
Abstract
Objectives
This study examined the health discussion networks (HDNs) of people with inflammatory bowel disease (IBD). We sought to test if HDN characteristics were associated with IBD management self-efficacy outcomes.
Methods
We recruited a sample of adults with IBD (N = 112) in December 2020 to take an online survey. Participants listed up to five people (alters) who they discussed their health with, and we used those data to construct individual HDNs. Participants provided demographic information about alters, and characterized alter by relationship, closeness, and support provided. We used multivariable regression to examine associations of HDN characteristics with IBD symptoms, remission, and emotions management self-efficacy outcomes.
Results
Participants reported data for 412 alters (mean HDN size: 3.68). Alters were mostly friends (40%) or family members (36%); few were healthcare workers (6%). In multivariable analyses, HDN size was associated with remission and emotions management self-efficacy (ps < .05), and the amount of support offered by alters was associated with emotions management self-efficacy (p < .05).
Discussion
HDN size and alter support variables were associated with some IBD management self-efficacy outcomes among our study sample. These findings provide empirical evidence about HDNs among people with IBD and support the notion that disease management is a collective effort.
Keywords
Introduction
Inflammatory bowel disease (IBD) is the umbrella category of chronic gastrointestinal (GI) diseases—including Crohn's disease and ulcerative colitis—that affects nearly seven million adults worldwide. 1 Common IBD symptoms include chronic diarrhea, bloody stool, and fatigue. IBD symptoms are dynamic and complex, making it difficult to monitor disease activity and keep symptoms in remission. 2 Having a strong social support system to turn to when in need could help people manage and cope with some of the emotional and physical side effects associated with IBD.
Managing a chronic illness is rarely an individual effort.3,4 Close network ties, such as friends and family members often contribute critical disease management resources and advice.5,6 This is particularly true in the context of IBD, as research has shown that social support can improve wellbeing among those with IBD.7–9 For example, one study found a negative correlation between social support satisfaction and distress among participants with IBD who had high baseline levels of perceived stress. 7 Additional research has similarly shown associations between social support and other IBD management outcomes, including disease activity and mental health. 10 Finally, there is a substantial literature showing that people with IBD use online social networking sites to seek or provide one another with IBD-related information.8,9,11–14
The interpersonal qualities and structural characteristics of personal networks may also play a key role in self-managing a chronic condition. Here, we define personal networks as a group of individuals connected to a single person through some means or relationship (friendships, work colleagues, peers). 15 Personal networks are also commonly referred to as ego-networks. A recent study by Sentell et al. 16 examined personal networks of people hospitalized with preventable conditions for heart disease and diabetes. Most patients in this study noted receiving illness management help from family members in their networks, which is consistent with other research investigating the role of family in disease management. 17 Similarly, Vassilev and colleagues 18 examined personal networks of 300 people with chronic disease and found that spouses contributed a substantial amount of “work” (e.g., scheduling appointments, providing emotional comfort) toward disease management activities. Moreover, their study found that individuals who did not have a spouse in their personal networks tended to distribute illness-related “work” to other network ties, suggesting that disease management support may be substitutable across individuals in networks.
To date, few investigations have explicitly examined personal networks among people with IBD. There is some evidence that having a healthy relationship with a GI provider can benefit treatment adherence among this population, 19 but it is unclear whether people with IBD typically want or view healthcare providers as key individuals in their personal networks. In addition, one study examined the size of personal networks among people with IBD, but this work did not evaluate effects of network size on health outcomes. 7
One important question that has yet to be investigated is whether personal networks are associated with people's perceived ability to manage their IBD—which is commonly referred to as IBD management self-efficacy. 20 For example, research has shown that perceptions of support can improve some of the emotional and physical effects associated with IBD, 21 and that social support is a key component in IBD self-management. 22 Is there also a network effect present such that having a large or supportive personal network improves disease management self-efficacy among people with IBD, and if so, to what extent?
The current study aimed to examine the characteristics of personal networks among a sample of people with IBD and to test whether certain network properties (e.g., size, types of network relationships) were associated with IBD management self-efficacy outcomes. Ultimately, the goal of this work was to generate empirical evidence on the role that personal networks play in facilitating support among a sample of people with IBD.
