
Abstract
Background:
Colorectal cancer is one of the five most common cancers in China, and its incidence is steadily increasing. An accurate and non-invasive screening method is needed to increase the population uptake of colorectal cancer screening. Secreted frizzled-related protein 2 (SFRP2) has been found to be hypermethylated in most colorectal cancer patients, and it may fulfill the role of a non-invasive biomarker for colorectal cancer screening.
Methods:
Methylation status of SFRP2 was examined in 17 cancer tissues and paired adjacent paracancer tissues by a new SFRP2 MethyLight assay, which was also used to test the serum of 62 patients with colorectal cancer and 55 normal individuals.
Results:
The limit of detection of the SFRP2 MethyLight assay was about 200 pg per reaction. The SFRP2 methylation level was higher in 94.1% colorectal cancer tissues than in paired adjacent paracancer tissues (P<0.001). The sensitivity and specificity of SFRP2 for detecting colorectal cancer in serum were 69.4% (95% confidence interval (CI) 56.2, 80.1%) and 87.3% (95% CI 74.9, 94.3%), respectively.
Conclusion:
SFRP2 methylation in serum has the potential to be a non-invasive biomarker for colorectal cancer screening.
Introduction
Worldwide, colorectal cancer (CRC) is the third most common cancer in men and the second in women, causing almost 1,360,000 cases per year. 1 In China, CRC also is one of the five most common cancers, and due to the changes in diet and a westernized lifestyle, its incidence is steadily increasing. 2 The 5-year relative survival rate of Chinese CRC patients increased from 47.2% to 56.9% during the past decade, but more than 8% survival gaps were still found between China and the developed countries.3,4
The CRC screening guideline in China recommends that people aged between 40 and 74 years old be screened with Guaiac-based fecal occult blood test (gFOBT) and followed up with a digital rectal exam and colonoscopy. 1 However, the program has had significant difficulty in reaching the entire population, and screening uptake in China is very low. The national registry used to track clinical outcomes is estimated to capture only 13% of the country’s population. 1 Although colonoscopy is the gold standard for CRC screening, its compliance in the screening setting is low due to its invasiveness and bowel preparation. 5 Meanwhile, the colonoscopy procedure highly depends on local medical resources. It is hardly a primary CRC screening method in developing countries or regions with limited resources. gFOBT is the most widely used CRC screening method in China, but its accuracy is low. 6 Hence, a more accurate and non-invasive screening method is needed to increase the uptake of early CRC screening.
In recent years, several studies reported the application of DNA methylation biomarkers in CRC diagnosis and screening.5,7,8 Among them, secreted frizzled-related protein 2 (SFRP2) was found to be hypermethylated in most CRC patients, 9 such as in feces or blood samples,7,10 indicating that SFRP2 may serve as a potential non-invasive biomarker for CRC screening. In this study, we used a newly developed quantitative methylation specific polymerase chain reaction (PCR), quantitative methylation-specific PCR-based assay—SFRP2 MethyLight assay—to detect methylated SFRP2 in serum samples from CRC patients, to evaluate the application feasibility of this assay as a non-invasive screening tool for CRC.
Materials and Methods
Sample collection
Fresh-frozen cancer tissues (n = 17) and paired adjacent paracancer tissues (n = 17) from CRC patients were collected at the time of radical surgery for CRC at the Affiliated Hospital of Xuzhou Medical University. Serum specimens were collected from 62 CRC patients and 7 advanced adenoma (AA) patients (histologically confirmed by a pathologist) who were undergoing colonoscopy at the Affiliated Hospital of Xuzhou Medical University (Table 1). AA was defined as adenomas with high-grade dysplasia or with ⩾25% villous histologic features or measuring ⩾1 cm in the greatest dimension. Control serum specimens were collected from 55 subjects without apparent digestive tract diseases (normal individuals). Blood (2 mL) was drawn from each subject and stored at 4℃ for up to 30 minutes. The serum fractions were then separated by centrifugation at 600 g for 15 minutes, and 1 mL serum samples were immediately frozen at −80℃ until used. The study was approved by the Institutional Review Board of the Affiliated Hospital of Xuzhou Medical University, and informed consent was obtained from all participating patients and healthy control subjects.
Characteristics of patients examined by SFRP2 MethyLight assay.
