same two reviewers. Twenty-seven studies were excluded after full-text assessment for the following reasons: the population did not involve patients with cancer (n = 5), the intervention did not involve technology-based psychosocial education (n = 14), the study design was not a randomised controlled trial (n = 5) or insufficient data were provided to calculate pre- and post-intervention means and SDs for both intervention and control groups (n = 3). Any disagreements during the selection process were resolved through discussion, with the involvement of a third reviewer when necessary to reach consensus. Ultimately, 11 eligible studies were identified through database searches. An additional three relevant studies were located through manual searches, including Google Scholar and reference lists of related reviews. This resulted in a final sample of 14 studies included in the meta-analysis. A detailed summary of the selection process is illustrated in Figure 1. PRISMA flow diagram of study selection and the characteristics of the included studies are summarised in Table 1.
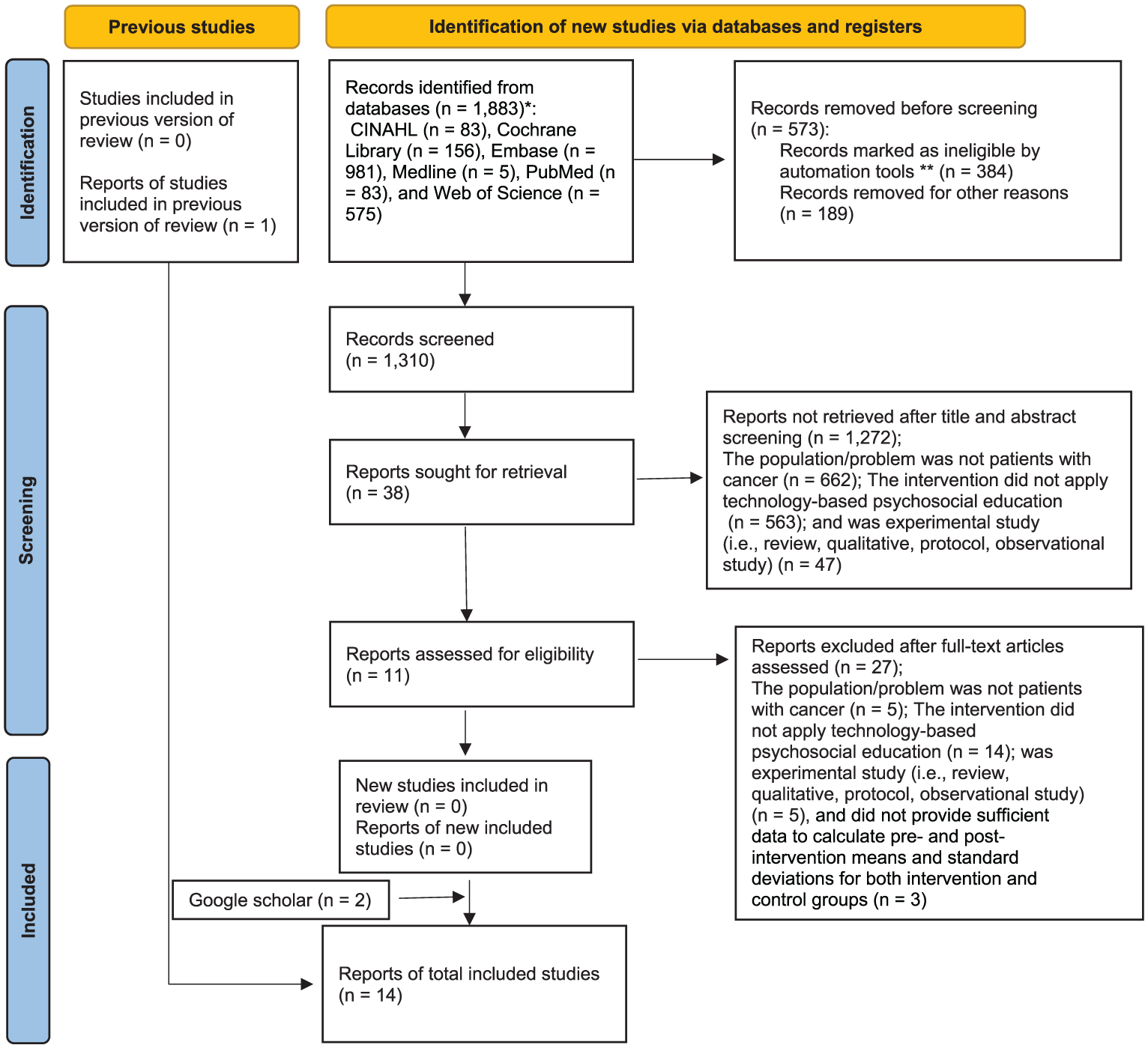
PRISMA flowchart diagram.
