
Abstract
Background:
Hospitalisation affects children’s quality of life (QoL) regardless of illness, treatment and care.
Aims:
The objective of this study was to create an instrument for evaluating QoL of hospitalised children aged 7 to 18 years.
Methods:
Initially, 46 items for the preliminary Hospital Quality of Life for Children Scale (HQL-children) were developed through a combination of literature reviews and individual interviews. The study was conducted with 230 participants from a general paediatric ward of a hospital. Exploratory and confirmatory factor analyses were conducted to examine the construct, convergent and discriminant validities of the measure. Criterion validity was assessed by confirming split-half reliability, whereas reliability was established using Cronbach’s alpha coefficient.
Results:
The HQL-child scale consists of 17 items and the total variance is 51.14%. The scale is categorised into five sub-dimensions: illness, fear, activity, hospital and perception. The scale demonstrated construct, convergent and divergent validity, discriminant and split-half reliability, with Cronbach’s alpha coefficient 0.75.
Conclusions:
The scale is a promising instrument to determine children’s perception by capturing their experiences on hospitalisation. Assessing the QoL in hospitalised children is crucial for enhancing patient satisfaction and facilitating the development of health policies based on patient self-reporting in Turkey.
Introduction
Children’s mental state is very vulnerable to stressors as a reaction (Esmaeeli et al., 2014). Medical conditions and hospitalisation cause a major source of stress for the child (Dutra Farias et al., 2017; Sarman and Günay, 2023). Several studies have evaluated the effects of illness and hospitalisation on children particularly in terms of their emotional well-being (Marshall et al., 2022; Sarman and Günay, 2023; Zahed and Koohi, 2020).
Hospitalisation causes a sudden change in the child’s daily routine (Dutra Farias et al., 2017), and it is an unfamiliar situation for the child (Üstün et al., 2021). Hospitalisation causes children to lose control and stay away from their home, personal belongings, family life, social circles and habits (Santos et al., 2016; Stragliotto Bazzan et al., 2020). The child may begin suffering by being exposed to too much anxiety and stress (Dutra Farias et al., 2017). In addition, differences in food and restricted play due to the hospital environment (Coyne, 2006), staying with people they do not know and treatment interventions in hospital may lead children to experience more difficulty (Azevêdo et al., 2017; Chorney and Kain, 2010). Following hospitalisation, the child goes through periods of uncertainty about his/her clinical picture and may even face the possibility of clinical deterioration to cause mortality risk. The child may have a hostile perception of the hospital environment (Azevêdo et al., 2017). This may cause a prolonged recovery period and decrease the child’s quality of life (QoL; Möller et al., 2016, Richardson et al., 2018). Therefore, it is important to find strategies to ameliorate these effects. It is necessary to make administrative and organisational changes as well as individual and executive interventions paediatric units to reduce the effects of hospitalisation on children’s QoL (Boone et al., 2004). An increased number of researchers and clinicians have focused on measuring quality outputs (Ahmed et al., 2017; Arvidsson et al., 2019).
QoL is recommended as an important measure of the impact of health in a gradually increasing manner (Aspesberro et al., 2015; Conlon et al., 2009). Measuring the QoL helps in determining unique information about the child compared with disease symptoms and patient functionality measurements (Bourland, 2000). It also enables obtaining data on the patient’s perceptions and experiences of the symptoms through assessing the QoL and (Wallander and Koot, 2016). QoL scales are divided into general and disease-specific instruments. Generic tools represent all health conditions, whereas disease-specific tools focus on potential areas affected by expressing the challenges of a particular health condition (Bullinger and Quitmann, 2022). However, it is not possible to evaluate the QoL of children due to being in a hospital environment with these tools. It is thought that the evaluation of being in a hospital, which is a foreign environment where the child’s daily routine changes, is an important deficiency in terms of QoL. Because the focus is on the hospital environment and the child’s perception of it, not the evaluation of the quality of nursing care with self-report (Gabes et al., 2020) or the treatment adherence due to chronic illness or the effect of acute diseases on the child. There is no comprehensive tool to measure the hospital QoL of children in literature. The scale developed in this study was asked to respond to determining the QoL of the hospitalised child, regardless of the general or disease-specific QoL. Thus, strategies and plans can be made easily according to children’s self-reports.