Methods
Participants and procedure
Participants were recruited via Reddit and Twitter to take an online survey. Recruitment took place from December 2020 to January 2021 on a rolling basis. Data from this cross-sectional study are from a pretest survey that was part of a separate eHealth and IBD self-management intervention. 23 Screening criteria were that participants had to 1) have IBD (self-reported diagnosis), 2) be from the U.S., 3) have a smartphone, and 4) report at least some IBD-related distress. Criteria 3 and 4 were required for intervention purposes and information about how IBD-related distress was measured is discussed below. For a more detailed overview of participant recruitment and eligibility, see Rohde et al. 23 Overall, recruitment efforts yielded N = 114 prospective participants.
After meeting eligibility and providing informed consent, participants answered questions about their demographics and IBD characteristics, as well as various items about their IBD self-management self-efficacy. Finally, participants answered questions about their personal health discussion networks (HDNs). We collected HDN information using an egocentric (i.e., personal) network approach adapted from previous research.15,24 Participants were asked to list up to five individuals who they discuss their health with or whom they can count for help when they have physical or emotional problems. This type of question is referred to as a name generator. Per convention, we refer to the individuals listed in the name generator as “alters” and the participants filling out the survey as “egos.” The alters collected from this process were used to construct unique networks at the individual level (i.e., one ego-network per participant). Only those who provided HDN information are included in this study, resulting in a sample size of N = 112 participants.
We administered the online study using Qualtrics, a popular survey technology platform. All procedures and methods used in this study were approved by the UNC-Chapel Hill IRB.
HDN variables
Participants were asked to provide demographic information about each of their HDN alters, including their age, gender, and relationship to the ego. Relationship categories were spouse/partner, family member, friend, healthcare worker, or other. For relationship type, participants could select more than one category. Participants were then asked to rate how close they were to each alter, with responses being on 11-point scales ranging from “not close” (1) to “close” (11). Finally, participants were asked to identify whether each alter: 1) listens to them; 2) tells them they care for them; and 3) makes practical suggestions. We interpret these items as indicators of general social support (i.e., not limited to IBD-related experiences) provided by alters. Responses to each of the alter support items were binary, meaning an ego identified an alter as either providing that type of support or not. Participants were allowed to select multiple support items for each alter. They could also choose to select none of the support options per alter. All HDN questions and measurement scales were adapted from previous research.15,24
For analytic purposes, we chose to compute a single, continuous proportion measure of total available support that an alter provided as opposed to having three separate binary variables. We calculated this proportion by taking the number of support opportunities offered by alters (max value of 3 for each alter) divided by the total number of possible support opportunities in each ego's network (network size*3).
For the alter relationship variable, we computed a single continuous measure of relationship heterogeneity using the Blau index of diversity.
25
The formula for this measure is:
IBD management self-efficacy outcomes
The outcome of this study was self-efficacy, which we measured using the inflammatory bowel disease self-efficacy scale (IBD-SES). 20 The IBD-SES has been evaluated in several prior studies, including large clinical trials.26–28 We assessed shortened, adapted versions of the following three subscales from the IBD-SES: 1) symptoms management, 2) remission management, and 3) emotions management. The symptoms subscale is comprised of three items about managing the physical effects of IBD, such as fatigue. The remission subscale is comprised of five items about staying on top of general IBD management and self-care. Finally, the emotions subscale is comprised of three items about managing the emotional effects of IBD, such as stress. Subscales began with the stem, “In the past two weeks, how confident were you in your ability to…” Example items for each subscale were, “reduce IBD symptoms,” “manage your IBD,” and “do something to reduce sadness from IBD,” respectively. Responses to all self-efficacy items were on 11-point scales ranging from “not at all confident” (1) to “totally confident” (11). Reliability of the subscales ranged from α = .78–.85. For each subscale, higher scores correspond to improvements in self-efficacy outcomes.
