
Abstract
Background/Aims
Individuals with neurofibromatosis, including neurofibromatosis 1 (NF1), neurofibromatosis 2 (NF2)–related schwannomatosis (SWN), and other forms of SWN, often experience disease manifestations and mental health difficulties for which psychosocial interventions may help. An anonymous online survey of adults with neurofibromatosis assessed their physical, social, and emotional well-being and preferences about psychosocial interventions to inform clinical trial design.
Methods
Neurofibromatosis clinical researchers and patient representatives from the Response Evaluation in Neurofibromatosis and Schwannomatosis International Collaboration developed the survey. Eligibility criteria included age ≥ 18 years, self-reported diagnosis of NF1, NF2, or SWN, and ability to read and understand English. The online survey was distributed internationally by the Neurofibromatosis Registry and other neurofibromatosis foundations from June to August 2020.
Results
Surveys were completed by 630 adults (18–81 years of age; M = 45.5) with NF1 (78%), NF2 (14%), and SWN (8%) who were mostly White, not Hispanic/Latino, female, and from the United States. The majority (91%) reported that their neurofibromatosis symptoms had at least some impact on daily life. In the total sample, 51% endorsed a mental health diagnosis, and 27% without a diagnosis believed they had an undiagnosed mental health condition. Participants indicated that neurofibromatosis affected their emotional (44%), physical (38%), and social (35%) functioning to a high degree. Few reported ever having participated in a drug (6%) or psychosocial (7%) clinical trial, yet 68% reported they “probably” or “definitely” would want to participate in a psychosocial trial if it targeted a relevant concern. Top treatment targets were anxiety, healthier lifestyle, and daily stress. Top barriers to participating in psychosocial trials were distance to clinic, costs, and time commitment. Respondents preferred interventions delivered by clinicians via individual sessions or a combination of group and individual sessions, with limited in-person and mostly remote participation. There were no significant group differences by neurofibromatosis type in willingness to participate in psychosocial trials (p = 0.27). Regarding interest in intervention targets, adults with SWN were more likely to prefer psychosocial trials for pain support compared to those with NF1 (p < 0.001) and NF2 (p < 0.001).
Conclusion
This study conducted the largest survey assessing physical symptoms, mental health needs, and preferences for psychosocial trials in adults with neurofibromatosis. Results indicate a high prevalence of disease manifestations, psychosocial difficulties, and untreated mental health problems in adults with neurofibromatosis and a high degree of willingness to participate in psychosocial clinical trials. Patient preferences should be considered when designing and implementing psychosocial interventions to develop the most feasible and meaningful studies.
Keywords
Introduction
The neurofibromatoses (NFs), consisting of neurofibromatosis type 1 (NF1), neurofibromatosis type 2 (NF2)-related schwannomatosis (SWN), and other forms of SWN, are complex genetic disorders that affect multiple body systems and predispose individuals to developing nerve sheath tumors.†1,2 The tumors characteristic of these conditions may cause significant morbidity, such as disfigurement, pain, and functional difficulties including problems with gait, hearing, and swallowing depending on tumor type and location.3–5 Due to these manifestations, individuals with NF can experience significantly reduced quality of life (QOL) across the life span.6–8 Although descriptive studies and clinical trials have focused predominately on characterizing and treating physical manifestations, increasing attention is being directed toward understanding and addressing the psychosocial difficulties experienced by individuals with NF, including reduced QOL, anxiety, depression, and other mental health issues in children6,9 and adults.10,11
Specifically in adults with NF, poor QOL8,12 and higher incidences of depression and anxiety were documented compared to the general population using validated questionnaires10,13–18 and described in qualitative focus groups.19,20 A high occurrence of suicidal ideation also was identified in an NF sample prior to starting a psychosocial intervention. 21 In addition, physical manifestations, such as NF-related pain, are common11,16,22,23 and substantially interfere with daily life.16,22,24 Depressive symptoms mediated the relationship between pain intensity and pain interference in NF 24 and negatively impacted QOL, 14 suggesting that treating depression may decrease the effects of pain on daily functioning 24 and help improve QOL. 14
Additional domains of QOL that particularly are affected in adults with NF1 include cognitive functioning, appearance, and fatigue. 15 NF1-related learning problems and perceived physical appearance are predictors of mental health difficulties10,16 while higher disease severity and visibility are associated with poorer QOL,15,18 worse psychosocial well-being, and an increased need for psychological support. 15 Despite these clear psychosocial needs,10,14,15 adults with NF1 have reported a lack of routine evaluation of their mental health and difficulties finding appropriate psychological services. 20
In adults with NF2, the most severely affected disease-specific domains include hearing loss, dizziness, and balance problems 25 while psychosocial effects, future uncertainty, and pain are most predictive of overall QOL. 26 Furthermore, adults with larger vestibular schwannomas, 27 facial weakness, hearing loss, and imbalance have reported poorer QOL. 26
Limited research has investigated psychosocial and QOL issues in individuals with other forms of SWN, underscoring the need for high-quality studies in this area.8,12 Merker et al. 11 found that the QOL of adults with SWN was particularly affected in the domains of physical role and bodily pain, and pain is often the initial and most reported symptom of SWN.11,28 Furthermore, higher pain intensity has been associated with greater total-body tumor volume 10 and the SWN-related germline mutation.29,30
Given that NF can significantly impact mental health and QOL, a critical need exists for psychosocial interventions to address these difficulties. However, few psychosocial interventions have been implemented in the NF population. Vranceanu et al. 31 developed a mind–body program to improve QOL in NF using qualitative research. An in-person pilot study of this program improved resiliency, increased life satisfaction, and was highly acceptable; however, feasibility was low due to travel burden. A subsequent single-blind, virtual randomized controlled trial (RCT) of the group mind–body program showed excellent feasibility and acceptability, and improvements in QOL, anxiety, and resiliency over an attention control group 32 for up to 1 year. 33 This intervention was also tailored for adults with NF2 who are deaf and showed comparable results. 34 Recently, a fully powered efficacy single-blind, virtual RCT evaluating this same mind–body program group improved QOL 35 and coping 36 more than in an attention placebo control group, with results sustained over 12 months. Martin et al. 37 implemented interventions using Acceptance and Commitment Therapy (ACT) for NF1 chronic pain. A pilot study using a 2-day in-person small-group workshop, including some young adults with NF1 and their parents, was acceptable, feasible, and resulted in declines in pain but not functional outcomes or mood. A subsequent RCT with adults with NF1 using a hybrid model with both in-person and online sessions resulted in decreased pain interference. 38 Despite the benefits of these psychosocial interventions, improvements varied by domain, sample sizes were small except for the recent fully powered RCT,35,36 and not all were devised with patient input.
