
Abstract
Introduction
Over the past few decades, there has been an increasing focus on promoting self-determination for individuals with intellectual disabilities (Kúld et al., 2023; Wehmeyer, 2001, 2020). This entails granting individuals with intellectual disabilities the opportunity to make their own choices and decisions regarding their lives, allowing them to act as primary agents in their own lives. Respect for self-determination also requires reducing restrictive measures as a form of coercive care. Restrictive measures can broadly be defined as any actions that are resisted by a person and limit volitional behaviour. Legal frameworks, in the Netherlands as well as in other countries, assert that such coercive care should be minimized wherever possible. Since 2020, the Care and Coercion Act (Wet zorg en dwang psychogeriatrische en verstandelijk gehandicapte cliënten Care and coercion act psychogeriatric and clients with intellectual disability, 2020) has been in effect in the Netherlands, formalizing the obligation of care organizations to continually work towards reducing restrictive measures. Bakkum et al. (2023), for instance, reported a significant reduction in registered involuntary care following the introduction of the Act in a large care organization in the Netherlands. The Care and Coercion Act aligns with the United Nations' Convention on the Rights of Persons with Disabilities, which became effective in 2008 (United Nations, 2008). The systematic elimination and reduction of restrictive measures belongs to standards for good care across various countries (Deveau and McDonell, 2009; Frederiks et al., 2017; Schreiner et al., 2014; Singh et al., 2009). Consequently, care organizations are confronted with the challenge of effectively addressing the reduction of restrictive measures in a sustainable manner, grounded in scientific knowledge. The current study describes how this may be done through the Multidisciplinary Expertise Team (MDET) program and investigates its effectiveness in reducing restrictive measures within sheltered care homes for people with intellectual disabilities.
In the Netherlands, prior to 2020, restrictive measures were broadly defined as any action that limited the autonomy or freedom of a person with an intellectual disability in a specific situation. With the Care and Coercion Act of 2020, coercive care remained broadly defined into nine categories. These categories are (1) administration of nutrition, hydration, or treatment; (2) restriction of freedom of movement; (3) seclusion; (4) surveillance; (5) clothing or body searches; (6) searches for dangerous materials or substances in private property; (7) checks for the presence of drugs; (8) freedom restrictions in daily life; and (9) visitor restrictions.. The new act, however, emphasized that resistance to such measures is required to classify these as coercive care. People with intellectual disabilities may, however, not always overtly express their resistance. Therefore, care staff need to be made aware of the wide spectrum of actions that clients may perceive as restrictive, as highlighted by Frederiks et al. (2017). Consequently, the description of distinct types of restrictive measures should be comprehensive and non-limitative in nature to account for their diversity. Additionally, it is crucial to understand what is considered restrictive through dialogue between clients, their families, and staff members to take the perspectives of clients into account (Embregts et al., 2019).
The multidetermined nature of restrictive measures (e.g., Richardson et al., 2020) as well as the numerous contextual factors that facilitate or hinder the implementation of healthcare innovations (Fleuren et al., 2004; May et al., 2016) suggest that a multidisciplinary, multi-component approach is essential for its reduction. While understanding individual residents' behaviour and tailoring responses, for example through Applied Behaviour Analysis (Williams, 2010) or Positive Behavioural Support (LaVigna and Willis, 2012) may be helpful in many cases (Iffland et al., 2024), other situations may require different interventions, for example aimed at staff-client relationships or group dynamics. A meta-analysis of non-pharmacological interventions for challenging behaviour of adults with an intellectual disability concluded that overall this group of interventions are moderately effective but also that no particular intervention or technique stands out unequivocally as being more effective than others (Bruinsma et al., 2020). Intervention programs that target multiple levels simultaneously, including the resident, staff members, and the broader organization, may be needed to achieve overall reductions instead of replacing one restrictive practice with another. Björne et al. (2022) surveyed staff members of community services for individuals with intellectual disabilities in Sweden to identify the factors necessary for reducing the use of restrictive measures. Structural characteristics of the service, including its design and staffing, broader policy and legislation, and the training and supervision of staff members, were cited as critical factors. However, Björne et al. (2023) found that practical challenges such as limited time and resources, inadequate environments, and a shortage of skilled staff make it challenging to effectively reduce the use of restrictive measures.