Research aim
The aim of this study is to create the HQL-children scale, a context-specific instrument designed to assess the perceptions of QoL among children during their hospitalisation. Measuring QoL at the individual level is important. Therefore, this scale is to measure the QoL of the child because of the hospital environment and the effects of variables related to this environment during any time, for any child as an in-patient. This study can contribute to QoL in routine evaluations and follow-ups in the clinical process. This will also ensure that children’s care, treatment and health services satisfaction are determined, and health policies are planned according to the results.
Methods
Research design and process
This study represents a methodological endeavour aimed at the development and evaluation of the HQL-children scale. The HQL-children scale was developed with three main stages of scale development (item creation, assessment of content validity and item analysis; DeVellis, 2016).
Development of the HQL-children scale
In order to establish the sub-domains of QoL for hospitalised children, we conducted a comprehensive review of both domestic and international literature, as well as existing QoL scales. The obtained data were grouped by thematic analysis. Consequently, we categorised hospitalised children QoL domains into the illness domain, child’s mental state domain, school/friend domain, social and daily activities domain, family/home life domain and hospital domain. We conducted in-depth interviews to test these areas. Nevertheless, upon conducting in-depth interviews, we discovered certain limitations in these domains when assessing the QoL of hospitalised children.
In-depth individual interviews using semi-structured questions were conducted from June to October 2021 with 18 hospitalised children (7–18 years of age). The interviews were conducted by the researchers. Participants were recruited from children staying in the paediatrics department of a University Hospital in western of Turkey. The qualitative thematic analysis method was used in the analysis of qualitative data obtained through individual interviews. The analysis was conducted utilising the framework proposed by Diekelmann et al. (1989), which is grounded in hermeneutic-phenomenological principles (Diekelmann et al., 1989). To ensure the reliability of the interview data, reliability, applicability, consistency and neutrality were used using the Lincoln and Guba’s (1985) qualitative research criteria (Lincoln and Guba, 1985).
Ten experts (three paediatric nursing professors, five paediatric nursing associate professors and two statisticians) tested the content validity of 63 items. The experts are national experts determined by the snowball method. The experts used a four-point scale to rate and assess the clarity and suitability of each item (1 = not suitable, 2 = relevance cannot be determined without item revision, 3 = suitable but requires minor modification, 4 = highly suitable). In addition, the comment of each item was requested. The item-level CVI (I-CVI) was used to calculate the Content Validity Index (CVI). Mean of the scale-level CVI (S-CVI/Ave) was used to measure the item’s content and relevance. Each item was scored by 10 experts. In order to have content validity, the results must be at least 0.78 for I-CVI and 0.80 for S-CVI/Ave (Polit and Beck, 2010). Our content validity findings were I-CVIs between 0.70 and 1.00 and S-CVI/Ave was 0.86. Fourteen excluded items have an I-CVI value of 0.78 or less. Finally, a pool of 46 items was created.
Evaluation of the HQL-children scale
The corrected item-total correlation coefficient, which is the first step followed in the item analysis of a scale, was calculated. Subsequently, we proceeded with the analysis of the ‘inter-item correlation matrix’ and obtained information on the estimated changes if an item was removed from the scale (Ferketich, 1991). Exploratory factor analysis (EFA) is used where there is no knowledge among the items of the scale, that is, how many factors there are between the items and which factors are determined by which items. The aim of confirmatory factor analysis (CFA) is to verify whether the defined item set fits the collected data and to validate the conceptual framework (Hurley et al., 1997). The scale items were tested with EFA. An average variance extracted (AVE) test by DFA and construction reliability were used to verify reliability. Furthermore, Cronbach’s coefficients were computed as part of the analysis.