Summary of included studies
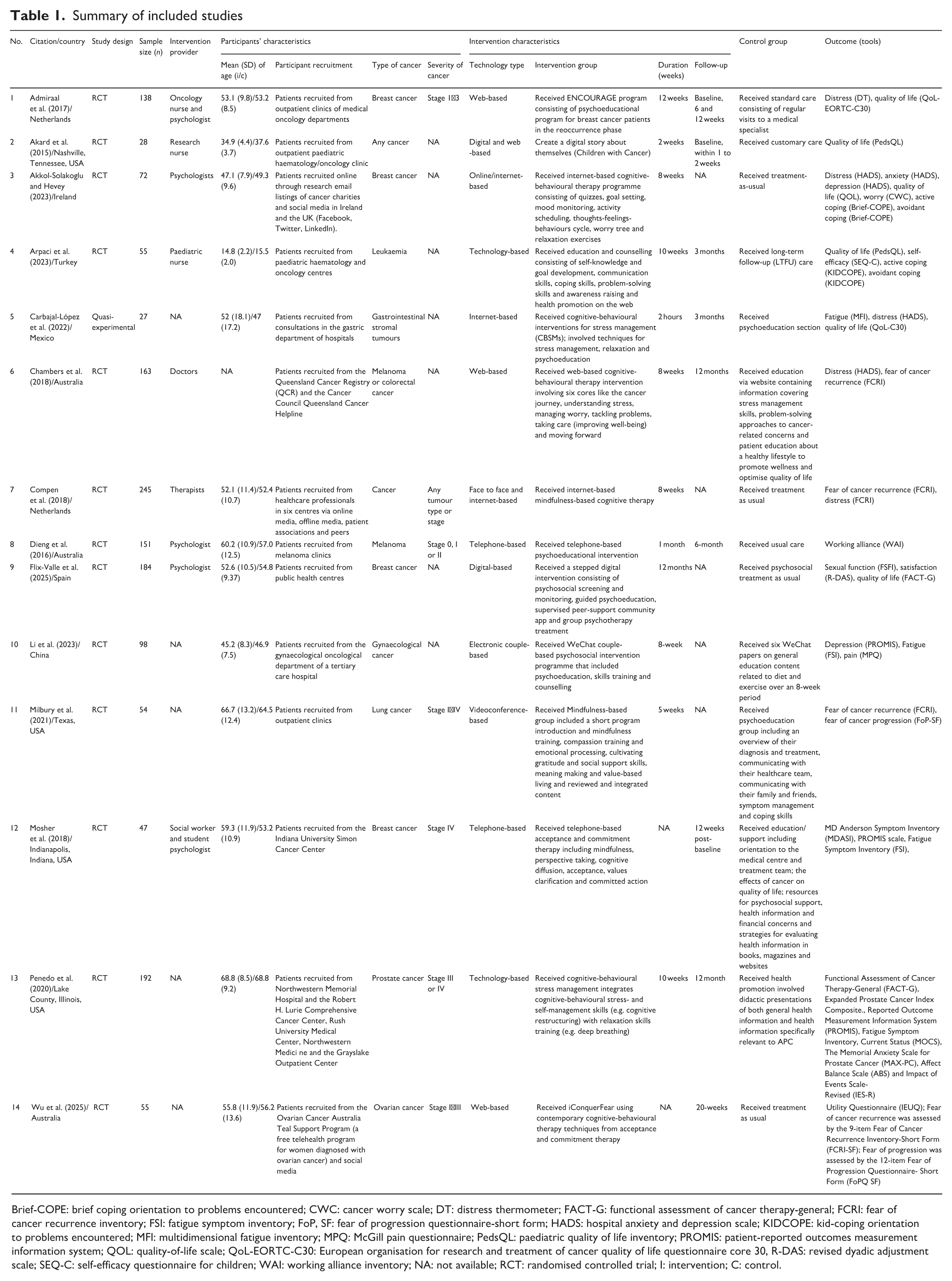
Brief-COPE: brief coping orientation to problems encountered; CWC: cancer worry scale; DT: distress thermometer; FACT-G: functional assessment of cancer therapy-general; FCRI: fear of cancer recurrence inventory; FSI: fatigue symptom inventory; FoP, SF: fear of progression questionnaire-short form; HADS: hospital anxiety and depression scale; KIDCOPE: kid-coping orientation to problems encountered; MFI: multidimensional fatigue inventory; MPQ: McGill pain questionnaire; PedsQL: paediatric quality of life inventory; PROMIS: patient-reported outcomes measurement information system; QOL: quality-of-life scale; QoL-EORTC-C30: European organisation for research and treatment of cancer quality of life questionnaire core 30, R-DAS: revised dyadic adjustment scale; SEQ-C: self-efficacy questionnaire for children; WAI: working alliance inventory; NA: not available; RCT: randomised controlled trial; I: intervention; C: control.
