
Abstract
In Ireland, the provision of behavior support services has developed following the introduction of Health Information and Quality Authority (2013) standards and the regulation of Positive Behavior Support (PBS) under the Health Act (2007). The purpose of this study was to explore what factors facilitate and act as barriers to implementation of behavioral recommendations in Intellectual Disability organizations from the practitioner’s perspective. Twelve interviews were carried out, audio recorded, transcribed and analysed using Braun and Clarke’s (2006) Thematic Analysis. One superordinate theme (administrator support), four themes (values, resources, relationships and implementation of consequences) and five sub-themes (staff turnover and burnout, training and knowledge, time and physical contact, relationships between practitioners and staff and staff and service users) were identified, all interconnected in the implementation process. A common thread reflected throughout the themes, was the practitioner’s acknowledgment of barriers overpowering facilitation which resulted in a less than optimum implementation of PBS.
In Ireland, disability services are either publicly or privately funded. Publicly funded services are provided directly by the Health Service Executive (HSE) or by charity organizations, in receipt of public funding, to deliver health and social care services to care for individuals with intellectual disability across residential and day services, and community and education settings. Irrespective of funding, all providers are monitored at a national level by the Health Information and Quality Authority (HIQA, 2013), a government funded agency set up to monitor the safety and quality of health and social care systems in Ireland. Irish legislation, through the Health Act, (2007) mandates that any adult with an intellectual disability, who presents with challenging behavior and resides in residential care, should be provided with Positive Behavior Support (PBS). Grey, Lydon and Healy (2016) discuss the need for further research in the provision of PBS in Ireland given its increasing presence in disability services. They proposed that its increased application is a direct result of its efficacy as an approach in reducing both the frequency and severity of challenging behaviour displayed by individuals with intellectual disability, but also because it resonates strongly with the values underpinning modern service provision. PBS has emerged as a model of intervention from three major sources: (i) Applied Behavior Analysis (Carr & Sidener, 2002; Tincani, 2007), (ii) the normalisation/ inclusion movement and (iii) person centred values.
PBS is an evidence based practice (EBP; Gore et al. 2013) and is widely used and accepted in the intellectual disability sector in Ireland and is delivered through the implementation of Behavior Support Plans (BSPs). At a national level the delivery of PBS is overseen by HIQA through inspections and investigative reports. HIQA guidelines recommend that social care organizations consult with behavior support specialists when providing training and recommendations in PBS (HIQA, 2019). In order to enhance our healthcare and social care systems for people with intellectual disabilities, attempts must be made to explore the barriers and facilitators to the implementation of what is considered to be good practice, as it may then lead to enhanced endorsement and implementation (Fixsen, Naoom, Blase, Friedman, & Wallace, 2005).
Emerson (2001) highlights a significant challenge for services in the widespread implementation (i.e. delivery and maintenance) of PBS in social care settings. Across organizations and services, there are variance in the standards set for the implementation of PBS. The typical implementation process involves the completion of a functional assessment of challenging behavior, which culminates in the design of a BSP by a behavior support practitioner who provides recommendations to front-line staff. Following this, front-line staff are trained in the delivery of the components of the BSP and, subsequently, are responsible for the day to day implement of the BSP. In order for the service user to benefit from the BSP, the recommendations must be implemented accurately and effectively. Despite enhancements in the development of function based BSP and a growing field of implementation science, this has failed to translate into improved implementation of PBS in a way that is consistent across services and organizations. Therefore, there is value in exploring the barriers and facilitators to implementation of PBS, from the practitioner perspective.
Allen et al. (2005) in an review paper discussed PBS current status and future directions in the United Kingdom. The identified challenges including: lack of trained staff, goodness of fit and lack of resources. Lack of trained staff was described as too few staff trained to an adequate competency level for effective PBS, both in the context of the behavior practitioner and frontline staff. Goodness of fit was identified in the two contexts; firstly, when a plan is not feasible or adaptable to meet the capacity of the service in question, and secondly, when staff assigned to the service user availing of the BSP do not have a positive relationship with the service user. The final challenge identified was lack of resources. This includes both lack of staff and lack of facilities to support the goodness of fit. Allen and colleagues (2005) highlighted three key facilitators to implementation including: changes in the structure and quality of service systems, implementation carried out by normal care staff as oppose to external therapists, and function-based interventions (established via functional analysis/assessment).
To date, a small number of studies have looked at facilitators and barriers in the implementation of PBS, but these have largely focused on school-wide PBS (a three tiered system), and have used a variety of methods to examine the perspective of staff and practitioners. In 2007, Kincaid and colleagues used a systematic process to explore school personnel’s perceived barriers and facilitators to school wide implementation of positive behavior support (Kincaid et al., 2007). The study found staff buy-in was of the highest importance for school wide implementation of PBS. Similarly McIntosh et al. (2014) gathered quantitative and qualitative data from 257 school team members on their perceptions of contextual features and how they related to implementation and sustainability of school wide PBS. They concluded that administrator support and school team functioning were the primary facilitators to school wide PBS implementation. However, they echoed the findings of Kincaid et al. in that they found that staff support or “buy-in”, integration into typical practice, and parental involvement contributed to sustainability, but not necessarily to initial implementation.
The theme of staff buy-in also featured strongly in the findings of Pinkelman et al., 2015 who undertook an open-ended survey with 860 school personnel to identify perceived enablers and barriers in sustaining school-wide positive interventions and supports. The data were qualitatively analysed and produced 13 themes. The most frequent theme representing facilitators to behavior support in schools was staff buy-in; the commitment of teachers and staff in supporting positive behavior support implementation. This theme did not include buy-in from other stakeholders such as family members and community, suggesting that sustainability of behavior support implementation relies heavily on the buy-in from staff who actively implement the plan; an important conclusion that could be incorporated into training programs for staff is to ensure their role in implementation is emphasised and valued. Therefore, it is evident that there is a strong focus on staff buy-in for the implementation of school wide implementation of PBS. Albeit of interest, the findings from school-based studies (Bambara et al,. 2009; Bambara et al., 2012; Pinkleman et al., 2015) cannot be generalised to social care organizations due to the differences in the environments.