Measurement of the HQL-children scale
The survey consisted of the ‘socio-demographic information form’ (15 items) and ‘the HQL-children scale’. The scale consists of 46 items of 5-point Likert type and investigates the QoL of hospitalised children. Items suitable for the subscales that emerged because of the qualitative stage were included in the scale.
Sample
In factor analysis, it is recommended to have a sample size for the scale that is 5–10 times greater than the number of items (Şencan, 2005). In addition, it is recommended that the sample size be above 100. Being below this number is accepted as insufficient and unreliable (Şencan, 2005). The sample consisted of 230 hospitalised children from the paediatrics department of a University Hospital in western XX. Inclusion criteria for the study; (1) being able to communicate in Turkish, (2) permission to participate from the caregivers who agreed to participate in the research and (3) being between the ages of seven and eighteen. The data collection period was between January and April 2022.
Data analysis
Socio-demographic characteristics were analysed as frequency and percentage. CVI was determined by Davis technique and calculated for content validity (Davis, 1992). In construct validity analysis, (SPSS Inc., Chicago, IL, United States) was used for EFA, and (Amos Development Company, 2011) was used for DFA. EFA was performed with the promax rotation principal component analysis. The χ2 test, the root-mean-square error of approximation (RMSEA), the comparative fit index (CFI), the normal fit index (NFI), the goodness-of-fit index (GFI) and the standardised root-mean-square residual fit indices were analysed with DFA. Reliability testing was performed using Average Variance Extracted, Composite Reliability (CR) and Cronbach’s alpha coefficients.
Results
The mean age of the children was 12.11 years (SD = 3.38). About 26.0% of the children were male. The distribution of education of the children was close to each other. Most of the children (55.0%) were diagnosed a month before and longer, hospitalised once or twice before (60.0%), had invasive interference (87.0%), and no other disease (85.0%). Most of the children did not experience anything negative in the hospital (96.0%).
EFA involved assessing the adequacy of the dataset for factor analysis through the use of Kaiser–Meyer–Olkin (KMO) and Bartlett’s sphericity test. For the HQL-children scale, the KMO value was 0.75, and the sample size of the dataset was appropriate. Bartlett’s test of sphericity was found to be significant, and the variables were correlated with each other ( χ2: 1357.606, p < 0.000).
Forty-six items were included in the principal component analysis, and factor analysis was performed using the promax rotation method. Factors with eigenvalues greater than 1 were examined and evaluated. The 17-item scale and 5 factors were determined. As a result of the principal component analysis, the total variance explained for the five-factor structure was 51.14%. In the analysis using promax rotation, the first factor explained 19.24% of the variance. Other factors explained 17.18%, 6.08%, 5.36% and 3.25% of the variance, respectively.
As a result of the EFA, the HQL-children consisting of 5 subscales and 17 items was created. In the evaluation, it was determined that there was no item with a factor load below 0.40. The factor loadings of the HQL-children model ranged from 0.62 to 0.79 in the first factor, 0.65 to 0.90 in the second factor, 0.62 to 0.71 in the third factor, 0.46 to 0.61 in the fourth factor and 0.59 to 0.71 in the fifth factor.
CFA: Fit indices (χ2/df, RMSEA, CFI, GFI, NFI, AGFI and NNFI) were calculated to evaluate the fit of the data to the model. CFA results of the HQL-children are given in Table 1. The fit indices yielded the following results: χ2/df:1.85, RMSEA: 0.061, GFI: 0.91, AGFI: 0.87, CFI: 0.92, NFI: 0.86 and IFI: 0.93 (Table 1). It was found that χ2/df, RMSEA, NFI, GFI, CFI, AGFI and IFI indices had acceptable values. The CFA results confirmed that the scale comprised five distinct factors: illness (38, 39, 40, 41), fear (22, 23, 24), activity (15, 28, 33), hospital (26, 27, 35, 36) and perception (16, 43, 44), as shown in Figure 1. The factor loadings within the HQL-children model varied between 0.55 and 0.93 for the first factor, 0.64 and 0.86 for the second factor, 0.57 and 0.77 for the third factor, 0.38 and 0.81 for the fourth factor and 0.58 and 0.79 for the fifth factor.
