
Abstract
Involuntary care in intellectual disability care may be reduced by deployment of multidisciplinary consultation. The Multi-Disciplinary Expertise Team (MDET) method proved effective in a previous trial on increasing involuntary care reduction. The current study aimed to examine how four organizations adapted MDET during implementation, and tested whether these versions were also effective. Semi-structured interviews with MDET-coordinators were analyzed using the Framework Reporting Adaptions and Modifications-Expanded. A quasi-experimental interrupted time-series design tested change in weekly counts of involuntary care recordings from before to during MDET implementation, in care homes that implemented MDET (n = 24) compared to care homes providing care-as-usual (CAU). Adaptations to MDET varied. These included implementing MDET without an independent MDET-team and loosening recordings of involuntary care. No differential changes in recordings were found between the implementation- and CAU-groups. Scaling-out MDET to other organizations led to adaptations that may have undermined its effects on reducing involuntary care.
Introduction
Long-term care organizations for people with intellectual disabilities provide care to clients who might have complex needs for care, support and treatment. These complex needs may arise from additional disabilities such as visual, hearing, and motor impairments (Vlaskamp et al., 2007), as well as from challenging behavior, for example apathetic, destructive, aggressive or self-harming behavior (Emerson and Einfeld, 2011). To protect clients with intellectual disabilities, direct care staff and their surroundings in unsafe situations, care professionals may apply involuntary care. Examples of involuntary care include restrictive and coercive measures, such as pulling wheelchair brakes, seclusion, fixation or locked doors and cabinets (Schippers et al., 2018). In the Netherlands, care professionals are obliged under the Convention on the Rights of Persons with Disabilities (CRPD) (United Nations, 2006) and the Care and Coercion Act (CCA) (Staatsblad, 2018) to respect and uphold clients’ right to self-determination and apply involuntary care minimally and as briefly as possible. The organizations in which care professionals work are obliged to support care professionals to this end.
Care needs of people with intellectual disabilities are complex, challenging behavior is multidetermined (Hastings et al., 2013; Poppes et al., 2010), and involuntary care can take many shapes and forms (Schippers et al., 2018). Therefore, phasing out involuntary care requires multidisciplinary expertise. For that purpose, the Multi-Disciplinary Expertise Team (MDET) method was developed and proven effective in a randomized controlled trial (Schippers et al., 2024). However, being effective in one care organization does not guarantee effectiveness when scaling out the method to other care organizations, because contexts of these organizations vary in size, structure and culture (Kersten et al., 2018; May et al., 2016). Implementing the MDET-method in other contexts may need adapting the method to provide a better fit (Chambers and Norton, 2016). Moreover, when executing MDET, effectiveness may be influenced by varieties in work routines, collaboration and communication among care professionals in a specific organization (Bisschops et al., 2022; May et al., 2016). In this study, the MDET method was implemented in four care organizations. The aims were to identify how organizations would adapt MDET to their context and to test the effectiveness of these adapted versions for reducing involuntary care.
MDET is a multi-component method aimed at reducing involuntary care through consultation by MDET-experts in care teams working with clients with intellectual disabilities (Schippers et al., 2024). MDET-experts were care professionals with different backgrounds working in the organization, such as behavioral specialists with a background in psychology and pedagogical sciences, occupational therapists and physicians with expertise in phasing out involuntary care measures. They were brought together by a MDET coordinator to form an independent MDET-expert team. The choice to involve particular MDET-experts was determined by the questions and challenges that existed in a specific care home. MDET-experts investigated the causes and application of involuntary care and restrictive measures to clients, suggested options for phasing out these measures, and discussed these with care teams. The method involved three core components: (1) inventory and recording of all applied forms of involuntary care, (2) a consultation plan for phasing out involuntary care for individual clients, and (3) advising on changes at the team level to recognize and reduce involuntary care (Schippers et al., 2024). The protocol for MDET followed a series of six consecutive phases: preparation, start, plan, action, completion and follow-up (Bisschops et al., 2022). Schippers et al. (2024) tested MDET in a large long-term care organization for people with intellectual disabilities in the Netherlands. This study showed 20.1% more reduction of involuntary care in randomly chosen care homes in which MDET was implemented compared to randomly chosen care homes that provided care-as-usual (CAU).
Development of the MDET method ran parallel to preparations for the introduction of the CCA, which was aimed to improve the rights of clients with intellectual disabilities and clients with psychogeriatric disorders (Staatsblad, 2018). The CCA came into effect in January 2020 and replaced the old Special Admission Act (Bakkum et al., 2023; BOPZ, 1994; Frederiks and De Visser, 2022). Within the Act, care is considered voluntary when clients either consent or do not show resistance, otherwise care is involuntary. Involuntary care can only be applied as a temporary measure of last resort, against a significant risk of harm to oneself or others, while acknowledging the limitation it imposes on a client’s freedom (Frederiks et al., 2017). New to the CCA, in comparison with the Special Admission Act, was that all care organizations were obliged to have plans for reducing involuntary care, following a step-by-step plan with multidisciplinary consultation which is part of CCA. MDET provides organizations a method for complying with this obligation.
The complexity of the long-term intellectual disability care context, where care is administered by multiple professionals across various aspects of a client’s life, poses challenges for care organizations when it comes to implementing multi-component methods such as MDET. When implementing innovations organizations might need to change policies and work processes (May et al., 2016). Furthermore, care professionals might need to change their behavior and work routines (Nilsen et al., 2012). Processes of implementing innovations and scaling out these innovations to other organizations may be challenged by the degree of applicability and fit of the innovation to these contexts. Also, care professionals’ resistance to the innovation, quality of care dilemmas, and a lack of available resources in organizations could be hindering factors in implementation processes (Bisschops et al., 2023; Voss et al., 2021).
The degree to which components of innovations can be adapted to overcome challenges in implementation, without impeding effectiveness, is called the plasticity of the method (May et al., 2016). When scaling out MDET to other organizations, coordinators tasked with implementing MDET might need to tailor the method to align with the work structures, relations and routines within each specific organization (Bisschops et al., 2022). On the other hand, organizations might put effort in changing these work structures, relations and routines to support their professionals in implementing MDET, which is called elasticity (May et al., 2016). By examining what is done in practice, researchers might be able to distinguish between adaptations that are necessary to improve the fit of an innovation to different contexts, and changes that undermine the fidelity of the innovation (Chambers and Norton, 2016; Moore et al., 2015). Therefore, besides examining which adaptations were made to the initial version of MDET, testing the effectiveness of adapted versions of MDET is necessary.