Data extraction
Data extraction from the included studies was conducted by the first author and subsequently verified by the second author to ensure accuracy. Extracted information included the study citation, country of origin, study design, sample sizes of both intervention and control groups, details about the intervention provider and statistical data including the mean and Standard Deviation (SD) for each group. Additional data collected included participants’ living environments, cancer characteristics (e.g. type and severity), the technology used, the nature of the intervention provided in both groups, the intervention dosage (including frequency, duration and follow-up) and the outcome measures employed.
Quality assessment
The quality of the included studies was independently assessed by two authors using the Risk of Bias 2 (RoB 2) tool, as recommended by Cochrane (Sterne et al., 2019). This tool evaluates five key domains: the randomisation process, deviations from intended interventions, missing outcome data, measurement of the outcome and selection of the reported results. Each domain was rated as having a low, unclear or high risk of bias. Any discrepancies in the quality assessment were discussed between the two reviewers, and when consensus could not be reached, a third reviewer was consulted to resolve the disagreement.
Statistical analysis
The meta-analysis was conducted using Stata 17 (StataCorp, 2021). To standardise effect sizes across studies employing various measurement tools, we calculated standardised mean differences (SMDs; Borenstein et al., 2021; Hopkins and Rowlands, 2024). For each study, we extracted the mean and SD at both baseline and post-intervention for both intervention and control groups. Given the anticipated variability among study results, a random-effects model was applied using the DerSimonian–Laird method to estimate pooled SMDs with 95% confidence intervals (CIs) for outcomes including fear of cancer recurrence, psychological distress and quality of life (DerSimonian and Laird, 2015). Statistical heterogeneity was assessed using the I² statistic, with values exceeding 50% indicating substantial heterogeneity (Higgins and Thompson, 2002). To evaluate the potential impact of publication bias, we employed Egger’s regression test (Egger et al., 1997; Sterne and Egger, 2005). Sensitivity analyses were performed using the leave-one-out method to assess the robustness of the pooled SMDs by sequentially excluding each study to determine its influence on the overall effect size.
Results
Study characteristics
The included studies were published between 2015 and 2025 and involved a total of 1509 cancer patients. Participant ages ranged from a mean of 14.8 years (SD = 2.2) to 68.8 years (SD = 9.2). The populations studied included individuals diagnosed with various types of cancer, including breast cancer, leukaemia, gastrointestinal stromal tumours, colorectal cancer, melanoma, gynaecological cancers, lung cancer and prostate cancer. Disease stages among participants spanned from stage I to stage IV (stages I–IV describe cancer progression from localized [Stage I], to larger or locally spread [II], to lymph node involvement [III], and finally distant metastasis [IV]. Participants were primarily recruited from outpatient oncology clinics, cancer centres, public health settings or community/online platforms. The digital psychosocial interventions varied across studies but included digital storytelling for paediatric patients, educational and counselling services, cognitive-behavioural strategies for stress management, mindfulness-based approaches and acceptance and commitment therapy. These interventions were delivered using a range of technologies, including web platforms, internet-based applications, video conferencing and telephone support. Control groups received standard care or non-digital psychosocial interventions. Intervention frequency was typically once per week. Follow-up periods extended from baseline assessments to up to 12 months post-intervention. A comprehensive summary of the intervention characteristics and participant demographics is provided in Table 1.
