
Abstract
Acupuncture at pericardium 6 (PC6) shows a consistently positive efficacy in nausea response suggested by consensus expert guidelines. Nausea encompasses aversive symptom as well as strong emotional components. Disgust is a subjective emotion of uneasy commonly accompanying with a physiological response that is accompanied by strong visceral sensations (e.g., nausea). Understanding the brain circuitry by which acupuncture influences the disgust emotion may further elucidate the modulation effect of acupuncture on aversive experience. In the present study, a well-established aversive conditioning model on healthy subjects was combined with acupuncture intervention at PC6, as well as different acupoints (both local PC7 and distant GB37) as separate controls, to investigate the brain network involved aversive regulation with acupuncture; 48 healthy subjects were enrolled and randomized into four parallel groups: group 1 received disgust-induced (DI) stimuli only; groups 2, 3, and 4 received acupuncture at three single acupoints separately prior to the DI. Disgust sensations were rated at baseline and following disgust stimuli. Acupuncture PC6 can induce significant attenuations in disgust sensations than that of no intervention and acupuncture at other acupoints. Neuroimaging further showed that increased causal interaction strength between the cerebellum (nodulus) and insula can predict greater attenuations in aversive experiences. We also found evidence for radical reorganizations of local stronger casual interaction patterns to disgust-induced brain responses targeted by acupuncture at different acupoints. This study provided the brain substrate for acupuncture on aversion modulation. The coupling between the cerebellum (nodulus) and insula supported interoception system and vestibular control which provided the specific neural basis.
Keywords
Introduction
The use of acupuncture in the treatment of psychological disorders has increased considerably, especially for affective regulations. 1 One review has identified acupuncture at pericardium 6 (PC6) as one of the most frequently used points in this effective treatment regimen. 2 Moreover, acupuncture PC6 has also been proposed as a recommendable option to prevent nausea and vomiting (especially for surgery and associated with chemotherapy) suggested by consensus expert guidelines.3–7 However, the neurophysiological mechanism by which acupuncture influences the desired outcome remains unclear, partly due to complex confound factors from the variable pathology and multiple-drug combination in these patients. Nausea encompasses aversive symptom as well as strong emotional components. 8 Previous study has identified the interaction of emotional state and nausea experience. 9 Disgust is an aversive emotion commonly accompanying with a physiological response of salient visceral sensations (e.g., nausea). Understanding the brain circuitry by which acupuncture influenced the disgust emotion modulation may further elucidate its antiemetic effect through aversive experience regulation.
Acupuncture, an ancient healing technique, overlaps significantly with these disgust-induced (DI) brain areas mainly involved the limbic-cerebellar system.10,11 Studies on the neural basis of disgust revealed the important role of the insula in processing and integrating visceral information. 12 One recent study has also discovered that the neural loss in the insula was associated with the diminished disgust responding in both self-report and physiological reactivity. 13 Moreover, activation of the cerebellum in the regulation of affective processes is also in agreement with an increasing number of clinical and neuroimaging reports that relate the cerebellum to emotional control in health and in disease.14–17 This function is supported by its neuroanatomical foundation with intimate afferent and efferent connection to the brainstem and limbic system. 18 Accumulated neuroimaging studies further suggest that modulation of the insula and cerebellum may constitute an important pathway of acupuncture action.19–22 Our previous study also indicates that the cerebellar nodulus, participating in the vestibular control, has been identified as important activation loci modulated by acupuncture stimulation at PC6. 23 This study provides further evidence that antiemetic effect of acupuncture PC6 may be mediated by the cerebellar vestibular neuromatrix.
The present study adopted a well-established aversive conditioning model on healthy subjects to assess whether (i) the disgust sensation can be attenuated with acupuncture PC6 intervention, compared with no intervention in DI stimuli group and (ii) acupuncture at PC6 has the relative functional specificity in aversive regulation, whose effect may be superior to acupuncture at PC7 (belonging to the same meridian and median innervation as PC6) and acupuncture at GB37 (distant body sites, located at different meridian for PC6). Of note, one study indicated the potential effects of acupuncture PC6 on gastric myoelectrical activity, vagal modulation, and cerebellar vestibular activities in functional magnetic resonance imaging (fMRI), 24 which may be related with its function of regulating nausea and vomiting. We further hypothesized that the insula and cerebellum, centrally implicated in the interoception system and vestibular control, may be crucial neural substrate underlying the antiemetic effects of PC6 on aversive experience regulation.
