
Abstract
Background:
To understand the association between driver gene variations and age and gender in patients with lung adenocarcinoma, we investigated mutations of the three most important driver genes—epidermal growth factor receptor (EGFR), anaplastic lymphoma kinase (ALK) fusion genes and c-ros oncogene 1 (ROS1)—in this retrospective cohort study.
Methods:
Patients newly diagnosed with lung adenocarcinoma who received EGFR and ALK/ROS1 gene tests at our hospital from September 2014 to May 2019 were enrolled. EGFR mutations and ROS1 fusions were examined by ARMS-PCR and ALK fusions by Ventana-D5F3 IHC assay and ARMS-PCR.
Results:
Of 2544 eligible subjects, 2539 accomplished EGFR mutation tests. The prevalence of EGFR mutations was 62.1% in females, higher than that of 45.1% in males. In females, the EGFR mutation rate remained relatively stable at 60%–65% across the six age groups. Females showed an increased distribution of EGFR L858R and a decreased distribution of exon 19 deletion (19Del) by age. The incidence of ALK/ROS-1 rearrangements decreased significantly with age.
Conclusions:
EGFR 19Del mutation is more prevalent in younger males and females, while L858R mutation is prevalent in older females. Both ALK and ROS1 rearrangements are more common in younger lung adenocarcinoma. The young lung adenocarcinoma population is a distinct group rich in targetable genomic alterations, and more research is needed to understand the mechanism.
Keywords
Introduction
Lung cancer is still the most common malignancy and the leading cause of cancer death in the world, accounting for nearly 20% of all cancer deaths. 1 Recently, China saw a rapid increase in lung cancer incidents in both genders, imposing a serious threat to public health. 2 Since molecular targeted therapy greatly improved the prognosis of patients having positive driver mutations, the Committee of the 2017 National Comprehensive Cancer Network (NCCN) Guidelines for Non-Small-Cell Lung Cancer (NSCLC; Version 1) have for the first time emphasized the broad molecular profiling in patients. 3 Over the last decade, with the progress of medical insurance policy and the development of gene-testing platforms in China, driver mutation profiles for NSCLC have become more prominent and sophisticated, which can precisely identify the patients who may harbor the mutations of epidermal growth factor receptor (EGFR) and the fusion of anaplastic lymphoma kinase (ALK) or c-ros oncogene 1 (ROS1), to achieve clinical benefits.
Some large sample cohorts report that the frequency of EGFR mutations is approximately 50%–60% among Asian NSCLC populations. The ALK arrangement, as the first discovered targetable fusion oncokinase, has been identified in about 6.0% of Chinese NSCLC patients. The prevalence of ROS1 fusions in NSCLC ranges from 0.9% to 3.9% in previous studies.4-8 Although many published studies described EGFR mutations, ALK, or ROS1 fusions in clinical practice, evidence about the prevalence of these mutations or fusions in Chinese lung adenocarcinoma (LUAD) individuals of different genders and ages is insufficient. To understand the relationship between driver gene variations and age and gender in this population, we conducted this retrospective, non-interventional, single-center cohort study of LUAD patients in Beijing, China.
Methods
Patients and samples
Patients who received their first diagnose as LUAD at Beijing Chest Hospital from September 2014 to May 2019 were consecutively enrolled in this study. The inclusion criteria were defined as follows: (a) patients were diagnosed with the adenocarcinoma subtype of NSCLC; (b) pleural, pulmonary or superficial lesions were histologically diagnosed after surgery, percutaneous pulmonary biopsy, or bronchoscopic biopsy; and (c) EGFR mutations or ALK/ROS1 gene rearrangements in these samples were examined at Pathology Department, Beijing Chest Hospital. The exclusion criteria were as follows: (a) small cell lung cancer (SCLC) or other subtypes of NSCLC; (b) a history of second primary tumor within 5 years. This study was approved by the Ethics and Scientific Committee of Beijing Chest Hospital (No. BJXKYY201802-01). The procedures of subject selection and assignment are illustrated in Figure S1.
Detection of EGFR mutations
EGFR mutations were detected using an EGFR Mutations Detection Kit (Amoy Diagnostics, Xiamen, China), including mutations in exon 18-21 (G719A, G719S, G719C, T790M, L858R, L861Q, and S768I), three types of exon 20 insertions, and 19 types of exon 19 deletions. Positive and negative controls were used in each experiment, according to the manufacturer’s instructions.