To date no studies have been undertaken to examine the barriers and facilitators in the implementation of PBS in social care setting, from the perspective of the practitioner. However, a recent study by Bosco et al. (2019) undertook a process evaluation of a randomised controlled trail of PBS-based staff training in an adult intellectual disability setting. As part of this study they reported findings from participating therapists which reported challenges including managing heavy caseloads, staff turnover and service commitment to implementation as significant barriers to implementation of PBS. This suggests a significant difference in the implementation process of PBS in schools and in social care settings. Therefore, these findings by Bosco et al. (2019) indicate that the social care settings may provide a unique set of challenges which differ from that of school based delivery of PSB, which warrant further investigation.
The current study aims to gain insight into the barriers and facilitators to implementation from the perspective of the behavior support practitioner, working in social care settings. The hypothesis for this study was; do barriers and facilitators have a role to play in the implementation of PBS. Semi structured interviews will be undertaken with participants across organizations in Ireland in an effort to represent a generalised behavior support population. The current study will use a phenomenological approach. This methodological approach will allow for learning based on individuals lived experience, in this case the practitioner role in PBS implementation.
Method
Recruitment and Inclusion Criteria
Participants were purposively targeted with a recruitment flyer posted in a closed social media group for people working in the field of behavior support. Following this snowball sampling was used to recruit other participants whereby initial participants were asked to share details of the study with their own networks. This method of sampling is cost effective, efficient, and widely used for similar research studies whereby the objective is to identify populations of a specific nature (Johnson, 2014). Participants were not recruited based on their title but held titles similar to behavior therapist, behavior specialist, psychologist and behavior analyst.
Recruitment materials (i.e. poster/flyer) advertised a request for practitioners who provide behavioral recommendations and/or create behavior support plans in social care settings. This criteria was included to differentiate from frontline staff who engage in the implementation of said support plans. The target population were practitioners who worked in an interactive consultancy capacity, providing expert recommendations while also assisting with staff facilitation through training and follow up feedback sessions. The settings include residential services and day service settings for individuals with intellectual disability. Participants were included if they were: (i) actively engaged in carrying out functional assessments and function-based behavior support plans in providing positive behavior support; (ii) working in the intellectual disability sector; (iii) aged over 18 years of age.
Participants and Setting
Demographic Table of participant qualifications, duration in their current role and job title.
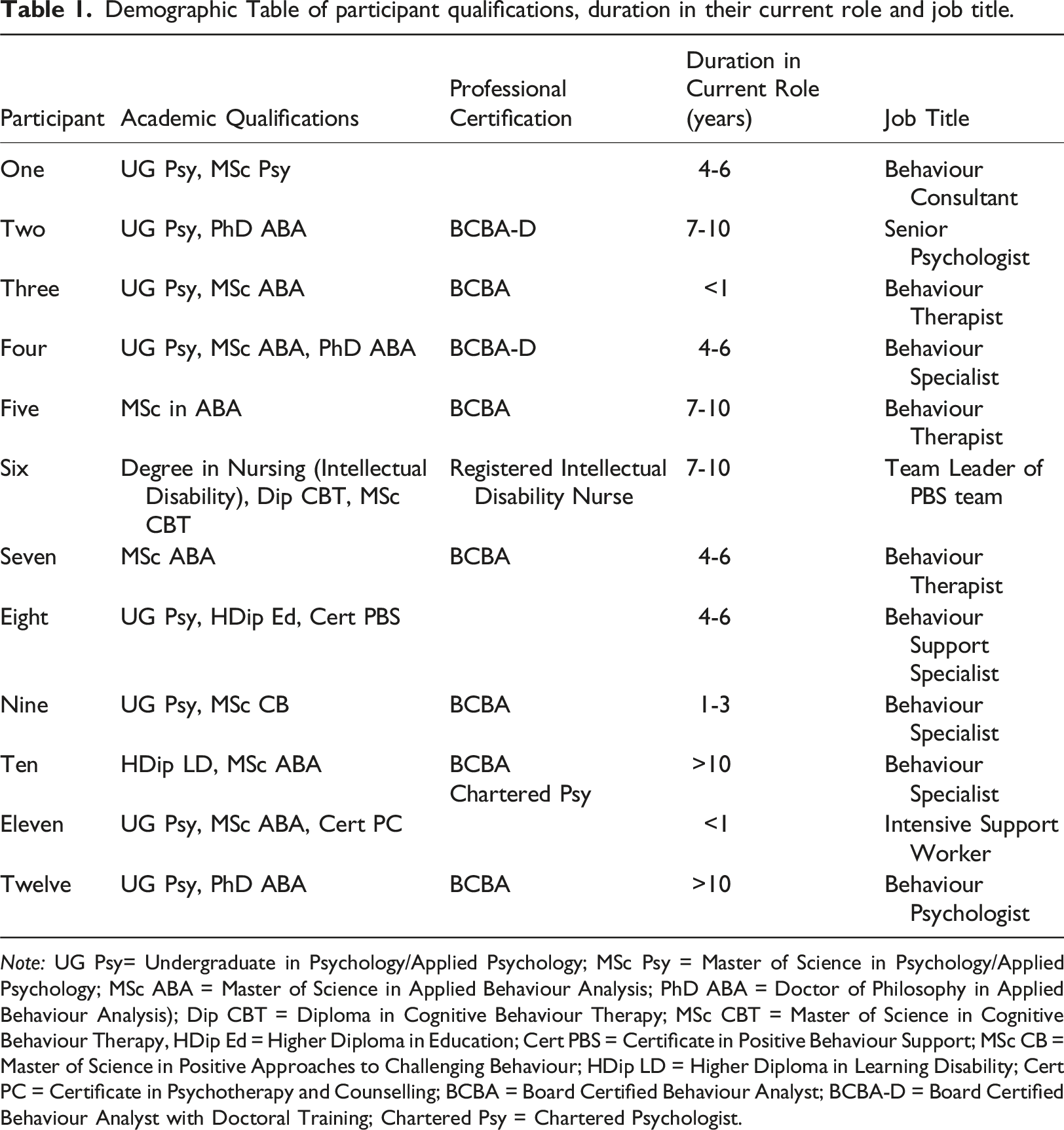
Note: UG Psy= Undergraduate in Psychology/Applied Psychology; MSc Psy = Master of Science in Psychology/Applied Psychology; MSc ABA = Master of Science in Applied Behaviour Analysis; PhD ABA = Doctor of Philosophy in Applied Behaviour Analysis); Dip CBT = Diploma in Cognitive Behaviour Therapy; MSc CBT = Master of Science in Cognitive Behaviour Therapy, HDip Ed = Higher Diploma in Education; Cert PBS = Certificate in Positive Behaviour Support; MSc CB = Master of Science in Positive Approaches to Challenging Behaviour; HDip LD = Higher Diploma in Learning Disability; Cert PC = Certificate in Psychotherapy and Counselling; BCBA = Board Certified Behaviour Analyst; BCBA-D = Board Certified Behaviour Analyst with Doctoral Training; Chartered Psy = Chartered Psychologist.
