
Abstract
Various robotic rehabilitation devices have been developed for acute stroke patients to ease therapist’s efforts and provide high-intensity training, which resulted in improved strength and functional recovery of patients; however, these improvements did not always transfer to the performance of activities of daily living (ADLs). This is because previous robotic training focuses on the proximal joints or training with exoskeleton-type devices, which do not reflect how humans interact with the environment. To improve the training effect of ADLs, a new robotic training paradigm is suggested with a parallel manipulator that mimics rotational ADL tasks. This study presents training of the proximal and distal joints simultaneously while performing manipulation tasks in a device named spherical parallel instrument for daily living emulation (SPINDLE). Six representative ADLs were chosen to show that both proximal and distal joints are trained when performing tasks with SPINDLE, as compared to the natural ADLs. These results show that SPINDLE can train individuals with movements similar to the ADLs while interacting with the manipulator. We envision using this compact tabletop device as a home-training device to increase the performance of ADLs by restoring the impaired motor function of stroke patients, leading to improved quality of life.
Keywords
Introduction
About 6.6 million individuals in the United States suffer from stroke-related motor impairments, and every year, about 800,000 individuals experience new or recurrent strokes. 1 Stroke patients often lose function of their upper limbs and have difficulty performing activities of daily living (ADLs). After the onset of stroke, the first 3 months is a crucial window when most of the rehabilitation happens by spontaneous neurological recovery. 2
During this acute stage, motor learning may help reduce motor impairment and facilitate recovery. The process of motor learning can be accelerated by rehabilitation, which may reduce chronic disabilities. 3 Occupational therapy (OT) services are often utilized to remediate or restore the function of the upper limbs. However, even after the completion of standard therapy, around 58% of individuals experience continuous challenges with ADLs. 4 Importantly, 4 years after the stroke incident, only 6% of patients are satisfied with the function of their impaired arm. 5 These residual impairments affecting ADLs indicate that OT may only have been moderately effective in improving ADLs outside of the hospital or clinic setting. 6,7 Stroke patients appear to often receive insufficient therapy for what is needed for effective rehabilitation. 8 Improvement of motor function for ADLs may occur through more intensive therapy. 9
Robotic interventions have been developed in the past to satisfy high-intensity and repeated training. Many robotic interventions have been successful in improving upper limb motor scores and strength with devices such as MIT-Manus or Armeo Power, 10 –13 but the consensus in literature demonstrates that these improvements do not always transfer to the performance of ADLs. 13 This may be due to the fact that these devices could have focused on the training of proximal joints, whereas integrating proximal with distal arm training may enhance functional gains needed for ADLs. 14,15 Second, many robotic interventions are focused on reaching tasks that are different from object manipulation. Many ADLs include manipulation tasks that require complicated three-dimensional (3D) hand posture changes. Third, robotic training sessions are often limited to patients in clinical settings because robotic systems are bulky and expensive, which make home-use challenging.
Various types of wrist rehabilitation robots have been developed to address this issue by training the distal arm. Earlier, wrist rehabilitation devices emphasized axial wrist rotation (pronation/supination) with an interface for stroke patients to practice grasping and wrist control. 16 Other exoskeleton-type designs with additional degrees of freedom (DoFs) were explored by adding wrist flexion/extension to the pronation/supination such as in Wrist Gimbal. 17 Furthermore, RiceWrist 18 employed three active DoFs with series elastic actuators to change the stiffness of the wrist joint during manipulation.
Soft robotic designs have also been developed for distal limb rehabilitation using cables and pneumatic actuators. CRAMER 19 and CDWRR 20 were developed featuring low-cost and lightweight cable-actuated mechanisms. However, these cable-actuated mechanisms showed high friction in their translational joints and low maneuverability during the wrist’s fine motor control. Pneumatic actuator devices with a glove-type apparatus were developed for stroke patients as well, 21,22 adding wrist flexion/extension or radial/ulnar deviation. 23,24 These pneumatic designs have the benefit of being lightweight and having low inertia, resulting in higher safety from the compliance of the soft robotic structure. But these systems face issues with force/torque accuracy and are less compact due to the pneumatic system for actuation. Recent rigid exoskeleton-type devices for upper limb rehabilitation focus on having a higher range of motion, better manipulability, and higher torque performance. 25,26 Another new direction of wrist devices focuses on the compactness of the devices to develop lightweight systems stressing on the practical use of the devices. 27 –30 Researchers tried to make the system more compact by implementing a compact series elastic actuator for variable stiffness control or employing smart mechanism for a fully portable 5-DoF wrist-elbow rehabilitation device. 29,30