Detection of ALK fusion
Ventana-D5F3 immunohistochemistry (IHC) assay was carried out on a fully automated VENTANA Benchmark XT stainer using the VENTANA anti-ALK (D5F3) rabbit monoclonal primary antibody, together with the Optiview DAB IHC detection and Optiview amplification kits (VENTANA Medical Systems, Roche Group, USA). According to the manufacture’s scoring algorithm, a binary scoring system (positive or negative for ALK status) was applied for the evaluation of staining results. The presence of strong granular cytoplasmic staining in tumor cells (any percentage of positive tumor cells) was deemed ALK-positive, whereas the absence of strong granular cytoplasmic staining in tumor cells was designated as ALK-negative (Figure S2). Rabbit Monoclonal Negative Control Ig was used as negative quality control. Specimens of the benign appendix were used as positive quality control. False-positive staining was performed to exclude alveolar macrophage cytoplasm, neurogenic cells (nerve and ganglion cells), normal mucosa and alveolar epithelial cell coloring, necrotic material nonspecific coloring, and others.9,10 Reverse transcriptase-polymerase chain reaction (RT-PCR) analysis was alternatively used to detect ALK rearrangement using an ALK Fusion Detection Kit (Amoy Diagnostics), according to the manufacturer’s protocol which was designed to detect 21 types of known EML4-ALK rearrangements and 5 uncommon rearranged types (4 types of KIF5B-ALK, and TFG-ALK).
Detection of ROS1 fusion
ROS1 fusion genes were examined using a ROS1 Fusion Detection Kit (Amoy Diagnostics) according to the manufacturer’s protocol which was designed to detect 14 different fusion types, including 4 types of SLC34A2-ROS1, 2 types of CD74-ROS1, 3 types of SDC4-ROS1, 2 types of GOPC-ROS1, as well as TPM3-ROS1, EZR-ROS1, and LRIG3-ROS1.
Statistical analysis
The chi-square test for linear trend was used to assess the relationship between the frequency of gene mutations and age. Pearson’s chi-square test was used to assess the distribution of gene alterations by gender. Fisher’s exact test was used when the frequency was less than 5 in the two-way contingency table. Statistical significance was set at a two-tailed level of 0.05. Statistical analysis was performed using SPSS Version 24.0 Statistical Software (SPSS Inc., Chicago, IL, USA).
Results
Characteristics of enrolled LUAD patients
From September 2014 to May 2019, 4335 patients were diagnosed with LUAD, and 2544 (58.7%) who completed tests for EGFR mutations or ALK/ROS1 fusions were included. The clinical and demographic characteristics of patients are listed in Table 1. There was almost an equal proportion of LUAD in females (1256, 49.4%) and males (1288, 50.6%). Patients were divided into six groups (a: ⩽40 years, b: 41–50 years, c: 51–60 years, d: 61–70 years, e: 71–80 years, f: ⩾81 years). According to the distribution of LUAD by age (Table 1), LUAD was most prevalent in patients 61–70 years of age (933, 36.7%), followed by the prevalence of 25.6% (650) in patients 51–60 years of age. apart from 325 cases (12.8%) lacking detailed stage information, 329 (12.9%), 117 (4.6%), and 365 (14.3%) patients were classified as stage I, II, and III, respectively. The other 1408 patients (55.3%) were classified as stage IV. More than half of the subjects (1628, 64.0%) in this study were never-smokers.
Characteristics of 2544 LUAD patients.
