
Abstract
To observe the effects of Fu’s subcutaneous needling (FSN) and acupuncture treatment on the mitochondrial structure and function of the skeletal muscle tissue of rats with sciatica. Forty Sprague–Dawley rats were divided into control, model, acupuncture, and FSN groups (10 each) according to a random number table. The control group was left untreated. Rats in the FSN group were treated with FSN once every 2 days for three times, respectively (days 1, 3, 5, and 7), to cooperate with reperfusion approach. The acupuncture group was treated at the same timeline as that of the FSN group. Changes in the mechanical pain threshold, mitochondrial ultrastructure, mitochondrial citrate synthase (CS) activities, mitochondrial respiratory chain complex II, and mitochondrial COX- I protein expression in the skeletal muscle of rats treated with different treatments were compared with those of the model group. The pain thresholds of the rats were remarkably higher after FSN treatment and acupuncture, and the pain threshold of the FSN group was higher than that of the acupuncture group. Compared with the control group, the mitochondria of the model group had a damaged ultrastructure, were arranged in a disorganized manner, accumulated under the basement membrane, and appeared vacuolated with autophagosomes. The state of mitochondria in the FSN group was close to that in the control group and was remarkably better than that in the acupuncture group. The activities of mitochondrial CS and respiratory chain complex II in the skeletal muscle of the treated rats decreased compared with the control group (p < 0.05), and their levels were better in the FSN group than in the acupuncture group (p < 0.05). FSN treatment for 1 week considerably improved the pain thresholds and improved the skeletal muscle mitochondrial ultrastructure and mitochondrial function in rats with sciatica.
Keywords
Introduction
Fu’s subcutaneous needling (FSN) was invented by Dr. Zhonghua Fu in 1996. Dr. Fu integrated modern anatomy, sports medicine, physiology, biomechanics, and fasciology in developing a special field of medicine for more than 20 years; he formed FSN’s characteristic theoretical system and clinical diagnosis and treatment patterns.1–3 FSN therapy is widely used, and its efficacy is exact for somatic and visceral pain; it also has remarkable effects on non-painful conditions, such as chronic bronchitis, stress urinary incontinence, chronic superficial gastritis disease, Parkinson’s disease, myopia, and intractable diarrhea, but its specific mechanism of action is yet to be elucidated.4–6 The diseases that FSN can treat, including painful or non-painful diseases, are initially caused by muscle problems. Long-term muscle overload, exercise, incorrect force posture, and muscle atrophy and degeneration lead to ischemia and hypoxia of muscle tissues and cause myofascial trigger point (MTrP) via the theory of energy crisis. 7 FSN acts on connective tissues that are closely related to muscles, particularly tightened muscles (TMs), as proposed by Dr. Zhonghua Fu in 2014. TMs are muscles with a single or multiple MTrPs and present as tightness and cramps when the central nervous system is relaxed but the target muscle is fully or partially stiff because of ischemia or hypoxia in local muscle tissues. 8
In 2011, the International Pain Association defined neuropathic pain as a chronic pain caused by nerve injury. Sciatica belongs to neuropathic pain, including primary and secondary pain. Intervertebral disc herniation is the most common cause of sciatica. Other causes include the inflammatory material exudation of muscle injury, intraspinal tumor, and lumbar spinal stenosis 9 as well as sacroiliac arthritis, pelvic tumors, and diabetes. Clinically, acupuncture and FSN can improve the clinical symptoms of sciatica. Many clinical studies have shown that the overall efficacy of acupuncture, including electroacupuncture, warm acupuncture, and FSN, is better than that of conventional Western medicine therapy, and acupuncture can effectively reduce pain symptoms and improve the quality of life of patients without any toxic and side effects.10–11 Whether the good effects of FSN or acupuncture is exerted through subcutaneous connective tissues and muscle tissues still needs to be explored. Muscles have nutritious and innervated nerves. Muscle denervation and innervated nerve apoptosis occur following nerve injury. In the absence of nerve activity, muscle will atrophy; muscle mass will be reduced; and muscle strength, fiber diameterm and quantity will be reduced in varying degrees.12-14 Although sciatic nerve injury belongs to peripheral neuropathy, relevant literature reported that ligating the sciatic nerve will induce severe pain and lead to the atrophy of related muscles. 15 Therefore, FSN is hoped to be used to treat the injured nerve and muscle tissue, improve mitochondrial function, and prevent muscle atrophy.
