
Abstract
Background:
Molecular diagnostic testing is necessary to guide optimal first-line treatment. The number of patients who receive first-line treatment based on biomarker analysis in Japan is unknown. We aimed to determine the proportion of nonsquamous non-small cell lung cancer (NSCLC) patients for whom first-line treatment was selected based on biomarker testing.
Methods:
This retrospective, multicenter, observational study registered patients aged ⩾20 years with locally advanced or metastatic nonsquamous NSCLC who started first-line treatment between August and December 2017 in Japan. Data were collected from medical records between January and May 2018. The primary endpoint was the proportion of patients with confirmed biomarker status for first-line treatment decision.
Results:
Among 202 patients enrolled from 11 centers, 161 (79.7%; 95% confidence interval, 74.2–85.2%) had confirmed biomarker status. The testing rate was highest for epidermal growth factor receptor (EGFR; 97.5%), followed by anaplastic lymphoma kinase (ALK; 88.1%), programmed death ligand-1 (PD-L1; 87.1%), and ROS1 (67.3%). For first-line treatment, 70/75 patients with EGFR-positive tumors were administered an EGFR-TKI; 14/15 patients with ALK-positive tumors received an ALK inhibitor; 2/2 patients with ROS1-positive tumors received a ROS1 inhibitor; and 29/36 driver mutation-negative patients with a PD-L1 tumor proportion score ⩾50% were administered an anti-PD-1 monoclonal antibody. Median times from confirmed diagnosis date to first-line treatment initiation, and from first biomarker test order to last biomarker test result were 19 and 11 days, respectively.
Conclusions:
The proportion of nonsquamous NSCLC patients with confirmed biomarker status for first-line treatment was considered insufficient and in need of improvement.
Introduction
According to recent statistics, lung cancer is among the most common cancers in both men [84,500 cases (15%)] and women [40,600 cases (9%)] in Japan. 1 In 2018, lung cancer was the leading cause of cancer deaths among men [55,100 deaths (25%)], and the second leading cause of cancer deaths after colon/rectum cancer among women [22,400 deaths (14%)] in Japan. 1
Although there have been recent advances in the development of molecular-targeted agents and immunotherapy for lung cancer, these agents are effective only in patients with targeted molecular biological characteristics. Cytotoxic chemotherapy, molecular-targeted therapy [epidermal growth factor receptor (EGFR), anaplastic lymphoma kinase (ALK), and ROS proto-oncogene 1 (ROS1) inhibitors], and immune checkpoint inhibitors [anti-programmed cell death protein-1 (PD-1) antibody] have been approved as first-line treatment for advanced nonsquamous non-small cell lung cancer (NSCLC) patients in Japan.
Molecular biomarker testing is necessary to guide the selection of optimal first-line treatment with demonstrated effectiveness against the molecular defects relevant to each individual patient. Some molecular biomarker tests were available in daily clinical practice in Japan. Specifically, the following molecular biomarker tests were used in Japan in conjunction with laboratory-developed tests for the detection of several markers: the cobas® EGFR Mutation Test (Roche Diagnostics, Indianapolis, IN, USA) for the detection of EGFR mutations as a companion diagnostic test with EGFR-tyrosine kinase inhibitors (EGFR-TKIs), the Vysis ALK Break Apart FISH Probe Kit (Abbott Laboratories, Chicago, IL, USA), and the Histofine ALK iAEP kit (Nichirei Bioscience, Tokyo, Japan) for the detection of ALK as companion diagnostic tests with ALK inhibitors, the OncoGuide AmoyDx ROS1 gene fusions detection kit (Amoy Diagnostics Co Ltd., Xiamen, China) for the detection of ROS1 as a companion diagnostic test with ROS1 inhibitors, and the programmed death-ligand 1 (PD-L1) IHC 22C3 pharmDx and PD-L1 IHC 28-8 pharmDx (Dako, Carpinteria, CA, USA) for the detection of PD-L1 as companion diagnostic tests with anti-PD-1 monoclonal antibodies.
