
Abstract
Hospitalization due to non-transmissible chronic disease (NTCD) affects people and health institutions negatively. Healthcare systems need integral strategies to minimize this impact.
Objective
To determine the effect of an anticipated care plan, structured around hospital discharge (PC-AH-US), regarding the caregiving load of people with NTCD residing in Colombia, 2019–2021.
Method
This is a quasi-experimental study with pre- and post-intervention measurements. It includes 1170 participants who represented 585 chronic disease patient–caregiver pairs. We compared the PC-AH-US intervention, to the regular intervention.
Results
The PC-AH-US intervention group showed better results in all dimensions when compared to the regular intervention group: Awareness 8.7 (SD: 0.7) and 6.8 (SD: 1.7); Acknowledgement of their unique conditions 11.3 (SD: 1.0) and 9.4 (SD: 1.8); Capacity to fulfill care tasks 8.8 (SD: 0.7) and 7.5 (SD: 1.5); Wellbeing 11.4 (SD: 0.90) and 8.87 (SD: 2.3); Anticipation 5.88 (SD: 0.4) and 4.7 (SD: 1.1) and Support Network 11.4 (SD: 0.8) and 9.9 (SD: 2.5).
Conclusion
The PC-AH-US intervention group showed a statistically significant decrease in the caregiving load for people with NTCD (p < 00). There were no significant institutional differences in readmissions or deaths. The PC-AH-US intervention backs institutional policies meant to care for people with NTCD.
Keywords
Introduction
Non-transmissible chronic diseases (NTCDs) are among the main causes of death and morbidity worldwide, and they affect people, families and healthcare systems through a huge social impact. 1 According to the Pan-American Health Organization (2020), 2 these diseases have a specially alarming trend in countries with medium to low income.
Interventions to improve patient and family caregiver care skills are globally associated positively with a lighter caregiving load. 3 In some cases these interventions involve family caregivers directly. 4 Psychoeducational interventions for caregivers make it possible to increase their awareness regarding diseases, help improve their capacity for care, help them make the right choices and to look for the help they need. 5
Structured and anticipated interventions meant to guide the care of people with chronic diseases in their transition from the hospital to their homes, have minimized frequent symptoms, 6 reduced risk factors, 7 reduced times of stay in the hospital, 8 and controlled readmission processes. 9
Research shows that the caregiving load increases when chronic illnesses act up and people are hospitalized, and this creates a need for more interventions. 10 On the other hand, caregiving load is inversely correlated to awareness regarding these diseases. 11
There are no reports regarding anticipated and structured care plans that tackle the issue of chronic illness patient, family member and health institution caregiving load in an integral fashion. This project tried to assess the effect of an anticipated and structured health plan for hospital discharge (PC-AH-US) on the caregiving load of people with chronic diseases residing in Colombia, from this integral perspective.
Method
This is a quasi-experimental quantitative study, with measurements made before and after the intervention. The sample gathered 585 pairs of people with chronic diseases and their family caregivers, selected through a convenience criterion in three university hospitals for 18 months.
All participants were over 18 years of age. The patients were diagnosed with chronic diseases including diabetes mellitus, arterial hypertension, cardiac insufficiency, ischemic cardiac disease and chronic lung obstructive disease. All of them had 48 or more hours of hospitalization. Their family caregivers were required to be the primary caregivers.
Prior to the beginning of the quasi-experimental phase, researchers carried out a characterization that included: demographics; the perception of burden and support and appropriation of ICT. Then, we assigned the participants to the treatment group made up of 403 pairs in two institutions that received the PC-AH-US intervention, and to the control group, made up of 182 pairs in one institution, and who received the regular intervention. Finally, we compared the effect on their caregiving load before and after they received each intervention. Figure 1 illustrates the procedure.