The first objective of this study was to understand how MDET was implemented in four organizations and which components were adapted to align with each organization’s work routine. The second objective was to evaluate the effectiveness of the adapted MDET versions in reduction of involuntary care recordings during implementation in four care organizations, compared to care-as-usual (CAU). To ensure MDET and the expected reduction of involuntary care did not have an adverse side effect on clients’ incidents, the effect on incident reports was also examined. The research questions were: 1. How was MDET implemented and which adaptations were made to align MDET with the needs and work routines of organizations? 2a. Did MDET impact the number of weekly recorded involuntary care over time in care homes that implemented the MDET method, compared to homes in which MDET was not yet implemented (CAU)? 2b. If there was a difference between care homes in the implementation condition and the care-as-usual condition, did implementation of MDET enhance reduction in the number of weekly recorded involuntary care compared to the period before MDET implementation? 3. Did the number of weekly recorded incidents involving clients with intellectual disabilities remain stable during implementation of MDET compared to the period before MDET was implemented?
Method
Study design
This multi-method study was conducted in four intellectual disability care organizations. To investigate adaptations to the MDET method (research question 1), interviews and presentations abouts implementation were qualitatively analyzed. To address research question 2, a retrospective quasi-experimental interrupted time-series (ITS) design (Penfold and Zhang, 2013) was conducted to test changes in weekly counts of involuntary care recordings from before to after the start of implementation of MDET in care homes (n = 25) and compare these to changes in care homes that carried on as usual (n = 25). The interruption was defined as the date on which the MDET method started in the implementation condition. In the analysis, we accounted for the nesting of involuntary care recordings within care homes. Lastly, to examine whether implementation of MDET was not associated with an increase in incident reports we compared the number of weekly recorded incident reports before and after the MDET start date, moderated by care home condition (implementation vs. CAU), and accounting for the nesting of incident reports within care homes (research question 3).
Data collection
Participants and data collection qualitative study
MDET coordinators of four participating organizations collaborated in a Community of Practice (CoP) since June 2019 with the aim to exchange insights and ideas about implementation of methods that reduce involuntary care (Bisschops et al., 2023). A CoP is a group of people with a mutual interest in a domain or topic who work and learn together (Wenger et al., 2002). CoP meetings were held every two months. The agenda was set jointly and included topics such as implementation experiences, phasing out involuntary care, changing socio-political context and executing the MDET method. In organizations A and C, MDET coordinators were policy workers. In organization B, the coordinator was a psychologist. Organization D had two coordinators: one policy worker and one psychologist.
In September 2023 MDET coordinators evaluated their implementation experiences, which included possible adaptations to the method in a semi-structured interview with the first author. The interview guide was developed in line with the five-step process described by Kallio and Colleagues (2016). Interview questions were informed by Normalization Process Theory (May et al., 2022) and are to be found in the Supplement. During the last CoP meeting in October 2023, coordinators presented their experiences with implementing MDET to each other and the research team. Both the interviews and presentations by MDET coordinators were analyzed to examine the implementation and adaptations to MDET. This qualitative study was approved by the Ethics Committee of the faculty Behavioral and Movement Sciences, Vrije Universiteit Amsterdam VCWE-2019-090R1.
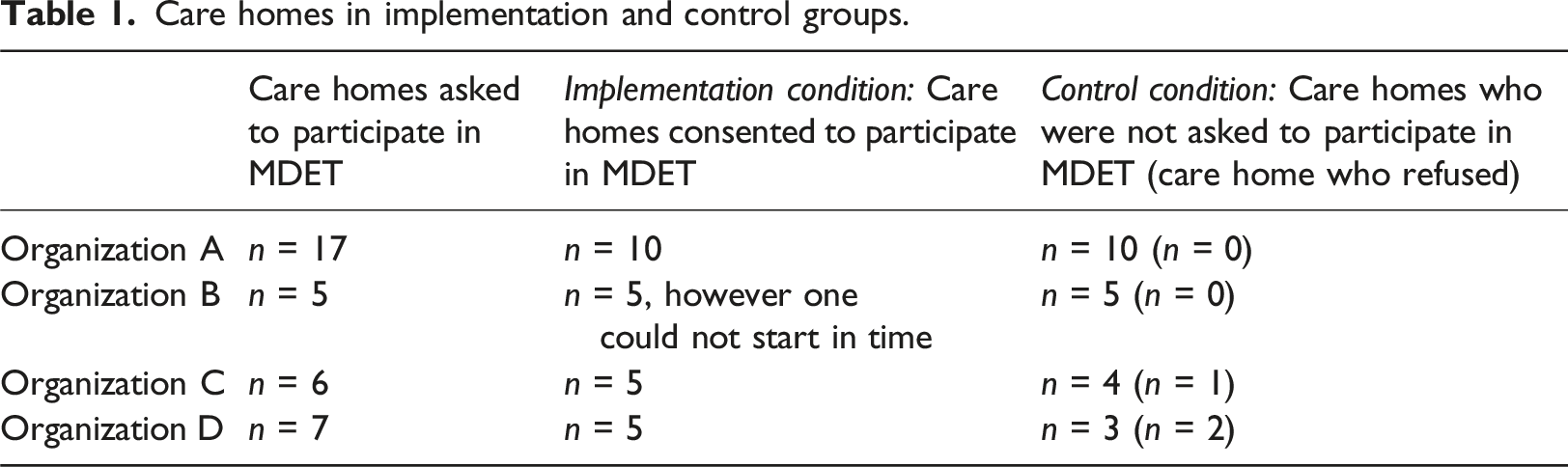
Participating care homes quantitative study
Care homes in implementation and control groups.
Data items: Recordings of involuntary care and incidents
Care professionals record involuntary care and incidents in the organization’s digital reporting system. The involuntary care reporting system enables the monitoring of all records and facilitates the tracking of progress in phasing out involuntary care practices. A previous reliability study showed that 46% of coercive measures were correctly recorded (Schippers et al., 2018). In cases of emergency situations that place clients or others at immediate risk, involuntary care measures can be applied even though these are not yet recorded. Afterwards care staff report this within 48 hours as ‘unforeseen care’, with a maximum validity period of two weeks. Because these emergency situations often involve incidents with clients, care staff also report these incidents in the digital reporting system. This incident reporting system contains a semi-structured form including questions about when and where the incident occurred, who was involved, what type of incident it was, whether people were left injured and how the incident was followed up (Schuengel et al., 2020).
For the purpose of this study, all forms of recordings of involuntary care and unforeseen care were combined, under the term involuntary care. A previous study found adequate reliability agreement (Cohen’s kappa >.50) between care staff and trained observers concerning recordings for 25 for the most common forms of involuntary care (out of 57 forms) (Schippers et al., 2018). Each recording includes the starting date and the form of the measure, such as restriction on freedom of movement, administration of medication, and restriction of visits or use of the telephone (Bakkum et al., 2023).