Due to the geographical spread of participants, telephone and face to face interviews were undertaken. Telephone interviews were carried out for eleven participants and one interview was carried out in person. The interviewer was a graduate student in Applied Behavior Analysis and had no pre-existing relationship with participants, only knowing that the participant being interviewed met the inclusion criteria for the study (Tong et al., 2007).
Procedure
Prior to the interview participants were provided with an information sheet and were invited to sign the consent form, and return this to the researcher. Following this, interviews were scheduled. All interviews were audio recorded. GDPR guidelines were followed as per the Data Protection Act 2018. All participants consented to being interviewed and recorded for the study and were aware that the transcript of their responses would be anonymized. Data was stored safely and securely. During the interview participants were asked for demographic information deemed to be relevant to the study including, qualifications, current role and how long they have been working in their current role.
Semi-structured interviews were used to allow participants to expand on topics (Miles & Gilbert, 2005). All questions were open-ended allowing the participants to discuss any aspect of the subject most relevant to them. The topic guide included the following questions: (a) Where does BSP implementation rank in your duties?; (b) Can you describe the implementation process?; (c) Who’s responsibility is it to get the BSP implemented?; (d) What barriers do you face in the implementation of BSPs?; (e) What facilitates the implementation of BSPs?; and (f) How do you overcome the barriers to implementation? The researcher drew on the anchor points from the topic guide for the study in a flexible and appropriate way. Interviews ranged in duration from 35 minutes to 1 hour.
Data Analysis
A Phenomenological Approach guided the design of this study whereby the focus of the research was on the commonality of a lived experience (Neubauer et al., 2019), in this case the practitioner role in PBS implementation. A latent approach within thematic analysis was used to interpret various aspects of the research questions in order to provide a rich detailed account of the data (Braun & Clarke, 2006).
The six phases of thematic analysis as outlined by Braun & Clarke (2006) were followed. Phase 1 involved familiarization with the data. As the researcher, collecting the data interactively and keeping a journal throughout data collection allowed for familiarization with the data. Phase 2 involved generating initial codes. The data was analysed on two levels with the researcher generating initial codes first and then focused codes. For example, Extract from transcript 4: ‘I think it’s how they view the behavior as well like if they don’t buy in to the idea that you’re working with the person or the environment, you’re never going to get on that well with them’. The initial codes generated for this quote included ‘highlighting importance of staff values & staff buy-in for PBS depending on belief in practitioner and positive relationship with practitioner. The focused code generated from the initial code includes; staff buy-in impacting implementation of PBS.
Data Analysis; Phase Two and Phase Three of Braun & Clarke’s (2006) six phases of Thematic Analysis.