Several studies have been conducted to study effectiveness of intervention programs targeting multiple levels simultaneously. First, a study on a multi-component approach intervention, combining Positive Behavioural Support, Safewards (an integrated model for conflict and containment in psychiatric wards), and data-led practices (including restrictive care monitoring), showed a 42% reduction in the overall use of restrictive measures, a 42% reduction in seclusion, and a 52% reduction in the use of rapid tranquilization (Riding, 2016). Schreiner and colleagues (2014) described a multi-component approach for their clients with developmental delays and severe psychiatric disturbances. Their approach involved assessment of the restrictive measures and employed a comprehensive evaluation of the factors initiating and perpetuating the use of these measures. Guided by this evaluation, they implemented interventions that included staff education, client treatment, and the promotion of collaboration between a multidisciplinary advisory committee and an interdisciplinary treatment team. As a result of their intervention, the use of seclusion decreased by 35%, and the use of mechanical restraints by 43%. Finally, Williams and Grosset (2011) examined the implementation of an organizational behaviour management (OBM) plan to reduce the use of mechanical restraints in a residential setting for individuals with intellectual disabilities. Their intervention provided direct instruction to implement behavioural intervention plans and had the management team provide positive or corrective feedback to the support staff. After 17 months, they observed an 80% reduction in mechanical restraints, and the use of behavioural intervention plans doubled. None of these studies, however, included a control or care-as-usual group in their designs.
Building on previous work, a multi-component intervention was developed to address the complexity and multiformity of restrictive measures in the context of integrated care offered in sheltered care homes in the Netherlands, the Multidisciplinary Expertise Team (MDET) program. This multi-component intervention assembles a team of professionals from various disciplines from the care organization, all recognized for their expertise in fields that are relevant to reducing restrictive measures. They undergo additional training to ensure that they possess the current scientific, legal, and practical knowledge on the subject. The MDET program has a threefold focus: 1) raising awareness regarding the use and the causes of restrictive measures and monitoring the registered deployments of these measures; 2) providing multidisciplinary consultation at the staff level, and 3) delivering multidisciplinary consultation and intervention at the residents' level. Throughout a consultation process with the care unit staff within the organization, the MDET aids in identifying all forms of restrictive measures applied to residents, with the goal of responsibly and sustainably reducing these. The MDET approach is systematic and aligns with the prescribed procedures outlined in the Care and Coercion Act (2020) in the Netherlands.
This study
The primary objective of this cluster randomized trial is to evaluate the effectiveness of the MDET program in reducing restrictive measures in residential care units for individuals with an intellectual disability compared to care as usual. To address potential confounding with effects of the MDET program on registrations of restrictive measures through increased awareness, we also tested effects for restrictive measures that were registered before the start of the program.
Methods
Study setting
The care organization in this study served at the time about 9,500 individuals with varying degrees of intellectual disabilities, spanning all age groups and across hundreds of locations. The organization operates across the Netherlands, offering a spectrum of services including sheltered care homes, day care, and outpatient clinic care. Their services encompass several types of support, such as living support for individuals with intellectual and physical disabilities, and treatment for additional mental health problems, challenging behaviours, and physical problems. For this study’s purpose, we selected a random sample of 50 care units from the 566 24-hour care units within the organization. Care units were eligible for inclusion if they provided support to a minimum of four residents, a criterion established to facilitate the estimation of unit-level effects (Snijders and Bosker, 2011).