When developing interventions for individuals with NF, patient engagement is strongly recommended. 39 Involving patients in research design improves feasibility, increases enrollment rates, and ensures the study is more clinically relevant and meaningful. 40 Some studies have used focus groups and interviews of patients with NF to gather perceptions about their symptoms and concerns to guide the development of NF-specific psychosocial31,41,42 and cognitive 43 interventions and assessment measures.19,44 Additional engagement of adults with all types of NF regarding their psychosocial difficulties and preferences for the design of behavioral interventions is needed to develop the most appropriate patient-centered trials.
Previously, we gathered data from an anonymous online survey of adults with NF1, NF2, and SWN and determined that participants endorsed moderate to high amounts of stress and worry related to COVID-19, particularly the impact of the pandemic on their emotional and physical health. 45 The primary aims of the current study were to examine additional results from this survey to (1) describe the clinical characteristics, psychosocial difficulties, and impact of NF on daily functioning; (2) identify any differences across NF diagnoses and sex regarding these difficulties; and (3) summarize patient preferences for psychosocial interventions, including treatment targets, designs, outcomes, and barriers, to plan future clinical trials more effectively.
Methods
Participants
Adults aged 18 years and older with a self-reported diagnosis of NF1, NF2, or SWN who could read and understand English were eligible to participate in this study.
Measures
Clinical researchers and patient representatives from the NF community who are members of the multidisciplinary Response Evaluation in Neurofibromatosis and Schwannomatosis (REiNS) International Collaboration developed an anonymous survey in English. The REDcap (Research Electronic Data Capture) online survey aimed to assess perspectives about the design and conduct of patient-centered psychosocial trials. This survey assessed demographic information, NF clinical characteristics, psychosocial well-being, and preferences for psychosocial clinical trials. The National Institutes of Health (NIH) Institutional Review Board (IRB) deemed the protocol for the anonymous adult survey exempt. Data from the following four main sections of the survey were included in the current study.
Demographic characteristics
Survey items asked about the respondents’ age, biological sex, gender identity, race, ethnicity, country of residence (US or other), highest level of education, and employment status.
NF clinical characteristics and impact on everyday life
The survey collected data on self-reported NF-related clinical characteristics, including type of NF, disease complications, and how much each endorsed complication of NF1, NF2, or SWN interfered with everyday life from “not at all” to “a lot.” Another item asked how much all their NF symptoms affected their everyday life (four options from “no effect” to “severe degree”). Of note, the revised nomenclature for NF2 and SWN occurred after participants completed the survey; thus, we retained the previous types of NF used in the survey for this report.
NF impact on physical functioning, psychosocial well-being, and mental health
Several questions asked how much NF affected participants’ physical, emotional, and social well-being, and functioning at work/school and home (five options from “not at all” to “a lot”). Additional items asked whether respondents had either a diagnosed or a suspected undiagnosed mental health problem, and whether they had seen a mental health professional or taken medication for a mental health problem recently. Another question asked the extent to which mental health difficulties affected everyday functioning (four options from “not at all” to “a lot”). Finally, items asked whether participants had experienced learning, social, or mood difficulties during childhood, and if they received services for those difficulties.
Psychosocial clinical trial preferences
Items asked whether respondents had ever participated in a drug or psychosocial trial and about a range of preferences related to psychosocial trial participation. These questions asked about the best ways to learn about NF trials, factors related to participation, types of psychosocial trials that respondents would participate in, and willingness to participate in a psychosocial trial.
For a copy of the Adult NF Psychosocial Survey, see the supplemental section or REiNS website at https://ccrod.cancer.gov/confluence/display/REINS/Patient+Reported+Outcomes.
Procedures
The Children’s Tumor Foundation distributed the REDcap survey internationally through their online registry to 4745 adults with NF1, NF2, or SWN 46 on June 19, 2020 with two follow-up emails in July and August 2020. The survey also was disseminated via email and social media by NF foundations in the United States (NF Network, NF Northeast, NF Midwest, NF Michigan, Littlest Tumor Foundation, and Texas NF Foundation). The survey was closed on August 10, 2020. No compensation was provided for survey completion.
Data analysis
All statistical analyses were conducted using SPSS version 27 by IBM SPSS Statistics. When surveys had missing values, we used pairwise deletion to analyze the available data. We used descriptive statistics to identify characteristics of the survey sample and portray participants’ mental health characteristics, preferences, and barriers to psychosocial trial participation. Chi-square tests of independence were used to analyze group differences in psychosocial trial preferences across NF type, severity, and participant sex. Post hoc analyses with Bonferroni corrections identified between-group differences in responses for all significant omnibus chi-square tests.
Results
Demographic characteristics
Of the 4745 adults sent emails, 886 individuals consented to take the survey, and 630 completed it, yielding an overall response rate of 13.3% and a completion rate of 71.1%. Participants’ mean age was 45.54 years (SD = 4.18) with with 71.1% reporting their sex at birth as female. The majority (85.6%) of participants identified as White and not Hispanic or Latino (90.2%). Most participants were from the United States (77.8%). Other countries with > 1% of participants included Canada (5.6%), the United Kingdom (5.8%), and Australia (2.3%). The distribution of diagnoses was NF1 (77.8%), NF2 (14.3%), and SWN (7.6%) (Table 1).
Demographic characteristics of the total sample.