The 2018 Guideline for Treatment of Lung Cancer of The Japan Lung Cancer Society recommends testing patients with nonsquamous NSCLC for multiple biomarkers, including EGFR gene mutation, ALK fusion, ROS1 fusion, PD-L1 expression, and BRAF gene mutation. 2 However, these biomarker tests cannot be performed in some patients with advanced NSCLC because tissue samples are insufficient for performing multiple biomarker tests. 3 Furthermore, tissue samples do not always contain sufficient tumor cells for the detection of such biomarkers. If biomarker tests are performed sequentially, some patients might have to wait to start first-line treatment until all the biomarker test results are available.
The number of patients who receive personalized first-line treatment based on the results of biomarker analysis in the real clinical setting in Japan is unknown. The present study aimed to determine the proportion of nonsquamous NSCLC patients for whom first-line treatment was selected based on biomarker testing results by investigating biomarker testing status before starting first-line treatment.
Methods
Study design
In this retrospective, multicenter, observational study, data were collected from the clinical records of patients with locally advanced or metastatic nonsquamous NSCLC in Japan. Subjects were asked for consent and data were collected from January 2018 to May 2018. The last patient’s last visit was in May 2018, and the database was locked in July 2018.
The following data were collected from patients’ clinical records: patients’ clinical background, sample collection, biomarker testing, and selection of first-line treatment. To avoid selection bias at the time of enrollment, patients who were eligible for this study were enrolled in a consecutive and sequential manner.
The study protocol was approved by the ethical review board and the institutional review board of each participating medical center, the names of which are presented, with approval numbers, in online supplementary Table 1. The study adhered to the guidelines set forth by the Declaration of Helsinki, and study patients provided written informed consent at study enrollment. In cases when patients could not be contacted owing to their death, change of residence, or other cause, patients were enrolled in this study by an appropriate method that was deemed equivalent to obtaining consent from the patients, in accordance with the decisions of the institutional review board at each center.
Patients
Patients aged ⩾20 years at the time of informed consent, with locally advanced or metastatic nonsquamous NSCLC, who did not have an indication for radical surgery or radiotherapy, with an Eastern Cooperative Oncology Group (ECOG) performance status (PS) of 0–1, and who started first-line treatment between 1 August 2017 and 31 December 2017, were included in this study. Patients with postoperative recurrence, those enrolled in clinical trials of an unapproved drug as first-line therapy for advanced NSCLC, and those otherwise considered unsuitable to participate in this study by the investigators at the study sites were excluded.
Endpoints
The primary endpoint was the proportion of patients with confirmed biomarker status for first-line treatment decision. According to the 2016 Guideline for Treatment of Lung Cancer of The Japan Lung Cancer Society, 4 the primary endpoint was defined as the proportion of patients who met criteria A, B, or C, as follows: (A) patients who tested positive for at least EGFR, ALK, or ROS1 gene alteration prior to starting first-line treatment; (B) patients who tested negative for all EGFR, ALK, and ROS1 gene alterations and had a PD-L1 tumor proportion score (TPS) ⩾50% prior to starting first-line treatment; or (C) patients who tested negative for all EGFR, ALK, and ROS1 gene alterations and had a PD-L1 TPS <50% prior to starting first-line treatment. The secondary endpoints were the proportion of patients who underwent each biomarker test, the proportion of patients who tested positive for each biomarker, the combination and order of biomarker tests performed, selection of first-line treatment, and time to initiation of first-line treatment. In this study, the driver mutations, that is, those that confer a growth advantage on the cancer cell, 5 specifically assessed were those for EGFR, ALK, and ROS1.
Statistical analysis
Sample size based on statistical power was not calculated because this was a descriptive study. This study aimed to enroll 200 patients from 10 to 15 sites in Japan, as this was considered the number of cases that could be collected during the study period. Although the width of a confidence interval (CI) depends on a true value of the primary endpoint, this sample size would yield a CI of a width of <15% for any value of a plausible range of the primary endpoint. Descriptive statistics were used for baseline demographic and clinical characteristics, with n (%) for categorical variables and median (range) for continuous variables. All endpoints were summarized descriptively. Base SAS® Version 9.4 (SAS Institute Inc., Cary, NC, USA) was used for statistical analysis.
Results
Patients
A total of 202 patients were enrolled from 11 medical centers in Japan. Patients had a median age of 70 (range, 32–89) years and 62.4% were male (Table 1). Most patients (68.8%) had an ECOG PS of 1 and were classified as having adenocarcinoma histological type (90.6%).