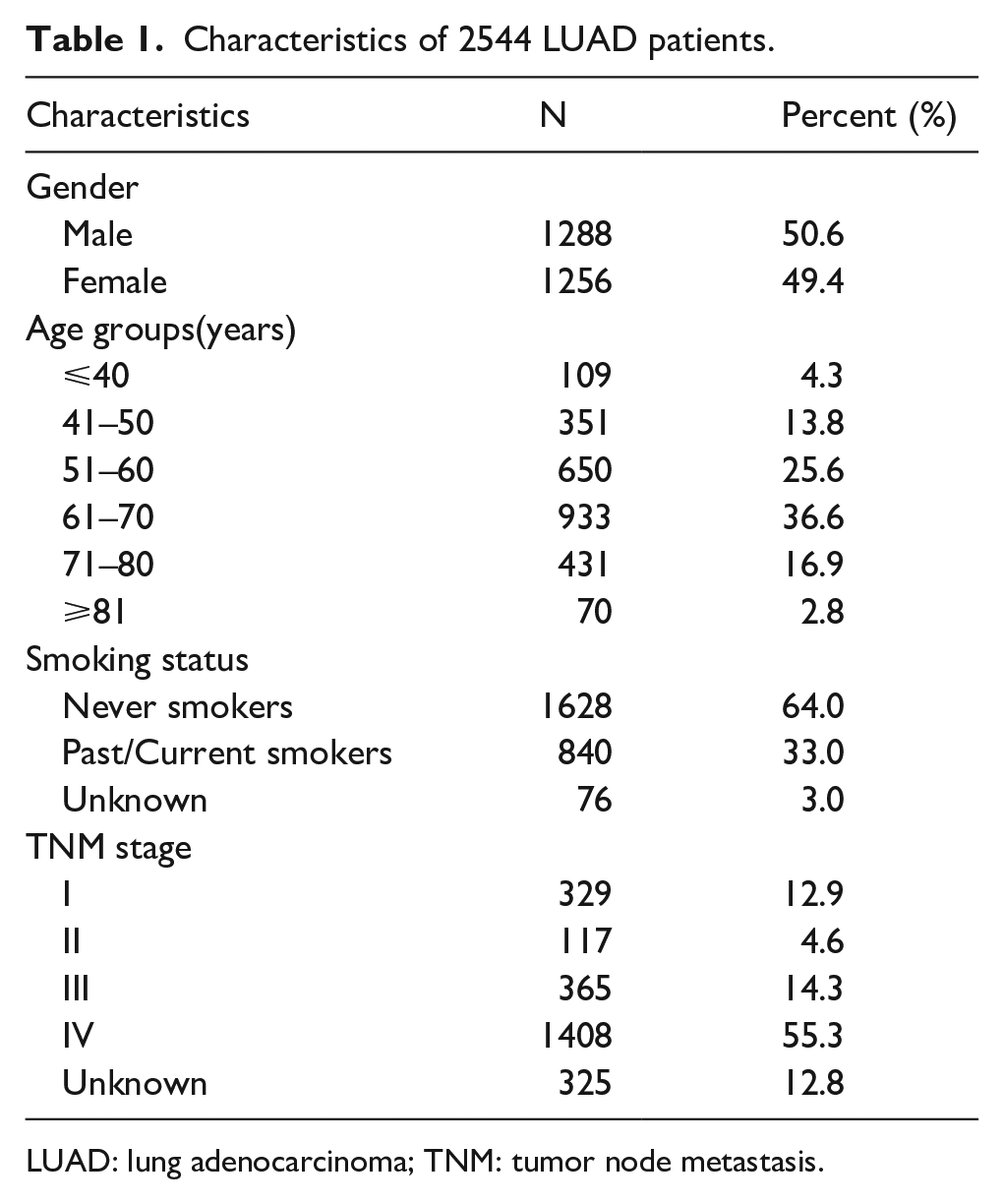
LUAD: lung adenocarcinoma; TNM: tumor node metastasis.
Comparison for distribution of EGFR mutation between different genders and age groups
In this cohort, 2539 cases completed the detection of EGFR mutations, including 603 cases (23.7%) of 19Del mutation, 609 (24.0%) of L858R mutation, 30 (1.2%) of exon 20 insertion (20 Ins), 30 (1.2%) of G719X mutation, 22 (0.8%) of L861Q mutation, 4 (0.2%) of T790M mutation, 2 (0.1%) of S768I mutation, 53 (2.1%) of compound mutations, and 5 cases without EGFR mutation results. First, the general associations between gene mutations and gender were analyzed. The results showed that the EGFR mutation rate was significantly higher in females than in males (P<0.001). The EGFR mutation incidence did not significantly change with age (Table 2). Second, we explored the distribution of EGFR mutations by gender and age. The prevalence of EGFR mutations significantly decreased with age in males from 45.1% in the ⩽ 40-year-old age group to 27.9% in the ⩾80-year-old age group (P=0.004), while the similar distribution was not observed in females (P=0.195). The prevalence of EGFR mutations in females remained stable at 60%–65% across all age groups (Table 3).