In consultation with MDET coordinators the following incident reports were included in this study, because of their potential link with involuntary care measures: aggression (including verbal and physical aggression, violence and sexual transgressions), falling, running away or being missing (whereabouts unknown), getting burned, fire setting, incidents involving pricking, cutting, biting and spitting, intake of harmful substances, suicide attempts, and incidents involving bumping, pinching, and colliding. Incident reports concerning medication errors were excluded.
Weekly counts of recordings of involuntary care and incidents reports for the care homes in both the implementation and CAU condition were extracted by data managers of the four organizations. They provided anonymized Excel tables for each care home in both conditions containing information about the start dates of MDET, the number of clients receiving care, and weekly recordings of involuntary care and incidents reports.
Data analyses
Qualitative data analysis
For research question 1, interviews with MDET coordinators of each organization and their presentations in the last CoP meeting were audio recorded and transcribed verbatim. Transcripts were uploaded in Atlas.ti Windows (Version 24.0.0.29576). The first author designed a codebook based on the Framework for Reporting Adaptions and Modifications-Expanded (FRAME) to determine how the four organizations implemented MDET and which adaptations were made (Wiltsey Stirman et al., 2019). The first and fourth author coded the data independently, after which they discussed the fit of the codebook and the codes that were added. Codes were divided into two main categories: “MDET components followed” and “MDET components not followed or changed” (Figure 1). When elements were not followed, these were further coded in four code groups: (1) For whom is the adaptation made, (2) What was the goal, (3) Reasons for adaptation, (4) Nature of adaptation. Main categories and subcodes.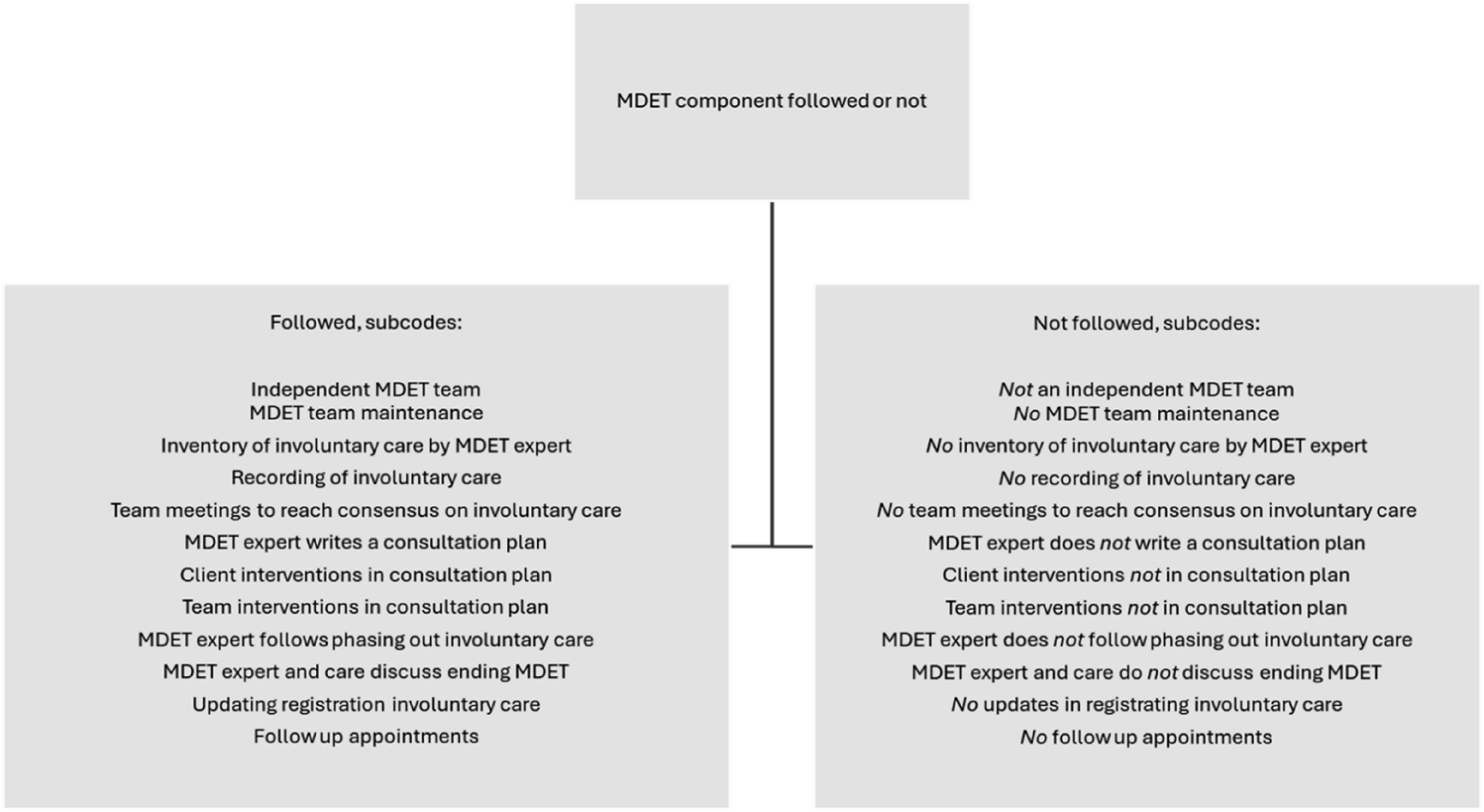
Quantitative data analysis
The data were analysed using R version 4.3.2 (R Core Team, 2023) in R Studio version 2023.12.1.402 (Posit team, 2024). R packages imputeTS (Moritz and Bartz-Beielstein, 2017), readxl (Wickham and Bryan, 2023), tidyverse (Wickham et al., 2019), and tsibble (Wang et al., 2020) were used for data cleaning and preparation, and psych (Revelle, 2024) was used for the descriptive statistics. Alpha levels were set at .05 for all analyses.
First, the data were cleaned and prepared for analysis. For each care home, missing weekly data were imputed using linear interpolation. Then, the outcome variable for research question 2 (weekly recorded involuntary care) was calculated by the sum of weekly recorded involuntary care and unforeseen care, averaged per 10 clients to aid interpretability of the results. For research question 3, a variable was created of the number of weekly recorded incident reports, also averaged per 10 clients. The time series data of care homes in the implementation and CAU conditions were then aligned. This was done by randomly matching pairs of care homes in both conditions (one in the CAU condition and one in the implementation condition) within each organization, finding the minimum and maximum overlapping weeks and years for each pair, and trimming both datasets to keep the rows that fall within the overlapping weeks and years. This way, the time series of each pair of care homes started and ended in the same week and year. Then, the variable indicating the start and end date of MDET of the care home in the implementation condition was copied to the care home in the CAU condition, which made it possible to compare the impact of MDET between care homes in both conditions. All pairs of care homes were then merged into the final dataset. Lastly, for each care home, a time variable was created, ranging from 1 to the total number of rows (weeks) in the data. Descriptive statistics (means, averages, frequency and range) were then calculated for all study variables, separately for care homes in the CAU and implementation condition.