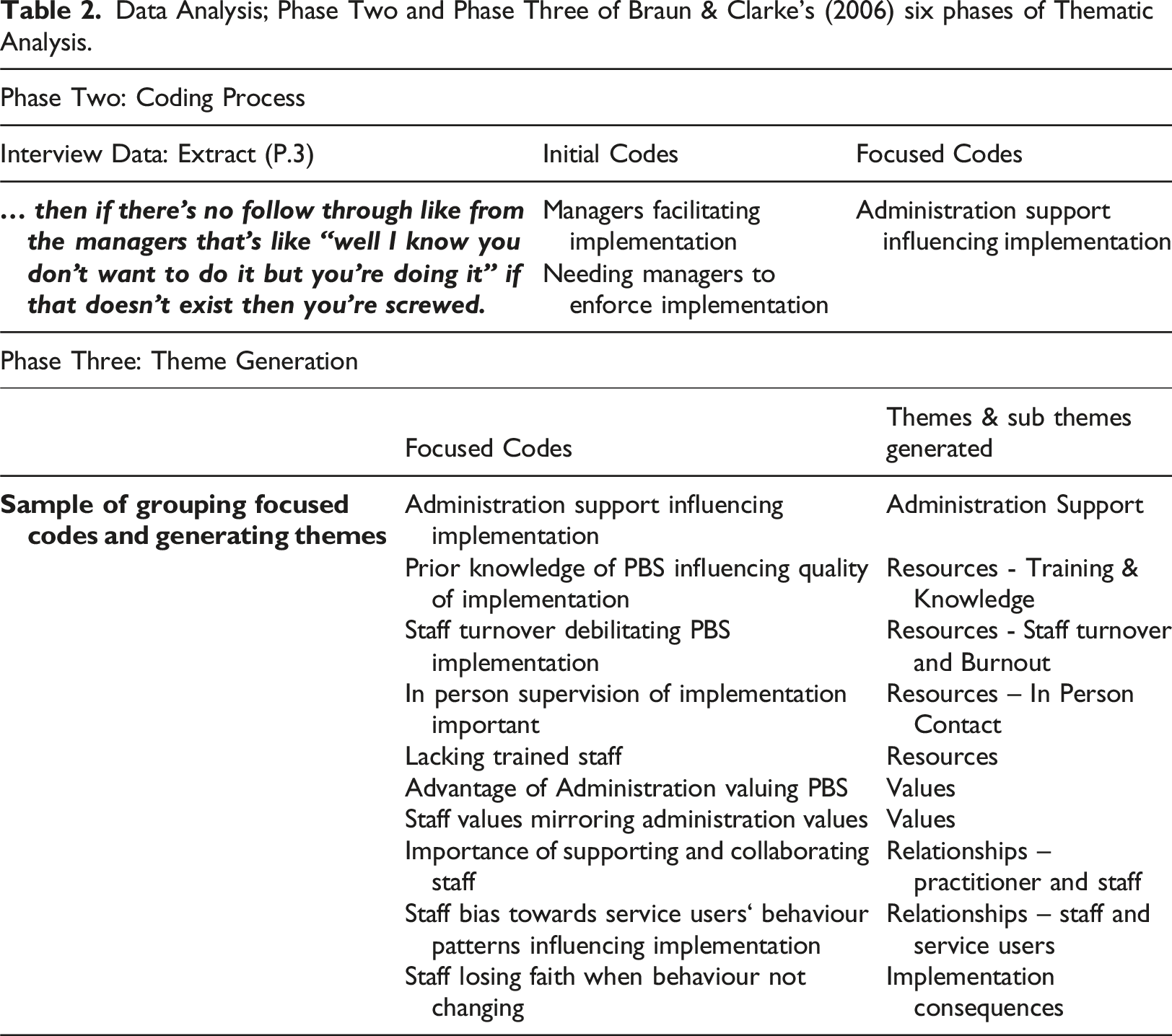
Phase 4 involved the refinement of themes. During this phase themes were grouped under main themes and analysed in their relation and connection to other themes. The final primary themes identified were Values, Resources, Relationships and Implementation Consequences with Administrator Support acting as the superordinate theme, connecting with and influencing each main theme significantly. Subthemes were grouped accordingly, however each theme is relative to another in its’ significance and presentation. Phase Five involved defining themes, writing a detailed analysis of each theme with examples from the data. Phase Six consists of the final write up of the report. When analysing the data, latent thematic analysis was used to search beyond the semantic content of the data. This approach involved looking for underlying assumptions and conceptualisations, that formed the semantic content.
The first author collaborated with an independent researcher who carried out phases two to six of Braun & Clarke (2006)’s thematic analysis on 20% of the data i.e. two full data transcripts and half of a third transcript. This process was in place in order to verify the theme refinement and ensure the absence of bias in the researcher’s identification of themes. There was clear consistency between both researchers in the theme identification and refinement.
Results
Administrator Support surfaced as the superordinate theme, given that all data appeared to be in some way influenced by the support of administration. The main themes which emerged included: (1) Values; (2) Resources, with sub-themes of; staff turnover and burnout, training and knowledge, time and in person contact; (3) Relationships, with sub-themes of practitioner and staff, staff and service user; and (4) Implementation Consequences. See Figure 1 for diagram of themes and sub themes. Participants collectively ranked BSP implementation high in their duties with considerable time allocated to this process within their respective organizations. Participants expressed that the responsibility for implementation was shared amongst themselves, frontline staff and the Administrator Support within their organization i.e. managers etc. Administrator Support includes support (i.e. financial, attitude, regulations) from any individual or organization in a superior role to the frontline staff member; for example, managers, team leaders, practitioners, service directors, and government agencies such as HIQA. As Social care organizations can be structured differently it is difficult to provide a generic model for the administration structure with respect to residential or day service for individuals with intellectual disabilities Results, Themes and Sub Themes.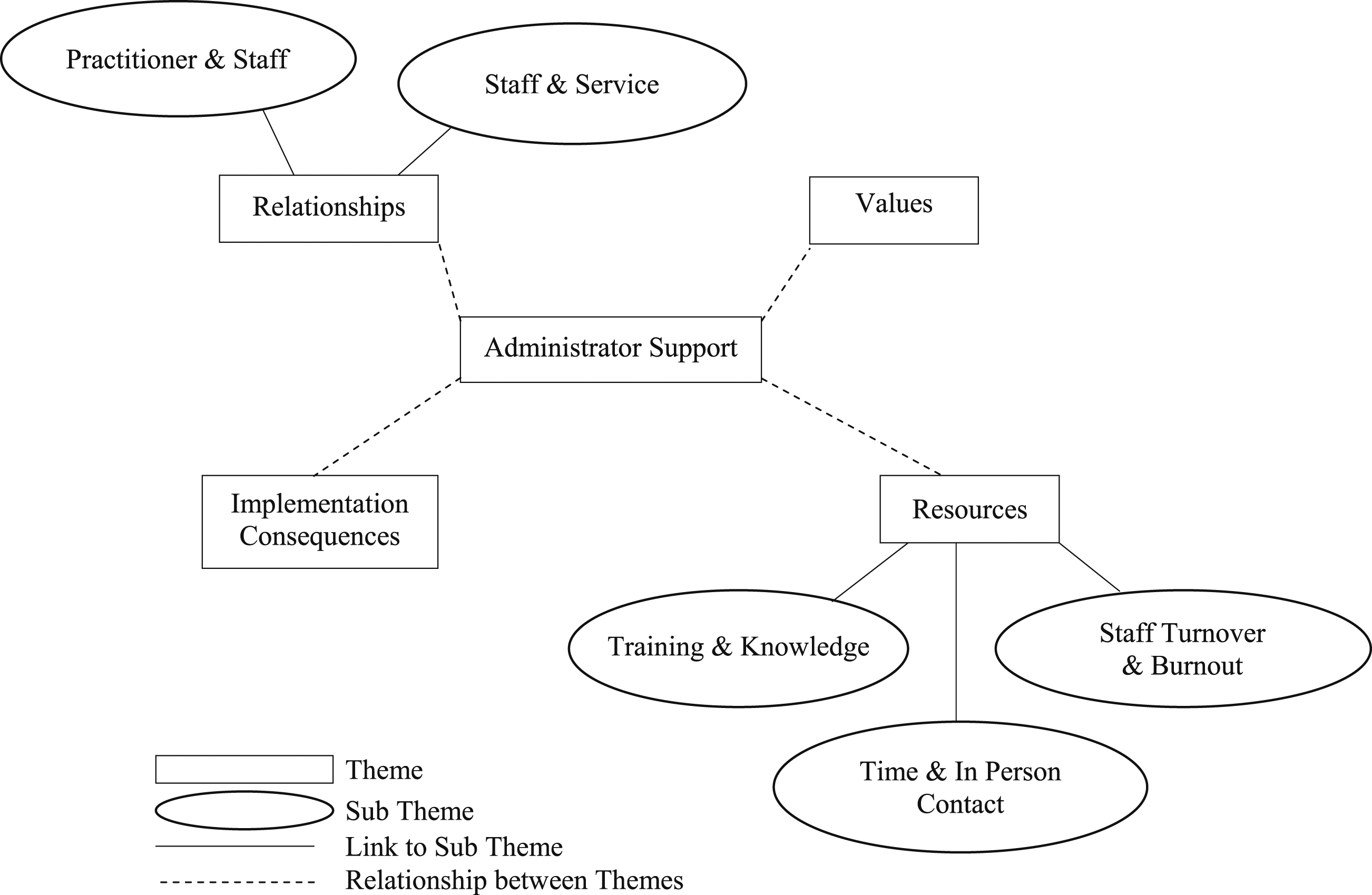
Theme: Values
Participants discuss the barrier of conflicting values between the practitioner, frontline staff and other members of the administration structure. Participants discussed the importance of administrator support within their organization, placing value on quality implementation and encouraging staff to do the same. Participants identified a barrier to implementation, when administrators place more value on the facilitation of other disciplines over PBS implementation, such as medical practice and medication delivery.