Design and procedure
The staff and residents of the care units were informed about the study and requested to provide their consent for participation. Staff members were informed and consented to the study through email, with a subsequent phone conversation if necessary. No staff members declined participation. The residents or their legal representatives were contacted via a letter containing detailed information about the study and an informed consent form. The ability of residents with an intellectual disability to provide their own informed consent was determined through consultations involving the care staff, legal representatives, and the residents themselves. Following the letter, an employee of the care organization conducted a follow-up phone conversation. At the study’s onset, 202 residents either provided written informed consent themselves or had it provided by their legal representatives. Subsequently, there was a drop-out of 33 residents because no restrictive measures were recorded during the study, and 62 more residents were excluded because they changed care units during data collection. The medical ethical review committee of VU medical centre approved the informed consent procedures and privacy protocol (12/065).
To evaluate the effectiveness of MDET in reducing restrictive measures, a cluster randomized trial was conducted. In this trial, an independent researcher employed a random number generator to randomly allocate the 50 care units in the sample into two groups: an experimental group and a care-as-usual group. Consequently, residents and their recorded restrictive measures were grouped as clusters and assigned to the group of their respective care unit. In the experimental group, care units followed the MDET consultation trajectory (see below for a detailed description of MDET). Meanwhile, the care-as-usual group received the standard amount of support for the staff members. Within care-as-usual, it is customary for the care unit’s coordinator to organize regular meetings with the support staff, the consulting physicians, and therapists to discuss the clients’ care (not only focused on restrictive measures). Furthermore, care-as-usual also underwent organization-wide efforts aimed at reducing restrictive measures (such as campaigns to increase awareness of the use and the prevention of restrictive measures). The implementation of a mandatory registration system to record all instances of coercive care was part of these organization-wide efforts.
Researchers sent periodic reminders to ensure the registration system’s accuracy and cross-checked the entries by comparing them with the residents’ electronic files and treatment plans. Additionally, the registry featured precise start and end dates for each recorded restrictive measure. Only registrations for residents from whom written informed consent was obtained and did not change care unit (n = 107), were considered in this study, encompassing a period spanning from three months prior to the intervention to 18 months thereafter.