Materials and methods
Subjects
All the subjects were recruited from a homogeneous group of 48 college students (24 males, ages of 20.3 ± 1.2). They were all acupuncture naïve and right-handed healthy subjects according to the Edinburgh Handedness Inventory. 25 Exclusion criteria included the major medical illnesses, head trauma, neuropsychiatric disorders, intake of prescription medications within the two weeks, previous acupuncture experience, and any contraindications for exposure to a high magnetic field. Considering that nausea induced by disgust can easily be affected by various psychological factors, such as anxiety, disgust sensitivity and suggestibility, 26 each participant filled in four trait questionnaires concerning disgust (Questionnaire for the Assessment of Disgust Sensitivity, QADS), 27 anxiety (State Trait Anxiety Inventory, STAI), 28 depression (Beck Depression Inventory) 29 and suggestibility. 30 Only subject with normative levels for these psychological factors can be included. 31 In the case of the women, the experiments were performed outside the catamenial period, leaving three days on either side, with the aim of avoiding possible hormonal influence on the affective states.32,33 The experiment was approved by a Tiantan Hospital subcommittee on Human Studies and conducted in accordance with the guidelines of Declaration of Helsinki. Written informed consent was obtained from all the subjects.
Experimental paradigm
This was a randomized, controlled, single-blinded, and parallel-group study. On commencing the study, an envelope method was used to allocate subjects into four groups with 12 subjects on average, and each group only receive acupuncture treatment at one of the three acupoints and non-treatment prior to disgust stimuli in a random sequence. There were no significant differences in the ages, sex, and educational levels among these four groups (ANOVA, P > 0.1). In order to control the potential effects on disgust reactions, factors such as the gender, disgust sensitivity, depression, trait anxiety, and suggestibility were all balanced across the four groups (ANOVA, P > 0.6). Group 1 received the disgust stimuli only and groups 2, 3, and 4 received acupuncture at three single acupoint separately prior to the disgust stimuli (PC6 as the study group, and PC7 and GB37 as separate controls for both local and distant site comparison, respectively) (Figure 1).
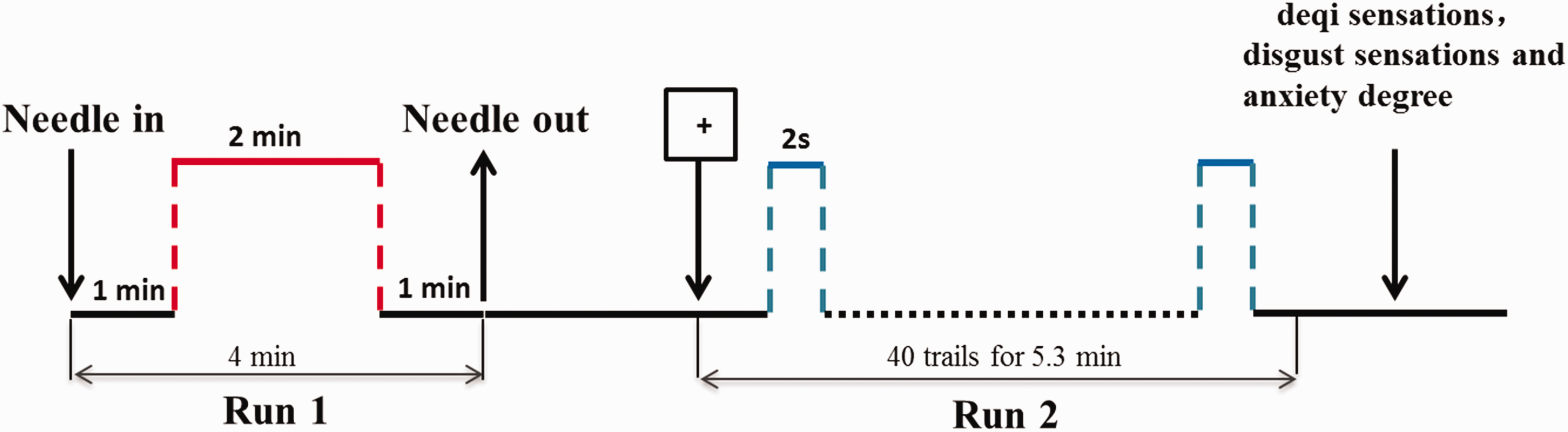
Experimental design. Run 1: A non-repeated event-related (NRER) fMRI acupuncture run for 4 min, including 2-min needling manipulations preceded by a 1-min rest, and followed by another 1 min rest scanning. Run 2: Disgust stimulus tasks were presented using a rapid event-related design; 20 trials for each type (disgust and neutral pictures) and 40 null trials (fixation cross) were presented in a random order. Group 1 conducted the disgust stimuli only and groups 2, 3, and 4 received acupuncture treatment first and then disgust stimuli. After each fMRI scanning, deqi sensations, disgust sensations, and anxiety degree were assessed using a 10-point visual analogue scale (VAS) across the four groups.