Demographics, IBD characteristics, and other covariate measures
Participants self-reported their age, gender, race, Hispanic ethnicity, education, household income, and sexual orientation. For IBD characteristics, participants self-reported what type of IBD participants had (ulcerative colitis, Crohn's disease, indeterminate colitis, or other), what age they were diagnosed with IBD, and if they were currently taking daily oral medication to treat their IBD or to maintain IBD symptoms. We also assessed IBD activity using the single-item Manitoba IBD Index (MIBDI). 29 For the MIBDI, participants were asked to self-report how active their IBD symptoms were in the past 6 months, and response options were on a 6-point scale ranging from “I was well in the past 6 months, what I consider a remission or absence of symptoms” (1) to “constantly active, giving me symptoms every day” (6). Finally, we assessed general IBD-related distress using a six-item scale adapted from the short-form version of the diabetes distress scale.30,31 The items in the distress scale cover topics related to the physical, emotional, and social effects of IBD. The scale begins with the stem, “During the past 2 weeks, how much have you…” Example items were: “felt overwhelmed with the demands of living with IBD” and “felt that your friends or family don’t appreciate how difficult living with IBD can be.” Responses to distress items were on a five-point scale ranging from “not at all” (1) to “a great deal” (5). Reliability of the scale was α = .72.
Data analysis
We used descriptive statistics to characterize participant demographics and IBD characteristics, as well as their health discussion networks, such as network size, alter relationship heterogeneity, closeness, and the proportion of alter support provided. We computed separate multivariable linear regression models to assess correlates of the three self-efficacy subscales. Each model included the same following HDN variables as predictors: network size, alter relationship heterogeneity, mean alter closeness, the proportion of total available support offered by alters, and whether an HDN had a spouse/partner or healthcare worker alter (0 = alter not in network [reference] vs 1 = alter in network). We included whether a spouse/partner or healthcare worker alter was in an HDN in the model because research suggests these alter types may serve different roles in personal networks for people with chronic illness (e.g., spouses offering emotional support vs healthcare providers offering informational support). 18 Multivariable models controlled for the following covariates: age, IBD type (0 = ulcerative colitis [reference] vs 1 = Crohn's disease), whether a participant was diagnosed with IBD in the past five years (0 = no [reference] vs 1 = yes), IBD activity, and IBD-related distress. Analyses were computed using base R functions (version 4.1.2).
Results
Participant characteristics
Mean age of participants was 29 (range: 19–53; Table 1), most were white (83%), and approximately 9% identified as Hispanic. Over half (61%) of participants were female and more than one-third (39%) identified as gay, lesbian, or bisexual. A little less than half (46%) of participants had a bachelor's degree or higher. Household income varied, with 47% of participants making less than $50,000, 34% making between $50,000 and $99,999, and 17% making $100,000 or more. Most participants had Crohn's disease (73%) or ulcerative colitis (19%); though, a small proportion (8%) self-reported other IBD diagnoses, such as lymphocytic colitis. Mean age at diagnosis was 22 years and about half (51%) of participants had been living with IBD for five years or fewer. Most participants (63%) were currently taking daily oral medication to treat their IBD. IBD activity (mean[M] = 4.65, standard deviation [SD] = 1.28) and IBD-related distress (M = 3.35, SD = .68) varied.
Demographic and IBD characteristics of the study sample; N = 112.
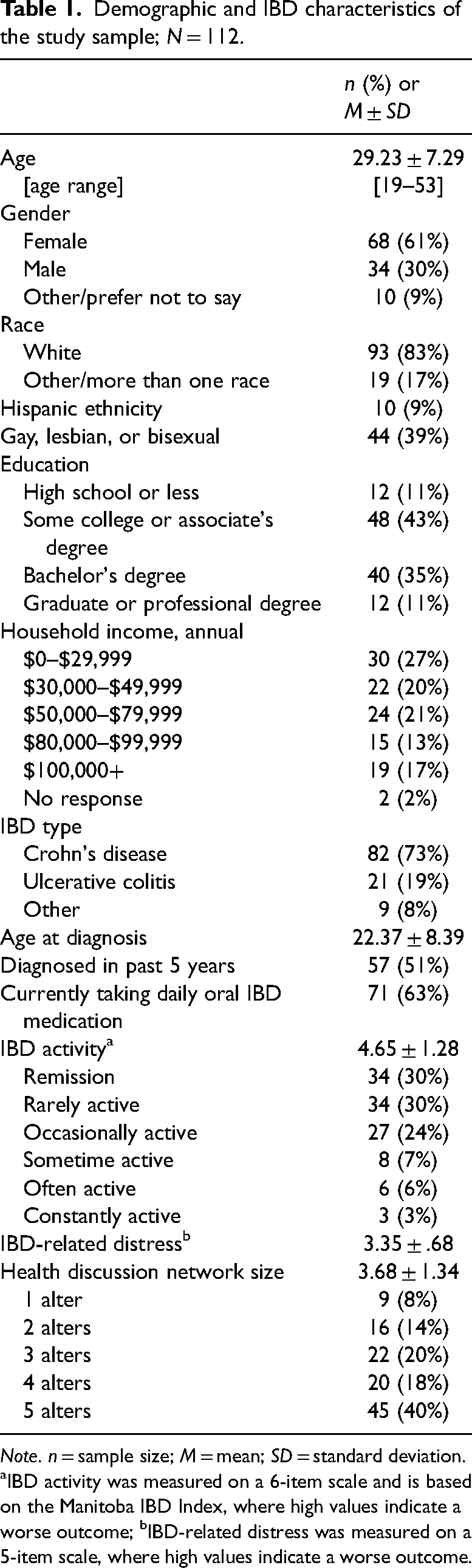
Note. n = sample size; M = mean; SD = standard deviation. aIBD activity was measured on a 6-item scale and is based on the Manitoba IBD Index, where high values indicate a worse outcome; bIBD-related distress was measured on a 5-item scale, where high values indicate a worse outcome.