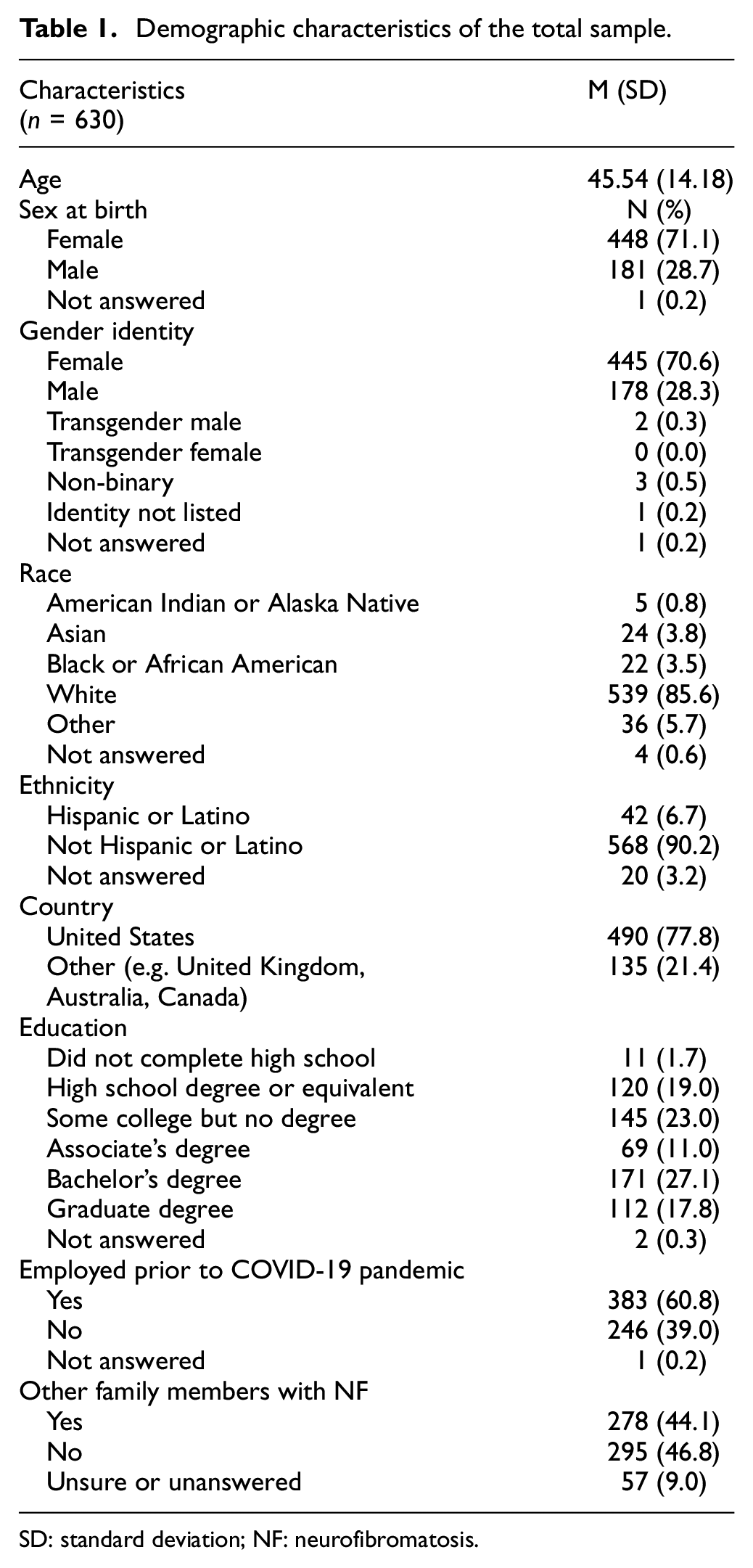
SD: standard deviation; NF: neurofibromatosis.
NF clinical characteristics and impact on everyday life
More than 90% of participants reported that their NF disease manifestations had at least some effect on everyday life, with 17.1% indicating a severe effect. For each of the three NF types, a majority (> 50%) endorsed having tumors (e.g. cutaneous/plexiform neurofibromas, vestibular schwannomas/acoustic neuromas, intracranial/spinal tumors), physical problems (e.g. pain, hearing difficulties, orthopedic problems), and psychosocial difficulties (e.g. learning difficulties, mental health concerns, sleep problems) that affected their everyday life from “somewhat” to “a lot” (Table 2).
Clinical characteristics of the total sample by NF type.