Materials and methods
Experimental animals and grouping
Forty rats (specific pathogen-free grade, body weight 250 ± 10.5 g, aged 7 weeks) were purchased from Ponyue Animal Center, Jinan, China. The rats were caged, given standard rat chow and water, and housed in the laboratory animal center of Wei Fang Medical College with the approval of the ethics committee of Wei Fang Animal Medical Center (SCXK(鲁)20190003). The environment was kept at a constant temperature of 25°C, a relative humidity of 40%–70%, and a 12-h light/dark cycle. The rats were adaptively housed for 7 days and divided into four groups using a random number table method with SPSS: Control (COT) group, Model (MOD) group, acupuncture (ACP) group, and FSN group (Figure 1). Flow chart of animal experiment.
Main instruments and reagents
The instruments used include a horizontal decolorization shaker (Beijing Dingguo Biotechnology Co, Ltd.), an ultrapure water machine (Shanghai Hetai Instruments Co., Ltd.), a low-temperature high-speed centrifuge (Eppendof, Germany), a pipette (Biosharp, China), a −80°C cryogenic refrigerator (Japan), a transmission electron microscope (JEM-1400, Japan), a special imaging system for transmission electron microscope (Gatan, USA), a microplate reader (BioRad, USA), an electrophoresis apparatus (BioRad, USA), an electrophoresis tank (BioRad, USA), and a gel imaging system (BioRad, USA). The BCA Protein Quantification Kit, Animal Tissue Mitochondria Isolation Kit, Rat Citrate Synthase (CS) Enzyme-linked Immunosorbent Assay (ELISA) Kit, and Respiratory Chain Complex II ELISA Kit were purchased from Beyotime Institute of Biotechnology, Shanghai, China. Anti-GAPDH and anti-Cox I were from Abcam (Nanjing).
Modeling method
Bennet et al. established a sciatic nerve model with chronic constriction injury (CCI) in 1988.
16
The rats were placed prone on the operating table. The right hind limb was shaved and disinfected. The leg skin was cut, the subcutaneous fat and superficial fascia were separated layer by layer, and the biceps femoris was passively separated with ophthalmic forceps with both hands to expose the sciatic nerve trunk. The sciatic nerve trunk was picked out with a glass minute needle and ligated four times with a spacing of about 1 mm. The ligation force should not affect the blood transport of the nerve adventitia (4-0 medical catgut was used as the ligation line), and a slight twitch of the limbs was observed during ligation. After ligation, the muscle and skin were sutured layer by layer, and penicillin sodium powder was applied to the wound before and after suturing to prevent infection
16
(Figure 2). The control group was not operated. The other three groups were divided according to the rat model of sciatica, and then the sciatic nerve was double ligated to establish the chronic injury model. After modeling, the pain threshold was measured on days 1, 3, 5, and 7. Neuropathic pain appears indicates that the modeling was successful, and the unsuccessful rats were excluded. The intervention began on day 1. (Figure 3) (a) 4-0 medical catgut was used to ligate the sciatic nerve and four knots. (b) Anesthetized rat was fixation for skin preparation and posterolateral thigh surgery. Time flowchart of this study. Before modeling, the pain threshold of rats of each group was measured as an initial threshold. Since the first day (-7) after modeling, the pain threshold in each group was measured, and followed by every 2 days respectively (-5, -3, -1, 1, 3, 5, 7) days. The pain threshold measured on "-1″ day indicated that the modeling was successful. After the completion of modeling, the intervention started on "1″ day. Except for the COT and MOD group, the FSN and ACP group were treated with FSN needle and acupuncture at fixed time points on (1, 3, 5, 7) days respectively. FSN: Fu’s subcutaneous needling; ACP: acupuncture; MOD: model; COT: control.

Treatment protocol
After modeling, the ACP and FSN groups were treated. The rats were fixed and disinfected prior to treatment. The ACP group was treated with acupuncture. Rats were acupunctured with 1.25 mm-diameter needles in two acupoints: "Wei-zhong (BL40)", and "Huan-tiao (GB30)" (Figure 4(b)) without anesthetization. The location of "Wei-zhong (BL40)" was on the depression in the posterior square of the knee joint of the hind limb and "Huan-tiao (GB30)" was on the posterior upper edge of the hip joint of the hind limb.