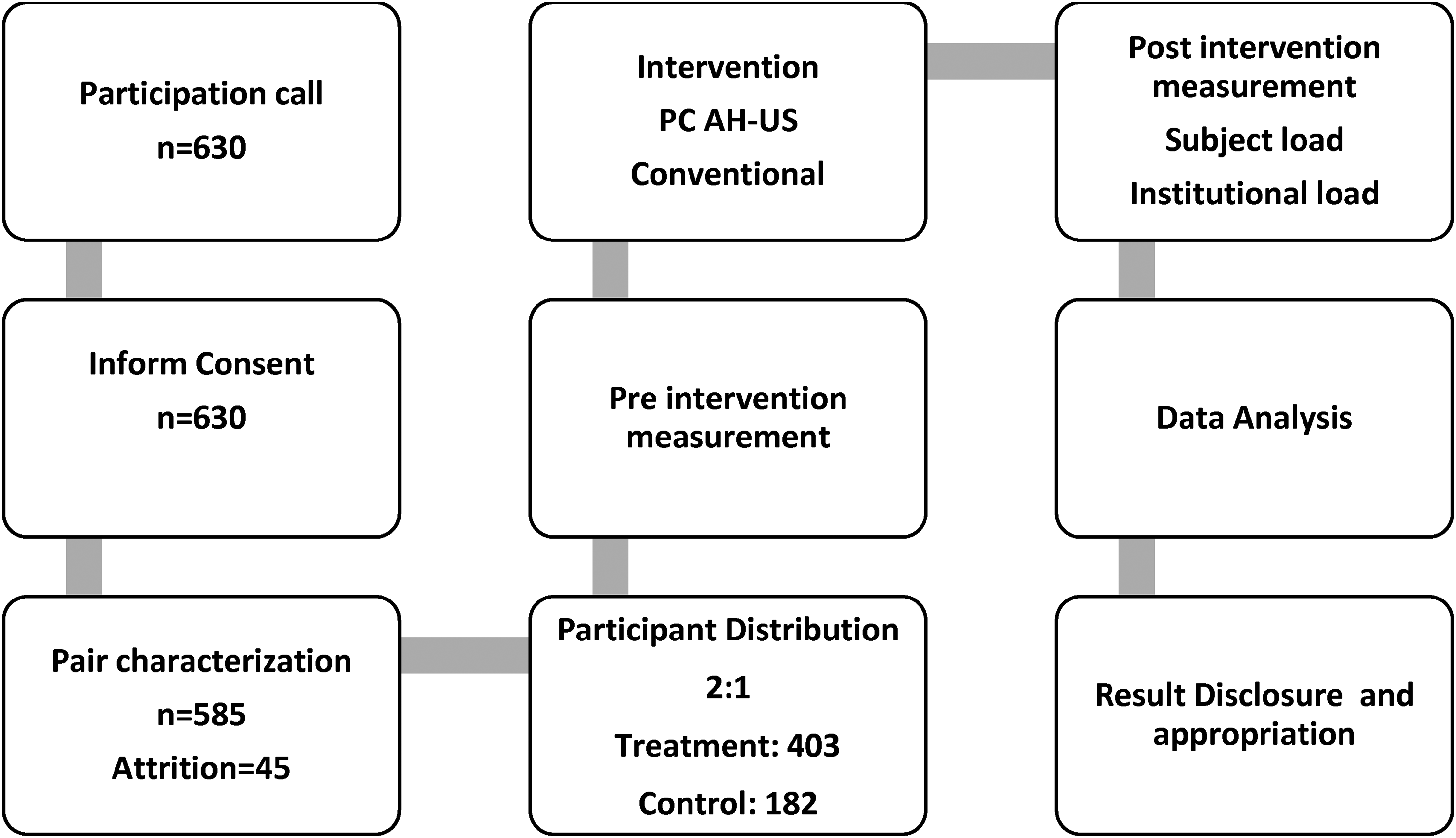
Study procedure. Source: Research data.
We used the survey for the characterization of care of patient–family caregiver pairs (ENCT in Spanish), validated in Spanish, to characterize pair members for care. 12 This survey included three components: first, it evaluated functionality and cognitive capacity levels; second, the perception of care-related burden and support and third, the use of information and communication technologies for care.
We valued the caregiving load of people in the process through the patient or patient–family caregiver CUIDAR instrument abbreviated versions. Carrillo et al. 13 designed this instrument to measure care competences in the hospital–home transition, and to evaluate the load through the level of awareness, recognition of uniqueness, instrumental capacity, the availability of basic well-being conditions, the abilities to make adequate decisions and to anticipate risks and emergencies and to use the network and social relationships of the pair adequately. The CUIDAR instrument has psychometric Cronbach tests of 0.97 14 and rates care competences as “low” between 0 and 36, “medium” 37 and 48 or “high” 49 and 60.
Institutional caregiving load included the cost valuation of preventable complications through the number of readmissions, the number of required hospital bed days and the number of deaths in each group during the 6 months after the intervention. We collected this information using an Ad Hoc questionnaire based on follow-up interviews of pairs, and a review of our electronic institutional records.