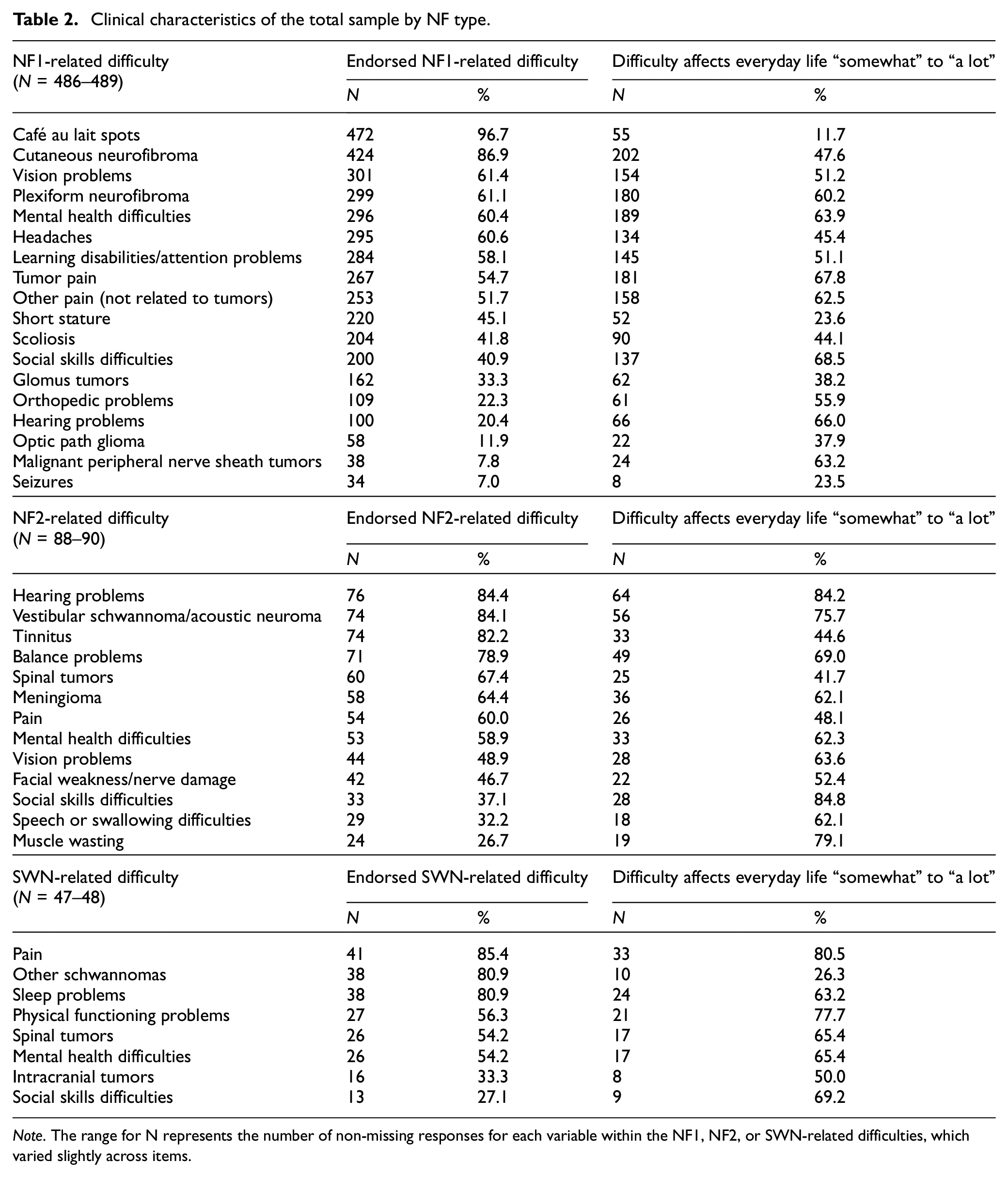
Note. The range for N represents the number of non-missing responses for each variable within the NF1, NF2, or SWN-related difficulties, which varied slightly across items.
NF impact on physical functioning, psychosocial well-being, and mental health
Impact of NF on physical functioning and psychosocial well-being
For questions about how much NF affects well-being, 43.1% of respondents indicated that NF affects their emotional well-being, 38.3% indicated that NF affects their physical functioning, and 35.1% indicated that NF affects their social well-being from “pretty much” to “a lot” (Figure 1). While only 17.4% of participants indicated that NF influences their functioning at home “pretty much” to “a lot,” 25.8% of participants reported that NF affects their school or work functioning to this high degree.
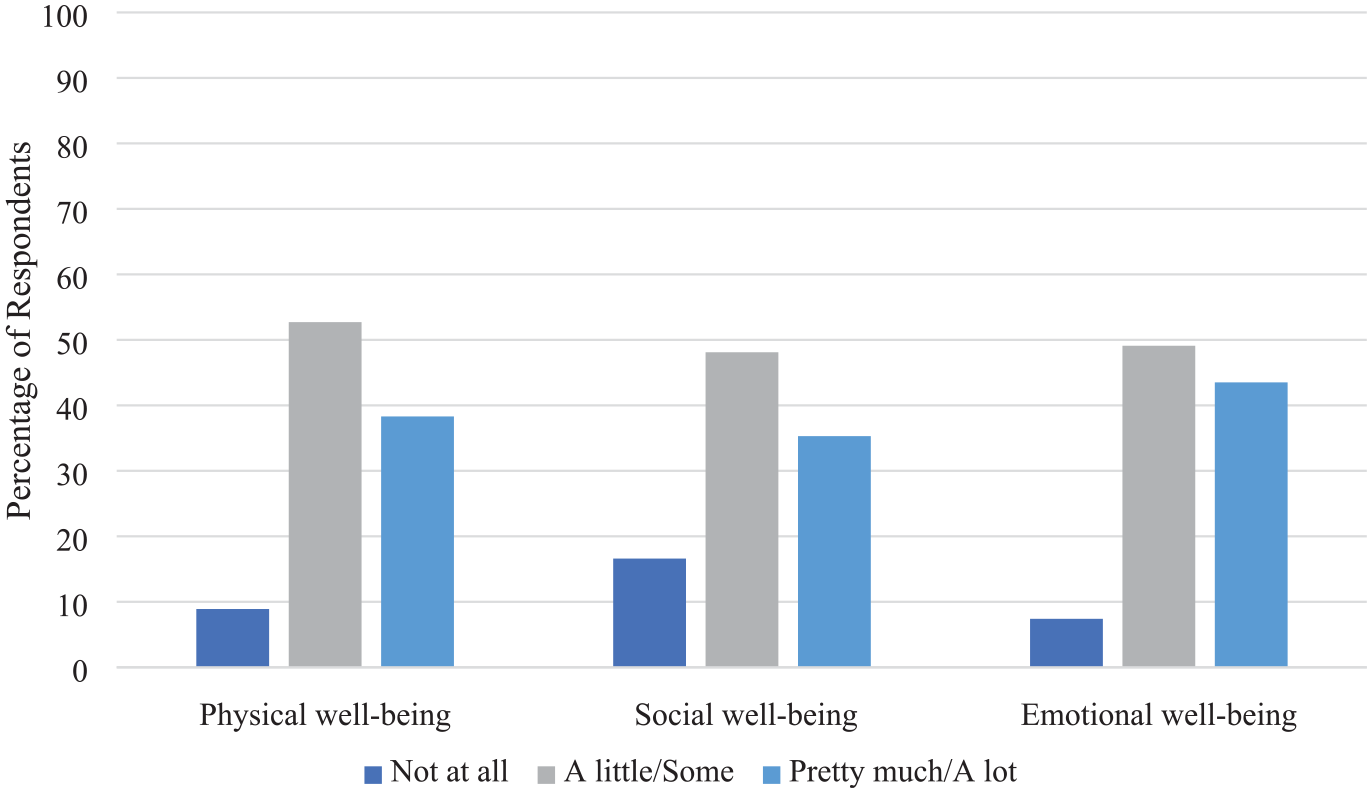
Impact of NF on the physical, social, and emotional well-being of the total sample.