17
After the rats in the ACP group were fixed with the rat fixator, the needles were kept for 20 min after the needle entered the acupoints. During this period, we observed the situation of the rats and whether the needle fell. If the needle fell, acupuncture was performed again. The rats were fixed and received intervention without anesthesia. (a) Fu’s subcutaneous needling (FSN) with the needle tip toward the gluteus maximus muscle was manipulated as the swaying movement (blue fan) in FSN group. (b) Acupuncture (ACP) was needled on "Huan-tiao (GB30)" and "Wei-zhong (BL40)" points (blue arrows) in ACP group.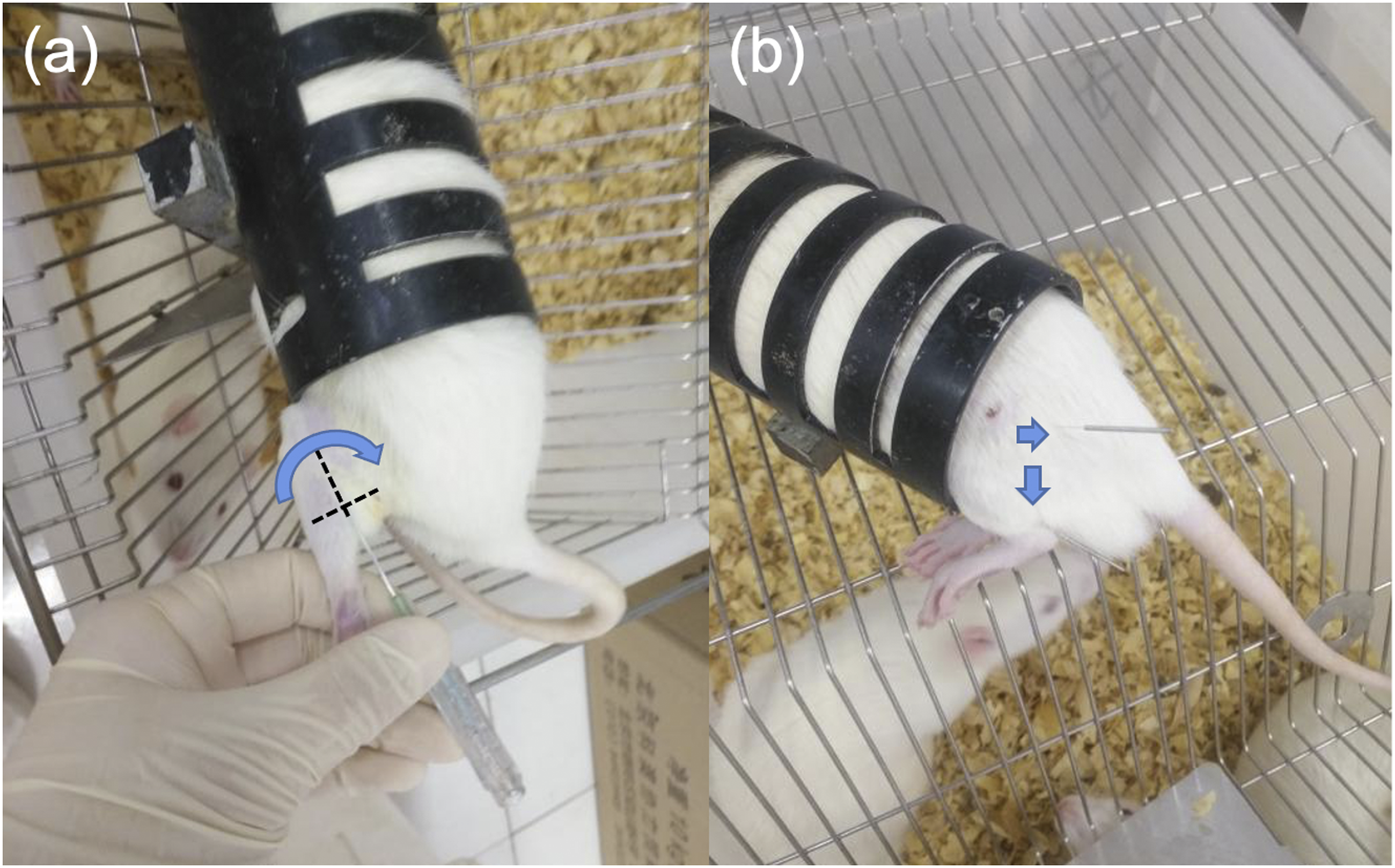
The FSN group was treated with FSN disposable needle (Nanjing paifu). (Figure 4(a)). The FSN needle was inserted toward the TM (the needle entry position was approximately near the gluteus maximus muscle). The needle was rapidly advanced to prevent the rat from being tense, which causes the muscle to contract and hinder the entry of the needle. Once the needle entered the skin, the needle was swayed, and the reperfusion approach was performed. The swaying movement, a key procedure for FSN, is a smooth, soft, fan-style waggle that uses the thumb as the fulcrum. The index, middle, and ring fingers stay in a line. The middle finger and thumb affix the needle in a face-to-face way, whereas the index and ring fingers alternately move back and forth. The FSN group was treated with a FSN needle with both hands combined with swaying and reperfusion approach. The frequency was 100 times/min, and the operation was about 1 min. The manipulation was performed once every 2 days for four times (days 1, 3, 5 and 7). The ACP group was treated the same time as the FSN group.