Effects of technology-based psychosocial education for cancer patients
Fear of cancer recurrence
Four studies were included in the analysis examining the impact of digital psychosocial interventions on fear of cancer recurrence (Akkol-Solakoglu and Hevey, 2023; Compen et al., 2018; Dieng et al., 2016; Wu et al., 2025). The pooled SMD was −0.21 (95% CI: −0.42 to −0.01; I² = 4.7%, p = 0.04), as shown in Figure 2(a). These results suggest a statistically significant reduction in fear of recurrence among patients receiving digital interventions compared to those receiving standard care or conventional psychosocial support.
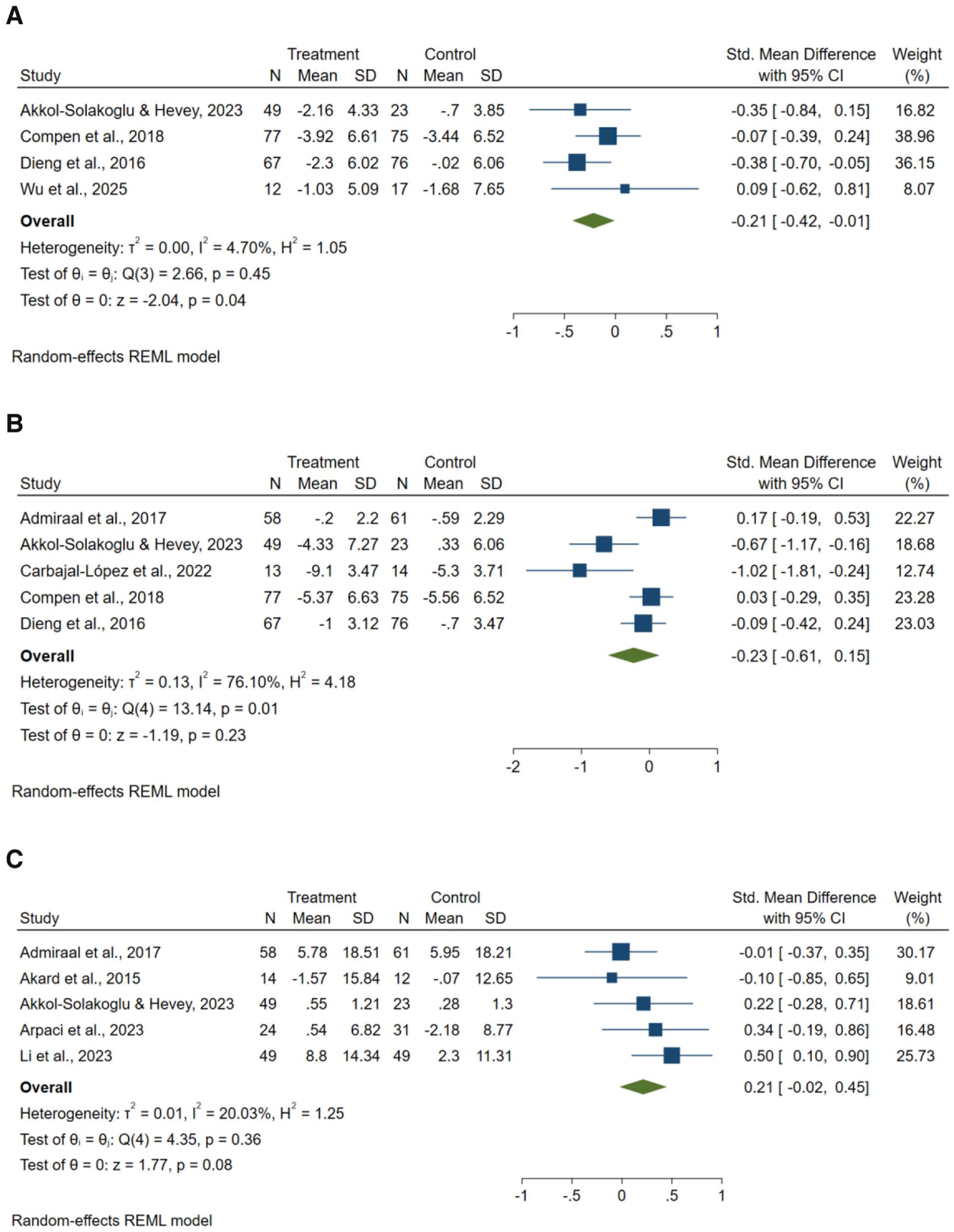
Forest plot of technology-based psychosocial education for cancer patients: (a) fear of cancer recurrence; (b) psychological distress and (c) quality of life.