For research question 2, linear mixed effects models (package nlme; Pinheiro et al., 2023) were developed, with a random intercept for care home and an autoregressive correlation structure. Weekly recorded involuntary care was the outcome variable. The first model (model 1) was an unconditional means model with a random intercept for care home. The intraclass correlation coefficient (ICC) was calculated as an indicator of the variability in weekly recorded involuntary care between different care homes. We explored the unconditional means model with a random intercept for organization, and calculated the ICC to examine the variability of registrations between the four organizations.
Successive growth models were built as follows: a model with a random intercept for care home and an autoregressive autocorrelation structure (AR1), to account for the dependency of observations over time within care homes (model 2); time (continuous) added as a fixed effect (model 3); the start of the MDET method (coded 0 or 1) as a fixed effect (model 4); the interaction between the start of the MDET method and time as a fixed effect (model 5); and the interaction between start of the MDET method, time, and care home condition (CAU or implementation condition, coded 0 or 1) as a fixed effect (model 6). Confidence intervals (90%) were calculated for the effect size (beta coefficient) of the interaction between time, start of the MDET method, and care home condition on weekly recorded involuntary care (model 6).
For research question 3, the same models as for research question 2 were developed, but with weekly recorded incident reports as the outcome variable. Then, we conducted equivalence tests as follows: 90% confidence intervals were calculated for the effect size of the interaction between time, start of the MDET, and care home condition on incident reports. The smallest effect size of interest was a priori set at [-0.2; 0.2]. If the values in the 90% confidence interval would fall within this range, we would conclude that there is no meaningful difference between care home conditions (CAU versus implementation condition) regarding the effect of MDET on weekly recorded incident reports over time.
For all linear mixed effects models, differences between goodness of model fit were calculated using log-likelihood ratio tests (package lmtest; Zeileis and Hothorn, 2002).
Results
Qualitative analysis
Implemented, not implemented and adapted MDET-components.
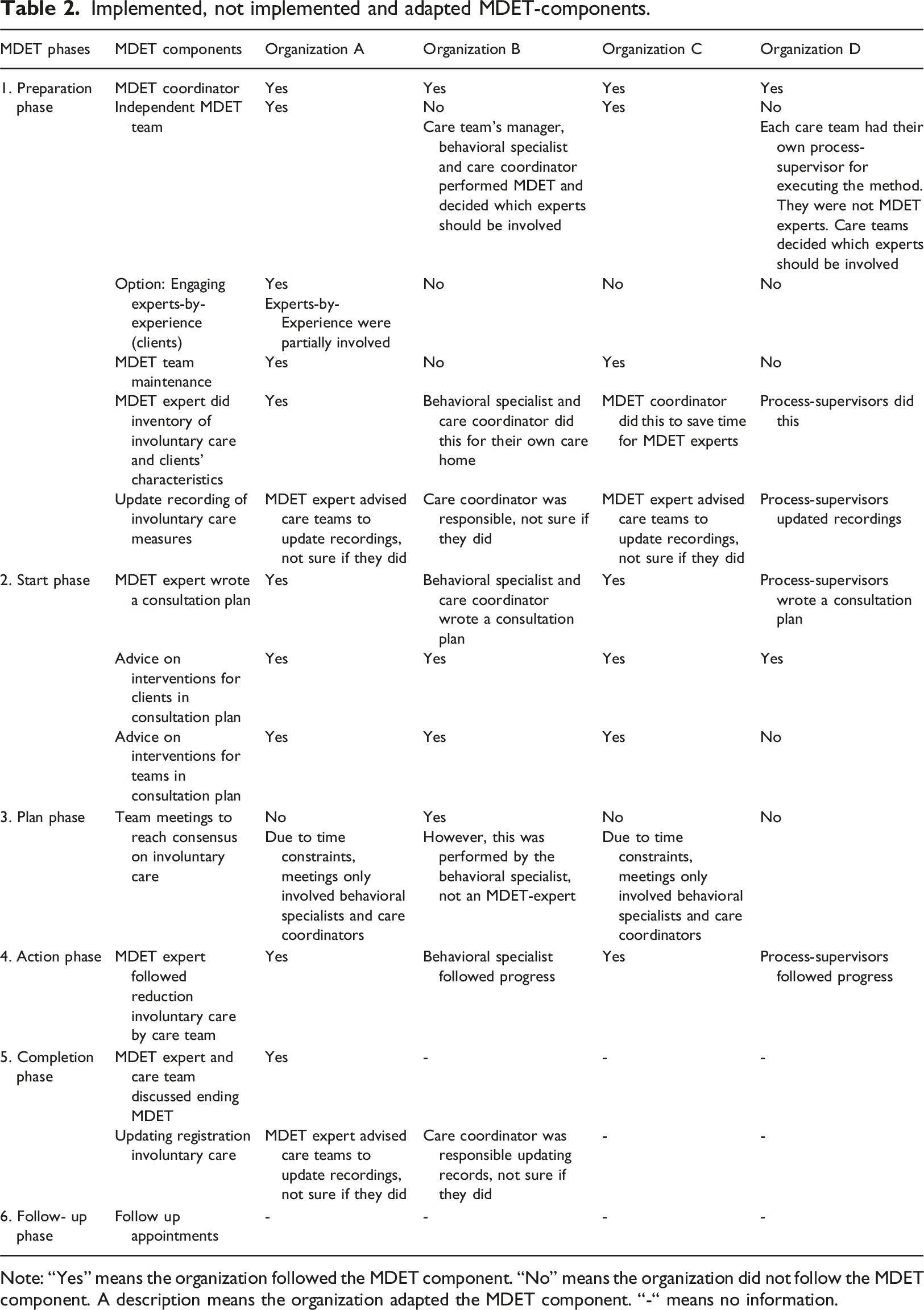
Note: “Yes” means the organization followed the MDET component. “No” means the organization did not follow the MDET component. A description means the organization adapted the MDET component. “-“ means no information.
Prerequisites to execute MDET
Organizations A and C appointed independent MDET-expert teams, overseen by a coordinator responsible for implementing MDET. These coordinators initiated MDET team meetings aimed at sharing experiences in performing the MDET method and discussing difficult cases with regard to reduction of involuntary care. Organization B and D did not appoint independent MDET-expert teams. Because organization B is a small organization, they chose to embed the MDET method into the regular work routines of all behavior specialists. “Actually, we kind of let go of an actual expert team. At our 5 care homes, we created 5 expert teams in which the basis was formed by the triangle of behavioral expert of that care home, the care coordinator and the team leader. And then two experts were added to the team to look at involuntary care from an independent perspective. Because, of course, if only this triangle reflects on involuntary care, it's quickly a colored view. However, we did leave it up to the triangle to decide which people to include as expert.” (Organization B)
Organization D determined that executing MDET in care homes would be overly demanding in terms of time for experts and could feasibly be managed by process supervisors, who were care professionals involved in one of the care teams in the implementation condition who were cross-matched to another care team in the implementation condition.