Our research group developed the PC-AH-US and coordinated it with other actors. We followed the systematic healthcare intervention standard put forward by Whittemore and Grey. 15 The PC-AH-US is an anticipated and structured intervention that educates and instructs patients and family caregivers preemptively, through an evaluation of their care needs when they enter the hospital. We provided educational material before the discharge, tailored to their base pathology. We followed the protocol previously established by Carrillo et al. 16 to define how to work with the pairs and to measure care competences. This protocol establishes that, if the patient is highly functional and cognitive, nurses should work alongside the patient and their caregiver and measure their care competences. If, on the other hand, functionality or cognition is compromised, nurses should work with the caregiver alongside the patient and measure the caregiver’s competences for care. In either case, the intervention includes both members of the pair.
The regular intervention responded to the institutional hospital discharge protocols; included administrative procedures and care and medication instructions; and directed to the patient and their family caregiver.
We guided the study using two hypotheses: the PC-AH-US is more effective that the regular intervention to decrease the caregiving load of a group of people with NTCD in Colombia, and the PC-AH-US is more effective to reduce the institutional caregiving load of a group of people with NTCD residing in Colombia.
We used descriptive statistics for the analysis. We used mean averages and dispersion for the quantitative variables, and frequency distributions and percentiles for categoric ones. We used the non-parametric Wilcoxon test to make within-group comparisons before and after the interventions, and the non-parametric Mann–Whitney U-test to compare between groups with a p value <0.05.
The ethics committees of participating entities approved the study after they evaluated its compliance with international ethical standards by using the Helsinki guidelines 17 (Code ENF-252018). Each participant signed an informed consent. The researchers made a commitment to have a complementary intervention for the treatment group if the results were proven effective to reduce the caregiving load.
Results
Our characterization findings are summarized in Table 1. When analyzing these results, we found that the caregivers are on average 19 years younger than the patients. We observed that there are 9.2% more male patients and 5.4% more female caregivers.
Socio-demographic data of chronic disease patient–family caregiver pairs.
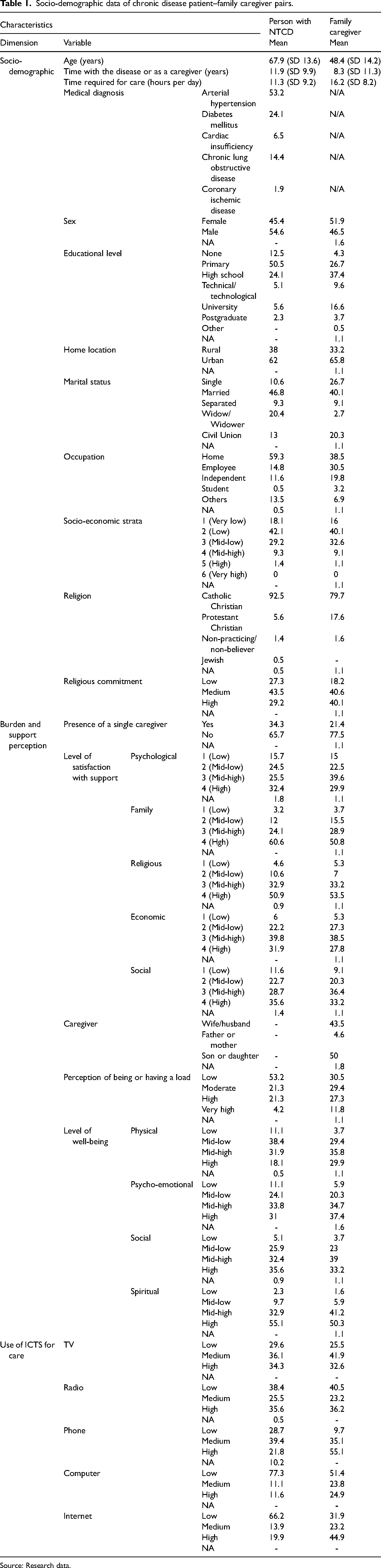
Source: Research data.
The educational level is higher in caregivers than in patients. Twenty-nine percent of caregivers have higher education while only 13% of patients do. The chronological and educational differences are reflected in the use of ICTs for caregiving, the most used being radio and television for patients, and cell phone and the Internet for caregivers.
Patients and their caregivers perceive the time spent on caregiving differently; caregivers perceive spending 4.9 more hours a day than patients do. Added to this, 52.6% of caregivers have work activities or educational commitments in addition to caregiving activities, while only 26.9% of patients have work activities or educational commitments. The difference in the perception of burden as high or very high among them is 13.6%, with a greater burden perceived by caregivers.