Fit indices for the HQL-children scale.

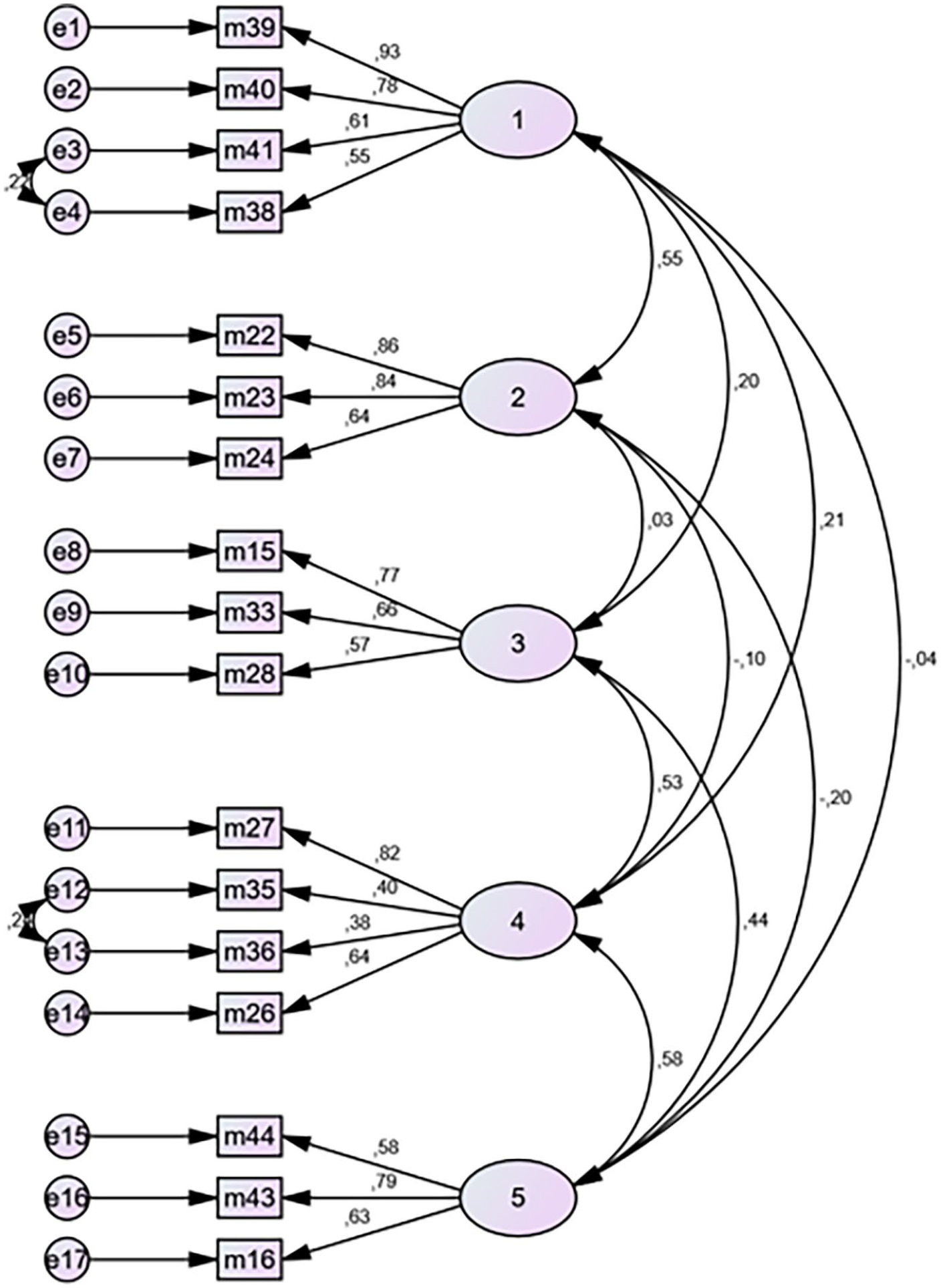
Path diagram for the HQL-children scale.