Patient characteristics.

Data are presented as n (%) unless otherwise stated.
Large cell carcinoma: three patients; neuroendocrine tumor of the lung: two patients; NSCLC not otherwise specified: 14 patients.
ECOG PS, Eastern Cooperative Oncology Group performance status; NSCLC, non-small cell lung cancer.
Endpoints
The proportion of patients with confirmed biomarker status for first-line treatment decision (primary endpoint) was 79.7% (95% CI, 74.2–85.2%) (Figure 1). The proportions of patients who met criteria A, B, and C were 45.5%, 17.8%, and 16.3%, respectively. Of 202 patients, 41 (20.3%) did not meet the criteria for the primary endpoint (Table 2).
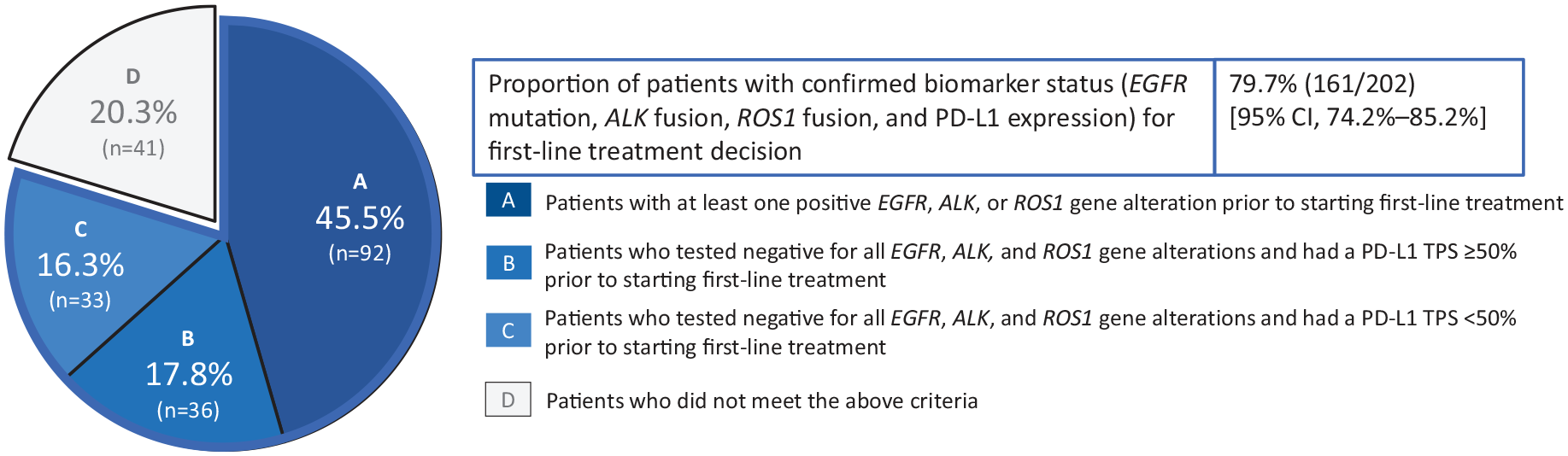
Proportion of patients with confirmed biomarker status (EGFR mutation, ALK fusion, ROS1 fusion, and PD-L1 expression) for first-line treatment decision.
Details of 41 patients who did not meet criteria for the primary endpoint.

Driver mutations: EGFR, ALK, ROS1.
ALK, anaplastic lymphoma kinase; EGFR, epidermal growth factor receptor; PD-L1, programmed death-ligand 1; ROS1, ROS proto-oncogene 1.
The proportions of patients who underwent biomarker testing for EGFR, ALK, ROS1, and PD-L1 were 97.5%, 88.1%, 67.3%, and 87.1%, respectively (Figure 2). A total of 206 EGFR tests were performed, among which 118 (57.3%) tissue samples were used for testing. A total of 212 ALK tests were performed, among which 164 (77.4%) tissue samples were used for testing. A total of 158 ROS1 tests were performed, among which 101 (63.9%) tissue samples were used for testing. A total of 204 PD-L1 tests were performed, among which 170 (83.3%) tissue samples were used for testing. Nontissue samples used included cytology samples and cell blocks. The proportions of patients who tested positive for EGFR, ALK, and ROS1 were 38.1%, 8.4%, and 1.5%, respectively (Figure 2). The proportions of patients with PD-L1 TPS <1%, 1–49%, and ⩾50% were 33.0%, 24.4%, and 40.3%, respectively. The driver mutations for EGFR, ALK, and ROS1 were mutually exclusive.