Multidisciplinary Expertise Team (MDET)
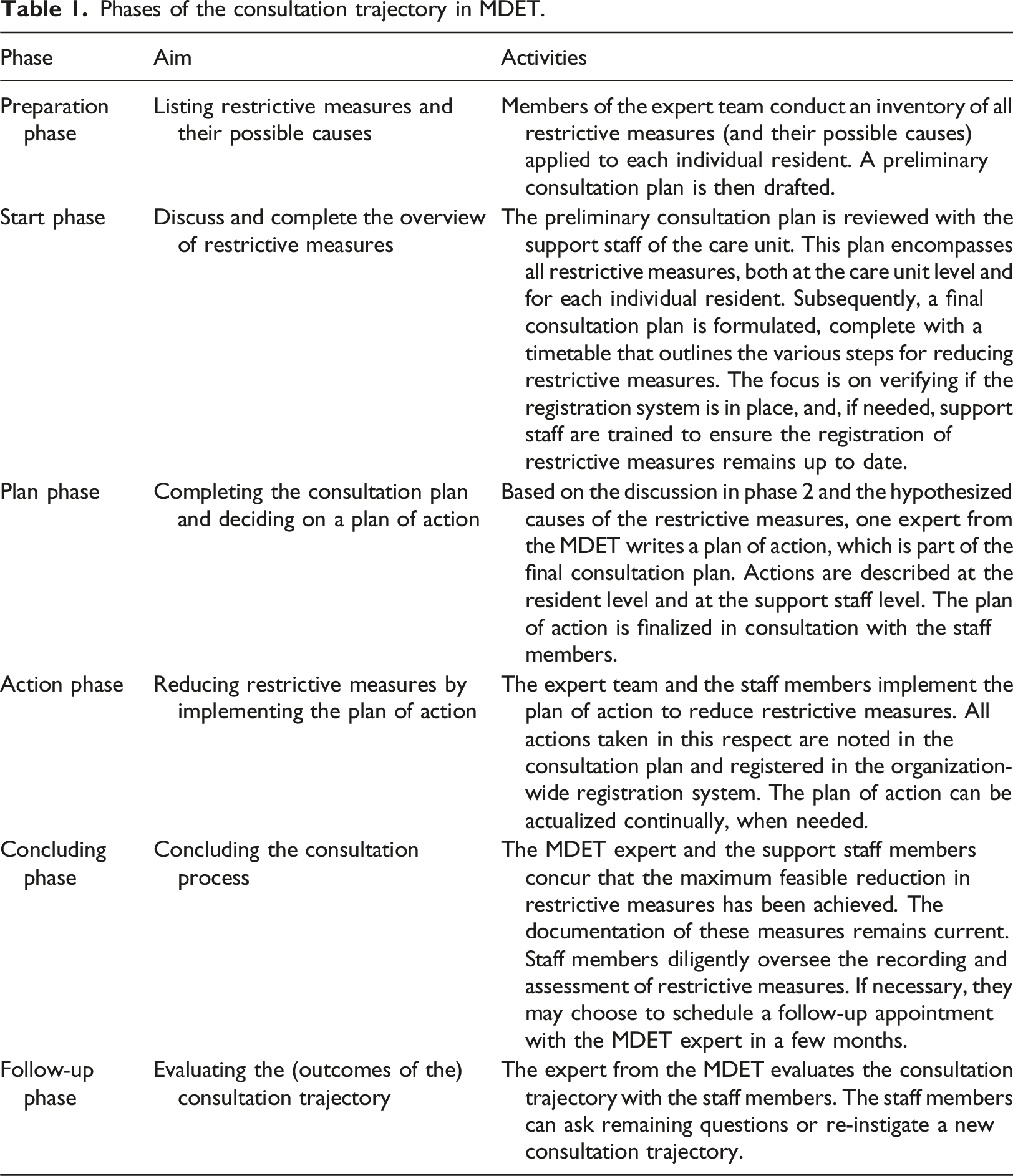
In the experimental group, care units followed a systematic and step-by-step consultation trajectory with a Multidisciplinary Expertise Team (MDET) to reduce the restrictive measures they employed. This consultation trajectory encompassed developing a plan at the care unit level and the individual resident’s level. Based on the multidetermined nature of restrictive measures, as reviewed in the Introduction, the MDET comprised experts from various disciplines within the organization, including special education specialists (in Dutch “orthopedagogen”) (n = 7), psychologists (n = 2), behavioral therapists (n = 2), physicians (n = 2), physical therapists (n = 2), an occupational therapists (n = 1), video feedback trainers (n = 4), a manager (n = 1) and a resident representative (n = 1). All MDET members were employed by the care organization and possessed expertise in the domain of restrictive measures specific to their respective disciplines. These disciplines were chosen for their expertise regarding factors associated with restrictive measures or their reduction (such as communication difficulties, antipsychotic medication use and a diagnosis of autism; May et al., 2016; Richardson et al., 2020; Riding, 2016). The MDET was supervised by a coordinator and a researcher (the first author) and received additional training before the study’s commencement (e.g., certification in functional behavioural analysis). The first and second author educated the team on the legal framework governing restrictive measures in the Netherlands, as well as the policies and regulations of the care organization. Within each discipline, experts identified areas requiring further training, which were accommodated within the study. Regular meetings were held among all MDET experts to provide mutual advice and consultation, each contributing their discipline-specific expertise.
Phases of the consultation trajectory in MDET.
Outcomes
The outcome variable in this study is the cessation of restrictive measures that were applied to individual residents either before the study’s commencement or during its course. In accordance with the Dutch Care and Coercion Act of 2020, restrictive measures are defined as any form of restrictions or coercive care that a client opposes. This resistance may manifest in overt expressions or be concealed, deferred, or gradually diminished through habituation. Therefore restrictive practices were recorded unless residents had agreed with such a measure.