Convergent validity of the measurement model in Table 2 was assessed through AVE and CR analyses.
CR and AVE values of the HQL-children scale.
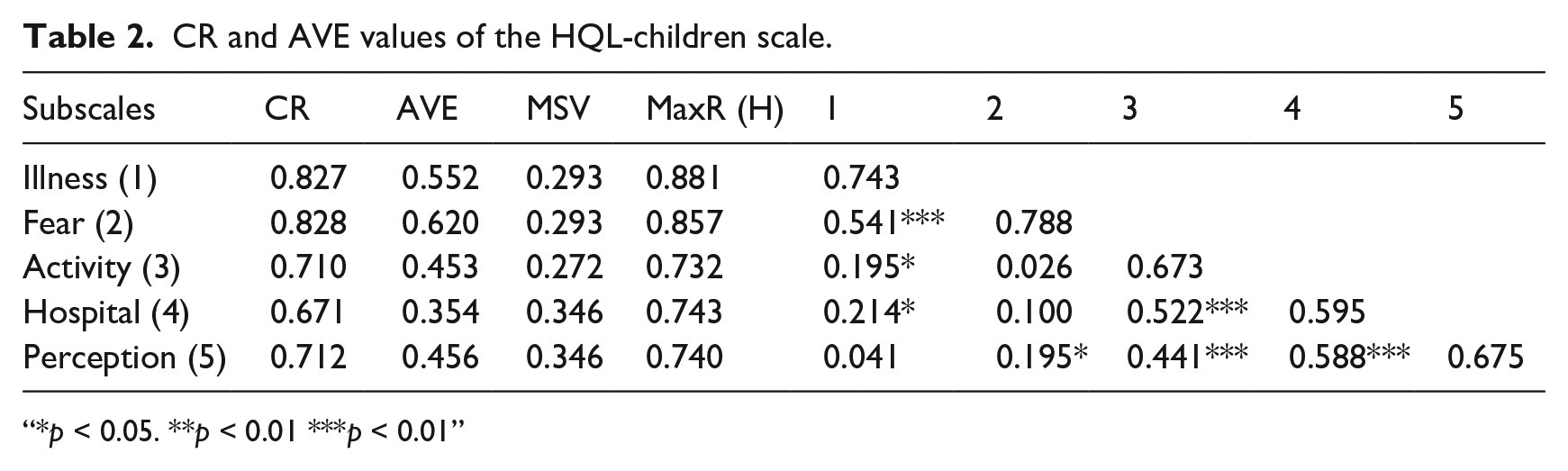
“*p < 0.05. **p < 0.01 ***p < 0.01”
Cronbach’s alpha coefficient for the HQL-children scale was determined to be 0.75. Cronbach’s alpha coefficients was 0.82 for illness, 0.82 for fear, 0.70 for the activity, 0.63 for the hospital and 0.70 for the perception. To assess the internal consistency of the scale, item analysis was conducted. The analysis revealed that the total score correlations of item subscales were within the range of 0.55–0.73 for illness, 0.58–0.73 for fear, 0.47–0.56 for activity, 0.37–0.57 for hospital and 0.48–0.59 for perception. As a result of the evaluation of the 27% lower-upper group mean scores for determining the item discrimination of the developed scale with Student’s t-test, statistical analysis demonstrated a statistically significant difference between the two groups for all items (p < 0.05; Table 3).