Distribution of driver gene alterations in different genders and age groups.
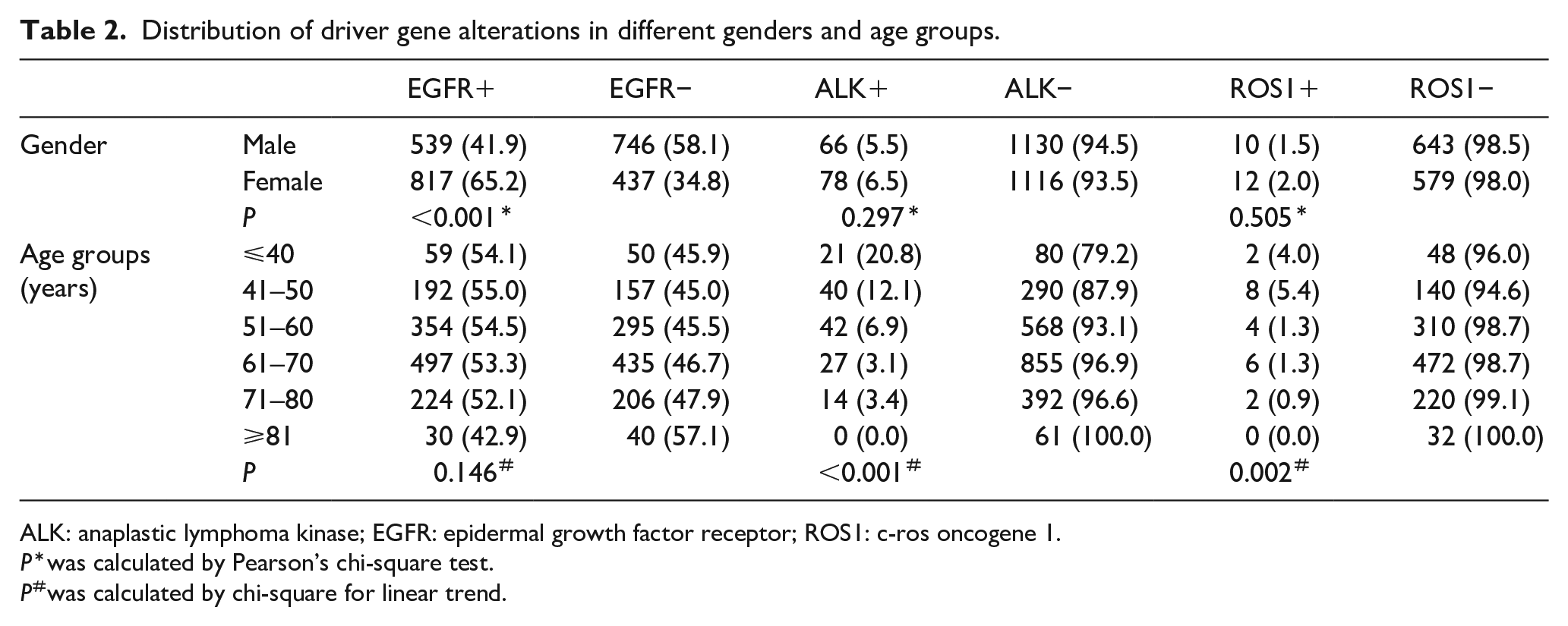
ALK: anaplastic lymphoma kinase; EGFR: epidermal growth factor receptor; ROS1: c-ros oncogene 1.
P*was calculated by Pearson’s chi-square test.
P#was calculated by chi-square for linear trend.
Comparison for EGFR mutation between age groups and genders.