Mental health problems in NF
Regarding mental health diagnoses, 51.3% of participants endorsed having been diagnosed with anxiety, depression, or another mental health problem. Of all respondents diagnosed, 71.7% reported having taken medication for a mental health problem recently, and 56.7% have seen a mental health professional recently. Of note, 26.5% of undiagnosed individuals still believed they had anxiety, depression, or another mental health problem. Of the respondents who endorsed having any mental health difficulties, 63.7% reported that these difficulties affected their everyday life from “somewhat” to “a lot.”
Psychosocial difficulties during childhood
Almost half (47.3%) of participants endorsed having mood difficulties during childhood, but only 21.2% of these individuals reported receiving intervention or support services during that time. Similarly, 62.9% of participants endorsed having social interaction difficulties while growing up, but of those with difficulties, only 9.9% received intervention or assistance. Finally, 53.8% of participants endorsed having learning difficulties as a child, with less than half of those (47.9%) reported receiving intervention or other assistance for these problems.
Group comparisons for psychosocial well-being and mental health
Across NF types (NF1, NF2, or SWN), there were no significant group differences in the prevalence of current reported mental health diagnoses or suspected mental health difficulties (χ2(4625) = 2.18, p = 0.70 and χ2(4299) = 4.74, p = 0.32, respectively). Results demonstrate significant differences across NF types regarding reported rates of learning, social, and mood difficulties during childhood (χ2(4628) = 98.5, p < 0.001; χ2(4623) = 51.51, p < 0.001; and χ2(4626) = 22.1, p < 0.001, respectively). Specifically, participants with NF1 reported significantly higher rates of learning and social difficulties compared to those with NF2 and SWN (all ps < 0.01). In addition, participants with NF1 were more likely to report experiencing mood difficulties during childhood compared to those with NF2 (p < 0.001) but not compared to those with SWN (Figure 2).
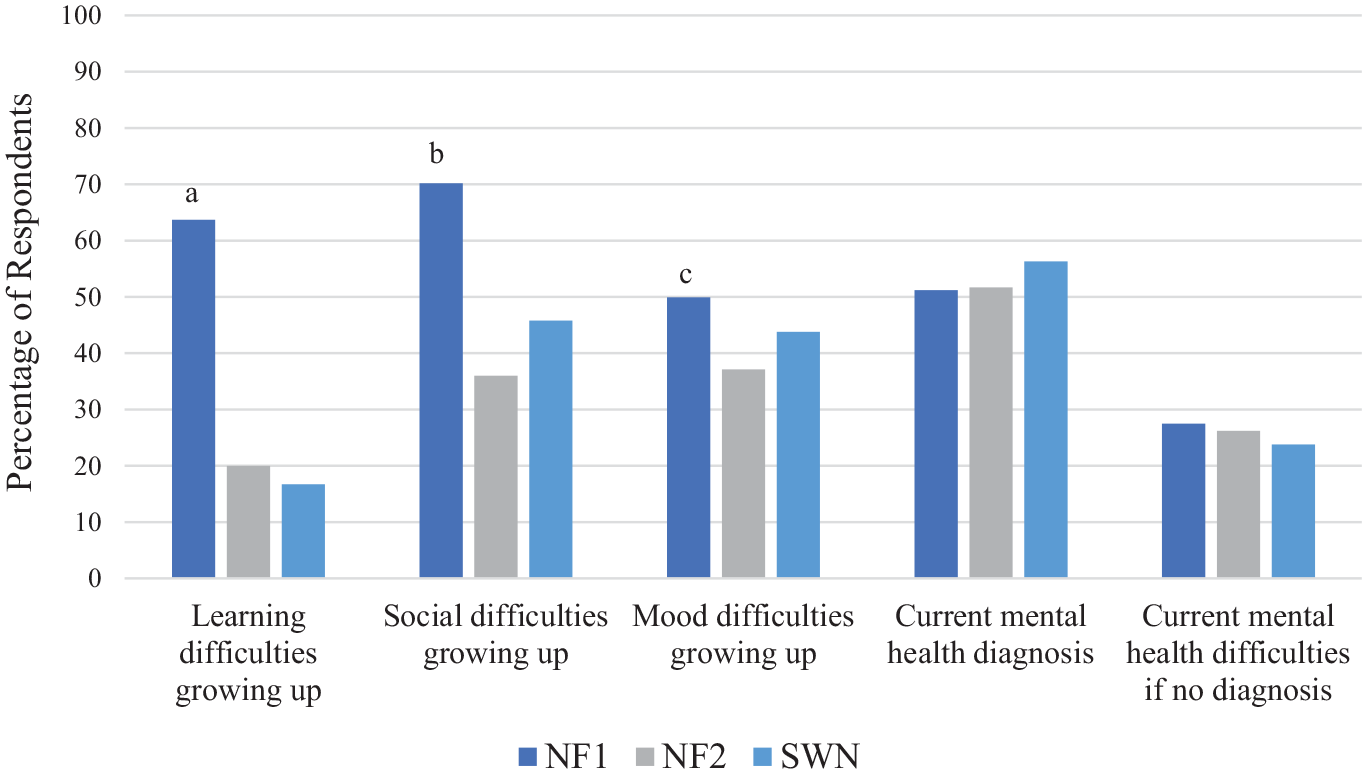
NF group comparisons regarding reported psychosocial difficulties in childhood and current mental health diagnoses and difficulties.