Organization A experimented with involving experts-by-experience (clients with a mild intellectual disability) in their MDET-expert team, to broaden the multidisciplinary perspective. They gave advice regarding proposed interventions in consultation plans. Their input was evaluated as valuable, even though for privacy reasons, they could only be involved in an advisory role. Other organizations mentioned the complexity of involving experts-by-experience. One organization also questioned whether clients with mild intellectual disabilities could sufficiently empathize with people with more severe intellectual disabilities regarding involuntary care.
Inventory of involuntary care recordings
In organization A, the inventory of involuntary care was conducted by MDET-experts, whereas other organizations opted for alternative personnel to fulfill this task. “First, the process supervisors identified involuntary care used within each care home. We used Schippers' list for this purpose (ed. Schippers et al., 2018). What do we actually have on restrictive measures and which part of that is involuntary care? Because those are still two different things. That was very helpful. It raised awareness.” (Organization D)
Across all four organizations, MDET-coordinators had concerns regarding updating involuntary care recordings, because care professionals did not see this as feasible during COVID-19, nor as a priority.
In all organizations, the process of reducing involuntary care was monitored during the action phase of MDET. The MDET coordinator of organization A mentioned that this phase could take a long time, posing challenges for MDET experts to follow progress. The extended duration of the action phase also posed difficulties in achieving a clear conclusion about the ending of MDET in care homes. In some cases, even after a year or longer, the highest attainable level of reduction of involuntary care had not yet been reached, complicating the process of formally finalizing the method with the teams and updating the records of involuntary care.
Consultation plans with client and team interventions
In all organizations, consultation plans were drafted; however, only in organizations A and C plans were formulated by the MDET expert, while in organization B the plan was written by the behavioral specialist and care coordinators already responsible for clients’ care, and in organization D the process-supervisor took charge of writing the plan. All consultation plans suggested client interventions aimed at reduction of involuntary care. Similarly, team interventions were proposed in all plans, except for organization D. Meetings to reach consensus about client- and team-interventions with all team members of a care team were achieved only in organization B, facilitated by behavioral specialists themselves. Because of time and personnel restraints, which peaked during COVID-19, the remaining organizations discussed the consultation plan and the proposed interventions with only the behavioral specialist and care coordinator involved in the care home.
Quantitative analyses
Descriptive statistics
Descriptives of Study Variables.
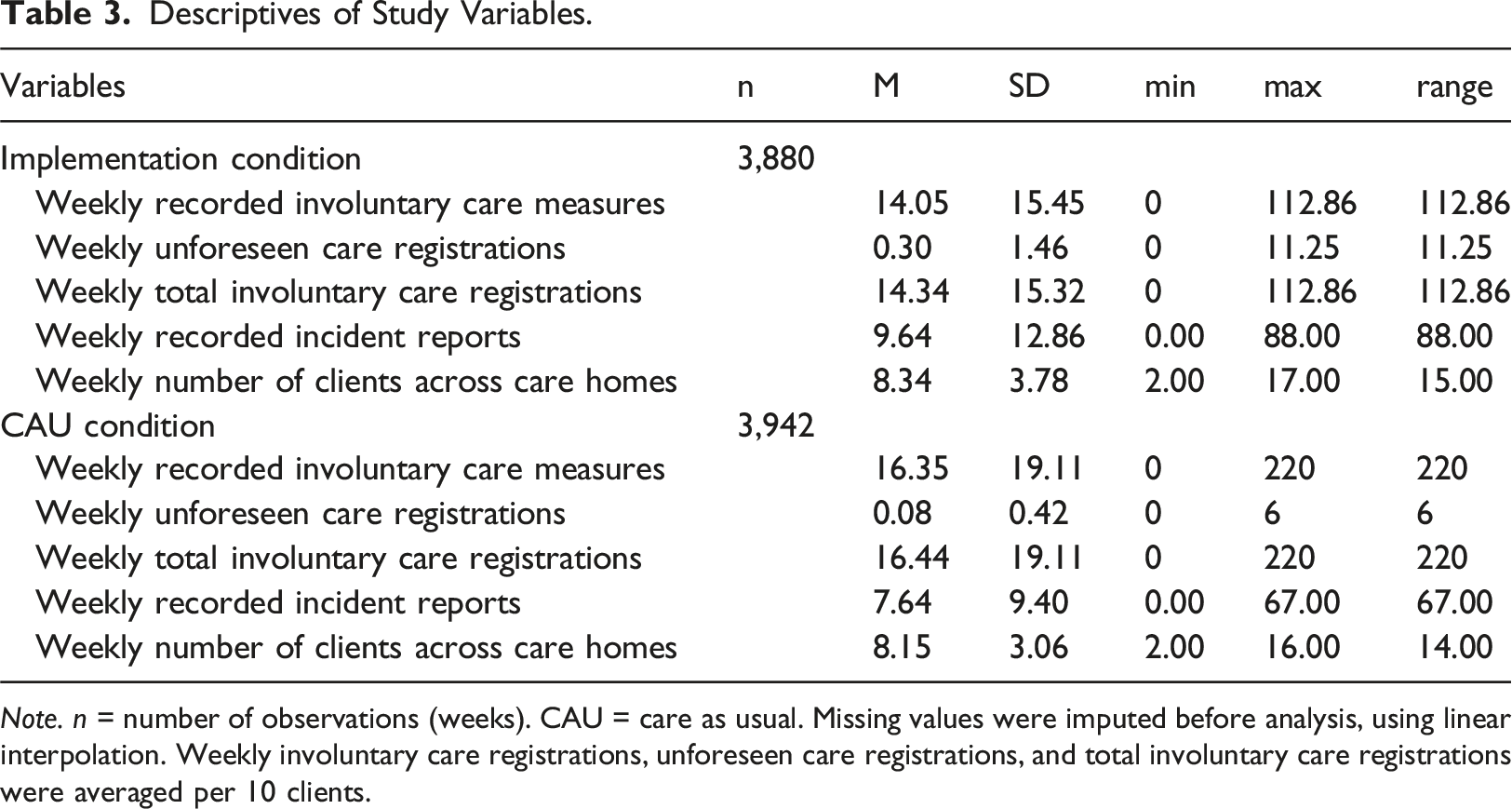
Note. n = number of observations (weeks). CAU = care as usual. Missing values were imputed before analysis, using linear interpolation. Weekly involuntary care registrations, unforeseen care registrations, and total involuntary care registrations were averaged per 10 clients.