Participant (P).8: ‘...something was prescribed by a medic, by a GP, that’s more in their psyche to follow, because it’s prescribed..’
In particular, the value placed on medical practice over PBS implementation presented challenges when participants felt that medication was impacting the implementation process.
P.11: ‘they’re on high medication they can be reluctant to rock the boat and change it and I suppose people don’t give themselves enough credit for the proactive stuff they do but I think it can be hard to try and challenge medication’
It is identified as “something we’re definitely struggling with” P.11. P.11 gives examples of service users unable to participate in recommended skills teaching programs because of sedation side effects of medication and service users being subjected to restricted practices when they are unwell.
Experienced participants discuss the shift in values towards PBS over the years following the establishment of HIQA under the Health Act in 2007. However, participants discussed the lack of regulation of behavior support standards in HIQA policies, which is negatively effecting the implementation process. Participants collectively suggested that HIQA in its capacity as a regulatory body should place more value on evidence of implementation and clear regulated standards for the implementation process and what a BSP should include.
P.3: ‘ I see that like … things that [government agency] say have to happen, happen … they are priority. So if it’s going to come on the radar of the regulator … then it will definitely happen’ ….
Leadership from Administrator Support within organizations is recognised as a variable which influences the value placed on implementation of BSPs in organizations. Participants discussed how the attitude of the person in a managerial role within the organization influences the attitude of staff implementing the BSPs and how values can be encouraged and shaped in staff by a good leader.
P.12: ‘the value that is placed on … quality of life, .. reduction of restricted practices, … All of those things, if that doesn’t come across from an operational management level, then the people who are in direct support roles who are tasked with carrying out support systems that are based upon all those tenants, tend to not place very high importance on those systems’.
Staff values are widely attributed to quality implementation and participants discussed their responsibility of changing values, so staff appreciate implementation and the framework under which implementation is based. A significant challenge was identified when behavior support practitioners are faced with changing said values throughout operational management, as they do not hold a managerial role.
Participants collectively made the point that implementation could be improved if there was an organization wide values base and that this change could be achieved through behavior skills training. Changing mindsets is the process by which values are placed on PBS implementation and the collective feeling from participants is that when values are placed on implementation, implementation will be improved.
Theme: Resources
Resources (i.e. appropriate staff numbers, consistent staff teams, access to training, sufficient time allocated to each service user) is considered a main theme in the data. Resources in organizations can only be influenced by Administrator Support including various government agencies.
Sub-theme: Staff Turnover and Burnout
Staff turnover and inconsistent staff teams, was highlighted as a significant and reoccurring barrier to implementation across the data. High instances of turnover inhibit consistency due to the need to provide training to new staff, any delays in which can impact implementation. According to the participants, turnover impacts predictability, therefore turnover and consistency are inversely linked. Turnover is discussed in the context of consistency of implementation becoming impossible to achieve and also impacting the behavior of service users as predictability is diminished with high rates of staff turnover in services.
P.4: ‘Am a high turnover of staff so kind of unstable staff teams so even like coming back every week you might find different people working … it’s just completely around consistency … you need a stable environment with like suitable staff space and consistent staff team, you’re never going to make progress without either of those. You’ll really struggle’.
P.4 highlights the impending failure of implementation without staff consistency and environment, both variables of resources.
P.11: ‘if there is significant challenging behavior …staff burnout, staff are just managing behavior a lot of the time .. and I suppose when they’re not managing behavior they’re kind of anxious cause they think it could happen, am so I think when you have those situations where you have staff who are really highly strung … understandable, you have staff calling in sick a lot you have staff who are emotional and you’ve staff who are tired …’
P.11 acknowledges staff burnout as a significant barrier to implementation and this barrier is repeated throughout the data. This barrier is challenging to overcome when resources to support staff are lacking. Interestingly, all participants spoke about the potential for burnout of frontline staff but do not allude to the same challenges in their own role.
Sub-theme: Training and Knowledge
Training is seen to facilitate knowledge which by extension, facilitates implementation.
P.4: ‘I think people just find it easier to do things when they understand why they’re doing it ..’
P.4 explains the merit in training staff and how training facilitates knowledge in staff which leads to a greater likelihood that a BSP will get implemented, as staff understand the purpose behind it. Each participant discussed training procedures for staff when a BSP is provided to them for implementation, however training is delivered ad hoc, depending on the skill level of the staff.