Psychological distress
Five studies assessed the effect of digital psychosocial interventions on psychological distress (Admiraal et al., 2017; Akkol-Solakoglu and Hevey, 2023; Carbajal-López et al., 2022; Compen et al., 2018; Dieng et al., 2016). The combined SMD was −0.23 (95% CI: −0.61 to 0.15; I² = 76.1%, p = 0.23), as illustrated in Figure 2(b), indicating no statistically significant effect. However, substantial heterogeneity was observed across studies. Given the limited number of included trials, formal subgroup analysis or meta-regression was not feasible. The variability in effect estimates may reflect differences in cancer type, intervention modality (e.g. web-based, telephone-based, mindfulness-based) and intervention duration. Therefore, this pooled estimate should be interpreted with caution.
Quality of life
Another five studies were analysed to determine the effect of digital psychosocial interventions on quality of life among cancer patients (Admiraal et al., 2017; Akkol-Solakoglu and Hevey, 2023; Arpaci et al., 2023; Li et al., 2023). The pooled SMD was 0.21 (95% CI: −0.02 to 0.45; I² = 20.03%, p = 0.08), presented in Figure 2(c). Although the results suggested a potential positive trend, the improvement was not statistically significant compared to standard care or non-digital psychosocial interventions.
Sensitivity analysis
To assess the robustness of the meta-analysis findings, a sensitivity analysis was conducted using the leave-one-out method. This approach involved systematically removing the study contributing the greatest statistical weight in each pooled analysis. The results showed that excluding these studies did not meaningfully alter the overall effect sizes. Specifically, the pooled SMD remained stable for fear of cancer recurrence (p = 0.58), psychological distress (p = 0.76) and quality of life (p = 0.54), suggesting that the meta-analytic conclusions were not unduly influenced by any single study.
Risk of bias assessment
The methodological quality of the included studies was evaluated using the Cochrane RoB-2 tool. None of the studies were rated as having a high risk of bias in any of the assessed domains (see Supplemental Material 3). However, some domains raised moderate concerns due to limitations in the randomisation process, unclear allocation concealment and insufficient blinding of participants, interventionists or outcome assessors. These methodological limitations should be considered when interpreting the findings, as they may have introduced performance or detection bias and potentially influenced the magnitude of reported intervention effects. Nevertheless, the overall absence of high risk of bias strengthens confidence in the general direction of the observed outcomes.
Publication bias
Publication bias was assessed using Egger’s regression test. The results did not indicate significant publication bias for fear of cancer recurrence (p = 0.69) or quality of life (p = 0.74). For psychological distress, the Egger’s test approached statistical significance (p = 0.05), suggesting the possibility of small-study effects. However, given the limited number of included studies, these findings should be interpreted with caution.
Discussion
Overview of main findings
This systematic review and meta-analysis explored the effectiveness of technology-based psychosocial interventions in reducing fear of cancer recurrence, alleviating psychological distress and enhancing quality of life among cancer patients. Overall, the findings indicate that digital psychosocial interventions demonstrate meaningful potential in oncology care, although their effects appear outcome-specific and shaped by clinical and methodological context. The findings provide promising, although not uniform, support for the use of digital psychosocial strategies in oncology care (Dong et al., 2025; Zhang et al., 2024a).
Effects on fear of cancer recurrence
Among the most consistent outcomes in the present meta-analysis was a statistically significant reduction in fear of cancer recurrence among participants receiving technology-based psychosocial education interventions. Consistent with findings from the broader oncology literature, this psychological burden is among the most commonly reported and distressing concerns among cancer survivors, associated with persistent anxiety and impaired quality of life (Mertens, 2019; Tauber et al., 2023). Interventions incorporating mindfulness, psychoeducation and cognitive-behavioural therapy appeared effective in addressing this concern by improving emotional regulation and reducing intrusive thoughts (Compen et al., 2018; Dieng et al., 2016). These findings align with broader evidence suggesting that digital delivery methods can enhance psychological outcomes by providing structured, accessible and scalable support mechanisms. For example, a meta-analysis of randomised controlled trials examining technology-based psychosocial interventions among children, adolescents and young adults with cancer similarly reported improvements in psychological outcomes, supporting the potential effectiveness of digitally delivered psychosocial support across different cancer populations (Ozturk and Toruner, 2022). Given that fear of recurrence is largely cognitively mediated, structured digital programmes grounded in cognitive-behavioural and mindfulness-based frameworks may be particularly well-suited to target this construct through repeated skill reinforcement and guided cognitive restructuring.