Over a period of two years, data was collected through the organization-wide registration system. Within this system, staff members documented all restrictive measures applied to individual residents, irrespective of the resident’s expression of resistance, and integrated these records into the electronic files of the residents. The registration system encompassed a comprehensive list of 76 restrictive measures, based on the nine categories of coercive care in the Care and Coercion Act. Reliability was established in Schippers et al. (2018), prior to the current study. The list was based on information from three primary sources: scientific literature, data from the Dutch Health Care and Youth Inspections, and input from a committee on restrictive measures within the care organization. Examples of restrictive measures from this list include ‘Physical restraints (holding down body parts)’, ‘Mechanical restraint of feet and legs’, ‘Camera/video surveillance (within resident’s private room and/or communal areas)’, ‘Locking the outer doors’, and ‘controlling access to a mobile phone’.
All restrictive measures in the list were categorized into four pre-defined subsets. The first subset (n = 14) included measures aimed at protecting or preventing direct danger, such as physically restraining a resident to prevent physical aggression. The second subset (n = 46) encompassed measures designed to prevent indirect danger or disadvantages (on the long-term), such as adhering to a strict daily program or dietary restrictions and rules governing the use of mobile phones. The third subset (n = 6) aimed to have surveillance on the residents by utilizing, for instance, surveillance technology, while the fourth and final subset (n = 10) encompassed measures to physically support the residents by using, for instance, ergonomic materials. Medications used to manage residents’ behaviour were not documented in the registration system by physicians due to a lack of consensus regarding which medications constituted restrictive measures and which did not. However, the administration of medication under coercion or without informing the resident was included in the list. Registration was dichotomous (a restrictive measure was either applied, denoted as ‘1’, or not applied, denoted as ‘0’, during a given work shift) and was regularly updated by staff members. Internal consistency was found to be inadequate for the four pre-defined subsets of restrictive measures, with Cronbach’s alphas .42 for protective measures, .43 for preventive measures, .54 for surveillance, and .61 for physical supports. Analyses were therefore only conducted on the overall number of restrictive measures (Cronbach’s alpha estimated at .80).
Data analysis
The dataset in this study had a hierarchical structure, with restrictive measures (level 1) nested within residents (level 2), who, in turn, were nested within care units (level 3). It contained information regarding the cessation of restrictive measures during the intervention period. Cessation was operationalized as a dichotomous variable, with ‘1’ indicating that the restrictive measure stopped, and ‘0’ indicating that it continued. The effect of the MDET program on the reduction of restrictive measures was assessed using generalized linear mixed modelling. Mixed modelling is an appropriate technique for datasets with a multilevel structure, as it correctly accounts for the dependencies among observations from the same clusters (in this case, restrictive measures were clustered within residents, and residents were clustered within care units) (Hox et al., 2017). More specifically, a binary logistic regression model (with logit link function) was used due to the dichotomous nature of the variable for cessation of restrictive measures. First, an empty model was specified to represent the hierarchical data structure without any predictor variables. In this model, the intraclass correlation (ICC) was computed for the level of restrictive measures and for the level of residents by quantifying the proportion of variance in the outcome variable attributed to each level (Davis and Scott, 1995). Second, the predictor ‘group’ was introduced into the model, with group 1 representing the experimental group and group 0 representing the care-as-usual group.
Furthermore, the analyses described above were repeated, including only the registrations of restrictive measures that were recorded prior to the study’s initiation. This step was taken to rule out the possibility that the intervention’s effect was solely attributed to increased awareness of restrictive measures due to the study, which might have led to more registrations of restrictive measures and an enhanced urge to reduce them. All analyses were performed using SPSS Version 23, using a statistical significance level of .05.