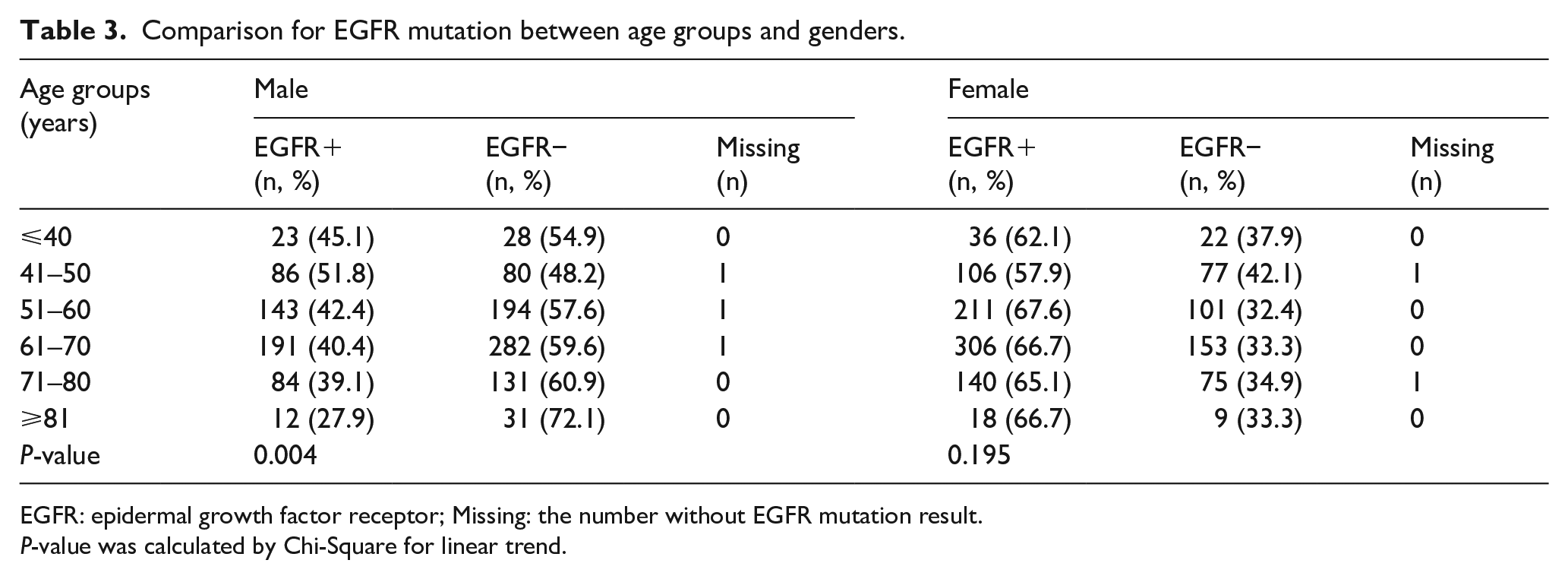
EGFR: epidermal growth factor receptor; Missing: the number without EGFR mutation result.
P-value was calculated by Chi-Square for linear trend.
The distribution of dominant EGFR mutations (L858R and 19Del) by age and gender was respectively explored. The results showed that in the female population the prevalence of L858R mutations significantly increased with age, from 20.7% in the ⩽ 40-year-old age group to 33.3% in the ⩾ 81-year-old age group (P<0.001). Also, the prevalence of 19Del mutation significantly decreased with age from 39.7% in the ⩽40-year-old age group to 22.2% in the ⩾80-year-old age group (P<0.001). Similarly, in male patients, the prevalence of 19Del mutation also decreased with age from 35.3% in the ⩽40-year-old age group to 14.0% in the ⩾80-year-old age group (P<0.001). Besides, the prevalence of L858R mutation did not significantly alter with age (P=0.800, Table 4).
The mutation distribution of L858R and 19Del in LUAD patients.