HDN characteristics
Participants had the option to list up to five alters in their HDNs. On average, participants listed between three and four alters (M = 3.68, SD = 1.34), and nine participants (8%) listed only one alter in their HDNs (Table 1). Participants reported data for a total of 412 alters (Table 2). A majority of alters were friends (40%), family members (36%), or spouses/partners (17%) of the egos. Few were healthcare workers (6%) or other/multi type alters (2%). Alter relationship heterogeneity was modest (M = .44, SD = .23; range: .00–.72). Most egos indicated that alters offered support by listening to them (93%), caring for them (75%), and by making practical suggestions (71%); though, the degree of alter support varied based on the ego-alter relationship. For example, nearly all spouse/partner alters (99%) provided support to egos by caring for them, whereas a smaller proportion of friend (77%), family member (73%), and healthcare worker (13%) alters provided egos this same type of support. Lastly, closeness was high for spouse/partner (M = 10.14, SD = 1.70), family member (M = 9.16, SD = 1.92), and friend alters (M = 9.04, SD = 1.90), but only modest for healthcare worker alters (M = 5.22, SD = 2.15). See Figure 1 for a visual of an aggregate ego-alter network.
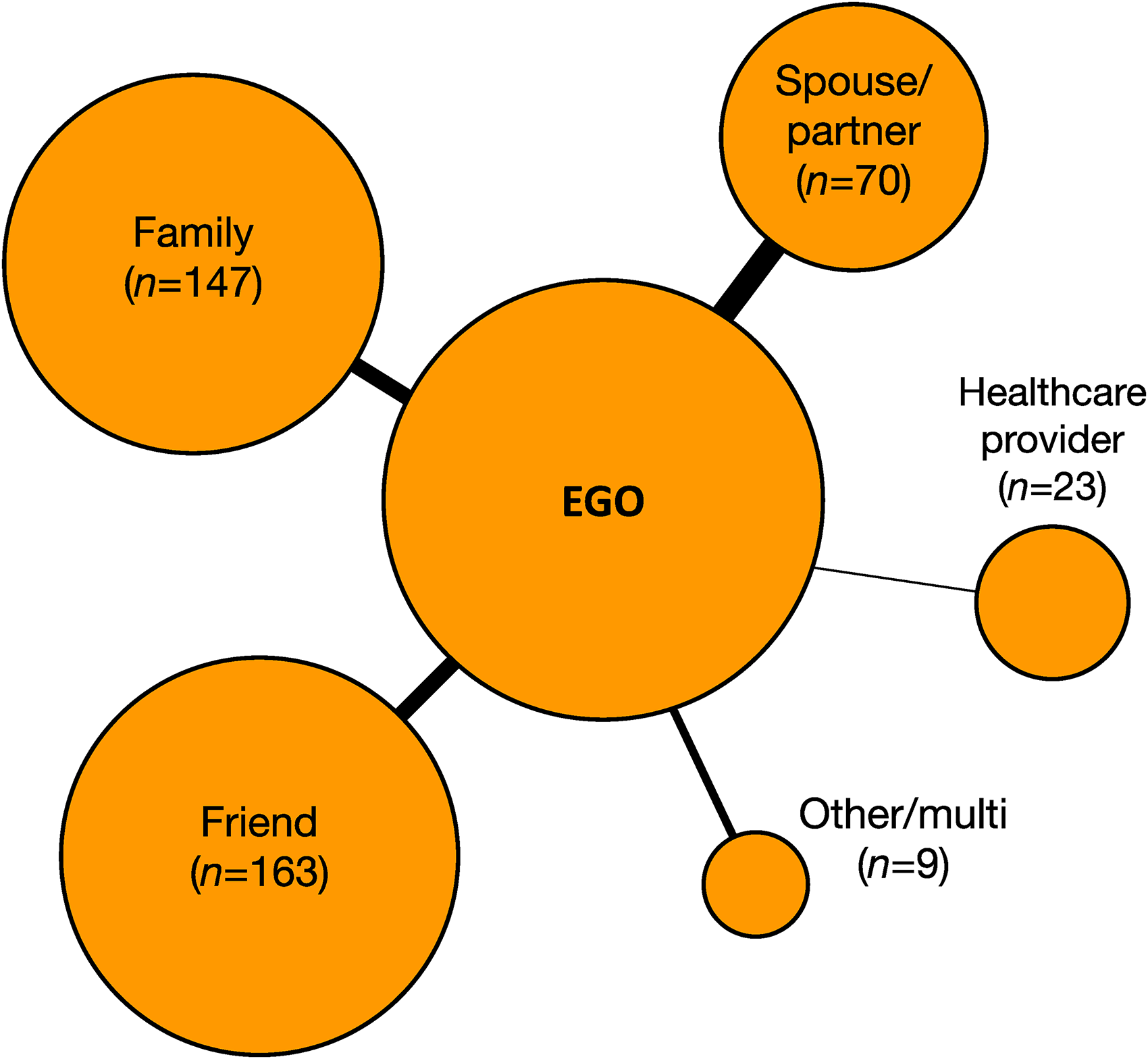
Ego-network graph of all ego-alter pairs; node sizes are weighted based on alter proportion with ego; edge widths are weighted based on mean ego-alter closeness.
Alter characteristics; N = 412.
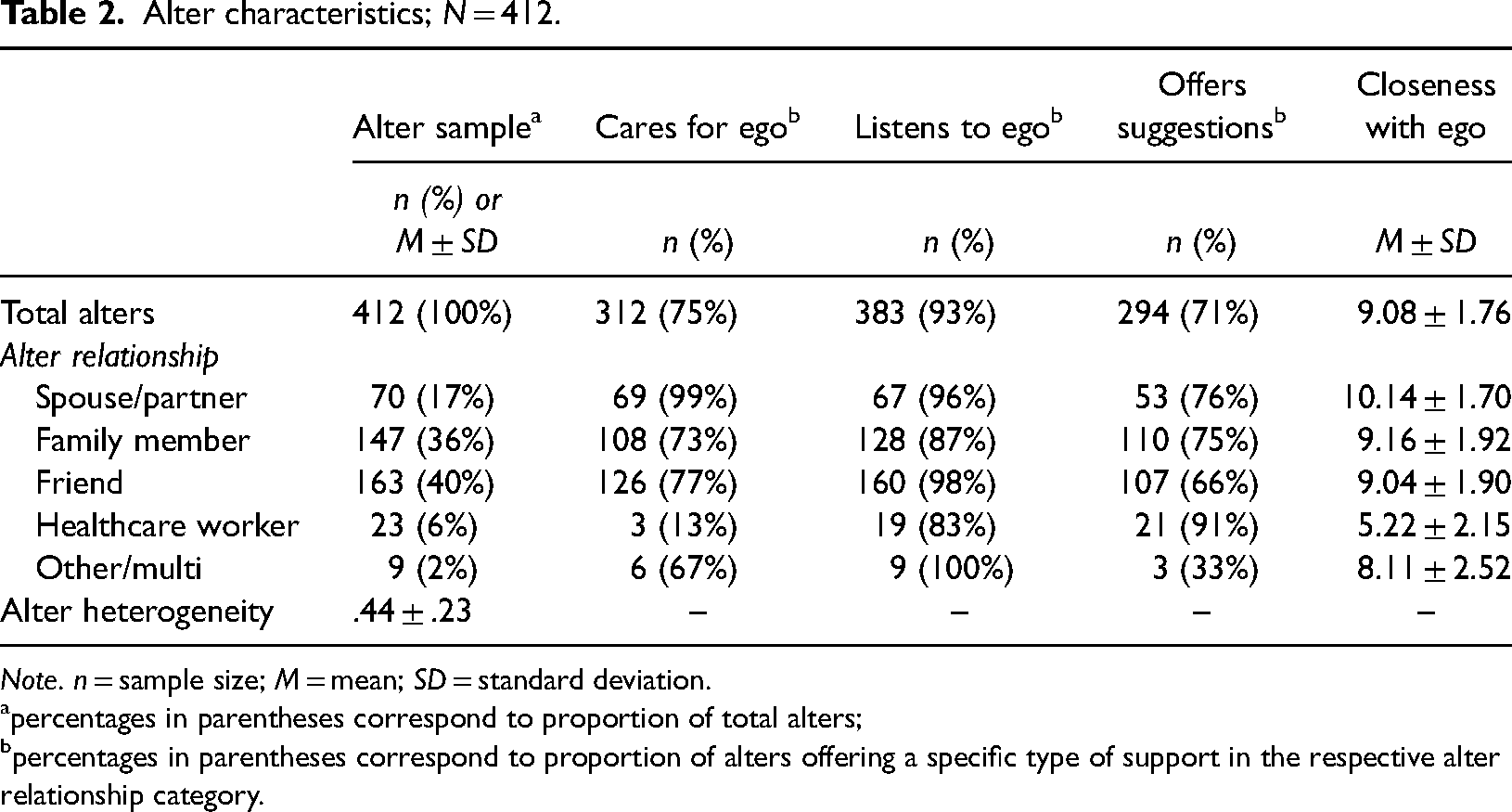
Note. n = sample size; M = mean; SD = standard deviation.
percentages in parentheses correspond to proportion of total alters;
percentages in parentheses correspond to proportion of alters offering a specific type of support in the respective alter relationship category.
HDN and covariate correlates of self-efficacy
Network size (b = .37, p = .022) was positively associated with remission management self-efficacy (Table 3). Both network size (b = .50, p = .002) and proportion of available support (b = 2.68, p = .017) variables were positively associated with emotions management self-efficacy. No HDN variables were associated with symptoms management self-efficacy. Some participant-level