When reviewing their marital status, we found no differences between patients and family caregivers, it is evident in both groups that most of them have a partner and most (77.5%) caregivers perceive support from other people in their caregiving work.
Finally, caregivers positively evaluate the support received in social, physical, economic, and especially in spiritual aspects. Caregivers reflect greater religious commitment with a difference of 10.9% with respect to patients (see Table 1).
We found that the sample group initially had a mid-low competence for care level.
Total care competences in all dimensions increased in both groups after the interventions. Nonetheless, the treatment group presented a significantly higher increase, and changed from low to high, while the group with the regular intervention remained at a medium level (see Table 2).
Pre- and post-intervention comparison between the PC-AH-US and the regular intervention groups regarding their competence for care.
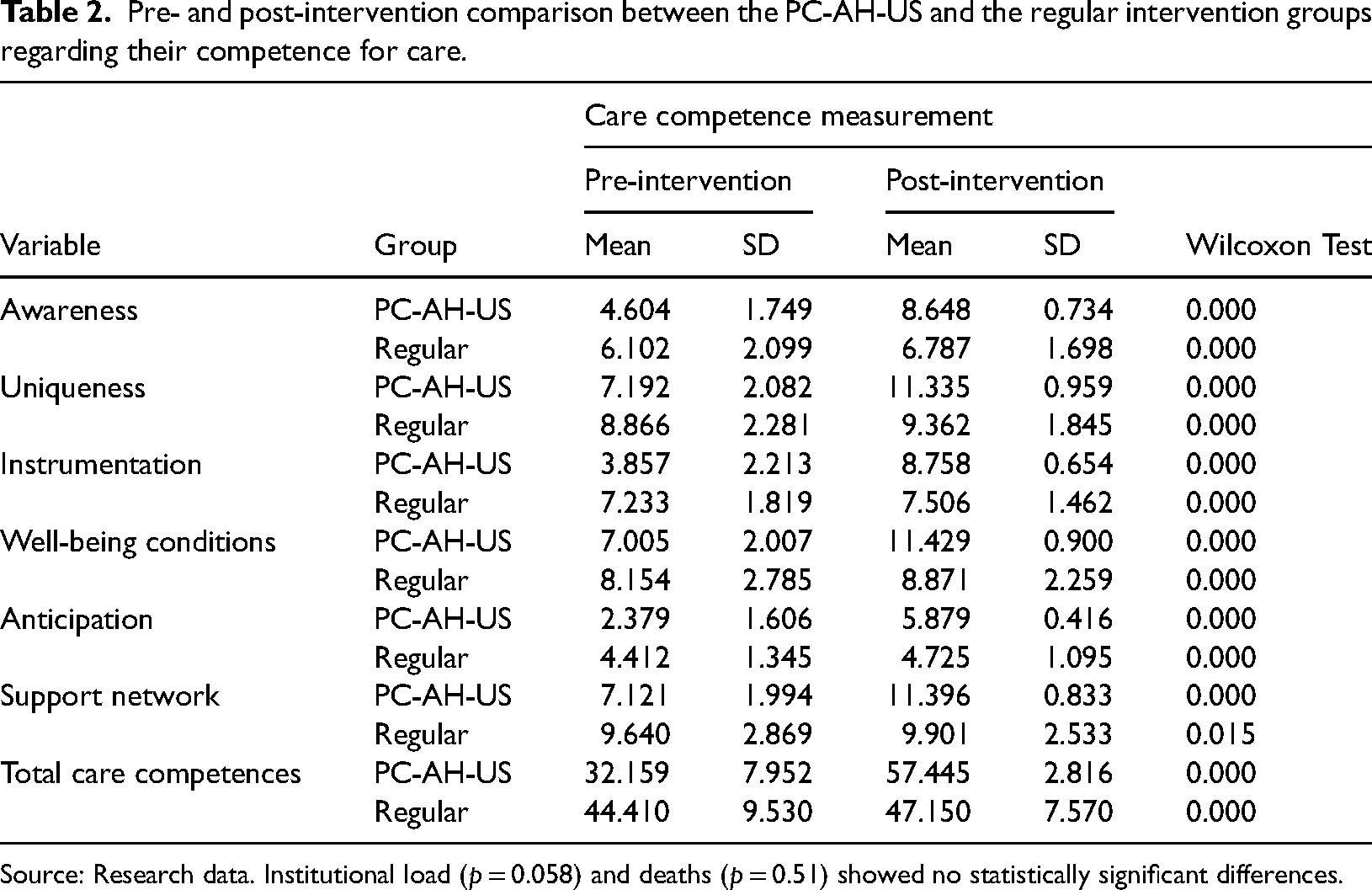
Source: Research data. Institutional load (p = 0.058) and deaths (p = 0.51) showed no statistically significant differences.