Results
Descriptive analyses
At the start of the study, consent was provided by 202 residents (or their legal representatives) distributed across 40 care units. Records of restrictive measures were available for 169 residents across 39 care units. Residents who transferred to a different care unit during the study (n = 62) were excluded, resulting in the inclusion of restrictive measures recorded for 107 residents in 30 care units. In total, the organization-wide system contained records of 428 restrictive measures, with an average of 4 per resident (range = 1-18), spanning across 41 different types, either at the beginning of the study or during its duration. The most frequently recorded types of restrictive measures were audio surveillance (registered for 40.2% of the residents), surveillance technology detecting whether a door opens (registered for 25.2% of the residents) and locking the outer doors (registered for 24.3% of the residents). Sixteen types accounted for 80% of all recorded restrictive measures.
Effectiveness of MDET
The proportion of restrictive measures that ended during and after the intervention period was 40.4% in the intervention group and 20.3% in the care-as-usual group. Statistically significant variance was observed across units (z = 2.05, p = .04), but the variance across residents was not statistically significant (z = 1.11, p = .27). The ICC correlation at the unit level was .25, and at the resident level, it was .06. An ICC greater than .05 indicates that the clustering dependencies cannot be disregarded, warranting the use of multilevel analysis (Hox et al., 2017). In other words, 25% of the variance in reducing restrictive measures could be attributed to differences between care units and 6% to differences between residents. Nesting of restrictive measures within residents and units was therefore included in the multilevel model, to avoid bias in testing the testing in intervention versus care-as-usual group. Analyzing the extent of the reduction in restrictive measures before and during the intervention period revealed a significant positive effect of the MDET program on the reduction of such measures (b = 1.42, t = 2.87, p = .009). In other words, the intervention group showed a significantly higher proportion of restrictive measures that were ended compared to the care-as-usual group. The intervention explained 9.3% of the variance in reduction across restrictive measures nested within residents and units.
Additional analyses addressed the alternative explanation for the reduction in restrictive measures, namely a potential increase in awareness and subsequent higher numbers of restrictive measures registrations. These analyses specifically examined the reduction of restrictive measures that were recorded prior to the intervention period (n = 234). Analyzing the extent of reduction of restrictive measures recorded before the intervention period also revealed a significant decrease in restrictive measures (b = 1.77, t = 2.12, p = .048). The intervention explained 10.9% of the variance in the reduction of restrictive measures nested within residents and units.
Discussion
This clustered randomized trial demonstrated the effectiveness of the Multidisciplinary Expertise Team (MDET) program in reducing the number of restrictive measures implemented in sheltered homes for individuals with intellectual disabilities in the Netherlands. The challenge of reducing restrictive measures, which have often become ingrained in staff members’ routines, is acknowledged. May et al. (2016) and Bisschops et al. (2022) emphasized the complexities of implementing healthcare innovations, noting that standard operating procedures and staff beliefs often persist despite new practices. This study highlights the potential of a multicomponent approach to reduce restrictive measures, addressing needs of residents, staff, and the entire organization.
The multi-component approach aligns with the recommendations of several authors emphasizing interventions across multiple interlocking system levels to effect changes in care practices, particularly in cases where restrictive measures are routinely employed to manage risk behavior (Huckshorn, 2004; Iffland et al., 2024; Luiselli, 2009; Schreiner et al., 2014; Williams and Grosset, 2011). For instance, Røstad et al. (2023) emphasized creating awareness of triggers for challenging behavior, identifying preventive strategies, and documenting them in individual plans. The MDET program is presented as an example of such a comprehensive, multi-component intervention.