Comparing males and females, there were no sex differences regarding the impact of NF on domains of physical and social well-being. However, results suggested that females were more likely to report that NF influenced their emotional well-being “pretty much” or “a lot” compared to males (χ2(2626) = 6.57, p = 0.037). Females also were significantly more likely to endorse having a mental health diagnosis compared to males (χ2(2626) = 24.35, p < 0.001); 57.8% of females and 39.2% of males endorsed a diagnosis of anxiety, depression, or another mental health problem. There were no significant sex differences regarding reported rates of childhood psychosocial difficulties.
Psychosocial clinical trials preferences
Only 6.9% of the respondents reported having previously participated in a psychosocial trial and 5.8% in a drug trial for NF. However, 67.9% reported they would “probably” or “definitely” want to participate in a psychosocial trial if it targeted an important concern they had about NF. Similarly, 64.4% and 60.2% of respondents indicated they would participate in a psychosocial RCT even if they might not get the intervention or might not know which intervention they would get, respectively. More than two-thirds (70.5%) of participants indicated they would be willing to participate in a psychosocial RCT even after a short waitlist period. Over half (51.0%) of respondents preferred obtaining information about research opportunities from NF foundation websites, while 44.3% preferred hearing about studies from their NF healthcare provider, and about a third preferred getting such information from the Children’s Tumor Foundation registry, social media posts, and email listservs (35.6%, 34.8%, and 33.5%, respectively). Of note, most participants (83.9%) stated that it would be fairly or very important for them to receive results of the study after completion. The most preferred methods of communicating study results were a summary email or letter (45.7% and 36.5% marked these as the first choice, respectively).
When respondents were asked to identify the types of psychosocial trials in which they would participate, the top three targets in order of descending preference were reducing anxiety, developing a healthier lifestyle, and coping with daily stress (Table 3 for additional targets). Regarding the main reasons for participating in psychosocial trials, 73.5% of respondents indicated that they would like to improve their health and well-being, 54.3% to help others with NF based on what could be learned from the study, and 48.9% to be cared for by NF experts. Finally, the three most important outcomes to measure in a psychosocial trial according to participants were improved symptoms of anxiety, self-esteem, and overall QOL (Table 4 for additional outcomes). The top reasons for not wanting to participate in psychosocial trials were distance to clinic/research center (58.3%), costs (52.4%), time commitment in clinic (34.3%), and time away from school/work (33.3%).
Psychosocial trial preferences of the total sample.
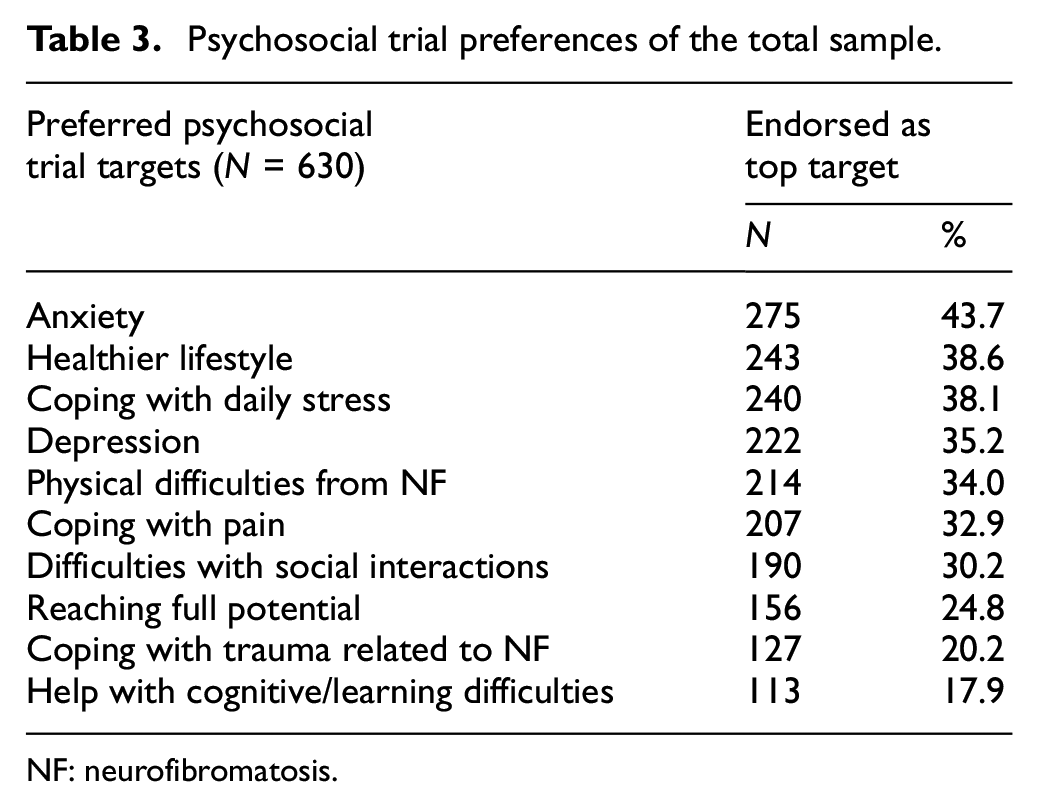
NF: neurofibromatosis.
Psychosocial trial preferences of the total sample.