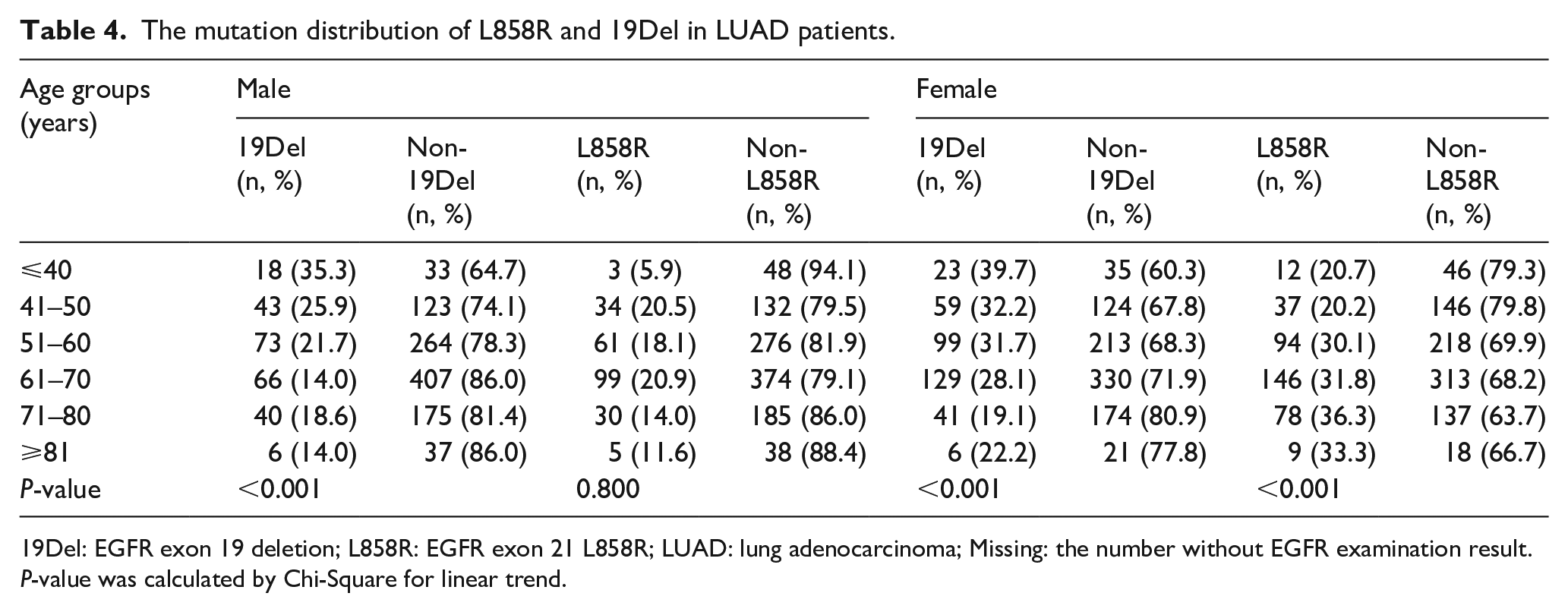
19Del: EGFR exon 19 deletion; L858R: EGFR exon 21 L858R; LUAD: lung adenocarcinoma; Missing: the number without EGFR examination result.
P-value was calculated by Chi-Square for linear trend.
Comparison of the prevalence of ALK and ROS1 fusions between genders and age groups
Despite 154 cases who did not complete the ALK detection, 2390 tumor samples were finally included in the tests for ALK fusions. The results showed that 144 cases (6.0%) were positive. Among these 144 patients, 66 (45.8%) were males and 78 (54.2%) were females. There was no significant difference in the prevalence of ALK fusions between genders. As for the distribution of ALK fusions by age, some published clinical studies reported that ALK fusions occurred more frequently in females of younger age. Some large sample cohorts reported inconsistent results of the prevalence of ALK fusions. Therefore, we analyzed the distribution of ALK fusions by age among the 144 participants. The results showed that the prevalence of ALK fusions significantly decreased with age (Table 2): it decreased from 20.7% in the ⩽40-year-old age group to 0% in the ⩾ 80-year-old age group in females; and from 21.1% in the ⩽40-year-old age group to 0% in the ⩾80-year-old age group in males (both P<0.001, Table 5).
Comparison for ALK fusion between age groups and genders.