Testing rate and positive rate for each biomarker.
Among 76 patients who were driver mutation-positive and underwent PD-L1 testing, 38.2% (29/76), 32.9% (25/76), and 25.0% (19/76) had a PD-L1 TPS <1%, 1–49%, and ⩾50%, respectively; 3.9% (3/76) had invalid test results. Among 70 patients who were driver mutation-negative and underwent PD-L1 testing, 28.6% (20/70), 18.6% (13/70), and 51.4% (36/70) had a PD-L1 TPS <1%, 1–49%, and ⩾50%, respectively; 1.4% (1/70) had invalid test results.
The patterns of biomarker testing performed are shown in Table 3. The most common testing pattern was concurrent testing of EGFR, ALK, ROS1, and PD-L1 (64/202, 31.7%), followed by concurrent testing of EGFR, ALK, and PD-L1 (37/202, 18.3%).
Patterns of biomarker testing performed.

Arrow (⇒) indicates sequential order of tests. Virgule (/) indicates concurrent testing.
ALK, anaplastic lymphoma kinase; EGFR, epidermal growth factor receptor; PD-L1, programmed death-ligand 1; ROS1, ROS proto-oncogene 1.
The selection of first-line treatment by biomarker status is shown in Table 4. Among the 75 patients who tested positive for EGFR, 93.3% (70/75) received first-line treatment with an EGFR-TKI. Among the 15 patients who tested positive for ALK, 93.3% (14/15) received first-line treatment with an ALK inhibitor. The patients who tested positive for ROS1 (100%) received first-line treatment with a ROS1 inhibitor. Among the 36 patients who were driver mutation-negative and had a PD-L1 TPS ⩾50%, 80.6% (29/36) received first-line treatment with an anti-PD-1 monoclonal antibody. All 33 patients (100%) who were driver mutation-negative and had a PD-L1 TPS <50% received first-line treatment with chemotherapy.