For some weeks, data were not provided by care organizations. These data were marked as missing in the dataset. Before analysis, missing data were imputed using linear interpolation. In total, 7.4% of the data on involuntary care registrations were missing, 8% of data on incident reports, and 3.3% of data on the number of clients were missing.
Effect of MDET on involuntary care recordings
Results of Linear Mixed Effects Models: Effect of the Implementation of MDET on Weekly Recorded Involuntary Care.
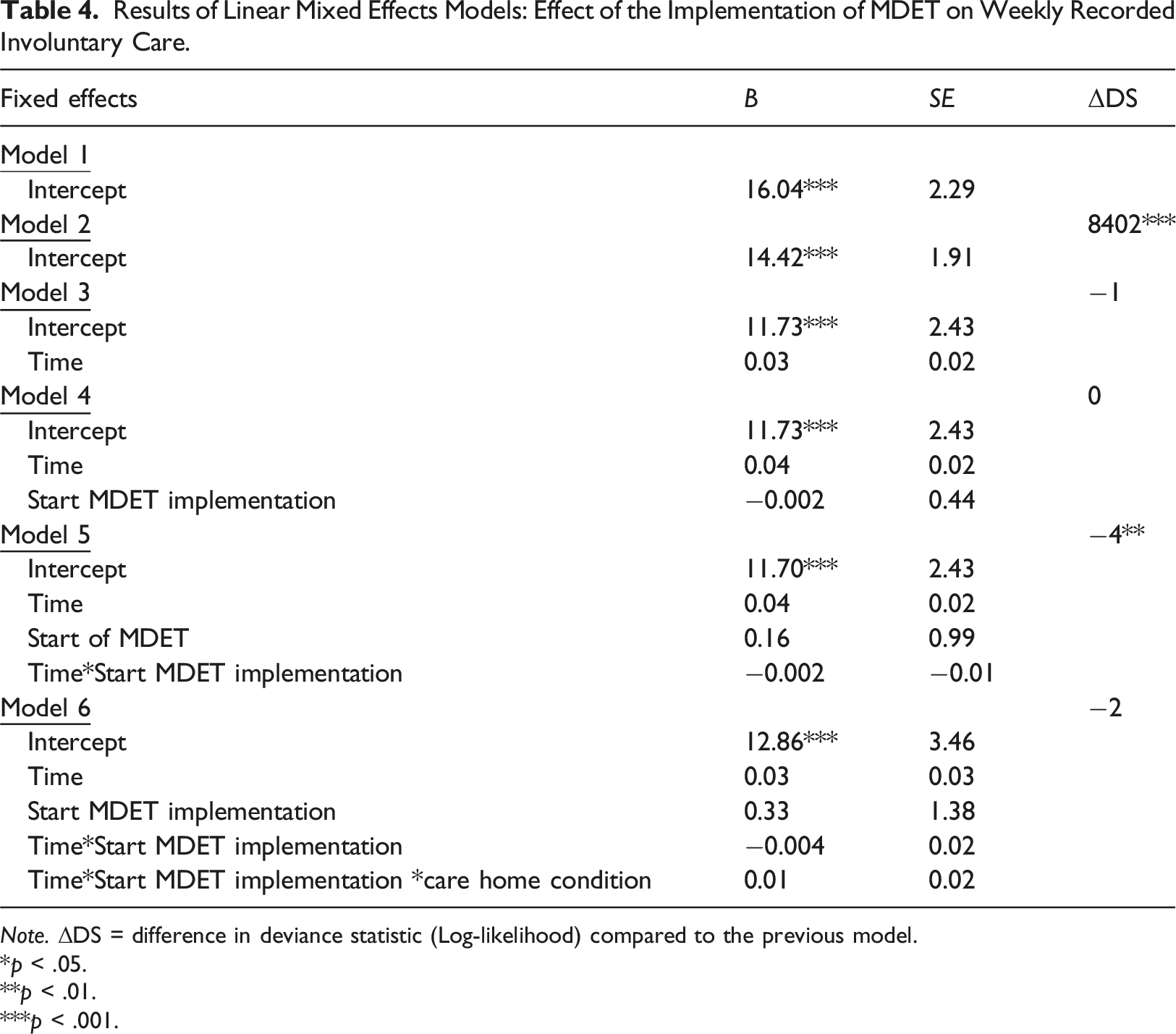
Note. ΔDS = difference in deviance statistic (Log-likelihood) compared to the previous model.
*p < .05.
**p < .01.
***p < .001.
First, an unconditional means model (model 1) was fitted, including only a random intercept for care home. The ICC of this model was 0.68, meaning that 68% of the variance in involuntary care recordings was accounted for by differences between care homes. To test if the level of organizations should also be included as a random effect, we also fitted an unconditional means model with a random intercept for organization. The ICC of this model was 0.065, meaning that 7% of the of the variance in involuntary care recordings was accounted for by differences between organizations. Because of the low ICC, we pursued the analyses with only a random intercept for care home.
In the next model (model 2), an autoregressive autocorrelation component was added (AR1). This model showed a significantly better fit to the data than the unconditional means model (χ2 (1) = 16.804, p < .001).
Next, time was added as a fixed effect (model 3). Time was not significantly associated with weekly recorded involuntary care recordings (B = 0.03, SE = 0.02, p = .074), and adding time did not significantly improve the model fit (χ2 (1) = 2.86, p = .091). Then, the start of implementation was added to the model (model 4), which was not significantly associated with involuntary care recordings (B = −0.002, SE = 0.44, p = .997). The model fit did also not significantly improve (χ2 (1) = 0.18, p = .674). The interaction between time and the start of implementation was then added to the model (model 5). The interaction term was not significantly associated with involuntary care recordings (B = −0.002, SE = 0.01, p = .854). Including this term made the model fit significantly worse (χ2 (1) = 7.02, p = .008). Lastly, we included the interaction between time, start of implementation, and care home condition (CAU versus implementation condition) in the model (model 6). The effect of the MDET method on the slope was not significantly different for CAU versus implementation homes (B = 0.01, SE = 0.02, p = .816), and the model fit did not significantly improve (χ2 (4) = 3.90, p = .420). The 90% confidence interval for the interaction term in model 6 was [-0.03; 0.04].
Effect of MDET on incidents reports
Results of Linear Mixed Effects Models: Impact of the Implementation of MDET on Weekly Recorded Incident Reports.