Reliability coefficients and item analysis of HQL-children scale.
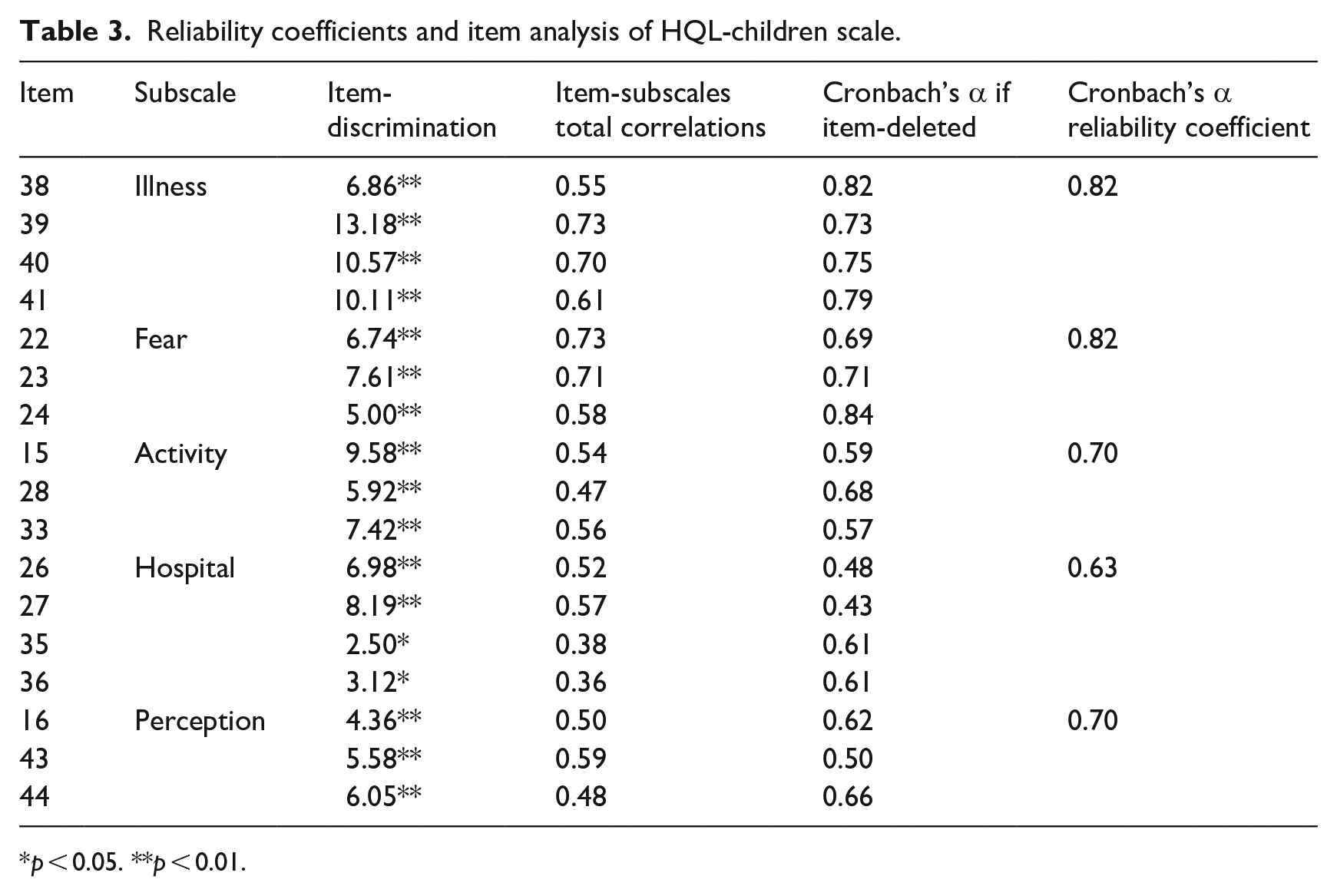
p < 0.05. **p < 0.01.