Session 1
Prior to the fMRI scanning, we conducted the first behavioral session to determine the appropriate pictures for both disgust and neutral stimuli, in order to control cultural differences in disgust elicitors. Affective stimulation was performed with pictures from the International Affective Picture System (IAPS) 34 that was validated also in a German population. 35 Considering that cultural evolution of disgust has involved a flexible and expanding elicitor system, we held that cultural differences in disgust may be associated with the evaluative system. In a prior behavioral study, an independent group of 200 Chinese college subjects categorized a set of IAPS pictures for their basic emotional valence, such as disgust, fear, sadness, happiness, and neutral content. They also rated the dimensions of valence, arousal, and dominance for both disgust and neutral pictures from IAPS, by using a pencil-and-paper version of the Self-Assessment Manikin rating system (SAM). 36 Only those disgust and neutral pictures with no difference ratings from our test compared with the normative ratings stemmed from the IAPS and consistently categorized by all subjects were selected as candidates in this experiment. Stimuli pictures were also matched according to both content and complexity; 20 disgust and 20 neutral pictures were finally determined. Disgust pictures included animals, physical deviations/death, poor hygiene, rotten food, and body products. And neutral picture displayed animals, furniture, and everyday life scenes with one or more persons. A pseudo-randomized order was created with the limitation that any condition did not occur more than three times consecutively.
Session 2
Session 2 was performed in the fMRI scanner to elucidate the modulatory acupuncture effect on brain responses to disgust stimuli. For group 1, the affective stimulus tasks were presented using a rapid event-related design; 20 trials for each type (disgust and neutral pictures) and 40 null trials (fixation cross) were presented in a random order. A fixation cross was presented with a mean of 4.5 s in an attempt to randomize the stimulus onset asynchrony in a geometric distribution; then a picture was present for 2 s. Jittering trial timing in this way increases the detestability of task-related responses in event-related fMRI and is most efficient using a geometric distribution. For emotional stimuli, a stimulus onset asynchrony with a mean of 4.5 s maximizes trial presentation rate while minimizing response attenuation due to stimulus repetition.
For group 2, 3, and 4, subjects first endured a non-repeated event-related fMRI acupuncture run for 4 min, including 2-min needling manipulations preceded by a 1-min rest, and followed by another 1-min rest scanning.37,38 Acupuncture was performed on different acupoint for three groups, respectively (shown in Figure 2): PC6 located approximately 3 cm above the midpoint of the transverse crease of the wrist, between the tendon of palmaris longus and flexor carpiradialis; PC7 (also called Daling, as indications for depressive psychosis and palpitation) at the midpoint of the crease of the wrist, between the tendons of the long palmar muscle and radial flexor muscle; 3 and GB37 located in the lateral aspect of the lower leg, with needle being inserted on the anterior border of the fibula. Acupuncture stimulation was delivered using a sterile disposable 38-gauge stainless steel acupuncture needle, 0.2 mm in diameter and 40 mm in length. Considering the anatomical differences, the needling depth ranged from 0.5–1.0 cm for both PC6 and PC7 to 1.5–2.0 cm for GB37. The needle administration was delivered by a balanced “tonifying and reducing” technique, 11 rotating clockwise and counterclockwise for 1 min at a rate of 60 times per min. The procedure was performed by the same experienced and licensed acupuncturist on all subjects. The precise locations of needling, the presumed acupuncture effects, and the stimulation paradigm were not divulged. During the experiment, the subjects were requested to keep their eyes closed and remain relaxed without engaging in any mental tasks. After acupuncture treatment, three groups all received the disgust stimuli, all of which was the same as conducted in group 1. Disgust sensations and anxiety degree were assessed using a 10-point visual analogue scale (VAS) before and after fMRI scanning across the four groups.