P.9: ‘If they have a solid training base … that’s a huge factor’
P.8: ‘ there’s not enough training in the service … we don’t have people with a huge understanding of behavior apart from what they were reared with themselves, and old-fashioned discipline ideas and you can’t blame the staff for that …’
Participants discussed the importance of training and knowledge about the function of a behavior. They believe that this knowledge is necessary in order for staff to develop a shared understanding about why the behavior is happening and facilitates implementation. When training is delivered ad hoc and separately for each BSPs, staff are unable to generalise their training to different clients. P.5 discussed a recurring barrier in repeatedly training the same strategies to staff. However, P.5 also discussed staff overgeneralising strategies that are not appropriate for every service user. The above barriers can be overcome if staff attend further training and receive on-going supervision with opportunities to receive feedback from Administrator Support. However, to overcome the barrier of lack of training, time must be taken into account as a variable.
Sub-theme: Time and In Person Contact
Time was repeatedly discussed as a variable which influenced implementation. Participants acknowledged that having a lack of time to make contact in person with staff teams and service users, for in-situ meetings and training, was a barrier to implementation. P.3: ‘So like, for me to find the time to do as thorough function assessments, and behavior support plans .. and staff training in a training room environment … and ongoing review of data and implementation and change elements to a plan, to find the time for all that, in the context of the caseload I have is nearly impossible’.
Lacking time is a barrier reiterated throughout the data for all participants. Time is discussed as a barrier in the context of workload, as made evident by P.3 and also in the context of geographical spread.
P.7: ‘so we cover (3 counties) , so I’m the only BCBA so trying to travel all over is challenging and I’m based in (county 1) so (county 1) gets loads but (county 2) and (county 3) don’t get as much because I don’t have the time to go down or we wouldn’t have as much time to spend on those people’
The time it takes to cover the geographical spread was echoed as a barrier primarily by P.2, P.3, P.7, P.9 and P.12, all who are required to support implementation across a large geographical area. Participants highlight the need for more practitioners, to ensure implementation can be supported across such wide geographical spreads. Similar to staff and training, time is another barrier of resources, that needs to addressed by the relevant administrators.
Practitioners available time and using the time to travel in person to each service (residential or day) to meet with and observe staff teams in person, is highlighted as an important variable in implementation. P.2: ‘the amount of contact you can have with the staff team is very important … we were able to bring in some really cool supports because I was seeing the staff team on certainly on a weekly basis compared to a geographical distance one where I’m travelling over an hour to a service and I might only see them on a monthly basis’
Practitioners making contact in-person with a staff team allows for observations, feedback and monitoring of implementation, all factors identified as significant facilitators to implementation. Participants highlighted the importance of encouraging implementation, in person.
P.6: ‘it does involve just talking with them, reassuring them that, you know, their fears and anxieties are real. We can help you to control them, to be able to see a side of the person that you’re supporting beyond the challenging behavior’
P.6 presents the process of implementation and the importance of ensuring staff are confident in managing challenging behavior. P.6 acknowledges the need for in-situ conversations with staff and how this can only be achieved when time is available to sit with staff and provide reassurance.
Theme: Relationships
Relationships, in particular how the stakeholders connect and collaborate with each other were repeatedly discussed as a variable which influenced implementation. Two particular sub themes emerged from the data: the relationships between practitioner and staff and between staff and service users.
Sub-theme: Relationships between practitioner and staff
Participants collectively identified positive relationships with staff as a significant facilitator to implementation. Using a team approach was identified as facilitating to the implementation process. All participants echoed the importance of collaboration and how including staff at each stage of the process facilitates implementation and the development of positive working relationships. This theme reiterates stakeholder involvement, one of the nine defining characteristics of PBS.
P.4: ‘It’s a lot down to having a good relationship with the team and finding a valid way of supporting them so not just throwing recommendations at them and walking out the door’
All participants discuss the importance of investing time in order to build a relationship with staff. Having a relationship with staff facilitates open communication and a greater likelihood that staff will communicate barriers to implementation with the behavior practitioner. Participants discussed their reliance on staff and managers to communicate these issues to the behavior practitioner when they are not available to monitor implementation.
P.7: ‘I was off on maternity leave for 9 months and there was somebody in covering me and there definitely wasn’t as many referrals and then I came back and there was a long list of referrals for me so they obviously didn’t refer to her’
P.7 discusses how she built a relationship with staff teams over the years and felt staff were comfortable approaching her with barriers and ideas for implementation. The relationship is evidently important as staff refrained from referring to a substitute therapist having no relationship developed and no established line of communication.
P.9 discussed the importance of building relationships with staff and the skills that are involved in this process, identifying areas for skills development in behavior support practitioners.
P.9: ‘but there is actually a good bit to do there in terms of understanding where staff are coming from, I think there should be more active discussion around that and sometimes behavior analysts don’t have the skills to do that’
P.9 highlights how practitioners sometimes have difficulty relating to staff and understanding the challenges facing staff. P.9 highlights how this skill deficit is an area for development that can largely impact the quality of implementation, and by extension, the quality of service provision from behavior support services.
Sub-theme: Relationships between staff and service users
Participants collectively identified positive relationships between staff and service users and staff knowing the service users well, as a consistent facilitator to implementation.
P.5: ‘to be honest they just need to be good with the person’
P.2: ‘a lot of the work in terms of the process is helping the staff to understand the importance of the relationship they have with the individuals, therein lies the heart of the strategies we would put in’
Participants evidently value the relationship between staff and service users and some participants linked the relationship back to values towards individuals with disability. Both P.5 and P.2 highly rank the relationship in terms of factors enabling implementation, with P.5 valuing the relationship over knowledge and expertise of the staff member. P.2 acknowledges their responsibility in helping staff to see the value of their relationship with service users.
P.3 explains how cultivating empathy in staff members can support the relationship, or help to build on poor relationships between service users and staff.
P.3: ‘I think a big part of it is empathy ..(describing case with challenging individual and negative attitudes from staff towards individual) …but the light bulb moment on the staff going “God yeah …I never thought of it like that’.
P.3 discussed empathy in the context of relationships between staff and service users, and how empathy can be viewed as motivation to stay with the plan.
Theme: Implementation Consequences
Each theme discussed thus far relates to the process preceding implementation, however, consequences of implementation or lack thereof, was identified as a theme across participants.