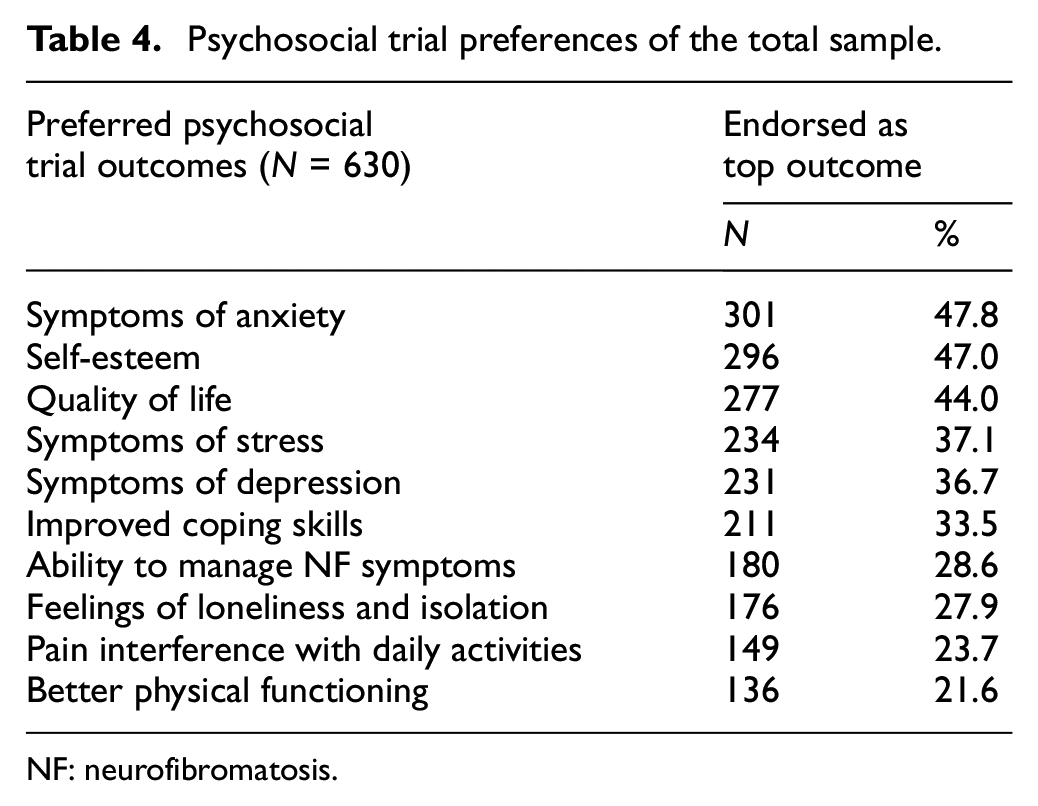
NF: neurofibromatosis.
When asked about various methods of participation, 64.4% of respondents endorsed a strong preference for having a hybrid model where they would come into the nearest NF clinic one to two times over the course of a 6-month study and complete most of the program virtually from home. Importantly, 99.5% reported having access to the Internet. In terms of type of program individuals most preferred, 55.9% of participants indicated they most preferred clinician-led individual sessions, 24% preferred clinician-led group sessions, 52.1% preferred a combination of group and individual sessions with a clinician, and 7.6% preferred group sessions with a peer facilitator. To help researchers plan psychosocial trials, the majority of respondents (69%) endorsed completing surveys before and after a trial as their first choice while participating in interviews (17%) and focus groups (11%) were less preferred.
Group differences regarding psychosocial clinical trial preferences
Across NF types (NF1, NF2, or SWN), there were no significant group differences in willingness to participate in psychosocial trials (χ2(4625) = 5.19, p = 0.27). There also were no differences in willingness to participate in psychosocial trials based on NF symptom severity (low versus moderate versus high severity: χ2(4626) = 6.24, p = 0.18).
In addition, no differences were found across NF types in interest in trials targeting improvement of social interactions, improvement of anxiety symptoms, improvement of depression symptoms, coping with stress, or developing a healthier lifestyle. However, significant group differences emerged across NF types in reported interest in trials targeting coping with pain (χ2(2628) = 27.31, p < 0.001). Bonferroni-corrected post hoc comparisons showed adults with SWN were more likely to prefer trials focused on pain support compared to individuals with NF1 or NF2 (p < 0.001 and p < 0.001, respectively). Similarly, there were significant differences across NF types with regard to reported interest in trials to support coping with increasing physical difficulties from NF (χ2(2628) = 9.62, p = 0.008). Bonferroni-corrected post hoc comparisons showed adults with NF2 were more likely to prefer trials focused on coping with increasing physical difficulties compared to individuals with NF1 (p = 0.01).
Comparing males and females, there were no sex differences in willingness to participate in psychosocial trials (χ2(1626) = 0.43, p = 0.51). The only significant sex difference in preferences for psychosocial trial targets was that females reported greater interest than males in trials to help cope with stress (χ2(1629)= 4.02, p = 0.045).
Discussion
Researchers and patient representative developed and conducted the largest survey of adults with NF (NF1, NF2 and SWN) to understand more about the impact of NF on everyday functioning, psychosocial well-being, and mental health, as well as patients’ interest and preferences for psychosocial clinical trials. Consistent with prior research, we found that within each type of NF, most adults reported having tumors, physical symptoms, and psychosocial difficulties that substantially affect their daily lives across both physical and emotional domains, with most impairment reported at work or school versus home. The majority had received a diagnosis of depression, anxiety, or another mental health problem, and more than half of those who were undiagnosed believed they would meet criteria for one of these diagnoses. These reported rates of mental health problems in our survey are higher than what was previously reported in the literature, 47 and combined with prior evidence of suicidal ideation in NF, 21 point to an urgency for routine assessment of mental health concerns in NF clinics, and development and implementation of feasible and accessible interventions for the large proportion of adults with NF in need.
Almost half of participants reported that their mood difficulties started during childhood, with less than half of them receiving psychosocial support for these problems while growing up. The pattern was similar for social interaction difficulties and learning problems, although there were some differences across NF types. Adults with NF1 reported high rates of learning and social difficulties in childhood, similar to prior studies, 48 and as compared to those with NF2 and SWN. In addition, adults with NF1 reported a higher prevalence of mood difficulties in childhood compared to NF2 but not SWN. Clearly, there is an urgency to evaluate and address these issues in childhood to promote psychosocial health and prevent the persistence or worsening of problems through adulthood. Three pediatric psychosocial interventions have been implemented for children through young adults with NF and their parents37,49,50 that were feasible and showed benefit, but more research, including fully powered trials, is sorely needed for youth with NF. 51 Although we found no differences in current mental health diagnoses or difficulties by NF type, females reported that NF affected their emotional well-being more than males, including having more mental health difficulties, which is consistent with previous research in the general population 52 and in NF1. 53 Thus, adults with all types of NF have significant mental health needs, with particularly higher concerns reported by women.