Most of the developed devices are exoskeleton type, which require aligning the human and robot joint axes before training the patient. These devices have the advantage of training the individual distal joints, but the training task is different from how humans use their upper limbs to interact with the environment. Exoskeleton-type devices control or apply forces on individual joints of the arm due to the alignment between its joint axis and human joint axis. This may lead to an increased burden on the patient as the device controls multiple joints simultaneously resulting in tight physical human–robot interaction. 31 In addition, a recent clinical study reported that the end-effector type of robotic training is more effective in Wolf Motor Function Test and Stroke Impact Scale scores, which represent the arm function related to the daily real-world activities. 31 Another study supports that robotic training is more efficient when combined with a transition-to-task OT, which indicates that the robotic intervention itself lacks the component to transfer the training effect to a real-world function. 32 Unlike other robotic designs that are built upon the human joint axis, the adaptive and automatic presentation of task (ADAPT) system was suggested to practice ADLs that require one-dimensional (1D) rotation of the tool. The tool was installed on a manipulator to change its orientation and height. 33 ADAPT is an innovative system with an emphasis on pieces of training similar to ADLs, but the tasks were limited only to a 1D rotation of the tool.
In this study, we propose a novel training strategy involving a rehabilitation robot named spherical parallel instrument for daily living emulation (SPINDLE). The design of the robot is inspired by the well-known agile eye structure, which is based on a 3-RRR parallel structure that enables 3D rotation. 34,35 This design allows for high stiffness, precise manipulation, and low inertia. Furthermore, it facilitates mimicking ADL tasks, which involve complicated manipulation of objects. The primary motivation behind the development of SPINDLE was to overcome some of the limitations of conventional OT and previous designs of rehabilitation robots, discussed earlier, to improve patients’ performance on ADL tasks. SPINDLE will (i) enable training of both proximal and distal joints of the upper limb, which are crucial for performing ADL tasks. 14,15 Training regimes involving movement of all 3DoF of wrist can also be incorporated using SPINDLE; (ii) interact with the user as a human typically interacts with the environment in the real world. As this training resembles the real-world tasks, there is a higher chance of transferring the positive effects of training to real-world functions; (iii) allow for flexibility in movement unlike exoskeleton-type devices discussed earlier. This minimizes the burden of unnecessary human–robot interaction because this device does not require a nominal target trajectory for each individual joint of the upper limb 31 ; (iv) enable training sessions to be carried out from home owing to its compact nature. Due to this, accessibility of the required therapy can be increased, a lack of which has been previously observed. 8 This compact nature will also enable high-intensity training, which has shown to improve performance in ADL tasks; 9 (v) allow for easier donning-doffing making it less time-consuming and less cumbersome compared to exoskeleton-type devices.
The rest of this article has the following structure: The design and structure of the suggested rehabilitation robot, SPINDLE, is presented in detail in the next section. Then, the optimization of design parameters and its result will be discussed in addition to the verification of the kinematic structure of SPINDLE. Following that, human testing will demonstrate SPINDLE as a training tool by presenting the usage of proximal and distal arm joints for six representative ADLs. The last part of this article presents the discussion and conclusion.
Mathematical model of SPINDLE
Architecture of SPINDLE
Since the early 1980s, researchers have been broadly exploring the kinematic architecture of the spherical 3-RRR parallel manipulator due to its advantage of high stiffness and accuracy. 36 –41 Motivated by the manipulator design in the previous study, 35 kinematic architecture shown in Figure 1 is chosen for training manipulation tasks during ADLs. The device employs 3-DoF rotation, which will allow the wrist to perform radial/ulnar deviation, flexion/extension, and pronation/supination. SPINDLE consists of three legs with three revolute joints and can create full-fledged three axial rotations in a large workspace. The patient will maneuver the top platform with a handle to generate 3D rotations to practice object manipulation tasks. The kinematic architecture of this structure is mathematically described with the following steps.