Occasionally, the immediate and perhaps temporary consequence of implementation can be nothing as it can take time for changes in behavior to be seen.
P.6: ‘I think sometimes what happens then is once they implement, implement strategies …, they expect the person to respond quite quickly and of course that doesn’t always happen … so it can be a bit frustrating. So they might say “oh it’s not working’.
P.6 acknowledges how it can be frustrating for staff when results cannot be seen following implementation. P.8 reiterates this challenge and how it can deflate staff’s motivation to implement and how the opposite can also be true where they see an immediate effect, ‘When they see an immediate effect they will keep doing it’. P.5 emphasised the importance of drawing staff attention to small progresses and minimal changes in behavior to provide reinforcement for implementation and motivate staff to continue implementing even if they are not seeing any significant changes.
When discussing the importance of Administrator Support, participants highlighted the need for managers to hold staff accountable for poor implementation.
P.3: ‘then if there’s no follow through from the managers that’s like
“well I know you don’t want to do it but you’re doing it”, if that doesn’t exist then you’re screwed’
P.3 identifies a reliance on support from relevant administrators, such as managers and team leaders, to hold staff accountable for poor implementation. All participants highlighted their lack of authority in their role as the practitioner. Participants identified their responsibility to aid the implementation process when poor implementation is accounted for by lack of knowledge and skills in staff. However, participants collectively identified the responsibility of managers to address poor implementation in staff when the issue is attributed to poor motivation or considered an operational issue.
P.1: ‘HIQA puts all their emphasis on the other aspects of the service, their feedback can be conflicting … staff see that as well and when they’re reading reports and they see feedback, they’re prioritising and if the behavior aspect isn’t up there even from a HIQA point of view….’
P.1 explains the impact of staff seeing negative feedback from Administrator Support influencing staff motivation to implement and the value staff place on implementation. It is the view of participants that consequence of negative feedback towards implementation, or lack of positive feedback, can impact staff motivation towards implementation.
Discussion
This study sought to explore facilitators and barriers to the implementation of behavior support plans and behavioral recommendations from the perspective of practitioners working in a behavior support capacity within the Intellectual Disability sector in Ireland. By talking with practitioners about the process of BSP implementation within their respective organizations, this study offers insight to the relationship between multiple variables and the implementation of BSPs in intellectual disability organizations. The variables which are thought to impact on the implementation process are presented as themes. Each theme is connected to another, influencing the impact of the variable on the implementation process.
Administrator Support was identified as the superordinate theme across the data, influencing all other themes in a natural operational management chain. Administrator Support includes management, team leaders, behavior support practitioner, directors, and government agencies. Staff values and the importance of Administrator Support in encouraging staff to value implementation was identified as a significant theme influencing the implementation process. The impact of this within the organization, is the frontline staff then consider other factors as holding more value (i.e. medication), in terms of its impact on behavior change, rather than proactive behavior support recommendations. This influential position of administrative support’s values, and its bearing on staff’s values, can hinders implementation of PBS and is a challenge for behavior support practitioners when they are striving to achieve a balance between BSP implementation and necessary delivery of other interventions (i.e. medication). Administrator Support was also found to influence resources, which presents as a significant theme across the data including monetary resources, time and in person contact, training facilities and staff. One barrier that exists is that behaviour skills training is often optional and if it were to be mandatory, organization wide change in values could be achieved which would improve implementation. Administration support could further support training by making some elements mandatory and making it a priority for staff to attend such trainings.
Relationships was viewed as a theme including relationship between practitioner and staff and service user and staff. With respect to the relationship between practitioner and staff in-person contact with a team is considered an important factor in developing relationships. When services have the resources to ensure consistency in staff, adequate training and skills development in staff, sufficient time for a practitioner to make frequent contact with service-users and staff, then implementation can be facilitated. Finally, the consequences of implementation was identified as a theme related to the facilitation of implementation, which is also influenced by Administrator Support in terms of the feedback staff receive from their superiors.
It is important to recognise the connection between the identified themes and the characteristics of Positive Behavior Support (PBS). In particular, Systems Change is one of the nine defining characteristics of PBS and is highly represented by the superordinate theme in the current study, Administrator support. Similarly, the importance of collaboration and relationships is reflected in the inclusion of relevant stakeholders, another defining characteristic of PBS (Johnston et al. 2006).
The themes generated in this study are in line with the existing literature. Within the current study, Administrator Support was identified as the super-ordinate theme. This finding is in line with previous research by McIntosh et al. (2014) and Pinkleman et al. (2015) who both founds that school administration support was a significant enabler to PBS implementation and sustainability, within the context of schools. The enabling factor of School Administrator Support is considered to be the leader’s belief in the plan and to show the staff why it is important. Within their studies, School Administrator Support included principals and vice principals, but did not include school district supporters. Within the current study, the data suggests that Administrator Support influence goes beyond the direct leaders in the organization (the equivalent to school principals), and includes government agencies. This finding is in contract to Pinkleman et al. (2015) and may be accounted for by the different context in which Administrator Support can play a role depending on the organizational structure and governance. For example, social care organizations, which are audited or under evaluation, may be more influenced by external authorities than schools.
Within the current research the values held by staff were largely deemed to be influenced by higher levels of management or governance (i.e. administrative supports) which held the potential to adapt an organisation wide values based in support of PBS and an emphasis on implementation. Participants collectively voiced the fact that organizations may demonstrate their commitment to their values base through ensuing that behavior skills training is mandatory, which would improve implementation. The current findings on the theme of values are considered directly linked to “buy-in” noted in previous research (Pinkleman et al. 2015; Kincaid et al. 2007; Castillo et al. 2016; Bambara et al. 2012).
Resources or lack of resources and lack of trained staff were first identified as a challenges by Allen et al. (2005) and was echoed by Kincaid et al. (2007). Kincaid and colleagues mentioned staff turnover but did not consider it a highly important factor, as it was in the current study. This contrast may be accounted for by the setting. Staff turnover is perhaps traditionally higher in social care organizations as opposed to schools, an important contrast to highlight when evaluating the literature and the importance of this variable. Unfortunately, even if staff value implementation, implementation cannot occur if those staff members are being moved around or are leaving the service. Staff leaving and high turnover can be attributed to the intensity of the workload and resources are needed to support staff and avoid burnout.