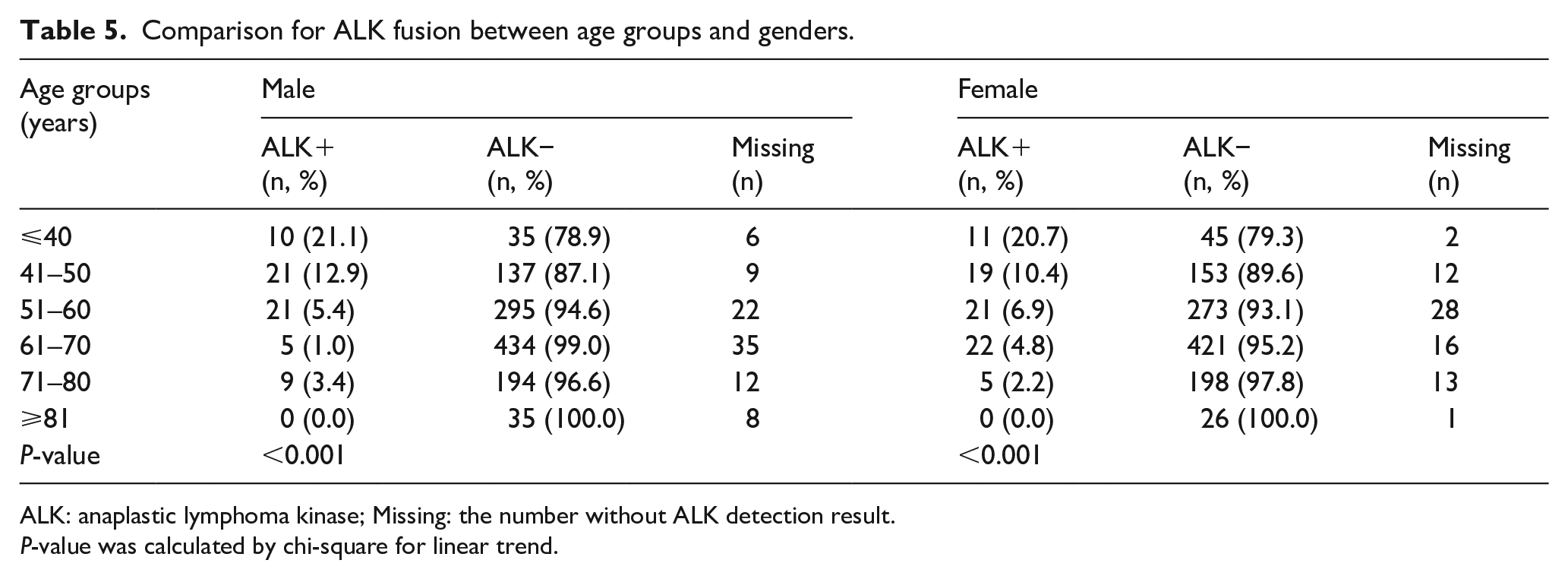
ALK: anaplastic lymphoma kinase; Missing: the number without ALK detection result.
P-value was calculated by chi-square for linear trend.
In the 1244 cases that had completed examinations for ROS1 fusions, 22 cases (1.8%) were tested positive (12 males (54.5%) and 10 females (45.5%)). There was a non-significant difference in the prevalence of ROS1 fusions between genders. Similar to the distribution of ALK fusions by age, the distribution of ROS1 fusion significantly decreased with age (Table 2). Due to the limited number of ROS1-positive subjects, the distribution of ROS1 fusions by gender in each age group was not explored.
Discussion
In the present study, we analyzed the test results of EGFR/ALK/ROS1 gene mutation profiles from 2544 LUAD samples. Our results showed a higher prevalence of EGFR mutations in females than males, and a higher prevalence of the EGFR L858R mutation in older females. The prevalence of 19Del mutation and ALK/ROS1 fusions were higher in younger patients (⩽40 years) in both genders.
Our finding showed a higher EGFR mutation rate in females than in males, which is consistent with the results of previous studies.4,6 In contrast to a higher prevalence of EGFR mutations in males, the prevalence of EGFR mutations in females of each age group remained within a narrow range of 60%–65%. It is reported that the proportions of 19Del and L858R mutations are nearly 90% of all EGFR mutation types.11 In this study, 19Del mutation was more prevalent in younger patients, and the results showed the prevalence decreased with increasing age in both genders, in contrast to the increased prevalence of L858R mutation with increasing age in females. Although 19Del and L858R mutations are both common-type EGFR mutations and these patients are under the same first-line therapy, only a few studies reported the differences in clinical and demographic characteristics between patients with 19Del and L858R mutations.12,13 In our study, the 19Del mutation was more prevalent in younger people, while the L858R mutation was more prevalent in older people. To our knowledge, few studies have explained why 19Del and L858R mutations occur in different age groups, which must be addressed promptly in a subsequent study series. In recent years, studies have revealed that patients with the 19Del mutation can benefit more from EGFR-TKI therapy than the L858R-mutant lung cancer patients. This may be attributed to the demographic difference between those with 19Del versus L858R mutations.14-16 This study provided evidence that the prevalence of ALK or ROS1+ LUAD mutations peaked at ⩽ 40 years of age. Of note, younger age is not a distinguishing feature of EGFR-mutated LUAD, especially in females, and a similar result has been documented in a large-sample, multinational, prospective study.6,17 This gives us a hint that it is of extreme importance for females to conduct EGFR mutation types in all age groups because the prevalence of EGFR mutations in older individuals is as high as that in younger people.