In the split-half analysis, it was found that the correlation between the two halves of the scale was 0.74, the Spearman–Brown analysis reliability coefficient was 0.85. The Guttman split-half reliability coefficient was 0.85. Hotelling’s T2 test was used to determine the response bias of the scale. As a result of the test, it was determined that the Hotelling T2 test value was significant, and the answers given by the participants were not biased (Hotelling T2:1882.87, p = 0.00).
Discussion
Children have to be hospitalised due to acute conditions that may occur as a result of various accidents and chronic diseases such as congenital anomalies, epilepsy, chronic kidney failure, cancers, haemophilia, diabetes and cystic fibrosis (Bolat, 2018; Sarman and Sarman, 2020). Illness and hospitalisation have negative effects on children, such as pain, as well as negative emotions such as aggression, anger, fear of injury, guilt, anxiety and fear (Yurdabakan and Demirtaş, 2019; Selbes et al., 2021). Also, illness and hospitalisation significantly diminishes the QoL for the child (Möller et al., 2016). Hence, there is a requirement for assessment instruments to gauge their QoL (Çeltek and Okan, 2016). QoL scales for children can be categorised into two groups: general scales and disease-specific scales (Verstraete et al., 2020). There is a substantial body of literature dedicated to examining both types of QoL scales for children (El Shafei et al., 2018; Ruggiero et al., 2018; Sood et al., 2018). However, children’s QoL could be affected by the places where they spend their time. For instance, the literature presents studies conducted on school QoL scales developed for children (Kırnık et al., 2021; Sarı, 2012). No scales could be found that have been developed or adapted specifically for hospitalisation. The present article is expected to contribute to the literature as the first article to look into the HQL-children scale.
The HQL-children scale was designed with five subscales: illness, fear, activity, hospital and perception. The domains, categories and items identified by the present study were created in line with a preliminary literature review and the results obtained from the analysis of the individual interviews.
KMO values were found over 0.50 for the HQL-children, and the result of the Barlett’s sphericity test was significant (p < 0.05). These results showed that the number of samples in the data set was at a sufficient level, and the data distribution was homogenous. Construct validity of the HQL-children was confirmed with EFA. As a result of the EFA, five subscales were obtained explaining 51.14% of the total variance. Total explained variance ranging between 40.0% and 60.0% is considered sufficient (Tavşancıl, 2005). Factor loadings for each item of the five subscales were in the range of 0.69–0.79, 0.65–0.90, 0.62–0.71, 0.46–0.61, and 0.59–0.71, respectively. Item factor loadings are over 0.40, which is at the acceptable level (Field, 2009). In order to determine the data-model fit, χ2/df, RMSEA, GFI, AGFI, CFI, IFI and NFI fit indices were evaluated in the CFA. RMSEA values indicate ⩽0.050=perfect fit, 0.050-0.080=good fit and 0.080-0.10=poor fit (Balcı, 2018). For a good fit, CFI and NFI values along with the RMSEA values must be equal to 0.90 or over, AGFI equal to 0.80 or over and GFI equal to 0.90 or over (Akgül, 2005; Balcı, 2018, Şimşek, 2007). Among the fit indices results, especially χ2/df ratio shows a perfect fit, whereas RMSEA, GFI, CFI, AGFI, IFI, PGFI and TLI values were found within the acceptable range. Some studies in the literature suggest that NFI has a value ‘between 0 and 1, and values closer to 1 indicate good fit’ (Schermelleh et al., 2003). The CFA results of the HQL-children scale showed that all the factor loadings (except item 36) were larger than 0.40, which is acceptable. In addition, two modifications were made in the CFA (Figure 1). In the modification, there was a contextual correlation between the items (35–36 and 38–41). CFA results indicated that the data-model fit was good, and it confirmed the five-factor construct. It is seen that the items and subscales are related with the scale, and the items of each subscale define their own factors sufficiently.