Illustration of anatomical locations of three acupoints: PC6 (Neiguan), PC7 (Daling), and GB37 (Guangming).
Session 3
The second behavioral session was designed to measure the psychophysical sensations during the acupuncture stimuli and to detect whether the ratings of pictures given by all the subjects in the task were consistently classified as disgust and neutral, respectively. At the end of each fMRI scanning, the subjects completed a questionnaire that used a 10-point VAS to rate their experience (or “deqi”) of aching, pressure, soreness, heaviness, fullness, warmth, coolness, numbness, tingling, dull, or sharp pain they felt during the scan.9,21 The VAS was scaled at 0 = no sensation, 1–3 = mild, 4–6 = moderate, 7–8 = strong, 9 = severe, and 10 = unbearable sensation. They also rated their feelings for the 40 pictures selected from IAPS in terms of valence (how pleasant/unpleasant), arousal (how calm/excited), and dominance (how controlled/in-control) on the SAM. SAM has been used effectively to measure emotional responses by using a nine-point graphic rating scale of all three dimensions.
fMRI data acquisition and analysis
The images were acquired on a 3T GE Signa scanner. A custom-built head holder was used to prevent head movements. Thirty-two axial slices (FOV = 240 mm × 240 mm, matrix = 64 × 64, thickness = 5 mm), parallel to the AC-PC plane and covering the whole brain, were obtained using a T2-weighted single-shot, gradient-recalled echo planar imaging sequence (TR = 2000 ms, TE = 30 ms, flip angle = 90°). Prior to the functional run, high-resolution structural information on each subject was also acquired using 3D MRI sequences with a voxel size of 1 mm3 for anatomical localization (TR = 2.7 s, TE = 3.39 ms, matrix = 256 × 256, FOV = 256 mm × 256 mm, flip angle = 7°, slice thickness = 1 mm).
All preprocessing steps were carried out using statistical parametric mapping (SPM 8, http://www.fil.ion.ucl.ac.uk/spm/). The images data first underwent slice-timing correction and then realigned to correct for head motions (none of the subjects had head movements exceeding 1.5 mm on any axis and head rotation greater than 1°). The images data were further processed with spatial normalization based on the montreal neurological institute (MNI) space and resampled at 2 mm × 2 mm × 2 mm. Finally, the functional images were spatially smoothed with a 6-mm full-width-at-half maximum Gaussian kernel. The statistics were color-coded and normalized to the standard Talairach-Daemon-based atlas. 39
For each subject, fMRI signal differences induced by disgust stimuli were estimated at every voxel across the whole brain by a general linear model in SPM8. Then, we compared brain fMRI changes between the two conditions (disgust vs. neural) within the DI group by using a one sample t-test. Further, three between-group comparisons of fMRI signal changes during the DI stimuli (disgust minus neural) were calculated by using a two sample t-test separately (PC6 vs. DI, PC7 vs. DI, and GB37 vs. DI).
Definition of region of interest
fMRI signal differences evoked by disgust stimuli for each subject were obtained by general linear model. First, we calculated the BOLD response changes in the rapid event-related design of disgust stimulus tasks with two conditions (disgust vs. neural), yielding a statistical significant map of brain activation (P < 0.01, false discovery rate [FDR] corrected) and thereby selecting 13 brain regions as the regions of interest (ROIs) for the following multivariate Granger causality analysis (mGCA) analysis. The spherical ROIs were centered on the local peak voxels with a set of voxels included in 6-mm (in radius) spheres. For bilaterally activated regions, we only selected the unilateral hemisphere area with a more significant “Z-score” as the representative ROI. Then, the time series of BOLD signal intensities were extracted by averaging across voxels within each ROI. Finally, the mean time course across subjects within each group (disgust stimuli task) was normalized to form a single vector per ROI which then served as the inputs for mGCA.