Effects on psychological distress
However, the impact of technology-based psychosocial interventions on psychological distress was less conclusive. Although several trials reported individual benefits, the overall pooled analysis showed no statistically significant reduction in distress when compared to control conditions (Admiraal et al., 2017; Carbajal-López et al., 2022). This discrepancy may be attributed to variations in intervention length, delivery format and patient engagement, which can influence intervention effectiveness. For example, a randomised controlled trial of web-delivered cognitive-behavioural therapy for distressed cancer patients demonstrated improvements in psychological outcomes, but intervention engagement and delivery characteristics influenced treatment effects (Chambers et al., 2018). Additionally, psychological distress is a multifactorial construct influenced by prior mental health conditions, disease severity, social support and cultural context, complicating efforts to achieve consistent outcomes (Arpaci et al., 2023; Fu et al., 2017). Several contextual factors may further explain the observed variability. The included studies differed substantially in technology modality, including web-based platforms (Admiraal et al., 2017; Chambers et al., 2018; Wu et al., 2025), telephone-based delivery (Dieng et al., 2016; Mosher et al., 2018), videoconferencing (Milbury et al., 2021) and hybrid (Akard et al., 2015; Compen et al., 2018) formats. Intervention duration ranged from brief exposures to extended multi-week or multi-month programmes. Furthermore, intervention providers varied across trials and included oncology nurses (Arpaci et al., 2023), psychologists (Akkol-Solakoglu and Hevey, 2023; Dieng et al., 2016; Flix-Valle et al., 2025), therapists (Compen et al., 2018), social workers (Mosher et al., 2018) and in some cases unspecified facilitators. Differences in professional expertise, therapeutic intensity and level of guidance may have influenced treatment fidelity and patient engagement, thereby contributing to outcome variability.
Participant setting also warrants consideration. Most studies recruited patients from outpatient clinics, community registries or online platforms rather than inpatient hospital settings (Admiraal et al., 2017; Akard et al., 2015; Akkol-Solakoglu & Hevey, 2023; Arpaci et al., 2023; Compen et al., 2018; Flix-Valle et al., 2025; Milbury et al., 2021; Mosher et al., 2018; Penedo et al. 2020; Wu et al., 2025). Patients in outpatient or survivorship phases may present with moderate baseline distress levels and distinct psychosocial needs compared to hospitalised individuals undergoing acute treatment. Such differences in clinical context may have moderated responsiveness to intervention and reduced the magnitude of detectable between-group differences. In addition, non-specific therapeutic effects may have attenuated pooled estimates. In several trials, control groups received standard care (Admiraal et al., 2017; Flix-Valle et al., 2025; Wu et al., 2025), structured education (Chambers et al., 2018; Li et al., 2023; Milbury et al., 2021; Mosher et al., 2018; Penedo et al., 2020), or supportive attention (Akard et al., 2015). These conditions may generate expectancy-related or attention-related benefits that reduce observable differences between intervention and control groups, particularly for outcomes such as distress and quality of life that are sensitive to perceived support. Therefore, the absence of statistically significant pooled effects should be interpreted with caution and not equated with a lack of clinical relevance.
Although understanding which specific intervention characteristics contribute most strongly to effectiveness would enhance the practical implications of this review, the limited number of studies per outcome and the substantial heterogeneity observed across trials precluded formal subgroup or moderator analyses. The included studies differed considerably in technology modality, intervention duration, theoretical orientation and degree of professional involvement. Although structured, multi-session programmes grounded in cognitive-behavioural or mindfulness-based frameworks appeared to show promising patterns, these observations should be interpreted cautiously. More rigorous trials with larger samples and standardised reporting of intervention components are needed to clarify which design features most consistently influence psychosocial outcomes.