Architecture of proposed 3-RRR spherical parallel manipulator. Three motors actuate together to change the end-effector orientation.
The manipulator consists of a top base and a bottom base connected by three curved isotropic legs, where each leg consists of three revolute joints in series. The center of the top base is indicated as H2, and the center of the bottom base is indicated as H1. This design minimizes the interference between linkages to utilize maximum workspace. The manipulator is designed to move along a spherical workspace with origin O. As shown in Figure 2, all revolute joints are designed to be located on the surface of the sphere and axes of these joints are perpendicular to the tangential plane on this spherical surface. Revolute joints at the movable top base are denoted as Vi (i = 1, 2, 3) of the i’th leg. Ui (i = 1, 2, 3) denotes revolute joints at the stationary bottom base, which are actuated by motors. The remaining revolute joints, placed between Vi and Ui, are denoted as Wi (i = 1, 2, 3). Rotating axes of joints Ui, Vi, and Wi are represented by unit vectors

Schematic diagram of the 3-RRR spherical parallel manipulator. Each leg has three revolute joints: Vi on the top base, Ui on the bottom base, and Wi between the Ui and Vi.
Two arc linkages are located between the rotational joints. Proximal link
Inverse kinematics
The inverse kinematics of the 3-RRR parallel manipulator is the foundation for motion control and trajectory planning. Prior to solving the inverse kinematics, it is crucial to first establish the home posture when all motor angles

3D CAD model of SPINDLE. The posture of the top base is denoted as a position
For a given orientation of the handle (

where


where
The next step is to define

where c indicates cos and s indicates sin. Then,

By the definition of

Through equation (6), two solutions can be obtained. Considering all three legs of the parallel manipulator, there are three different sets of equations, which lead to eight possible solutions for a given end-effector posture. The solution nearest to the previous solution is chosen to avoid ambiguity.
Forward kinematics
The forward kinematics of a spherical surface manipulator has been well described by Gosselin et al.
34
The inputs of the forward kinematics are the angles of three electrical motors (
Let the end-effector orientation be expressed by three unit vectors,

Using MATLAB fsolve function, multiple solutions satisfying equations (6) and (7) are identified. Similar to the inverse kinematics, the solution that is closest to the previous solution is chosen. The forward kinematics is cross-verified with the inverse kinematics.
Jacobian
The moving platform rotates with a rotation vector

A velocity vector-loop equation is obtained by differentiating both sides of equation (8)

Multiplication of both sides by

Let

and

The velocity equation for each leg of the spherical parallel manipulator can be written as

where

Design parameter optimization
The range of the workspace depends on the design parameters
The design parameters

where

where the norm of a matrix J is defined as

with

where n is the total number of discrete points and W is the volume of the workspace. The global maximum value of GCI is computed by dividing the hemispherical surface into discrete points with an interval of
The optimization result of GCI indicates that the optimal