Multivariate Granger causality analysis
In the current study, we used mGCA for detecting casual interactions between brain regions during disgust stimuli task. The mGCA was conducted by the computing directed transfer function (DTF), generated from a multivariate autoregressive model of the time series on the selected ROIs. 40 In this study, we also adopted the direct DTF (dDTF) with partial coherence in order to emphasize direct connections and inhibit mediated influences. Based on the principle of Granger causality, the dDTF can reflect the magnitude of causal influence between the ROIs. The algorithm was coded in MATLAB version 7.0 (The Math Works, Inc.). 37 Effective connectivity graphs were constructed using the thickness of connecting lines and arrows to indicate the strength and direction of the causal influences. Graphs were visualized using Pajek software (http://vlado.fmf.uni-lj.si/pub/networks/pajek/).
Local-enhanced causal interaction pattern in the network
A causal connectivity graph was constructed using the thickness of connecting lines to indicate the strengths of the causal influences. Only links that showed significant effective connectivity were presented in the network (P < 0.05, FDR corrected). The brain nodes that connect with the top two of the strongest casual influence were classified as central nodes, constituting the local-enhanced causal interaction pattern in the network.
Correlation between network parameters and the clinical measures
To identify brain network parameters significantly associated with the clinical measures, a correlation analysis was performed. We calculated the cross-subject correlation between the interregional causal strength and disgust sensations as well as anxiety degree, respectively, using Pearson’s correlative analysis with SPSS statistical software (version 20.0).
Results
Psychophysical results
The prevalence of deqi sensations was expressed as the percentage of the individuals in the group that reported the given sensations (Figure 3(a)). All the subjects experienced three types of psychophysical sensations during the acupuncture stimuli, with the frequency of soreness (PC6: 41.6% of subjects; PC7: 16%; GB37: 25%), numbness (PC6: 75% of subjects; PC7: 58.3%; GB37: 41.6%), and fullness (PC6: 75% of subjects; PC7: 75%; GB37: 50%). When grouped across all acupuncture acupoints, no difference was found in regard to the prevalence of the listed sensations or the type of sensations under Fisher’s exact test (P > 0.05). The intensity of sensations was expressed as the average score ± SE (Figure 3(b)). The average stimulus intensities (mean ± SE) were approximately similar during acupuncture on PC6 (3.65 ± 0.40), PC7 (4.22 ± 0.61), and GB37 (3.5 ± 0.51) under the analyses of variance test (P > 0.05). In addition, no significant difference was found with respect to the type of sensations (P > 0.1). Considering no significant difference in psychophysical response among three acupuncture groups, the neuroimaging findings were likely not the results of differences induced by the sensations.