Sampling and sample preparation
1. Electron microscopy sample preparation: The rats were weighed in batches and anesthetized by intraperitoneal injection with 3% pentobarbital (30 mg/kg). A blade was used to rapidly separate a small piece of rat pear Longus longitudinally along the muscle fiber into 2×1×1 mm3 and then pre-chilled in 2.5% glutaraldehyde at 4°C for electron microscopy. 2. Preparation of skeletal muscle mitochondria: Each muscle tissue sample (100 mg) was placed in a pre-chilled lysis solution and analyzed using the Beyotime Animal Tissue Mitochondria Isolation Kit.
Index and methods
1. Measurement of mechanical pain threshold: The pain threshold was measured every 2 days. The rats with a confirmed group and number were placed in a box on a metal net with six rats each. Wait for 15–30 min until the rats keep quiet in the strange environment (do not walk around the cage or the rats will lick themselves). According to the pre-experiment, the von Frey hair values of 4, 6, 8, 10, 15, 26, 60, and 100 g were used for measurement. When measuring, the middle value (10 g) should be set as the starting point, and the values were measured in ascending order. When crossing for the first time, measure the values four times. Von Frey hair acts on the bottom of the toe between the left foot pads of rats. This position has a moderate response to mechanical stimulation and can directly reflect the degree of neuralgia.
18
Handheld von Frey hair had an "S" shape, the action time was 6–8 s, and the interval between adjacent stimuli was at least 7 s. A reaction was considered a positive reaction if the rats lift their feet or lick the stimulated side during the action time. In the stimulation process, rat movements, such as moving around or lifting their feet, upon stimulation are considered suspicious; therefore, the measurements were carried out after the rats calm down. The positive result was recorded as X, and the negative was O. The measurement results were recorded. The calculation formula is 50% g (threshold) = ( 2. Transmission electron microscopy (TEM): The rat piriform muscle was rapidly isolated, and the surrounding muscle was removed with a blade. The samples were rinsed three times with 0.1 M prechilled PBS and then overnight at 4°C. Osmium (1%) was added the following day for 2 h fixation at 4°C. The slides were washed sequentially with a concentration gradient of 50%, 70%, and 90% ethanol; 90% ethanol:90% acetone 1:1, 90% acetone, and anhydrous acetone (three times) The dehydration time was 15 min. Briefly, anhydrous acetone was immersed with the embedding agent according to the following formula: 3:1, 1:1, and 1:3. Then, the pure embedding agent, was added by shaking for 30 min. Finally, the pure embedding agent was immersed overnight. The next day, the immersed samples were placed in an embedding plate into which the embedding agent was injected and polymerized, and the polymerization temperature was set to 37° C for 12 h, 45°C for 12 h, and 60°C for 24 h. The samples were embedding with epoxy resin (Spurr), cut longitudinally, made into ultra-thin sections and stained with acetic acid dioxygen axis and lead citrate. After the samples were dried, the mitochondrial ultrastructures were observed by TEM. Each tissue section was observed first in the low power field of view (500–1000×) and then in the high power field of view (20,000–50,000×) to observe the distribution, size, morphology, crista structure, and autophagosome formation of the mitochondria. 3. The mitochondrial CS content and respiratory chain complex II in gluteus maximus muscle were measured by ELISA. The specific procedures were performed according to the kit procedures. 4. Western blot analysis. The COX- Ⅰ protein content of the gluteus maximus muscle was determined by Western blot. Briefly, small pieces of gluteus maximus muscle were reduced in pre-chilled lysis buffer and homogenized by a homogenizer, centrifuged at 12,000×g for 10 min at 4°C, and finally boiled for 5 min at 98°C. The sample was stored at −20°C for future use.