covariates were also associated with the self-efficacy outcomes. For example, IBD-related distress was negatively associated with symptoms (b = −1.07, p < .001), remission (b = −1.12, p < .001), and emotions (b = −1.02, p < .001) management self-efficacy. In addition, IBD activity was negatively associated with symptoms (b = −.29, p = .043) and remission management self-efficacy (b = −.28, p = .045). Finally, whether a participant was diagnosed with IBD in the past five years was positively associated with emotions management self-efficacy (b = .73, p = .045). In total, the models accounted for 22%, 25%, and 22% of the variability in symptoms, remission, and emotions management self-efficacy outcomes, respectively.
Correlates of self-efficacy subscales; N = 103.
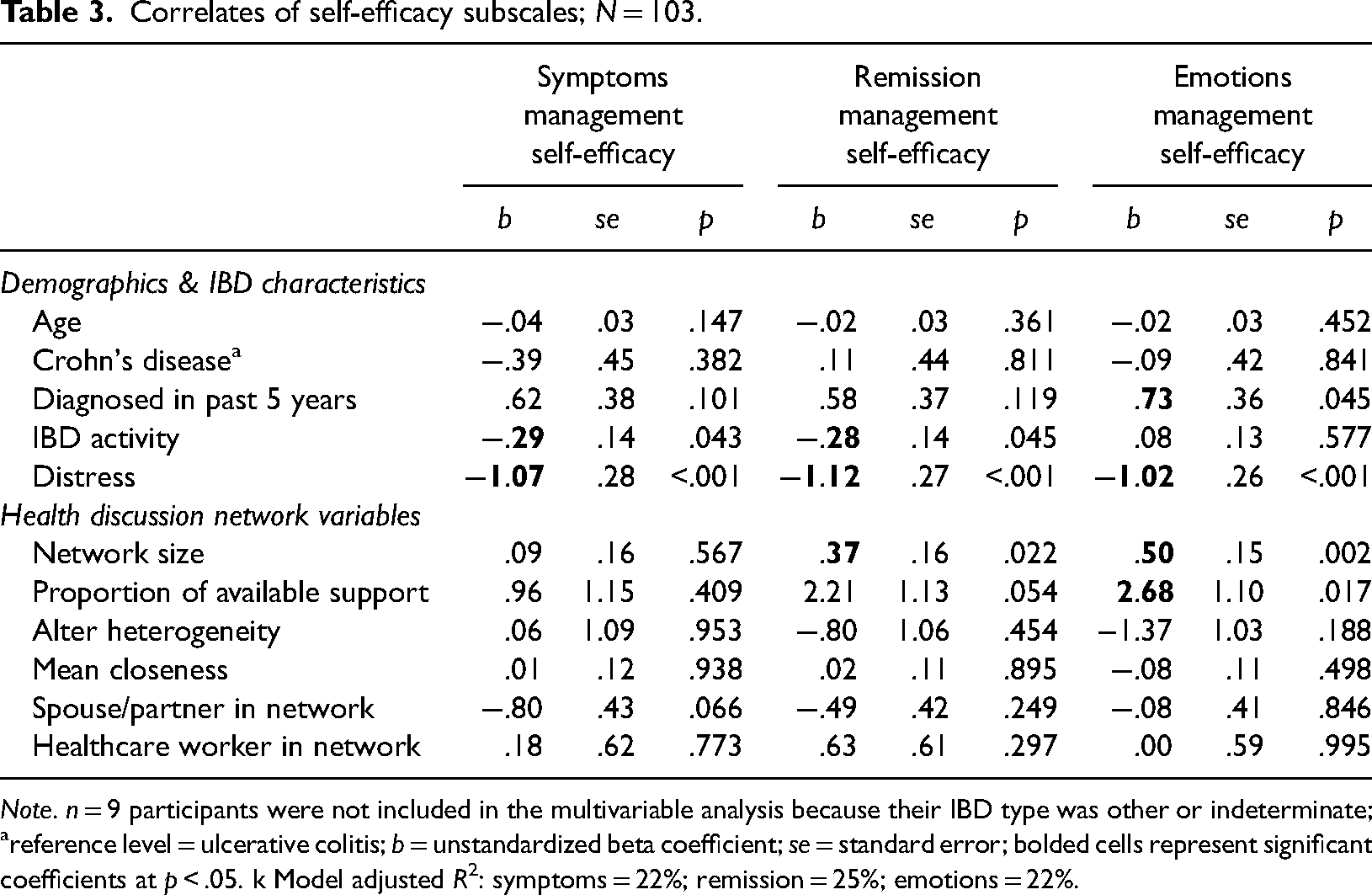
Note. n = 9 participants were not included in the multivariable analysis because their IBD type was other or indeterminate;
reference level = ulcerative colitis; b = unstandardized beta coefficient; se = standard error; bolded cells represent significant coefficients at p < .05. k Model adjusted R2: symptoms = 22%; remission = 25%; emotions = 22%.
Discussion
This study assessed the characteristics of HDNs among a sample of people with IBD, and tested whether HDN properties were associated with IBD management self-efficacy outcomes. Findings showed participants tended to construct highly supportive personal HDNs. Moreover, HDN size and the proportion of available support from alters were key determinants in some self-efficacy outcomes. These findings contribute much-needed empirical evidence about the utility of HDNs for people with IBD and suggest that HDNs may play an important role in the IBD self-management process.
Although some past work has examined personal network effects among people with IBD, 7 there was a dearth of research characterizing HDN composition. The current study found that friends, family members, and spouses/partners made up a large proportion of HDN alters among participants. Indeed, only three individuals (3%) did not include any one of those alter types in their HDNs. Moreover, alter support and closeness among these three alter types were high overall, speaking to their perceived importance in HDNs among our sample.