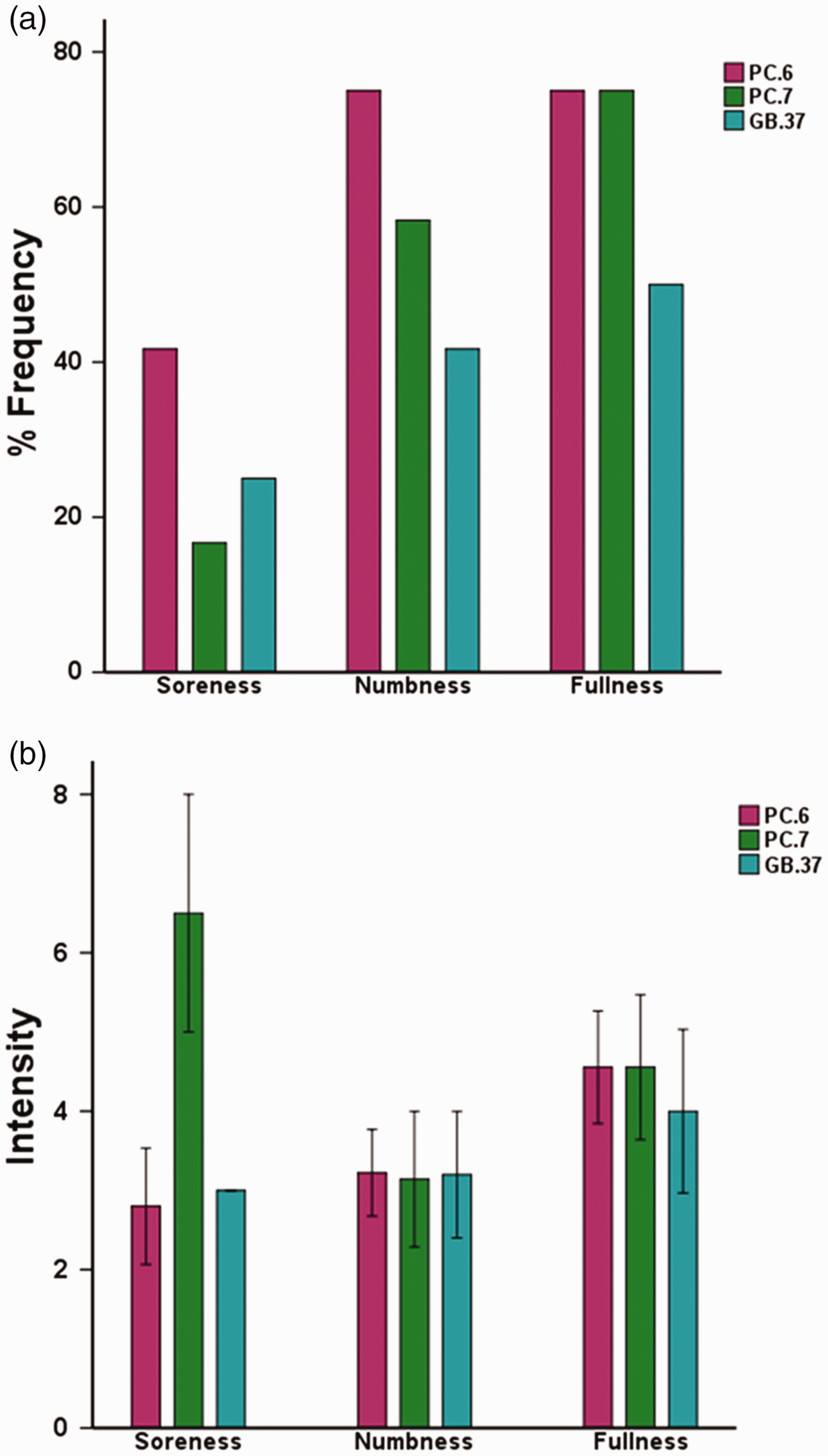
Averaged psychophysical response (N = 48). (a) The percentage of subjects who reported having experienced the given sensation (at least one subject experienced the seven sensations listed). (b) The intensity of reported sensations measured by an average score (with standard error bars) on a scale from 0 denoting no sensation to 10 denoting an unbearable sensation.
Subjective ratings of disgust sensations and anxiety degree
The two sample t-tests results showed that the acupuncture PC6 induced significant reductions in disgust sensation scales, compared with that of the DI stimuli group (P = 0.038), as well as acupuncture at PC7 (P = 0.048) or GB37 group (P = 0.041). There was also non-significant trend in the reduction of anxiety degree following acupuncture at PC6 (P = 0.051), compared with that of no intervention. Nevertheless, no significant differences were found for other contrast in both disgust sensations and anxiety degree at baseline and following disgust stimuli (P > 0.1). Thus, this analysis found that the disgust sensation only can be attenuated with acupuncture PC6 intervention.
fMRI results
Brain fMRI changes (disgust vs. neural) in DI group and three between-group comparisons (PC6 vs. DI, PC7 vs. DI, and GB37 vs. DI) were shown in Figure 4. The contrast disgust > neutral in DI group showed that disgust stimuli induced significant brain activations in the following regions: the hippocampus, thalamus, caudate, anterior cingulate cortex (ACC), medial prefrontal cortex, orbitofrontal cortex (OFC), supper occipital gyrus (SOG), primary somatosensory cortex, supplementary motor area, insula, and putamen (P < 0.01, FDR corrected). Acupuncture at PC6 produced significantly less activations in response to the disgust stimuli than that of DI group (with no intervention), including the flocculonodular lobe of cerebellum (nodulus and uvula), amygdala, insula, and hypothalamus. Additionally, significantly less brain activations were observed following acupuncture at PC7 compared with that of DI group, primarily in the brainstem structures (periaqueductal gray, PAG, and pons). In contrast, acupuncture at GB37 elicited greater fMRI signal increases evoked by disgust stimuli located within the vision-related occipital cortex, in comparison with that of the DI group. Statistical significance was thresholded at P < 0.05, uncorrected with 10 contiguous voxels.