Data statistics and processing
The data were analyzed by GraphPad Prism statistical software. The data were expressed s mean ± standard deviation. Two-way ANOVA was used to analyze the main effects of processing factors and sampling time factors and their interaction. The statistical method of individual effects among groups was analyzed by one-way ANOVA. If the variance was homogeneous, the SNK-q method was used. If the variance was not homogeneous, the original data was converted to become homogeneous before statistical analysis. For the index data that cannot be converted, the statistical results of Tamhane’s T2 were directly used for analysis. p < 0.05 was statistically significant.
Results
Changes in the mechanical pain threshold of rats
Changes of mechanical pain threshold in each group.

Data were expressed as mean ± SD; p value was analyzed by One way ANOVA FSN: Fu’s subcutaneous needling; ACP: acupuncture; MOD: model; COT: control;
Timeline -7, -5, -3, -1 represent the first, third, fifth, seventh days after nerve ligation; Timeline 1, 3, 5, seven represent the first, third, fifth, seventh days of intervention in each group. FSN group and ACP group compared with the MOD group: P* < 0.05; FSN group compared with the ACP group: P#< 0.05; MOD group compared with the COT group: P▲ < 0.05.
The experimental results showed that except the CON group, no significant difference in pain threshold was found between the other groups at days -7, -5, -3, and -1 days after the completion of modeling. From the first day after the intervention, the pain threshold of the MOD, FSN, and ACP groups changed considerably. After the intervention, the pain threshold of the FSN and ACP groups increased in varying degrees from the third day, and the pain threshold of the FSN group was higher than that of the ACP group (p < 0.05). From the first day, the pain threshold of the model group without any intervention still decreased in varying degrees, but the pain threshold of the FSN and ACP groups were higher than that of the MOD group in varying degrees (p < 0.05 between the FSN and MOD group, p < 0.05 between the ACP and MOD groups) (Figure 5). Change trend of pain threshold of rats in each group. FSN: Fu’s subcutaneous needling; ACP: acupuncture; MOD: model; COT: control.
Changes in the mitochondrial ultrastructure of the gluteus maximus muscle of rats in each group
In this study, TEM was used to observe the changes in the mitochondrial ultrastructure of rats with sciatica using different intervention maneuvers. Under an electron microscope, the myofibril structure of the COT group was clear and complete, the mitochondria were orderly arranged, the mitochondria were long strip or oval, the bilayer membrane structure was complete and clear, the ridge structure was full and dense, and no obvious phagosomes was found (Figure 6 a1, a2). Remarkable differences in the mitochondrial ultrastructure among the MOD, ACP, and FSN groups after successful modeling before any interventions. Compared with the COT group, the arrangement of the mitochondria in the MOD group was disordered, the Z-line was partially broken, the number of mitochondria was remarkably reduced, and no obvious vacuolized structure and autophagy were found (Figure 6 b1, b2). One week after ACP treatment, the mitochondrial structure was observed under an electron microscope. Some mitochondria of skeletal muscles were still unevenly distributed. The mitochondria existed under the muscle membrane; the morphology of the mitochondria was irregular; and the mitochondria became larger, swollen, and vacuolized with unclear ridge structure and autophagic vesicles (Figure 6 c1, c2). After treatment with FSN, the mitochondrial structure of the model rats was remarkably restored compared with those of the MOD and ACP groups. The morphology of the mitochondria was regular; the structure was clear; and a few swelling, deformation, and vacuolization of the mitochondria occurred (Figure 6 d1, d2). Changes in the mitochondrial ultrastructure of the gluteus maximus muscle of rats in each group under transmission electron microscope. The arrows and box indicated by the arrows in b1 and b2 represented the place where a large number of mitochondria were missing, and the number of mitochondria in tissue decreased. At the places indicated by c1 arrows and c2 box, mitochondria appear vacuolized structure. At the place indicated by d1 box and d2 arrow, the structure of muscle tissue and the morphology of mitochondria were improved. a1, a2: COT group; b1, b2: MOD group; c1, c2: ACP group; d1, d2: FSN group. Observation under 20,000x electron microscope: a1, b1, c1, d1; Observation under 50,000x electron microscope: a2, b2, c2, d2. Dyeing method: acetic acid dioxygen axis, lead citrate. FSN: Fu’s subcutaneous needling; ACP: acupuncture; MOD: model; COT: control.