The global test of the caregiving load level between baseline and the PC-AH-US intervention group was statistically significant (p < 0.001). The intervention had a significant impact among patients and caregivers who reported lower levels of awareness, uniqueness, instrumentation, wellbeing conditions, anticipation, and support network at their baseline, while no significant effect was found among patients with respect to institutional load (p = 0.058) and deaths (p = 0.51) (Table 2).
Patients with lower baseline care competences levels were particularly likely to benefit (Table 2). We found that the sample group initially had a mid-low competence for care level. Total care competences increased in both groups after the interventions, in each dimension that make them up. Nonetheless, the group with the PC-AH_US intervention presented a significantly higher increase, and changed from low to high, while the group with the regular intervention remained at a medium level (see Table 2).
The PC-AH-US intervention had a significant impact among patients and caregivers who reported lower levels of awareness, uniqueness, instrumentation, wellbeing conditions, anticipation and a weaker support network. The global test of care competences between baseline and the PC-AH-US intervention group showed statistically significant differences (p < 0.001). We did not find any significant effect among patients regarding institutional load (p = 0.058) and deaths (p = 0.51). Moreover, patients with lower baseline care competence levels were particularly likely to benefit from the PC-AH-US intervention (Table 2).
The inter-group comparison of post-intervention caregiving competence with the Mann–Whitney U-test for independent samples showed statistically significant differences (Table 3).
Comparison of change in score (pre- and post-intervention) between PC-AH-US and regular for various factors.
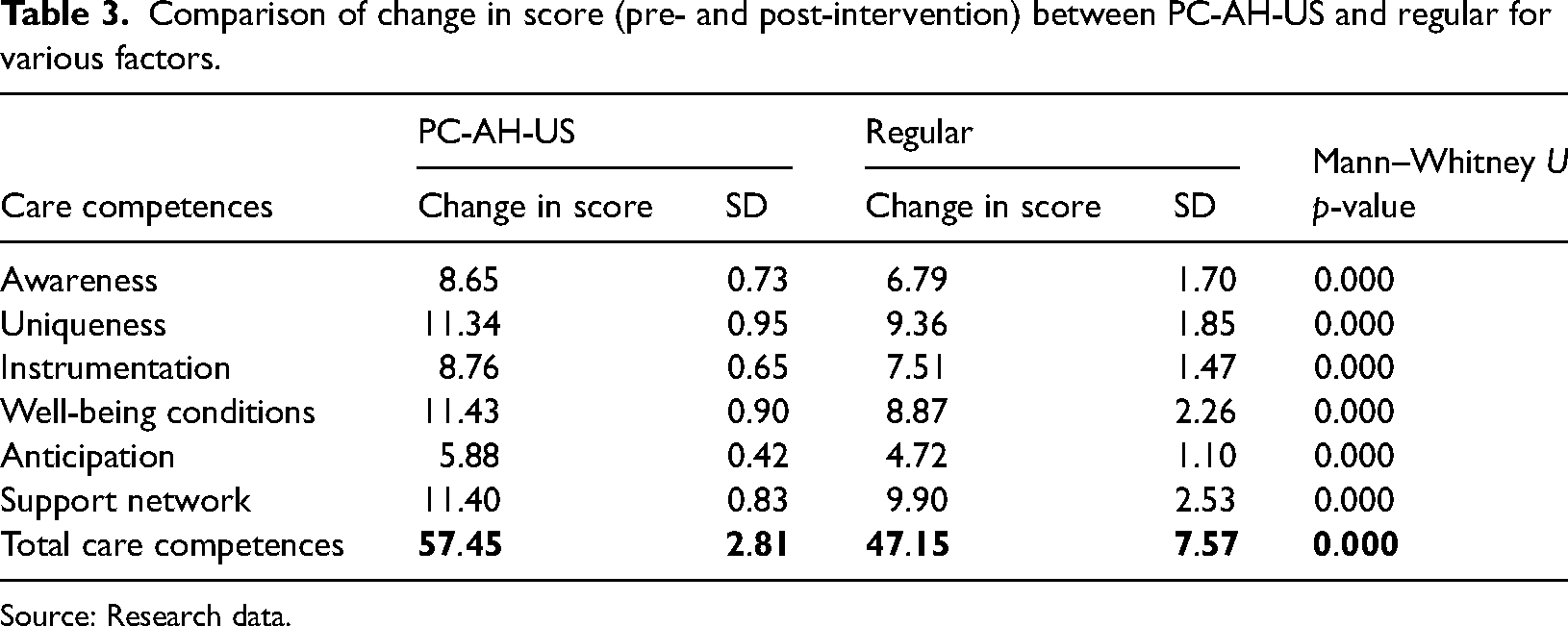
Source: Research data.