where

where
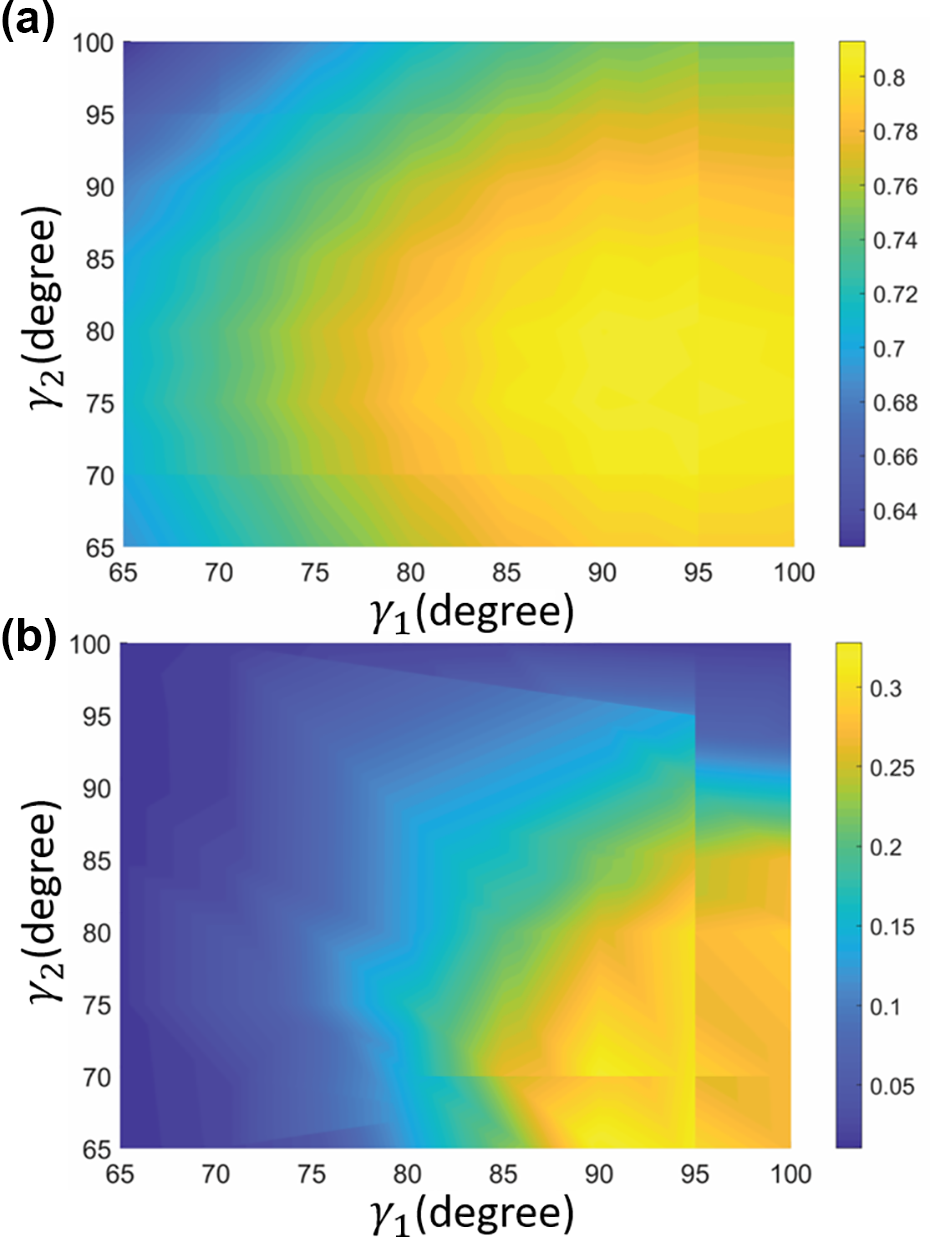
Results of design parameter optimization with respect to angles
Device set-up
Physical device
A rehabilitation device for stroke patients is designed as a 3-RRR parallel manipulator, which is capable of 3D rotational movements (Figure 5). Three legs of the manipulator connect a bottom base and a top base of the parallel manipulator. Motors with an encoder are installed on the bottom base of the manipulator to actuate these legs.
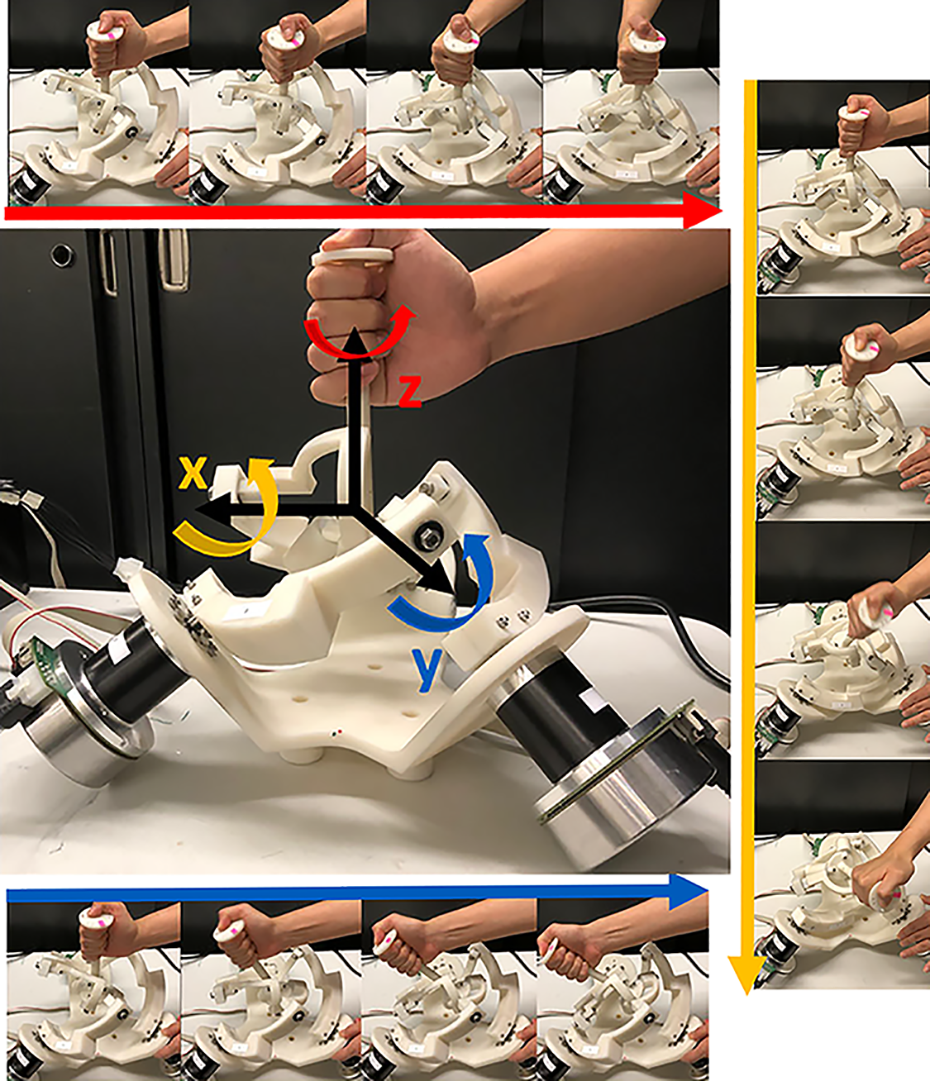
Prototype of the spherical parallel instrument for daily living emulation (SPINDLE). Different configurations of SPINDLE showing (right) roll (top) yaw (bottom) pitch manipulation. SPINDLE: spherical parallel instrument for daily living emulation.
The manipulator can provide nearly 180° of rotation in all three axes. The row, pitch, and yaw movements are shown in Figure 5. The manipulator is controlled by three EC 90 flat motors (Maxon Inc., Switzerland), which are powered by three ESCON 70/10 controller (Maxon Inc.). An amplitude of −90° to 90° can be achieved along X, Y, and Z axes with maximum torques of 7.34, 7.54, and 8.15 Nm, respectively. The dimensions of the SPINDLE are 427 mm (H) × 400 mm (W) × 348 mm (L) and it weighs about 4.5 kg. This system operates under the command of a remote control PC to myRIO 1900 (National Instrument Inc., Texas, USA) at a frequency of 500 Hz. The linkages of SPINDLE are made with tough resin material from a 3D printer to endure high stress and strain.
Verification of kinematic structure of SPINDLE
A motion capture system with 10 optical cameras (Vicon, UK) operating at 100 Hz was used to compare the kinematics of the mathematical model and physical device. There were 11 reflective markers attached on each part of SPINDLE. Four markers were on the handle to obtain the
The inverse kinematics of SPINDLE is used to calculate angles of the joints Ui with respect to the posture of the top base