Effects on quality of life
The findings also indicated a trend towards improved quality of life, although the result was not statistically significant. Nonetheless, this positive trend aligns with previous meta-analyses reporting that interventions involving mobile applications, brief therapy models and patient–provider communication can positively influence cancer-related quality of life (Li et al., 2022; Qin et al., 2022). Such interventions may help patients manage symptoms, reduce emotional burden and enhance daily functioning through skill-building and behaviour change (Akard et al., 2015; Penedo et al., 2020). Moreover, digital platforms allow for the flexible and repeated use of therapeutic content, which may support sustained engagement and long-term benefits (Marthick et al., 2021; Sharma et al., 2018).
Importantly, intervention duration varied widely across studies, ranging from 2-week programmes to digital interventions extending up to 12 months. Differences in treatment exposure, reinforcement intensity and follow-up length may influence both short-term responsiveness and sustainability of benefit, particularly for multidimensional constructs such as quality of life. Consequently, the absence of statistical significance at the pooled level may reflect methodological diversity and limited statistical power rather than the absence of clinically meaningful effects.
These findings can be further understood through established psychosocial and behavioural frameworks. Stress and coping theory suggest that structured psychoeducation and cognitive restructuring enhance adaptive coping and reduce maladaptive threat appraisal related to cancer uncertainty (Lazarus and Folkman, 1984). Similarly, self-efficacy theory posits that repeated skills practice and guided professional support strengthen patients’ confidence in managing illness-related concerns, which may translate into reduced fear of recurrence and improved emotional adjustment (Bandura and Wessels, 1997). Adaptation models in chronic illness further emphasise that ongoing access to coping resources facilitates psychological adjustment over time (Livneh and Antonak, 2005). Integrating these theoretical perspectives helps clarify why structured, skill-based digital interventions may demonstrate particular benefit for cognitively mediated outcomes.
Several mechanisms may explain the observed psychosocial benefits. Firstly, digital interventions offer opportunities for personalisation, which enhances user relevance and motivation (Golita and Baban, 2019; Zhang et al., 2022). Secondly, they reduce logistical barriers to care, such as transportation or scheduling, which are often cited by patients as impediments to accessing psychosocial support (Cox et al., 2017; Milbury et al., 2021). Thirdly, ongoing access to educational and therapeutic resources, along with asynchronous communication options, fosters patient autonomy and emotional resilience (Caminiti et al., 2023; Yang et al., 2024). Collectively, these characteristics position technology-based psychosocial education as a scalable and adaptable adjunct to conventional oncology services, particularly within survivorship and long term follow up care.
Overall, these results underscore the growing potential of digital health tools as adjuncts to traditional cancer care. The present meta-analysis demonstrated a statistically significant reduction in fear of cancer recurrence, whereas the effects on psychological distress and quality of life were not statistically significant. This difference may reflect the more targeted and modifiable nature of fear of cancer recurrence, which can be directly addressed through psychoeducation, coping strategies and reassurance delivered through structured technology-based psychosocial education interventions. In contrast, broader outcomes such as psychological distress and quality of life are influenced by multiple clinical, social and personal factors, including disease severity, treatment burden, social support and individual coping resources, which may limit the magnitude of change achievable through short-term interventions. Continued innovation and refinement of these tools may help overcome existing limitations and expand their utility across diverse cancer populations (Dong et al., 2025; Flix-Valle et al., 2025). From a nursing perspective, and consistent with the person-centred care framework introduced in the background, these findings suggest that technology-based psychosocial education can support nurses in delivering individualised psychosocial support, patient education and self-management guidance as part of holistic cancer care.
Strengths and limitations
This review has several strengths. It provides a focused synthesis of technology-based psychosocial interventions in oncology, clarifying their differential effects across key psychosocial outcomes. The findings highlight the particular responsiveness of fear of cancer recurrence to structured digital interventions and offer insight into how modality, duration and professional involvement may influence intervention effectiveness. By integrating empirical findings with established behavioural frameworks, this review advances both conceptual and practical understanding of digital supportive care in cancer survivorship. Despite these strengths, several limitations should be acknowledged. Heterogeneity in intervention formats, sample characteristics and outcome measures limits comparability across studies. In addition, the small number of studies for certain outcomes reduced statistical power. Substantial heterogeneity, particularly for psychological distress, restricted formal moderator analyses and may limit generalizability of pooled estimates. Variability in cancer type and stage, intervention modality, provider background and duration further complicate direct comparison across trials. Differences in participants’ digital literacy levels were not consistently reported across studies and may have influenced engagement, adherence and responsiveness to technology-based interventions. Methodological concerns, including limited reporting of allocation concealment and insufficient blinding, may have introduced bias. Cultural diversity was also variably addressed, and most studies were conducted in high-income countries, which may limit applicability to culturally diverse or low-resource settings. Furthermore, restricting inclusion to English-language, peer-reviewed studies may have excluded relevant data and contributed to publication bias. Finally, follow-up duration varied considerably across trials, with some studies assessing only short-term outcomes, thereby limiting conclusions regarding the sustainability of intervention effects over time. The certainty of evidence was not formally evaluated using the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach, which may limit the ability to comprehensively interpret the strength and clinical confidence of pooled findings. Future reviews should incorporate GRADE assessment to enhance transparency and decision-making relevance.