First-line treatment by biomarker status.
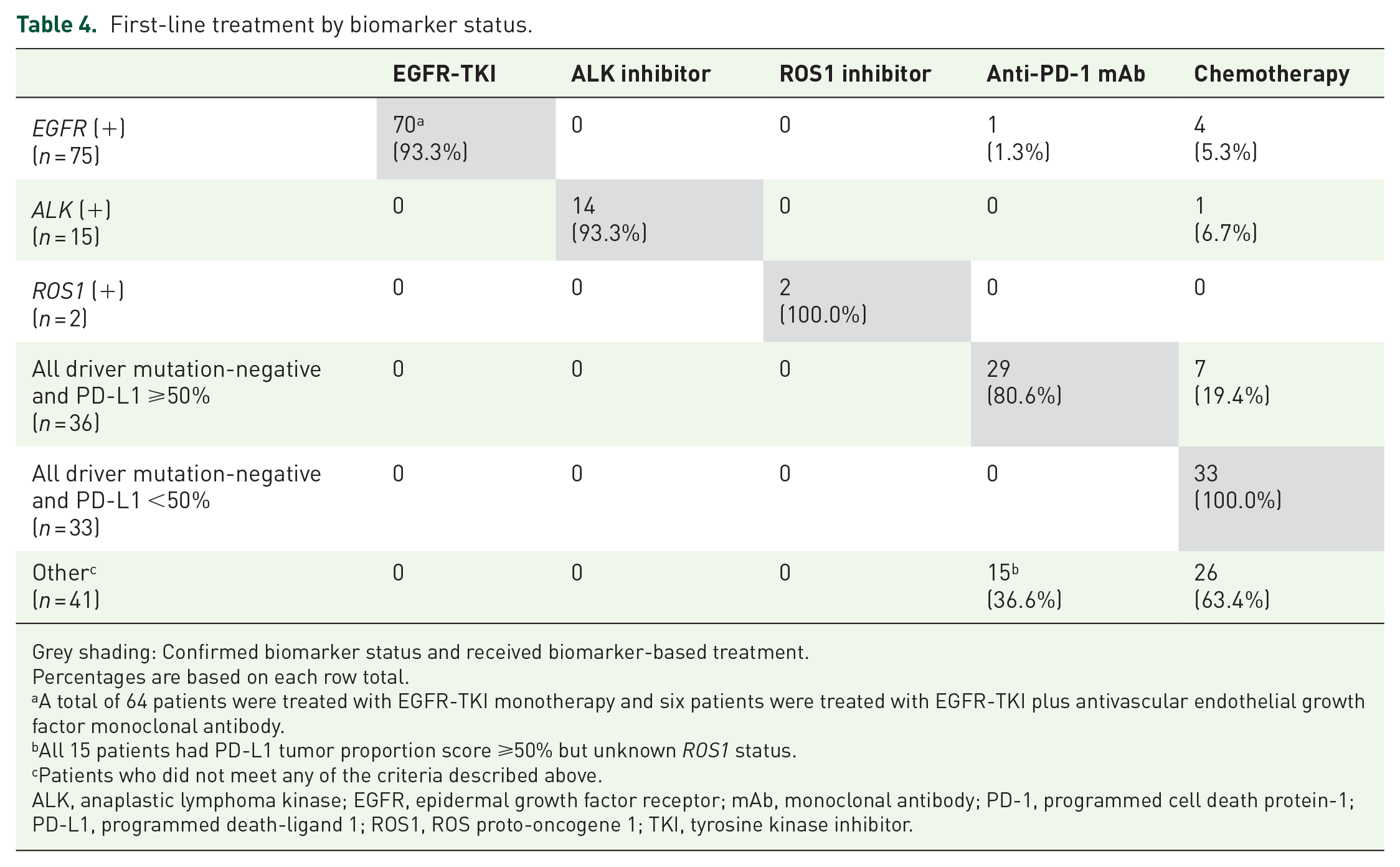
Grey shading: Confirmed biomarker status and received biomarker-based treatment.
Percentages are based on each row total.
A total of 64 patients were treated with EGFR-TKI monotherapy and six patients were treated with EGFR-TKI plus antivascular endothelial growth factor monoclonal antibody.
All 15 patients had PD-L1 tumor proportion score ⩾50% but unknown ROS1 status.
Patients who did not meet any of the criteria described above.
ALK, anaplastic lymphoma kinase; EGFR, epidermal growth factor receptor; mAb, monoclonal antibody; PD-1, programmed cell death protein-1; PD-L1, programmed death-ligand 1; ROS1, ROS proto-oncogene 1; TKI, tyrosine kinase inhibitor.
The median time from the date of confirmed diagnosis to initiation of first-line treatment was 19.0 (range, 0–232) days (n = 202). The median time between ordering the first biomarker test and receiving the last biomarker test result was 11.0 (range, 2–67) days (n = 197).
Discussion
Previous studies have investigated multiple biomarker testing rates and treatment patterns in NSCLC patients.6–9 However, to the best of our knowledge, the present study is the first to focus on the proportion of advanced nonsquamous NSCLC patients with confirmed biomarker status for first-line treatment decision.