Discussion
This study determined the characteristics of people with chronic illnesses and their family caregivers. People with chronic disease show a similar distribution of illness causes to that of the regional epidemiologic profile. 2
Conway 18 documented a higher load of care for women and proved that female caregivers have no awareness of the proper way to care for people who require hospitalization or rehospitalization.
This study showed that caregivers dedicate most of their day to care, but they keep their usual roles, and they have done so for a prolonged amount of time. These caregivers belong to the “sandwich generation,” and while they are a fundamental component in the health system that guarantees healthcare, it is important to remember that caregiving load is associated with their quality of life. 19
A higher recognition of the characteristics of people involved in the care of chronic disease will lead to more focalized interventions. 20
Our findings complement Kweon et al.’s 21 findings, which state that the type of technology that is being offered is important, for instance, emerging markets may find radio and telephone more suiting to their needs, rather than computers.
Members of these pairs have a specially high value for family support, having a permanent partner and identifying other caregivers that may be able to help them. Despite this, a fourth of them perceive a high or very high burden of care. This finding partially contradicts the propositions put forward by Yigitalp et al. 22 who point out that an adequate social support reduces the caregiving load.
Pair members show that spiritual well-being is perceived at the highest level, and physical well-being is at the lowest. These findings confirm those of Roger et al. 23 who point out that spirituality and religion are part of the support that people with chronic disease require.
Although evidence regarding the impact of self-handling of chronic diseases is weak, 24 this study supports this evidence and points out that the group who received the specialized intervention showed a higher level of awareness than the group who received the regular intervention. The PC-AH-US intervention in this study, like the one by Faronbi et al. 25 aims to preserve the well-being of people with chronic diseases and their family caregivers. In this case, the PC-AH-US intervention complements awareness with a focus on specific characteristics, instrumental ability, minimum well-being conditions, ability to anticipate, adequate choice-making, risk handling and available social networks. It is important to remember that the load of patients includes a decrease in their quality of life, pocket expenses, adherence to medication, inability to work, symptom control and elevated costs for caregivers. 26
This study did not present an important decrease in the institutional load. It is important to keep looking for ways to decrease this load, as this is a priority for countries with low and medium incomes Gheorghe et al. 27
In conclusion, hospitalization due to NTCD, and transit from the hospital to the patient's home, can negatively affect the people involved in these processes and the institutions that tend to them. We require integral strategies to minimize this impact. The PC-AH-US intervention was designed to support healthcare during the hospital-home transition of patients with NTCDs and their family caregivers. The PC-AH-US showed significant decreases on the caregiving load of people with NTCDs, as we pointed out in the first hypothesis. In this sense, the pairs that received the PC-AH-US showed significantly better results in their awareness, the recognition of their unique conditions, their capacity to instrument care tasks, their enjoyment of their own well-being, anticipation and risk management, and the strengthening of their support network with regards to those who received the regular intervention. Although PC-AH-US participants had less re-admissions and less deaths than those who receive the regular intervention, there were no statistically significant differences. The present study is limited by its sample allocation. We recommended that subsequent studies use a random sampling method.
The PC-AH-US is a nursing interdisciplinary and intersectoral coordinated answer to the global call to decrease the caring load for people with chronic illnesses, for individuals related to the process and for institutions.
Footnotes
Contributorship
Carvajal-Carrascal G., Fuentes-Ramírez A., Pulido-Barragán S., Guevara-Lozano M. and Sánchez-Herrera B. researched literature and conceived the study. Carvajal-Carrascal G., Fuentes-Ramírez A., Pulido-Barragán S., Guevara-Lozano M. and Sánchez-Herrera B. were involved in protocol development, gaining ethical approval, patient recruitment and data analysis. Carvajal-Carrascal G., Fuentes-Ramírez A., Pulido-Barragán S., Guevara-Lozano M., and Sánchez-Herrera B. wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received financial support from Universidad de La Sabana and E.S.E. Hospital de la Samaritana for the open access publication of this article.