Implications
The findings support the integration of technology-based psychosocial interventions into routine cancer care, particularly in survivorship programmes. Structured, multi-session interventions grounded in cognitive-behavioural or mindfulness-based frameworks appear, especially promising for reducing fear of cancer recurrence (Hall et al., 2018, 2020). Programmes that incorporate professional guidance and provide sufficient duration for skill reinforcement may further enhance patient engagement and promote sustained benefit (Lindsay et al., 2018; Zhang et al., 2021). These digital approaches may be particularly valuable for patients with limited access to traditional psychological services or for those seeking flexible and private forms of support. Nurses should consider patients’ digital literacy when recommending such interventions and may offer brief orientation or technical support to facilitate optimal engagement. In this context, oncology nurses are well positioned to support implementation and continuity of care. Nurses can help identify appropriate candidates for digital psychosocial interventions, reinforce skill use during follow-up visits and coordinate referrals to mental health professionals when needed. Integrating routine distress screening with structured digital referral pathways may further enhance timely and equitable access to supportive care. Future research should strengthen the evidence base for technology-based psychosocial interventions in oncology through adequately powered randomised controlled trials across diverse cancer populations and care settings. Studies should systematically evaluate key intervention characteristics, including delivery modality, duration, level of professional guidance and patient engagement strategies, to identify effective and scalable models of digital supportive care. Longitudinal research is also needed to assess the sustainability of intervention effects across the cancer trajectory. Additionally, future studies should consider the influence of digital literacy, cultural context and health system factors on intervention uptake and effectiveness and apply standardised outcome measures and evidence appraisal frameworks such as GRADE to enhance comparability and translation into clinical practice and policy.
Conclusion
Technology-based psychosocial interventions offer a promising, accessible and scalable means of supporting the emotional well-being of cancer patients. Although evidence supports their effectiveness in reducing fear of recurrence, their impact on broader psychological distress and quality of life remains variable. Given their scalability and potential for integration into routine oncology workflows, structured digital interventions may expand access to psychosocial care, particularly in survivorship and resource-limited settings. Future research should aim to standardise intervention protocols, assess long-term outcomes and explore patient-level moderators that influence treatment response. Priority areas include identifying optimal intervention duration, level of professional guidance and delivery modality, as well as evaluating implementation strategies that promote equitable access and sustained engagement. With thoughtful integration into cancer care pathways, digital interventions have the potential to enhance patient-centred support and improve survivorship outcomes.
Key points for policy, practice and research
Technology-based psychosocial interventions show promise in reducing fear of cancer recurrence among cancer patients.
Effects on psychological distress and quality of life remain variable; however, structured, multi-session interventions grounded in cognitive-behavioural or mindfulness-based approaches and supported by professional guidance appear most promising for implementation.
Future research should compare intervention modality, duration and level of professional guidance and standardise reporting of intervention components to optimise implementation in oncology care.
Supplemental Material
sj-docx-1-jrn-10.1177_17449871261442808 – Supplemental material for Technology-based psychosocial education for cancer patients: a systematic review and meta-analysis
Supplemental material, sj-docx-1-jrn-10.1177_17449871261442808 for Technology-based psychosocial education for cancer patients: a systematic review and meta-analysis by Ice Septriani Saragih, Huey-Ming Tzeng, Irwan Susanto and Ita Daryanti Saragih in Journal of Research in Nursing
Footnotes
Author contributions
Availability of data,code and materials
Data sharing is not applicable to this article as no new data were created or analysed in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study did not involve human participants; therefore, ethical approval was not required
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.