Furthermore, staff turnover has a knock on effect on the training and knowledge of staff as the loss of staff ultimately results in the loss of skills, which then becomes circular as further resources are required in order to train new staff. These findings are supported by related literature on the effectiveness of interventions, which reported staff access to training (Selick et al. (2017) and resources (Castillo et al., 2016) as a significant variable influencing implementation. With respect to training needs the current research yielded some interesting findings. In particular, all training for front line staff on implementation should include the organizations value base. With respect to the participants themselves, it was identified that they are practitioners and that they may need training in building relationships and connecting with staff and this was intrinsically linked to the final theme of relationships.
In the current study, relationship building was largely connected to resources (e.g., time and physical contact). It would appear from the literature that in person contact is not a commonly mentioned facilitator to implementation, although it was consistently mentioned as a significant facilitator across the data. Increasing staff self-efficacy is largely influenced by resources, as staff require training and therapeutic support, to overcome their apprehensions toward implementation and for practitioners to have the time to address this with staff.
Perhaps, similar to Staff Turnover and Burnout, the amount of in person contact is influenced by the context. For example, intellectual disability services are often provided on a smaller scale and embedded within the community, contributing to the larger geographical spread of an organization across a region, thus often requiring behavior support practitioners to travel for long periods of time from service to service with the time spent in the car considered unproductive. The geographical spread and the time required to cover all services impacts the on the time available for the behavior support practitioners to provide in person meetings or undertake on site observations (i.e. physical contact) with staff teams. This is in contrast to schools which cater for large numbers of children at one fixed location. There are other elements that may contribute to less turnover and burnout in a school setting such as the regular working hours as opposed to shift work and school holidays.
The current findings show the relationships between the behavior support practitioner and staff, and between staff and the service users are both hugely important in facilitating implementation. Firstly, the relationship between the behavior support practitioner and the staff team should be a team approach and involve a collaborative processes where the contribution of all members is valued. This finding is in line with Bambara et al. (2012) who found that positive working relationships between families, staff and administrator support was a key enabler. This finding highlights the importance of collaboration and open discussion of barriers, which is mirrored within the current findings. Secondly, the relationship between staff and service user is considered to be highly important in facilitating implementation. This is supported by existing research by Nilsen et al. (2015) and Selick et al. (2017) who report that the relationship between staff and client is critical to successful engagement with their respective interventions. Within the current research, the enhancement of the relationship between staff and the individuals they support was linked to the establishment and development of empathy. Empathy is a powerful force that helps maintain relationships and is the mechanism that allows people to understand and relate to others. The development of empathy often encourages cooperation and forgiveness, strengthens relationships, decrease judgment, and even improves mental and physical health (Batson, 2011).
Similar to each of the theme identified within the current research, consequences to implementation is highly influenced by Administrator Support as behavior support practitioners highlighted the need for Administrator Support to acknowledge good implementation and to hold staff accountable for poor implementation. This theme is reflected in the recognition of Administrator Support and policies in the literature as a facilitator to implementation (Pinkleman et al., 2015; Castillo et al., 2016). The importance of gaining insight from the behavior practitioner perspective is most evident within this theme. Participants within the current research highlighted that they are powerless in this aspect of their role as they do not hold any managerial status, and their recommendations are merely advise or guidance that they cannot enforce, thus they feel their impact on implementation is low, unless they receive Administrator Support. The implementation of consequences is considered a reactive approach to poor implementation and while considered to be important and needed in some circumstances, other themes represent more proactive variables in the implementation process and are considered more impactful.
Limitations
Limitations should be considered along with the findings. It is difficult to grasp the sample size of this study in relation to the larger population of behavior support practitioners as there is no data available on the number of professionals working in this capacity within intellectual disability organizations in Ireland. As the current findings indicate that this context is sufficiently different to research previously undertaken in schools, the results of this study should guide further research to determine whether the facilitators and barriers identified by the participants are representative of this population. The duration of time spent in their current role may be considered a limitation for two of the participants, as they had worked in their current role for less than 1 year. Given that participants’ insights are evidently shaped by the extent of their experience, one year may not have been a sufficient duration for them to become aware of all issues impacting on their role. However, it is worth noting that P.3 is in their current role for 9 months, however, they had previously worked in the field of positive behavior support for 13 years so may be able to draw on their previous knowledge and draw comparisons across organizations.
Future Research
This study presents preliminary findings as this is the first qualitative examination of this research question with this population. Although some of the current findings are consistent with previous findings represented in the literature, further research is warranted into barrier and facilitators in intellectual disability organizations. It may also be important to undertake research with frontline staff and managers working in intellectual disability organizations to identify if similar themes are found among other staff working in this sector. As the theme Administrator Support was identified as superordinate and directly influenced all other themes, it is suggested that participants who work in Administrator Support capacities should also be included in future studies, for example, managers, directors, team leaders and perhaps governing agencies such as HIQA regulators.
As stakeholders aim to be collaborative in implementation, researchers should aim to be collaborative in analysis. Therefore, it is also suggested that efforts are made to statistically analyses implementation across organizations. The difficulty around confidentiality and ethics of investigating proof of implementation is evident, however in order to categorically assess the standards of implementation across organizations, efforts need to be made to appropriately assess the level of implementation in social care settings.
Conclusion
The findings of this study present themes related to facilitators and barriers to implementation of BSPs from the practitioner’s perspective. Based on the findings of this study, it is evident that facilitators and barriers do have a role to play in the implementation of PBS. Administrator Support was identified as a superordinate theme influencing Values, Resources, Relationships and Implementation Consequences. Evidently, the findings show how the implementation process relies on the variables identifies as themes in this study and further research is needed to confirm the findings in relation to the general population of behavior support practitioners working in intellectual disability organizations.
Footnotes
Author notes
The research was conducted by the first author under the supervision of the last author in partial fulfilment of the requirements for her MSc in Applied Behavior Analysis at University of Galway.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.