Schematic to compare the joint angles

Comparison of angle values recorded by motor encoders and motion capture system. (a–c) The top, middle, and bottom diagrams represent the angles of motors 1, 2, and 3, respectively.
Feasibility human experiment for activities of daily living
Six example tasks performed on SPINDLE
To show the feasibility of training ADL tasks on SPINDLE, six representative tasks were designed, as shown in Figure 8. Six ADL tasks were chosen to demonstrate the training of both proximal and distal joints during object manipulation. The upper limb movement during the task was recorded by a motion capture system. The participant was blinded for the study and repeated each task for 10 trials. The inclusion criterion for the study required the participants (18–65 years old) to be healthy and fit to perform active daily living tasks. Individuals with upper limb prosthetics, loss of sensation, uncontrolled blood pressure, seizure disorder, severe arthritis, or other upper extremity orthopedic conditions that limit their activity level were excluded from this study.

Movement comparison of natural and SPINDLE tasks during activities of daily living: (a) opening and closing a jar cap, (b) stirring a ladle to mix a pot, (c) pouring water from a pitcher, (d) flipping a book, (e) pouring water from a cup, (f) using a screwdriver to tighten and loosen a screw. Euler angles are computed for ZYX Euler convention for α (blue),
The first task was to open and close a jar cap (jar), and the second task was to stir a pot with a ladle (ladle). This task started when the participant naturally held the ladle in hand and aligned the ladle with medial–lateral direction of the participant. The participant performed stirring action in the counterclockwise direction. The third task was to empty the water from a pitcher (pitcher). The participant started at the default position by holding the pitcher vertically. The participant mimicked emptying the water from the pitcher into a cup and was asked to be consistent with the height of the hand when holding the pitcher. The fourth task was to open and close a book (book). The fifth task was designed to mimic pouring water from a cup (cup). The cup task started while holding the cup vertically and performing pouring movements. Finally, the sixth task was to tighten and loosen a screw with a screwdriver (screwdriver). The default position of the screwdriver was 90° with the screw holder. Ten trials were performed for each task. After the completion of six tasks, the participant was asked to perform the same tasks on SPINDLE with similar instructions.
Comparison of upper limb angles measured from ADLs and SPINDLE
To understand the kinematic nature of ADL and SPINDLE training, 19 markers were attached to the upper body of a healthy participant. Markers were placed on the following positions to compute the ZYX Euler angles of the shoulder, elbow, and wrist: seventh cervical vertebrae, eighth thoracic vertebrae, sternum for the trunk; acromion, deltoid, lateral epicondyle of the humerus, medial epicondyle of the humerus, radial styloid, ulnar styloid, third metacarpal bone, mid-humerus, mid-radial, and mid-ulnar for the upper arm. The local axes to compute Euler angles were attached to the center of the joint. The local x-axis was set to be the flexion/extension axis of the joint and the local y-axis was set to be approximately in the direction of the segment of the upper limb. As shown in Figure 8, the Euler angles are presented for each joint of the upper limb along z, y, and x axes, which are indicated as α, β, and γ, respectively.