By contrast, few participants reported having a healthcare worker in their HDN. This finding is surprising given the high degree of involvement typically associated with managing IBD, such as regular medical appointments.22,32 One reason for this could be that we only allowed participants to provide information for up to five alters and that healthcare workers may still play a peripheral yet key role in HDNs among this sample. Regardless, GI clinicians should continually strive to improve on patient-provider communication skills and relationships to benefit IBD self-management outcomes. 22
Another important finding was the association between certain HDN characteristics and self-efficacy outcomes. Network size was associated with remission and emotions management self-efficacy. Moreover, the proportion of available support among alters was correlated with emotions management self-efficacy. These results suggest that having a sizeable and supportive network may help people overcome some of the implications (affective and other) that coincide with managing IBD. For example, individuals who have a readily available support system of some friends or family members to call on may be best equipped to manage the emotional effects of undergoing an unexpected disease flare. This notion supports the perspective that managing chronic illness is a collective effort.3,4 It should be emphasized, however, that our results come from a convenience sample of people with IBD who reported some levels of baseline distress. In addition, our recruitment period took place during the COVID-19 pandemic, which may have modified how participants utilized their networks. Thus, repeated studies from cohorts representing different sample characteristics across different time periods need to be conducted before generalizing our findings to broader IBD patient populations.
Surprisingly, we found no association between alter relationship heterogeneity and self-efficacy outcomes, suggesting that diversity in the types of alters that participants had in their HDN may not be important given they provide ample support. This finding partially corroborates the notion of substitutability in chronic illness networks discussed above. For example, Vassilev and colleagues found that alters distributed illness-related work in networks where egos did not have spouses. 18 In this study, we found that so long as support was offered by alters, the composition of HDNs did not matter. We also found that alter closeness was not associated with the self-efficacy outcomes, but this finding could be due to ceiling effects exhibited among this measure (M = 9.08 out of 11). In the same vein, although spouse, family members, and friends are different types of alters, the high degree of closeness among these alter types suggest they may functionally offer similar support. Thus, our alter relationship heterogeneity variable may lack tie strength variation, which could explain its null effect on self-efficacy outcomes. Future work should build on these findings by evaluating the role of HDN alter support and closeness in other research contexts, such as by testing their impact on additional health outcomes or in network intervention contexts.
Finally, we found that no HDN variable was associated with symptoms management self-efficacy among participants. These null effects could be explained by the fact that IBD symptoms are often unpredictable and difficult to manage. 2 In fact, the only covariates associated with symptoms management were IBD activity and distress, which is unsurprising given that those measures are derived from and related to IBD symptom experiences. It is possible that managing IBD symptoms are personal and time-dependent, and that alters in an HDN may not be able to contribute symptom-related support the same way they are able to offer emotional support.
Strengths of this study include the large sample size and characteristics of HDN alters reported by participants. A limitation was that participants were recruited as part of a separate study and were required to have some level of IBD-related distress. We also used a convenience sampling method to identify and recruit participants from Reddit and Twitter, which may introduce some sampling bias as not all people with IBD use or have access to these social media platforms. In addition, some of the study sample demographics and IBD characteristics were homogenous (e.g., 83% white). These limitations preclude us from generalizing our findings to broader IBD populations. Another limitation was that our modest sample size (N = 112) prevented us from computing subgroup analyses to examine HDN variability across participants. One last notable limitation is that we did not gather data on alter-alter relations. In the context of available support, we were only able to investigate what support was offered by alters, whereas examining the density of egos’ networks via alter-alter relations could explain the strength of support available. Future research should consider whether the connectedness of that available support impacts outcomes.
Conclusion
Personal HDNs may be important to IBD self-management. Findings from this study indicate that friends, family members, and partners/spouses provided substantial support through listening, caring, and offering suggestions to study participants diagnosed with IBD. Moreover, the support provided by alters in participants’ HDNs and their HDN size were associated with improvements to IBD self-efficacy outcomes. These findings support the notion that social support plays a key role in managing a chronic disease and that disease self-management is a collective effort.3,4
Footnotes
Contributorship
JAR and AJS designed the research study. JAR conducted literature searches, provided summaries of previous research studies, conducted all analyses, and wrote the first draft of the manuscript. AJS and XZ reviewed the manuscript. All authors contributed to and approved the final manuscript.
Availability of data and material
The data underlying this article will be shared on reasonable request to the corresponding author.
Code availability
The code used to compute the analyses for this article will be shared on reasonable request to the corresponding author.
Contributorship
JAR and AJS designed the research study. JAR conducted literature searches, provided summaries of previous research studies, conducted all analyses, and wrote the first draft of the manuscript. AJS and XZ reviewed the manuscript. All authors contributed to and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
All study procedures were approved by a university Institutional Review Board (approval number 20-2201).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article
Guarantor*
JAR
Informed consent
All participants provided informed consent in this study.