Comparison results from PC6 vs. DI, PC7 vs. DI, and GB37 vs. DI under the disgust stimuli task. Statistical significance was thresholded at P < 0.05 (uncorrected) and a minimum cluster size of 10 voxels. PAG: periaqueductal gray; DI: disgust induced.
mGCA mapping
In this study, we investigate the brain network during disgust stimuli task for these four groups, respectively. The effective connectivity patterns for disgust stimuli were described as directed graphs. The thickness of connecting lines and the directions of arrows indicated strength and directions of the causal influences, respectively (Figure 5). Significant effective connectivity (P < 0.05, FDR corrected) was divided into four levels (25%, 50%, 75%, and 100%) relative to the maximum casual strength.

Multivariate Granger causality relationships with significant connections (P < 0.05, FDR corrected) during disgust-induced stimuli following non-treatment and acupuncture at PC6, PC7, and GB37. Relative strength of path weights (in arbitrary units) was indicated by the width of the arrows. Phipp: hippocampus; ACC: anterior cingulate cortex; MPFC: medial prefrontal cortex; OFC: orbitofrontal cortex; SOG: supper occipital gyrus; SI: primary somatosensory cortex; SMA: supplementary motor area.
DI stimuli of DI group can induce extensive causal interactions of the wide brain areas primarily located in the limbic/paralimbic-cerebellum and subcortical areas. Notably, significant bidirectional regulation was forged between the nodulus and OFC. The nodulus projected the casual outflows to almost all other nodes in the brain network, including the ACC, hippocampus, thalamus, supplementary motor area, putamen, OFC, and medial prefrontal cortex. Additionally, the strongest casual influence originated from the ACC to the hippocampus.
Furthermore, the between-group analysis showed that the distinct local-enhanced casual interaction patterns were specifically constructed in the DI brain network following acupuncture at different acupoints. Following acupuncture at PC6, the nodulus sent the strongest outflow influences to the insula, and a bidirectional casual connection with maximal strength was emerged between the nodulus and hippocampus. Moreover, following acupuncture at PC7, the top two strongest casual outflow influences were detected from the amygdala to the hippocampus and ACC, respectively. By contrast, following acupuncture at GB37, intensive network connections during disgust stimuli task were primarily located within the vision-related cortex. The SOG emerged as a central network node receiving the strongest causal inflow from the ACC, and the maximal bidirectional casual influence was found between SOG and amygdala. Of interest, the strong nodule-insula causal connectivity only occurred during the disgust stimuli following acupuncture at PC6 compared with PC7 and GB37.
Correlation between network parameters and the clinical measures
Correlation results presented that increased causal interaction between the nodulus and insula can predict the greater attenuation of disgust sensation only following acupuncture PC6 (r = −0.71, P = 0.01). Other correlations were not significant (P > 0.1). The enhanced coupling between the cerebellum (nodulus) and insula was associated with aversion regulation modulated by acupuncture PC6.
Discussion
The present study investigated the specific neural circuits supporting acupuncture mechanisms for aversive experience modulation induced by disgust stimuli in healthy subjects. Our results demonstrated that acupuncture at PC6 is especially effective for alleviating subjective disgust sensations compared with that of no intervention group and the other two acupuncture intervention groups (PC7 and GB37). Neuroimaging findings have further identified that the enhancement of causal influence strength from the cerebellum (nodulus) to insula predicted greater attenuations in aversion responses following acupuncture PC6 intervention. Moreover, we found evidence for a radical reorganization of local stronger casual interaction patterns to DI brain responses targeted by acupuncture at different acupoints, implying a distributed core brain connectivity pattern underlying acupuncture modulation for different acupoints. The coupling between the cerebellum (nodulus) and insula may support the interoception system and vestibular control as a specific neural basis underlying the aversion regulation by acupuncture PC6.