For each trial, the minimum and maximum values of Euler angles during the tasks were computed. The average and standard deviation of nine trials were computed, as presented in Table 1 for six different tasks. To compare the actual task and SPINDLE, a one-way multivariate analysis of variance (MANOVA) was performed because this study includes multiple sample means between the actual and SPINDLE tasks, such as shoulder, elbow, and wrist Euler angles. MANOVA was performed for each task using statistics software SPSS (IBM Inc,. Illinois, USA) with shoulder, elbow, and wrist Euler angles as dependent variables. 44
Comparisons of upper limb joint angles for natural and SPINDLE tasks for six representative activities during daily living (N = 3).
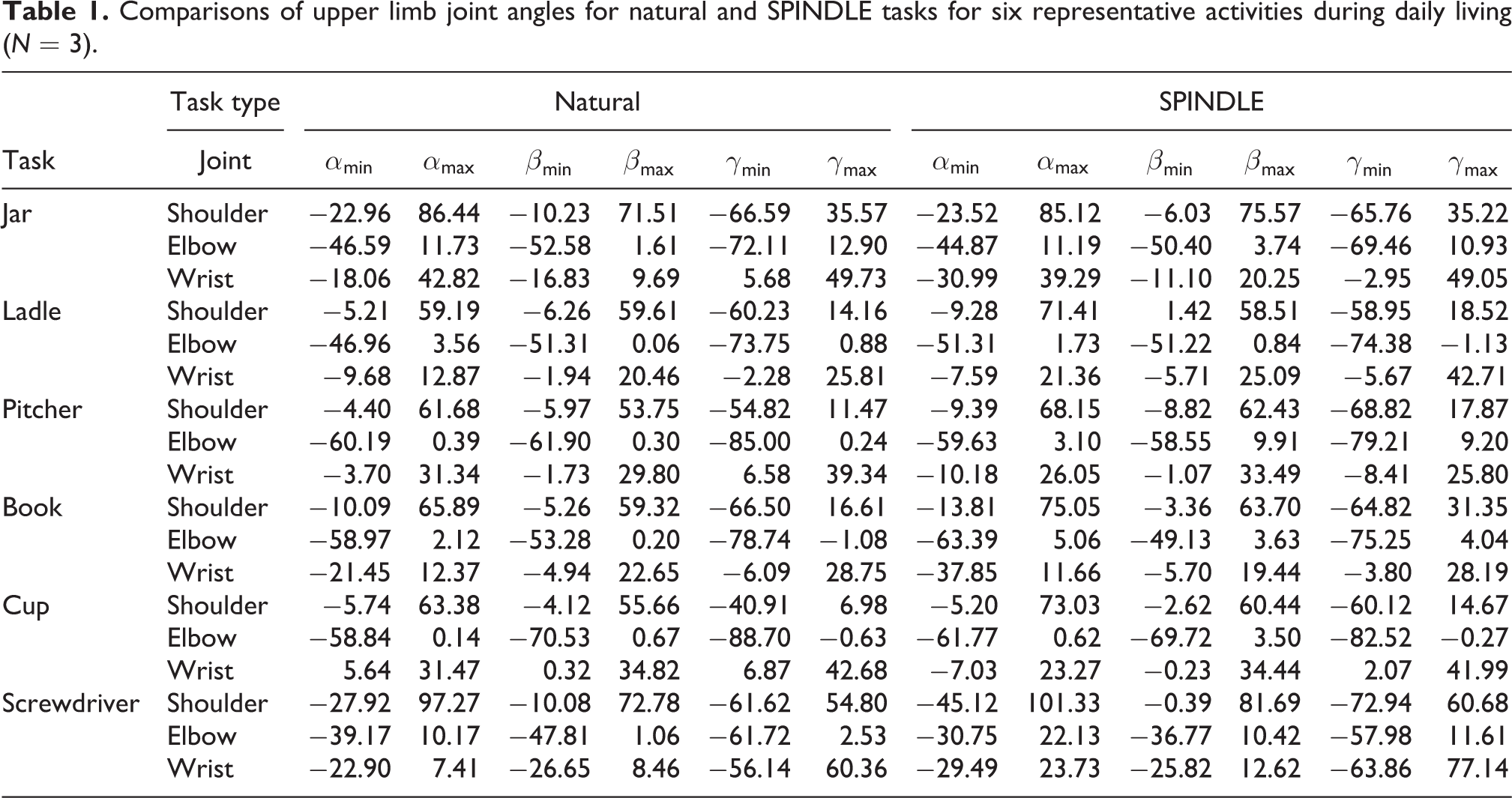
MANOVA was performed individually for each task to verify the significant differences between task types (natural vs. SPINDLE). For the book task, MANOVA showed that all participants reported no statistically significant differences in all Euler angles between natural and SPINDLE tasks (
Discussion and future work
This study presents a 3D rotational knob, SPINDLE, suggesting a rehabilitation strategy to let the user experience delicate rotational movements that are similar to ADL tasks. Particularly, this study shows the kinematic structure and the feasibility of SPINDLE as a training tool. Six representative ADL tasks were chosen to show that SPINDLE can train both proximal and distal joints of the limb with a range of motion similar to natural ADL tasks. The device features a wide range of motion and high torque capability compared to off-the-shelf haptic devices. Using mathematical models and encoder data, the device can serve as a measurement tool for quantifying the manipulation capability of patients with acute stroke by computing the range of motion from the end-effector rotation.
The device can address multiple issues of conventional OT and previous robotic intervention to enhance the performance of ADLs in stroke patients. First, stroke patients appear to receive only a small dosage of the needed therapy for effective rehabilitation. 8 SPINDLE is a tabletop device that has the potential to be installed at home due to its compact nature. Easier access to the training will increase the training time of patients with acute stroke. Second, the clinical assessments to measure the efficacy of OT appear to be coarse and insufficient. Due to the diversity of tasks used during therapy, quantification of the efficacy of OT has been challenging and has shown only moderate results to enhance the performance of ADLs. The current measures to evaluate the performance of OT interventions are the Barthel index, the Fugl Meyer, and the Nottingham extended activities of daily living, which are all descriptive and subjective. 45,46 SPINDLE can provide systematic quantification of task performance and manipulation capability of the patient. Immediate performance feedback to the patients can also positively influence participants’ motivation and self-efficacy. 47 –49 Third, the current robotic intervention has shown moderate results on the enhancement of ADLs. This may be due to the fact that these devices could have focused on the training of proximal joints, whereas integrating proximal with distal arm training may enhance functional gains needed for ADLs. 14,15 Six representative tasks showed thst SPINDLE can train both distal and proximal joints, which also enable practicing tasks of manipulating objects.
The errors of the kinematic verification might have been generated due to three possible reasons. First, the home position could not be set precisely during the calibration. The kinematics is computed based on the home posture, which could create bias of motor angles when computing inverse kinematics. Secondly, the backlash of the motor could create inaccurate measures of the motor angle when recording the movement of the end-effector. Lastly, markers used to identify the orientation and the position of the end-effector could not have been attached in an accurate position.