Mitochondrial CS content
Changes in the content of mitochondrial CS, Complex II/CS, and COX- I.

Data were expressed as mean ± SD; p value was analyzed by One way ANOVA; FSN: Fu’s subcutaneous needling; ACP: acupuncture; MOD: model; COT: control; CS: Mitochondrial citrate synthase; Complex II: Mitochondrial respiratory chain complex II; COX- I: Cyclooxygenase I.
FSN group and ACP group compared with the MOD group: P* < 0.05; FSN group compared with the ACP group: P# < 0.05; MOD group compared with the COT group: P▲ < 0.05.

Changes trend of mitochondrial CS content (a), complex II/CS ratio (b) and COX-I protein expression (c) in muscles with different intervention methods. CS: Mitochondrial citrate synthase; Complex II: Mitochondrial respiratory chain complex II; COX- I: Mitochondria Cyclooxygenase I. FSN: Fu’s subcutaneous needling; ACP: acupuncture; MOD: model; COT: control. FSN group and ACP group Compared with the MOD group: P* < 0.05; FSN group compared with the ACP group: P# < 0.05. MOD group compared with the COT group: P▲ < 0.05.
Mitochondrial respiratory chain complex II content
The CS content in the tricarboxylic acid cycle is often used to standardize the activity of the complex to eliminate the influence of quantitative mitochondrial changes, particularly the mitochondrial respiratory chain complex. The standardized experimental results showed that the activity of the mitochondrial respiratory chain complex II in rat skeletal muscle was significantly higher in the FSN and ACP groups than that in the model group (P* < 0.05), and the activity of respiratory chain complex in the FSN group was higher than that in the ACP group (P# < 0.05). A little difference was found between the COT and MOD group (P▲ < 0.05) (Table 2, Figure 7(b))
COX- I protein content in gluteus maximus muscle was determined by Western blot
The experimental results showed that the protein expression of COX- I in the skeletal muscle after different intervention methods was different and showed a downward trend. The protein expression of COX- I decreased after modeling. A remarkable difference in COX- I expression was found between the FSN and ACP groups. The COX- I protein expression of the FSN group was higher than that of the ACP group (P# < 0.05). The COX- I protein expression in the FSN group was significantly higher than that in the model group (P* < 0.05). Compared with the MOD group, have a significant difference in protein expression was found in COT group (P▲ < 0.05) (Table 2, Figure 7(c)).
Discussion
A large number of clinical studies has confirmed that FSN can effectively alleviate pain in the treatment of chronic diseases. However, no in-depth study has shown why intervention in connective tissues can improve the state of TM, as well as the possible influencing factors that can change the physical and chemical states of muscles. In this experiment, FSN was applied to the rat model of chronic pain. The specific mechanism of FSN in the treatment of chronic pain was analyzed by observing and comparing the morphological structures of mitochondria in muscle tissues before and after FSN treatment. Some important factors affecting mitochondrial energy metabolism were also analyzed. The experimental results showed that after 1 week of modeling, the number of mitochondria in the TM decreased; the structure and organization were disordered; and the mitochondria were deformed, swollen, and even vacuolized. The muscle tissues and fibers underwent atrophy, Z-line breakage, distortion and other phenomena. After 1 week of FSN treatment, a great degree of mitochondrial regeneration occurred, and the mitochondrial morphology and structure improved compared with the MOD and ACP groups. Compared with the MOD and ACP groups, the pain threshold in the FSN group was remarkably higher, which was similar to the results of another experiment. 22 After a week of FSN treatment, CS and mitochondrial complex II in the mitochondrial structure improved compared with the MOD and ACP groups. The CS contents in the FSN, ACP, and MOD groups were 8.66 ± 0.51, 7.79 ± 0.34, and 7.05 ± 0.39, respectively. The CS content in the FSN group was significantly higher compared with those in the ACP and MOD groups. This key enzyme reflects the activity and intensity of mitochondrial energy metabolism. After FSN treatment, the expression of mitochondrial COX- I protein in the muscle tissue increased. The COX- I protein activities in the FSN, ACP, and MOD groups were 1.03 ± 0.80, 0.57 ± 0.23, and 0.52 ± 0.19. The FSN group had significantly higher COX- I protein than the other two groups. COX- I protein expression is closely related to mitochondrial function and cell energy production. These results have a good response to the effect of FSN on muscles.