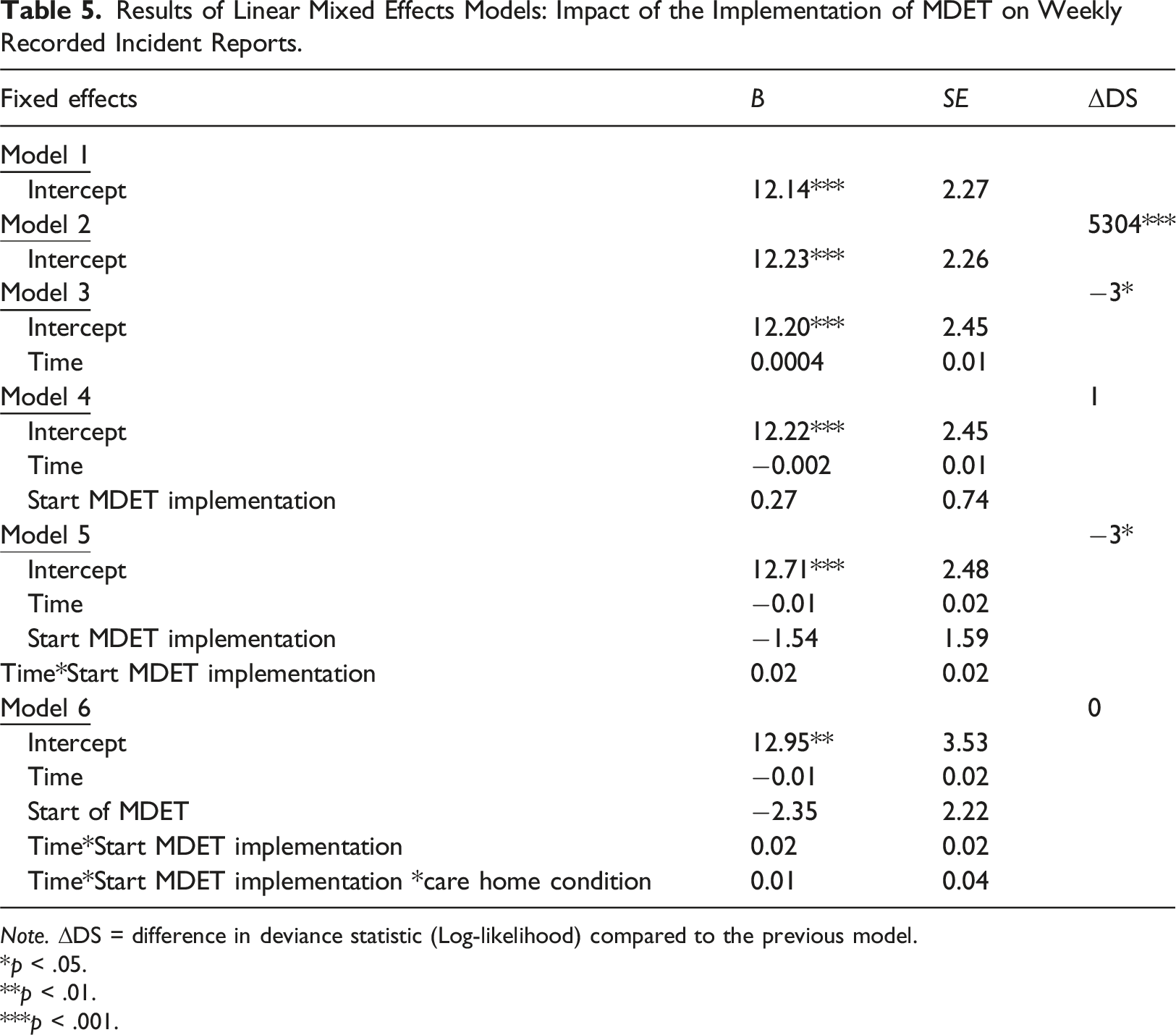
Note. ΔDS = difference in deviance statistic (Log-likelihood) compared to the previous model.
*p < .05.
**p < .01.
***p < .001.
The ICC of the unconditional means model (model 1) was 0.64, meaning that 64% of variance in incident reports was explained by differences between care homes. Model 2 included an autoregressive autocorrelation structure and had a significantly better fit than the unconditional means model (χ2 (1) = 10,681, p < .001). The time variable was then added as a fixed effect (model 3). Time was not significantly associated with incident reports (B = 0.0004, SE = 0.01, p = .974) and adding time resulted in a significantly worse model fit (χ2 (1) = 6.95, p = .008). In model 4, the start of implementation was included, which was not significantly associated with incident reports (B = 0.27, SE = 0.74, p = .720), and did not improve the model fit (χ2 (1) = 1.38, p = .241). Then, the interaction between time and the start of implementation was added to the model (model 5), which resulted in a significantly worse model fit (χ2 (1) = 4.56, p = .033). Implementation did not have a significant effect on the slope (B = 0.02, SE = 0.02, p = .200). In model 6, we added the interaction between time, start of implementation, and care home condition to the model (CAU versus implementation condition). The interaction term was not significantly associated with incident reports (B = 0.01, SE = 0.04, p = .810) and the model fit did not improve (χ2 (4) = 0.65, p = .958). The 90% confidence interval for the interaction term in model 6 was [-0.05; 0.07], which falls within the range of our smallest effect size of interest [-0.2; 0.2].
Discussion
This study examined adaptations to the MDET method that care organizations made during the implementation process and tested whether these adapted versions were effective in reducing involuntary care in intellectual disability care. As expected, all four participating organizations adapted MDET to their specific contexts. Adaptations varied in scale, ranging from minor adjustments such as reducing the number of participants in meetings aimed at consensus building on involuntary care, to major modifications, such as decreased attention to monitoring the recordings of involuntary care. Two care organizations did not appoint an independent MDET expert-team, which was a major adaptation. In these organizations the method was executed by process-supervisors or care professionals already involved in the care home. The reasons for adapting MDET often concerned feasibility and resources, such as personnel restraints during the COVID-19 pandemic. Also, some organizations mentioned that not all phases of the MDET were executed due to time constraints.
Care homes that implemented MDET in the four organizations did not significantly differ in the number of weekly recorded involuntary care over time, compared to care homes providing care as usual. A first possible explanation for the difference in the effectiveness of the MDET method between the study by Schippers et al. (2024) and the current study could be that the previous study was highly controlled by the researcher, which resulted in low plasticity of the MDET method which ensured fidelity to the protocol. Moreover, the researcher made sure that the organization was supported to change their work routines to fit in MDET, which resulted in a high elasticity of the organization (May et al., 2016). In the current study, the four organizations had the freedom to adapt MDET to their local needs and circumstances (high plasticity). This may have facilitated the implementation of the method, as pre-existing work routines and structures could be left intact and resistance to the method minimized (Chambers and Norton, 2016). However, the fidelity of the implementation to the original method may be compromised (Moore et al., 2015), reducing the efficacy. For example, the choice of organizations to involve only the behavioral specialist and care coordinator of a care team in inventorying involuntary care measures may have resulted in fewer professionals who were in support of reducing these measures. Second, actual disruption of care professionals behavior, work routines and structures by a new method may be what is partly driving effects in implementation and clinical improvements (Nilsen et al., 2012).