The proportion of patients with confirmed biomarker status for first-line treatment decision was 79.7% (161/202). Regarding the testing rate for individual biomarkers, the testing rate was highest for EGFR (97.5%), followed by ALK (88.1%) and PD-L1 (87.1%), and was lowest for ROS1 (67.3%). The main reasons for no biomarker testing were physician or hospital policies regarding ROS1 testing (29/66 patients) and ALK testing (6/24 patients), and insufficient sample amount for PD-L1 testing (11/26 patients). ‘Physician/hospital policies’ was a relatively frequent reason for a lack of ROS1 and ALK testing. We consider that a possible explanation for this is the relatively low frequency of these mutations. In Japanese lung adenocarcinoma cases, the frequency of ALK mutation was reported to be 3.9% and that for ROS1 mutation, 1.2%. 10 Of note, ROS1 testing (companion diagnostics for ROS1 testing; ROS1 fusion gene detection kit, Amoy Diagnostics, Xiamen, China) was launched in Japan in June 2017. Because the patients enrolled in this study initiated first-line treatment between August and December 2017, it is possible that the recently approved ROS1 testing method was not widely performed at the time of the study. This may explain the low rate of ROS1 testing in the present study. Another potential reason for this is that, in some centers, testing for ROS1 is conducted only if the results for EGFR and ALK testing are negative, as these tests are mutually exclusive. If we consider an additional 15 patients who were treated with an anti-PD-1 monoclonal antibody based on PD-L1 test results (Table 4) without undergoing ROS1 testing, the proportion of patients increases to 87.1% [(161 + 15 = 176)/202]. The most common testing pattern was concurrent testing of EGFR, ALK, ROS1, and PD-L1 (31.7%) followed by concurrent testing of EGFR, ALK, and PD-L1 (18.3%). The median time from diagnosis to initiation of first-line treatment was 19 days, and the median turnaround time for overall biomarker testing was 11 days. Finally, among the 161 patients with confirmed biomarker status, 148 (91.9%) received appropriate biomarker-based treatment.
In the PIvOTAL study, 6 a multinational retrospective study of molecular testing and treatment patterns in patients with advanced NSCLC, among the 129 Japanese patients included, the molecular testing rate was 81% for EGFR mutation and 19% for ALK rearrangement (versus 97.5% and 88.1%, respectively, in the present study). A possible reason for the higher ALK testing rate in the present study is that there is a greater awareness among clinicians and institutions of the current evidence-based guidelines on the subject and the overall importance of molecular testing in order to adequately select the best targeted therapy for patients. It should be noted that the PIvOTAL study was performed between 2011 and 2013, and that ALK inhibitors were first approved in Japan in 2012. Therefore, clinicians may have believed ALK testing to be unnecessary or they may not have been aware of this test before the approval of ALK inhibitors.
Consistent with the results of the present study, another previous multinational retrospective chart review conducted in the US and European countries that evaluated trends in NSCLC biomarker testing rates found that the majority of patients underwent EGFR and ALK testing. 8 In the present study, the testing rate was highest for EGFR compared with that for ALK, PD-L1, and ROS1. These results are consistent with those of the PIvOTAL study, which showed that in all countries included in the study, the EGFR testing rate was higher than those of other molecular tests. The proportions of patients in Japan who tested positive for EGFR and ALK in the PIvOTAL study were 42% and 8%, respectively; these values were consistent with those in the present study (38.1% and 8.4%, respectively).
The selection of first-line treatment with an EGFR-TKI, ALK inhibitor, and ROS1 inhibitor was performed in 93.3%, 93.3%, and 100% of patients who tested positive for the respective biomarker in the present study. These values were consistent with those reported in a previous retrospective study, which found that 96.8% (n = 61) of patients presenting with an actionable ALK, EGFR, or ROS1 mutation were prescribed an appropriate targeted therapy. 9 Ideally, the proportion of patients with confirmed biomarker status for first-line treatment decision would be 100%. However, this survey revealed that, in 20% of patients, the first-line treatment was selected even though their biomarker status was not confirmed. The biomarker testing rate was considered unsatisfactory; in particular, the ROS1 testing rate was low in the present study. To improve this rate in the real-world clinical setting in Japan, awareness of ROS1 testing should be increased among physicians because the low ROS1 testing rate was due to physician/hospital policies. In addition, an adequate amount of tissue samples should be obtained for multiple biomarker testing, given that the low PD-L1 testing rate in this study was attributed to an insufficient amount of samples obtained.
A single-center study by Yu and colleagues evaluated single-gene testing versus multiple biomarker testing rates using Oncomine Dx Target Test for advanced NSCLC. 7 The Oncomine Dx Target Test is a next-generation sequencing (NGS) panel for NSCLC testing, which could facilitate access to multiple biomarker testing using small tissue samples. In general, NGS can detect a number of gene alterations concurrently using a single sample. In contrast, the biomarker testing methods used in the present study require a sample each. Thus, the use of NGS methods might be useful in terms of saving tissue samples, or in instances in which tissue samples are too small for multiple biomarker tests. Therefore, the detection of gene alterations using NGS might lead to an increased proportion of patients with confirmed biomarker status at the time of selecting the first-line therapy.