After peripheral nerve injury, muscle denervation can lead to skeletal muscle atrophy and inactivation and reduce the contractile and metabolic functions of the skeletal muscle. 22 In the CCI rat model, the nutritional function of the corresponding innervated muscle decreases after ligation of sciatic nerve causes nerve damage, and metabolic abnormalities, such as the waste produced by muscle tissue produce energy crisis slowly forms pathological muscles (i.e. TM). Continuous TM causes pain. FSN and acupuncture target the connective tissue, which does not directly act on the damaged nerve and muscle parts but has also produced good results in clinic. In the many clinical neurological diseases, the main problem lies in the muscle rather than the nerve itself, which is worthy of our discussion. Therefore, in the sciatica rat model, this experiment changed the mitochondrial structures and function of muscles under the treatment of FSN to study the treatment mechanism of FSN for chronic pain diseases. The theory of traditional Chinese medicine and the research of modern histopathology and molecular biology have made great progress, which provides certain conditions for the discussion of the mechanism of FSN therapy. Mechanical connective tissue reaction instead of neural mechanism in FSN treatment was first investigated in a rabbit model on 2012. 23 This hypothesis was also supported in the study via Langevin and her colleagues. 24 Fascia theory holds that connective tissues have the functions of connection, nutrition, transportation, and defense but also has the functions of support and reserve. It can repair the body by stimulating fascia connective tissue. 25 Previous experiments showed that stimulating the fibers in connective tissue through mechanical traction can restore the disordered connective tissue fibers in the disease state to the arrangement state consistent with the stress direction, but it can also drive changes in cell morphology and cytoskeleton in the reticular scaffold through mechanical traction to transmit the extracellular mechanical signal to the cells. The change in connective tissue cell signal transduction resulted in the change of relevant cytokine concentration, caused the change of cell microenvironment, and finally promoted the body to return to equilibrium.26–27 FSN therapy has immediate, short-term and long-term effects on diseases. 28
The mitochondria exist in muscles, whereas the FSN acts on connective tissue. When FSN was removed from the animal body, it always does not look so smooth on the needle head, which is similar to something with small debris. An electron microscope study found that when the acupuncture needle was lifted, inserted, and twisted in the human body. The acupuncture needle was removed, and debris was found on the acupuncture needle, revealing that connective tissues, such as elastic fibers and collagen fibers were wound around the needle. 28 Connective tissue includes loose connective tissue, such as subcutaneous tissue and dense connective tissue, such as tendon. Connective tissue is generally composed of cells, fibers, and extracellular stroma. In cells, it includes common fibroblasts, adipocytes, and mesenchymal cells, as well as some uncertain macrophages, plasma cells, mast cells, and white blood cells exuded from blood. When the FSN was inserted into the skin, it had an important impact on the connective tissue, which enhanced the mechanical coupling between the needle and the connective tissue. The swaying movement of the FSN and the lifting, inserting, and twisting method of the needle continuously enhance this mechanical coupling. Acupuncture can transmit mechanical signals to connective tissue through this mechanical coupling. 24 The downstream effects of mechanical signals may include the synthesis and local release of growth factors, cytokines, vasoactive substances, degrading enzymes, and structural matrix elements. The release of these substances may affect the extracellular environment around connective tissue cells. 29 It may be related to reducing pain. However, at present, little is known about the innervation of connective tissue, and fully explaining why FSN entering the connective tissue can produce a good analgesic effect is impossible. However, fascia, especially extramuscular fascia and aponeurosis fascia, is recently considered a small straight fiber with high innervation, which can transmit nociceptive signals, especially in the presence of inflammation.30-32 Determining how much pressure and tension the connective tissue is under to produce a good painless feeling is also difficult. These factors need further study.
As the center of cell energy and material metabolism, the oxidative phosphorylation reaction on the respiratory chain of the mitochondria supplies energy for muscle contraction and other life activities and controls cell survival by producing adenosine triphosphate (ATP), which provides fuel for cell processes. In turn, it induces cell death by releasing pro-apoptotic factors, such as cytochrome C. Its fusion and division are the manifestations of mitochondrial dynamics. Mitochondrial fusion and division are the key to maintain the normal morphological structure and dynamic function of the mitochondria. Fusion and division come first, and apoptosis comes later. 33 Mitochondrial dynamics shapes the morphological structure of the mitochondria, which is closely related to mitochondrial dynamics and affects the metabolism of cell energy and the occurrence of autophagy and apoptosis. 33 The timely removal of damaged mitochondria through mitochondrial autophagy is very important for cell balance and function. The best predictor of mitochondrial content is mitochondrial CS activity, followed by complex I activity and complex II protein content. CS is a marker enzyme that reflects the structural integrity of the mitochondria, and its content directly reflects the number of surviving mitochondria in tissues. 34 Mitochondrial complex II, also known as succinate dehydrogenase, is a central provider of metabolic and respiratory adaptation reprogramming. It is a marker enzyme reflecting mitochondrial function. Its activity can be used as an index to evaluate the level of intracellular energy (i.e., ATP synthesis). The present study was found that FSN and acupuncture treatment for rats with chronic pain improved the morphological structure of the mitochondria and the expression of related proteins to a certain extent.