The majority of respondents were willing to participate in a psychosocial trial if it addressed an important concern, although only a small percentage had taken part in one, documenting a high unmet demand for these interventions. This enthusiastic support was evident even if the trial was randomized, blinded, or had a waitlist period. Participants also underscored the importance of being informed of the results at the end of the trial. Adults were interested in a variety of psychosocial trials and were motivated to participate to improve their own well-being and to benefit the larger NF population. Adults noted that trials should target and measure anxiety, depression, and stress, QOL, self-esteem, ability to manage NF symptoms, and loneliness and isolation. There were no differences by NF type except for pain coping, which was most preferred in SWN compared to NF1 and NF2. Published NF trials have aligned with these patient concerns31–33,37,38 except for loneliness and isolation, which have not been measured in prior trials.
Respondents noted that barriers to participation in psychosocial trials were distance, cost, and time commitment, specifically time in clinic and away from work or school. These obstacles to participation in clinical trials are common; 54 thus, virtual interventions that minimize travel and daytime conflicts may increase involvement and feasibility, particularly since almost all participants reported having Internet access. As such, participants noted that the best method of intervention delivery is a hybrid model that includes limited in-person visits with mostly remote sessions. Most adults preferred individual sessions or a combination of in-person and group sessions led by a clinician. No differences were found in preferences by NF type, and current psychosocial NF trials are consistent with these preferences.31–33,37,38
Results should be viewed in consideration of several limitations. First, this was a cross-sectional survey, with many questions answered retrospectively. Second, despite the high completion rate, the overall response rate was low, the sample was primarily White and educated, and the survey was in English; thus, the results may not generalize to the entire NF community. However, given higher rates of mental health problems among individuals from low socioeconomic backgrounds and minoritized individuals,55,56 it is likely the results are underrepresenting the actual mental health problems in NF. Clinical researchers and patient advocacy organizations are striving to increase diversity and representation in NF studies, and future work should prioritize community-engaged methodologies for equitable psychosocial NF research. Third, the survey was conducted during the COVID-19 pandemic. Although we asked about functioning prior to COVID-19, participants may have had difficulty considering only pre-COVID functioning in their answers.
Taken together, results confirm the critical need for psychosocial interventions among adults with NF to address the high rates of mental health problems and teach coping skills to manage stress and NF symptoms. Adults with NF are interested in participating in psychosocial clinical trials regardless of format (e.g. blinded or wait-list control), and findings support implementing psychosocial interventions across NF types and not necessarily for each type individually. Advancing the field of NF psychosocial research requires prioritizing funding as most has supported drug trials. While this has led to important drug approvals such as selumetinib to treat NF1 plexiform neurofibromas, 57 substantial mental health suffering remains that requires psychosocial interventions. Several small psychosocial trials31–33,37,38 have demonstrated high feasibility and improvement in outcomes that are important to adults with NF, one fully powered virtual psychosocial RCT demonstrated improved QOL 35 and coping, 36 and another full-powered trial currently is under way for adolescents. 51 Next steps include developing more psychosocial interventions for children and adolescents, using different modalities to expand access,49,58,59 conducting larger scale trials to fully evaluate new interventions for all ages, improving the transition from pediatric to adult providers,20,60 and incorporating empirically supported interventions 35 into routine clinical care as they become available. The survey results clearly emphasize the critical unmet need for meaningful interventions that are consistent with concerns and preferences of adults with NF and strongly indicate their desire to participate in psychosocial clinical trials.
Supplemental Material
sj-pdf-1-ctj-10.1177_17407745231209224 – Supplemental material for Perspectives of adults with neurofibromatosis regarding the design of psychosocial trials: Results from an anonymous online survey
Supplemental material, sj-pdf-1-ctj-10.1177_17407745231209224 for Perspectives of adults with neurofibromatosis regarding the design of psychosocial trials: Results from an anonymous online survey by Pamela L Wolters, Nour Al Ghriwati, Melissa Baker, Staci Martin, Dale Berg, Gregg Erickson, Barbara Franklin, Vanessa L Merker, Beverly Oberlander, Stephanie Reeve, Claas Rohl, Tena Rosser and Ana-Maria Vranceanu in Clinical Trials
Footnotes
Acknowledgements
The authors thank the NF organizations that recruited participants for this survey, including the Children’s Tumor Foundation, NF Network, NF Northeast, NF Midwest, NF Michigan, Littlest Tumor Foundation, and Texas NF Foundation. They thank Melissa Gates for her work on the technical development of the survey. They also thank the participants with NF who took the time and effort to complete this survey. The authors thank the Children’s Tumor Foundation for supporting the publication of this article.
Author contributions
All authors have agreed to the order in which their names are listed in the article. They all have contributed significantly to the work per the journal’s criteria as listed below. All authors have given final approval of the version to be published and agreed to be accountable for all aspects of the work. Contributions from others who do not meet the criteria for authorship are listed in the “Acknowledgments” section with permission from the contributor. P.L.W., S.M., D.B., G.E., B.F., V.L.M., B.O., S.R., C.R., T.R., and A-M.V. contributed in design and conceptualization of the study. P.L.W. and A-M.V. involved in acquisition of the data. P.L.W. and N.A.G. participated in the analysis. P.L.W., N.A.G., S.M., D.B., G.E., B.F., V.L.M., B.O., S.R., C.R., T.R., and A-M.V. participated in interpretation of the data. P.L.W., N.A.G., M.B., and A-M.V. involved in drafting the article. All authors contributed in revising the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Intramural Research Program of the National Institutes of Health, National Cancer Institute. This project has been funded in whole or in part with federal funds from the National Cancer Institute, National Institutes of Health, under Contract No. 75N910D00024. The content of this publication does not necessarily reflect the views or policies of the Department of Health and Human Services, nor does mention of trade names, commercial products, or organizations imply endorsement by the US Government.
Data availability statement
The data that support the findings of this study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.