In this study, ALK fusions were detected in 2390 LUAD patients, and 144 positive samples were confirmed. The positive rate of the ALK fusion gene expression was 6.0%, which was consistent with the results of two large, population-based studies.18,19 Owing to a low frequency of ALK fusion, there are still insufficient data to depict the distribution of ALK fusions by all ages and genders. In this cohort, we found that there was a non-significant difference in the prevalence of ALK fusions between males and females (5.5% vs. 6.5%). Across the six age groups, the prevalence of ALK fusions in both genders significantly decreased with age from over 20% in the ⩽ 40-year-old age group to 0% in the ⩾ 80-year-old age group. This trend has been reported in several studies.20,21 The current view of a high incidence of ALK fusion in younger NSCLC patients is perceived by the public, but current data are insufficient for a large population-based study which is representative of participants of all ages for more precise validation. 7 In our study, of the 1244 samples involved in the detection of ROS1 fusions, 22 (10 males, and 12 females) were positive. In the ⩽ 50-year-old age group, the prevalence of ROS1 fusions was up to 10%, much higher than the average reported. The results observed in our study indicate that the young LUAD population is a distinct subgroup that may harbor different natural history and underlying biological mechanisms.
In this study, as for females, although there was a non-significant difference in the prevalence of EGFR mutation between the six age groups, the prevalence of the sum of EGFR/ALK/ROS1 gene alterations was much higher in younger patients than that in older patients. These findings are consistent with the results of previous studies.21,22,23,24 While younger age is associated with more aggressive histologies and higher mortality in patients with breast cancer or colon cancer, whether age is a predictor of poor survival in NSCLC remains controversial.24-26 Some studies reported that younger patients with NSCLC, even with lower rates of comorbidities and functional impairment, did not show a survival benefit compared with older patients.17,22 Therefore, for younger patients rich in targetable genomic alterations, more effort must be made to improve the prognosis. Restricted by provisions of health insurance, only EGFR/ALK/ROS1 mutations were detected in the current study. Allowing for the high prevalence of gene alterations in LUAD in the young population, next-generation sequencing is more sensitive to multiple targetable genomic alterations to achieve more precise medical care.
However, there are several inherent limitations in this study, including the retrospective nature. In addition, our results can be subject to referral bias due to the single-center retrospective design. Last, but not least, multivariate analysis is unavailable due to incomplete data of clinicopathologic characteristics, including ethnicity, tumor diameter, the detailed metastatic organs, and the degree of tumor differentiation. Therefore, further studies and more clinicopathologic data must be obtained for more robust assessments.
Conclusion
EGFR mutations and ALK/ROS1 fusions dominate driver gene alterations in lung cancers, which have been considered as biopsy biomarkers and putative therapeutic targets of advanced NSCLC. We analyzed the data of these driver gene mutations from 2544 LUAD samples and the correlations between gene mutations and age and genders. Our findings demonstrate that younger patients with LUAD are a distinctive population possessing high proportions of targetable genomic alterations. Also, the prevalence of ALK and ROS1 mutations significantly decrease with age. EGFR mutations are more prevalent in females; 19Del mutations more frequently appear in the younger population; and L858R mutation is more common in older women. This study will inspire more new findings of clinical and demographic characteristics of driver gene alterations in the Chinese LUAD population.
Supplemental Material
figure_legend_-R3 – Supplemental material for Driver gene alterations in lung adenocarcinoma: Demographic features of 2544 Chinese cases
Supplemental material, figure_legend_-R3 for Driver gene alterations in lung adenocarcinoma: Demographic features of 2544 Chinese cases by Mingming Hu, Tongmei Zhang, Yuan Yang, Nanying Che, Jie Li, Zichen Liu and Baolan Li in The International Journal of Biological Markers
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Because this retrospective study was conducted using the data extracted from electronic medical records rather than recruited participants, we received an exemption for patient informed consent. The study design was approved by the Ethics and Scientific Committee of the Beijing Chest Hospital.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.