One reason for care organizations to choose to adapt the core components of MDET was the Covid-19 pandemic, which was a major challenge during implementation of MDET. The initial response of care organizations was to cancel or suspend MDET, because the government restrictions to prevent infection risk made it difficult to focus on implementing a new method. Moreover, some care professionals became ill or started to experience mental health problems (Sheerin et al., 2023), which made organizations reluctant to put extra burden on the care team. However, care organizations also saw a need and opportunity to attend to the adverse effects of involuntary care and restrictive measures on clients’ well-being, given that the COVID-19 restrictions made everyone aware of these effects. Therefore, all organizations resumed the implementation of MDET. However, they elected to avoid components that could potentially lead to resistance among care professionals, such as insisting on updating involuntary care recordings and monitoring this. Hence, difficult socio-political contexts, where care professionals face significant burdens, can be a double-edged sword for the implementation of multi-component methods such as MDET. On the one hand, awareness of weaknesses in care practices may increase openness to and motivation for implementation of new methods. On the other hand, the enhanced social-political pressure may also increase implementation challenges in care organizations by thwarting the focused attention needed to change a particular practice. Therefore, care organizations must balance the urgency for improvement with the need for a thoughtful, well-planned approach to implementation.
A second explanation accounting for the differences in effectiveness between the study by Schippers et al. (2024) and the current study may be found in the differences between the old Special Admission Act and the new Care and Coercion Act (CCA). The trial by Schippers took place when the previous Special Admission Act was still in effect, which obligated care professionals to record all forms of restrictive measures even when clients consented. Moreover, in this time period the Board of directors of the organization in which MDET was developed and tested spearheaded a policy emphasizing that people with complex care needs should have the freedom to self-determine their care and support. This policy may have led the organization more susceptible for change, which was strengthened by the preparations for the upcoming CCA, for which care professionals (including care staff, physicians, and psychologists) needed to transition to a new definition of involuntary care and a new way of evaluating care practices (Bij De Weg et al., 2021). Within this socio-political and organizational context MDET was developed and shown to be effective in reducing involuntary care. The effects of care organizations’ policies and the preparations for the new act may have waned when the current trial was conducted.
A third explanation for the differences in effectiveness between both studies may be that multidisciplinary consultation has become a part of a step-by-step plan inserted within the CCA. Although the MDET method is more thorough than the CCA step-by-step plan in detecting involuntary care and providing a broad range of advice including team interventions, both include the consultation of independent experts. The implementation of the CCA in 2020 (Bakkum et al., 2023) may have changed care as usual in such a way that the added value of MDET may be more difficult to detect.
Study limitations
Covid-19 not only had consequences for the organizations executing MDET but also for the design of the study. At the start of the pandemic, the original randomized controlled stepped wedge design needed to be changed to a less robust quasi-experimental interrupted time-series design. Although both designs can offer valuable insights in evaluating interventions, the new design interfered with making a clear comparison between implementation and control groups especially when compared to the randomized controlled study by Schippers et al. (2024). Care homes could decide if and when they were going to participate in implementing MDET, which resulted in an implementation group with various MDET implementation start dates and a mixed control group of care homes that had refused to participate in MDET and care homes to whom MDET had not been submitted for participation.
The limited monitoring of recordings of involuntary care during the implementation of MDET was another limitation to this study. In the interviews, all MDET coordinators mentioned their uncertainty about whether recordings of involuntary care were updated at the beginning and end of the MDET. Because this was pointed out as a core component of the MDET method by its developers (Schippers et al., 2018) and the data for the current study depended on these recordings, this was a major limitation.
Implications for policy, practice and future research
Future use of MDET in care organizations should address identifying care homes and circumstances where MDET offers value in addition to the CCA. Perhaps, under the CCA, MDET is beneficial in care homes with low awareness of involuntary care or where complex care needs require multidisciplinary consultation to find alternatives to involuntary care.
Implementation coordinators who facilitate future implementation of MDET in care organizations should take into account the delicate balance between preserving fidelity of the method and adapting the method to fit with local needs.
Future research concerning the MDET method may identify the conditions under which care homes may benefit most from implementing the MDET method. Other questions regarding the components and phases of MDET that are essential to effectively reduce involuntary care may be addressed.
Future research concerning implementation of methods in intellectual disability care may benefit from these findings by taking into account the advantages of combining both qualitative and quantitative methods to evaluate implementation processes of multi-components methods. Concerning the quantitative data from digital care recording systems researchers should be aware that these data may may be unreliable due to insufficient updates by care professionals.
Conclusion
Scaling out and implementing the Multi-Disciplininary Expertise Team (MDET) method to four intellectual disability care organizations resulted in various adaptations, such as minimizing the number of participants in meetings and not appointing an independent MDET-expert team. Effectiveness of the adapted MDET for reducing involuntary care was not demonstrated in this study. However, because the CCA, that came into effect in 2020 in the Netherlands, now mandates a multidisciplinary approach in a step-by-step plan within the law, the effects of MDET may have been less pronounced compared to the earlier trial by Schippers et al. (2024). Care organizations intending to implement MDET should consider their inclusion criteria for care homes to enhance the likelihood of the method adding value in reducing involuntary care. Furthermore, although the plasticity of multi-component methods was theorized as beneficial in implementation processes, as this would allow organizations to adapt and tailor these multi-component methods to specific organizational contexts (Chambers and Norton, 2016; May et al., 2016; Moore et al., 2015), the current study suggested that elasticity of organizations, such as changing work routines, structures and relations within organizations, may also be necessary to contribute to the expected objectives and outcomes.
Supplemental Material
Supplemental Material - Implementing the multi-disciplinary expertise team method to reduce involuntary care in intellectual disability care: Multi-methods study evaluating adaptations and effectiveness
Supplemental Material for Implementing the multi-disciplinary expertise team method to reduce involuntary care in intellectual disability care: Multi-methods study evaluating adaptations and effectiveness by Esther H. Bisschops, Lianne Bakkum, J. Clasien de Schipper, Britt Metselaar, Simone van der Plas, Petri J.C.M. Embregts, Carlo Schuengel in Journal of Intellectual Disabilities
Footnotes
Author contributions
Simone van der Plas: Investigation; resources; writing-review & editing
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Scientific Research Foundation’s Heeren Loo [grant number 2190200]; ZonMw [grant number 80-84500-98-402].
Ethical statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.