Future work will focus on different parts. First, the task movement between SPINDLE and the actual ADLs will be further studied. The current study presents only minimum and maximum values for comparison. Other factors such as smoothness, speed, and travel distance of the movement will be explored. Second, the implementation of an admittance controller to mimic the physical characteristics of different objects will be the main focus. An ATI Mini 45 (ATI Industrial Automation, North Carolina, USA), a six-axis force/torque sensor, will be installed on the handle to measure the human-interaction force and the data will be used to mimic the physical characteristics of virtual objects by electrical motors. These motors will render the virtual admittance that will be assigned by a physical or occupational therapist depending on the patient’s strength and motor control ability. Third, a virtual reality system will make the manipulator visually realistic. A virtual reality goggle will show a familiar object that is used frequently in daily activities. The wireless Vive Pro (HTC, Taiwan) will be used to create a virtual object and match it with the motion of SPINDLE using encoder values. In addition, exploration of different methods will provide proper visual feedback related to their performance during the task. New strategies to teach the SPINDLE how to train the patients by learning from occupational therapists will be also explored in the near future. 50,51 Lastly, acute stroke patients will be recruited by the team to show the feasibility of the intervention with SPINDLE. The target population will be stroke patients who have minimal strength to move their arm and have difficulties in performing dexterous manipulations.
Conclusion
We present a feasibility study to use a 3-RRR parallel manipulator, named SPINDLE, for training ADLs of stroke patients. The inverse kinematics, forward kinematics, and the Jacobian matrix of the SPINDLE are derived, and the design parameters are optimized to maximize the workspace and the control performance of SPINDLE. The physical device is introduced with a verification of the mathematical model using a motion capture system. The study shows six representative ADLs that were performed both on SPINDLE and the actual task. The experimental results show that SPINDLE can train both proximal and distal joints, which are essential for independently carrying out ADLs. Also, the upper limb joint movements are similar between the natural and SPINDLE tasks. SPINDLE can train the user in a way similar to how humans interact with their environment. This compact tabletop device could be installed in ICUs, homes, or community centers to train the upper limb of stroke patients for enhancing their ADL performance and quality of life.
The limitation of this work is that only three healthy participants were included in the study. In the future, more participants will be recruited, including stroke patients to show the efficacy of the presented training method. For stroke patients, the human–robot interface should also be further investigated to secure the hand of the stroke patients on the robot. We are also planning to use an elbow rest in case the participant is too weak to hold the arm against gravity. Future work will focus on the hypothesis-driven studies with stroke patients to verify whether the training from the ADL tasks on SPINDLE can transfer to actual real-world tasks by evaluating their daily activities using Barthel index or functional ability rating scale.
Footnotes
Acknowledgements
The authors thank Nicholas Lenhard for helping to collect and analyze the joint angle data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.