CR and AVE are calculated to estimate whether the observed items of the subscales are highly correlated with each other. To indicate an adequate convergent validity, AVE values should exceed the threshold of 0.50, whereas CR values should surpass the acceptable level of 0.70. It is acceptable if the CR value is between 0.60 and 0.70 (Hair et al., 2014). In this study, the CR values of the scale were found to be above acceptable values, and it had convergent validity. Nevertheless, the AVE values of the scale in the activity, hospital and perception subscales were below the threshold of 0.50.
Internal consistency of these subscales was examined by item-total correlations and Cronbach’s alpha coefficient. Cronbach’s alpha coefficient: <0.40 = not reliable; 0.40–0.59 = poor reliability; 0.60–0.79 = high reliability; 0.80–1.00 = very high reliability (Akgül, 2005). Total scale Cronbach’s α value is 0.75. Cronbach’s alpha coefficient for all the subscales and the overall scale were in acceptable limits (⩾0.70), except for the hospital subscale which is very close to 0.70.
The reliability of the scale items is demonstrated by the correlations between item subscales and the total score. These values are expected to be above 0.30 (Esin, 2014). The reliability scores of the subscales were found to be within an acceptable range. This result is evidence of all items within the subscales measure the same underlying property.
Reliability coefficient of dividing into two halves is expected to be over 0.70 (Büyüköztürk 2002). The correlation between the two halves of the scale is 0.74, which indicates that the measurement tool is consistent within itself.
The scale format may have an undesirable effect on the responses of the study participants. The Hotelling T2 test is used to determine whether participants’ responses to scale items are equal (Şencan, 2005). It was found to be significant because of the analysis (p < 0.05). It does not have response bias for the HQL-children scale in this study.
Since the study was conducted in a single centre, it is thought that the patient children were mostly evaluated in a single centre. This is one of the most important limitations of the study. It is recommended to conduct multi-centre validity and reliability studies of the scale in different regions and cultures. The scale covers the 7–18 age group of children and does not evaluate all children. This highlights the need to study in younger age groups. Additionally, since the 7–18 age group includes two different childhood age periods, it is recommended that the scale be evaluated carefully.
Conclusion
In conclusion, we found that the HQL-children scale was a valid, reliable and useful tool to accurately assess children’ QoL towards hospital conditions and effects. Additionally, the HQL-children allows the opportunity to notice risks that may occur due to hospitalisation. For this reason, the HQL-children scale is recommended for use in easing the safe and successful experience of hospital process in children and planning interventions for risks. It is important for the theoretical structure of the scale for it to be tested on different sample groups.
This study suggests that the scale is an appropriate assessment tool that can be easily practiced. The care, treatment and health services given by nurses to their patients should be met by questioning the QoL based on patient self-report. This tool will contribute to the satisfaction of health services and thus to the creation of patient-oriented health policies.
Key points for policy, practice and/or research
The nurse should develop strategies based on child patients’ self-report to identify their health needs.
Hospital care for child patients can be improved through creating greater satisfaction with health services.
Training programmes for hospital staff need to adopt a patient-oriented approach.
Hospital policies and processes need to be based on a patient-oriented health policies framework.
Footnotes
Disclaimer
The Abstract was presented as an oral presentation in the 7th International Congress on Quality of Life in Health. Manisa, Turkey on 8–10 December 2022. The manuscript was part of a research of Ph.D.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Manisa Celal Bayar University ethics committee granted ethical approval for the research (Approval date: 04/11/2020, File number:20.478.486/610). In addition, written permission was obtained from the parents and patients who agreed to participate in the study with the ‘Informed Volunteer Consent Form’.