The present study has some limitations, such as the relatively small sample size of 202, the brief study period of 5 months, the retrospective study design, and the descriptive nature of the findings. The timing of the study was another limitation as ROS1 was not widely performed at the time the patients were diagnosed and first treated. Furthermore, reimbursement for ROS1 testing became available in Japan on 1 June 2017, and this may have contributed to the low ROS1 testing rate in the present study. Another limitation related to the timing of the study is that the present findings may become less relevant as new approaches, such as multiplex testing and NGS, become more widely used. In addition, this study has limited generalizability in terms of extrapolating the results to the wider Japanese population because the investigational sites were specialized centers and the results may not reflect the approaches to biomarker testing at nonspecialist centers. Finally, as this study focused on the proportion of patients for whom first-line treatment was selected based on biomarker testing results, we did not collect treatment efficacy outcome data.
In conclusion, compared with other biomarkers [ALK (88.1%), PD-L1 (87.1%), and ROS1 (67.3%)], the highest testing rate was that for EGFR (97.5%). As a result, the proportion of nonsquamous NSCLC patients with confirmed biomarker status for first-line treatment decision was 79.7%. We consider that this proportion is still insufficient and in need of improvement. To increase the proportion of NSCLC patients with confirmed biomarker status, it is important to conduct genetic testing, even to detect genetic mutations with a lower mutation rate. In addition, it is necessary to collect sufficiently large tumor specimens to conduct multiple biomarker tests. Furthermore, to clarify the optimal strategy of biomarker testing for NSCLC patients in real clinical practice, it is necessary that future studies apply recently developed biomarker testing methods, such as NGS.
Supplemental Material
20191125_BRAVE_Supplementary_Table_1 – Supplemental material for Biomarker testing for personalized, first-line therapy in advanced nonsquamous non-small cell lung cancer patients in the real world setting in Japan: a retrospective, multicenter, observational study (the BRAVE study)
Supplemental material, 20191125_BRAVE_Supplementary_Table_1 for Biomarker testing for personalized, first-line therapy in advanced nonsquamous non-small cell lung cancer patients in the real world setting in Japan: a retrospective, multicenter, observational study (the BRAVE study) by Junichi Shimizu, Katsuhiro Masago, Haruhiro Saito, Kazumi Nishino, Takayasu Kurata, Yohji Itoh, Yoko Yoshimura, Yutaka Yabuki and Hirotoshi Dosaka-Akita in Therapeutic Advances in Medical Oncology
Footnotes
Acknowledgements
The authors would like to thank the patients and their families, as well as the staff and investigators at all of the participating study sites. The authors would like to thank Michelle Belanger, of Edanz Medical Writing for providing medical writing services, which were funded by AstraZeneca through EMC K.K. in accordance with Good Publication Practice (GPP3) guidelines (![]() ).
).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and publication of this article: This study was sponsored by AstraZeneca.
Conflict of interest statement
K Nishino declares receiving personal fees from AstraZeneca, and, outside this work, personal fees from Chugai Pharmaceutical and Boehringer Ingelheim. T Kurata declares receiving a grant from AstraZeneca for study funding, and, outside this work, personal fees (honoraria) from AstraZeneca, MSD, Eli Lilly, Ono Pharmaceutical, Bristol, and MSD. Y Itoh, Y Yoshimura, and Y Yabuki are employees of AstraZeneca K.K. Outside this work, J Shimizu has received personal fees (speaker’s bureau fees) from AstraZeneca, Chugai Pharmaceutical, Ono Pharmaceutical, MSD, Taiho Pharmaceutical, and Novartis Pharma. Outside this work, H Saito has received grants from Chugai Pharmaceutical, AstraZeneca, and MSD, and personal fees from Ono Pharmaceutical, Nippon Boehringer Ingelheim, and Novartis Pharma. Outside this work, H Dosaka-Akita has received grants from Taiho Pharmaceutical Co., Ltd., Eli Lilly Japan K. K., and Ono Pharmaceutical Co., Ltd., and personal fees from AstraZeneca and Chugai Pharmaceutical Co., Ltd. K Masago declares no conflict of interest.
Supplementary material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.