Our findings presented that increased causal interaction between the cerebellum (nodulus) and insula can predict the greater attenuation of disgust sensation only following acupuncture PC6. Of note, the nodulus also became an important node in the brain network, the maximal strength of path weight projecting from the nodulus to insula. The nodulus, located in the flocculonodular lobe as part of the vestibule cerebellum, receives vestibular projections from primary and secondary vestibular afferents as well as vestibular climbing fibers, 41 which contributes to the vestibular information perception via vestibular cortical pathways. 42 Furthermore, previous work has indicated that the insula responds selectively to a broad range of disgust-related stimuli (disgust-inducing pictures, unpleasant odors, disgusted facial expressions, etc.),43,44 considering as a specific brain locus for regulating gustatory and visceral motor functions including the control of nausea and vomiting. 45
Interestingly, Turner and his team demonstrated that the normal experience of unpleasant emotional stimuli among patients with cerebellar damage was achieved in association with increased recruitment of prefrontal and insula regions. 46 These findings suggested that there may exist coherent relationship of brain responses between the cerebellum and insula in the processing of aversion emotion. Along this line, we also detected that the strongest causal interaction between the nodulus and insula to disgust response only constructed following acupuncture PC6 intervention. Such enhancement of connectivity strength can also predict greater attenuations in aversion responses. Hence, the causal interaction between these structures may support the interoception system and vestibular control as a specific neural basis underpinning the aversion regulation of PC6 acupuncture.
Even as acupuncture intervention performed as the local site control (PC7), there existed differential causal interaction of brain areas compared with that of acupuncture PC6. The local-enhanced causal interaction pattern was exclusively located at the amygdala, ACC, and hippocampus. Notably, these regions, as part of the limbic system, play a dominant role in the affective encoding.47,48 From this point of view, PC7 can exert modulatory effects on emotion processing, thereby achieving its clinical beneficial for mental and psychosomatic disorders. 49 GB37 (an acupoint of the gallbladder channel) serves as the distal site with respect to PC6, as its name “brightness” suggests, which is considered as an effective acupoint for vision-related disorders treatment.50,51 Following acupuncture at GB37, mGCA results showed that the strong casual interaction pattern were occurred among the SOG, amygdala, and ACC. The SOG became an important node with strong casual influences with other brain regions. The SOG, as the primary visual cortex, is proposed to serve the vision-related processing.51,52 Results indicated that acupuncture stimulation at GB37 as a different meridian control can elicit distinct dynamic reorganization of effective connectivity pattern compared with PC6 and PC7, maybe pertinent to its specific curative efficacy in clinical settings.
A recently updated meta-analysis involving 7667 participants in 59 trials have found that PC6 acupoint stimulation was more effective than sham treatment for preventing the postoperative nausea and vomiting with minimal adverse events; the efficacy to prevent postoperative nausea and vomiting was similar between PC6 stimulation and antiemetic drugs. 53 However, the neurophysiological mechanism by which acupuncture influences the desired outcome remains unclear, partly due to complex confound factors from the variable pathology and multiple-drug combination in these patients. The current study, modeling aversion responses on healthy subjects, has led to the possibility of understanding the brain circuitry by which acupuncture influences the desired outcome on aversive experience. Our results have provided preliminary evidence to support that the interoception system and vestibular control engaged the attenuation of aversion responses by acupuncture PC6. The effective connectivity between the vestibule cerebellum and insula may become a valuable neural biomarker to predict clinical antiemetic effect of acupuncture PC6 treatment. Interestingly, we also found evidence for a radical reorganization of local strong casual interaction patterns to DI brain responses following acupuncture intervention at different acupoints, implying a specific effective connectivity pattern underlying function network organization.
Footnotes
Acknowledgment
The authors would like to thank Yijun Liu for his assistance in study design and revising the manuscript for content.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Natural Science Foundation of China (Grant Nos. 81571752, 81771914, 81473667, and 81072773), National key research and development plan of China (2016YFC0100300), Shaanxi Nova Program (2014KJXX-34), and Science and Technology Planning Project of Guangdong Province (2016A020215202).