The results indicate that residential units assigned to the MDET program reported a significant reduction in restrictive measures (40%) compared to the care-as-usual condition (20%). The MDET program involved raising awareness of restrictive interventions, systematic registration of their use at the organizational level, and multidisciplinary consultations and interventions at the residential care team and resident levels. None of these program elements on its own were assumed sufficient to reduce restrictive interventions on a large scale (Deveau and McDonnell, 2009; Riding, 2016; Schreider et al., 2014; Williams and Grosset, 2011). The multidisciplinary expert team’s effectiveness should therefore be interpreted against the background of these organization-wide efforts. Care practices arise in interaction between resident and support staff members (Stelk, 2006), requiring an integrated effort to reduce restrictive interventions by altering organizational context, care staff practices, and resident behavior. The importance of making registration of key care practices part of routine care has been demonstrated in the past (Deveau and McDonell, 2011; Huckshorn, 2004; Riding, 2016; Schreiner et al., 2014; Williams and Grosset, 2011). The study thus suggests that these elements, when combined, go together with an effective program.
During the intervention period, the experimental group recorded more restrictive interventions than the control group. This raises the possibility that the observed intervention effect might be partially ascribed to increased awareness and registration of restrictive interventions used and registered prior to and during the intervention period. This aligns with the findings of a study explaining an increase in registration following the implementation of new laws and regulations in Norway (Søndenaa et al., 2015). To distinguish the effects of the program through awareness raising from those through altering care practices, the current study additionally assessed the experimental effect on restrictive interventions that were already registered before consultation by the multidisciplinary expert team began. The program’s effectiveness remained statistically significant for this subset of restrictive interventions.
Limitations should be kept in mind. First, the coordination of the multidisciplinary team was partly provided by the first author, which implies that program effectiveness evaluations were not independent from the program implementation. It is expected that once the program is well-implemented within a specific care organization over time, the MDET program can be self-managed by the expert team of the care organization, thereby enabling future research to replicate the results of the current study. Second, the absence of quantitative data on the duration and frequency of the application of restrictive measures may have underestimated intervention effects. It is indeed possible that reducing restrictive measures might imply a reduction in the frequency or total duration or replacing a more intrusive restrictive measure with a less intrusive one, which could not be fully captured by the dichotomous approach in this study. However, overestimation of the effects is also possible, if the restrictive measures that were reduced additionally in the intervention condition would have concerned relatively minor, inconsequential forms, leaving more serious measures in place. Third, the broad definition of restrictive measures, although in line with the Care and Coercion Act, may have led to different interpretations of the concept, which in turn, potentially could have affected the accuracy of the registration. To minimize these possible differences in interpretation and conceptualization, the expert team received legal and theoretical courses on the subject from the research team at the onset of the study.
The current study focused on the effects of the MDET method on reduction of involuntary care. Although reduction of involuntary care would likely lead to increased quality of life, such beneficial effects are not guaranteed. Further research is therefore needed to investigate how the changes made as a result of consultation with the MDET method also impact self-determination and quality of life. This is particularly important to test whether accelerated reduction with MDET targets the restrictive measures that matter most for residents. Research in this direction would need to include the perspective of residents themselves. While involuntary is a sensitive topic, work on a community of practice for the implementation of MDET showed how the dialogue with experts of experience with an intellectual disability in this community of practice could be high valued and productive (Bisschops et al., 2024).
Conclusions
Findings require replication across and within care organizations to validate the promising effects of the MDET program. Although the program was protocol-based and standardized, the program’s effectiveness may be influenced by the team experts’ qualities and the care organization’s specific context. The development and implementation of MDET might have been as much an expression of the intentions and collective efforts towards change that the care organization already had in place to address restrictive measures as it was a catalyst for further systemic changes.. The importance of testing these contextual factors for their impact on program effectiveness is highlighted, contributing valuable insights into the implementation of care innovations in the future. Furthermore, by building multidisciplinary expertise in a team that consults across multiple sheltered care home teams, dissemination of such expertise may be promoted, which may have an overall positive influence on quality of care and prevention of coercive practices.
Footnotes
Author contributions
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Stichting Wetenschappelijk Onderzoek ’s Heeren Loo.