Mitochondrial structural damage and dysfunction have an important impact on the neurological diseases of the central and peripheral nervous systems. 35 The role of mitochondrial dysfunction in the pathogenesis of chronic pain is exerted through the five functions of the mitochondria, namely, mitochondrial energy generation system, reactive oxygen species (ROS) generation, mitochondrial permeability transition pore (MPTP), apoptosis pathway, and intracellular calcium mobilization. 36 Mitochondrial energy generation system is mainly completed by tricarboxylic acid cycle and mitochondrial electron transport chain. ATP is produced by enzymes on the electron transport chain through a series of reactions. Enzymes on the mitochondrial respiratory chain are closely related to the generation of pain. 37 ROS are generated when electrons in the mitochondrial respiratory chain leak out of the respiratory chain and consume about 2% of oxygen before being transferred to the terminal oxidase. The electron flux in the respiratory chain determines the amount of ROS generated. ROS include highly reactive species, such as hydroxyl radical (•OH), and weakly reactive species, such as superoxide (O2• −), which are the by-products of oxidative phosphorylation.38–39 To some extent, ROS participate in mitochondrial autophagy, the homeostasis of mitochondrial environment, and signal transduction. However, when the increase in ROS exceeds the antioxidant capacity of the mitochondria, excessive ROS will damage the morphological structure of the mitochondria, endanger cell function, and produce irreversible damage. ROS are also involved in persistent pain.39–42 Mitochondrial permeability transition pore (MPTP) is a group of protein complexes existing between the inner and outer membranes of the mitochondria. It is a non-specific channel. MPTP plays an important role in cell survival and apoptosis. It involves many fields, such as ischemia/reperfusion, tumor, aging, and neurodegeneration. 43 Mitochondrial permeability transition is closely related to pain. Inhibiting the opening of mitochondrial permeability may contribute to mitochondrial homeostasis. Apoptosis is a kind of programmed cell death, which occurs due to the production of several catabolic enzymes. In this process, some morphological and biochemical changes have taken place in the mitochondria. The mitochondria are the main organelles involved in apoptosis and control the apoptotic pathways in cells.44–45 FSN therapy acts on the connective tissue closely related to the muscle tissue. Through the continuous traction of connective tissues, FSN improves the cell and the extracellular environment of connective tissue, and improves the energy system of the muscle tissue (mitochondria) through the transmission of mechanical signals between tissues, which provides a theoretical basis for the FSN therapy of chronic pain diseases, it also provides ideas for the continuous development of FSN in the future.
Conclusion
The use of FSN treatment for chronic pain can improve the morphological structure and function of the mitochondria in the tightened muscle, increase the content of mitochondrial CS and Complex II, increase the active expression of COX- I protein in the muscle tissue, improve muscle energy metabolism, and relieve muscle pain in rats. These effects are related to the signal transduction of the connective tissue and muscle and the release of energy crisis. FSN therapy can remarkably improve this kind of neuropathic pain and promote the recovery of damaged nerves and muscles.
Footnotes
Author contributions
Yaping Li performed the animal experiment, analyzed the data and wrote the original draft and performed immunoprecipitation experiment; Xianghui Gao performed the transmission electron microscope work and wrote the original draft; Xiyan Zhou performed the pain threshold, analyzed the data and reviewed and edited the manuscript; Hailiang Huang performed the animal experiment and analyzed the data; Yunhua Zang reviewed and edited the manuscript; Li-Wei Chou reviewed and edited the manuscript and provided guidance and advice.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Qingdao 2018 medical research guidance plan (Project No: 2018-WJZD031) and Asia University Hospital (11051004).
Data availability
The data that support the findings of this study are available from the corresponding author, upon reasonable request.