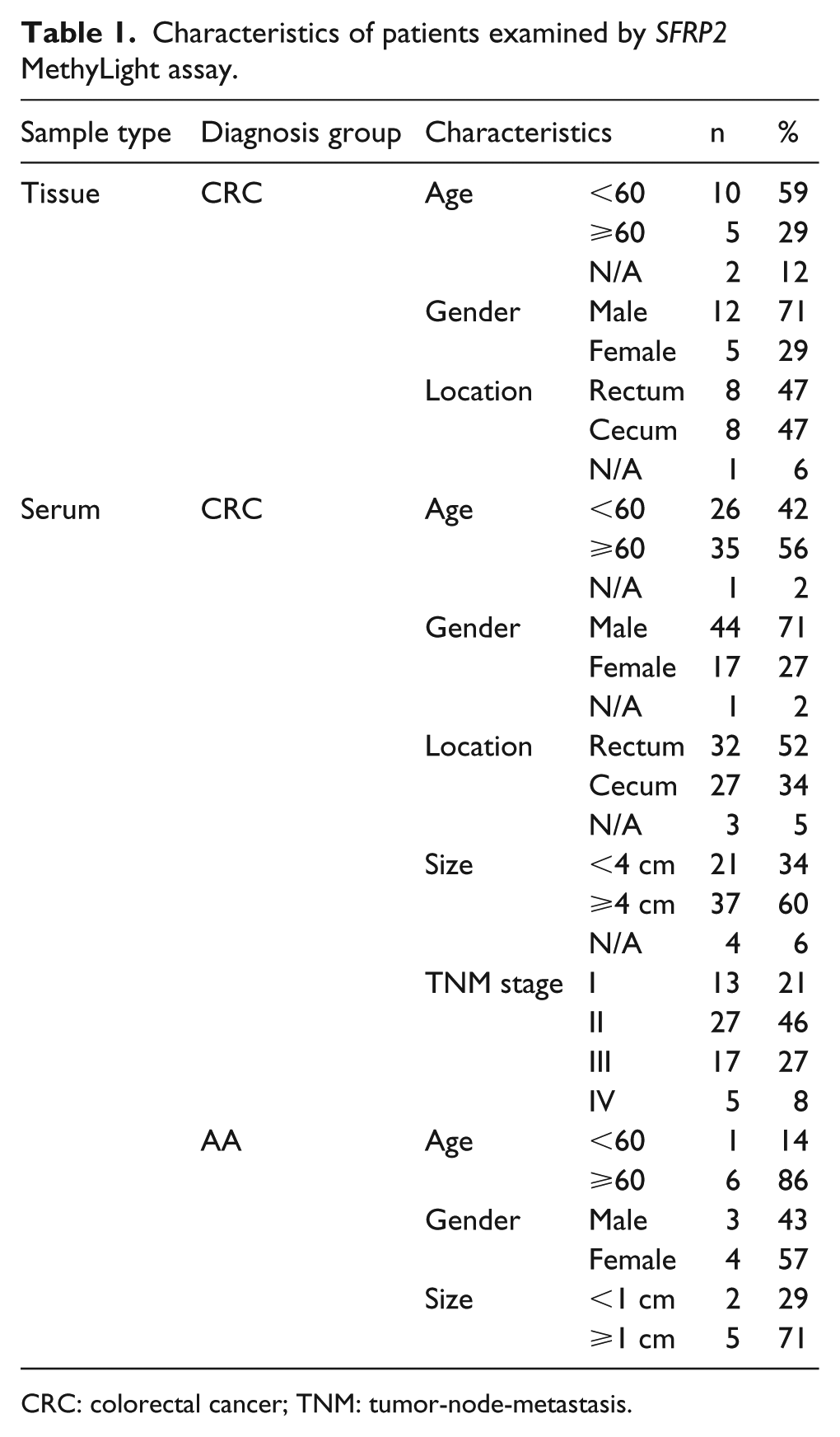
CRC: colorectal cancer; TNM: tumor-node-metastasis.
DNA extraction, bisulfite treatment, and quantitative real-time PCR
Genomic DNA was isolated from tissue specimens using a DNA mini kit (Qiagen, Hilden, Germany) and eluted in 100 μL elution buffer. Serum DNA was extracted using a cfDNA extraction kit (VersaBio Technologies Co. Ltd., Kunshan, Jiangsu, China) from 0.5 mL samples and eluted in a 100 μL elution buffer. Subsequently, 10 μL tissue genomic DNA and 100 μL serum cfDNA were used for bisulfite conversion, purified DNA was eluted in 100 μL and 30 μL of elution buffer, respectively. DNA bisulfite conversion and purification of the converted product was performed with a bisulfite conversion kit (VersaBio Technologies Co. Ltd.). All the kits were used according to the manufacturers’ instructions. The SFRP2 methylation level was determined by a MethyLight assay, where methylated SFRP2 and beta-actin (ACTB) reactions were performed as a duplex reaction. The total volume of the quantitative PCR (qPCR) was 30 μL using 15 μL DNA and 15 μL PCR Mastermix. Real-time PCR was performed on the LC480-II thermal cycler (Roche Diagnostics) using the following cycling conditions: activation at 95°C for 30 minutes, 50 cycles of 95°C for 10 seconds, 56°C for 30 seconds, and final cooling to 40°C for 30 seconds.
Analytical performance of SFRP2 MethyLight assay
To evaluate the analytical performance of SFRP2 MethyLight assay, replicate PCR reactions were performed with serially diluted DNA as templates. To examine the limit of detection (LoD) of SFRP2 MethyLight assay for detecting methylated SFRP2 DNA, different amounts of fully methylated genomic DNA were diluted into unmethylated genomic DNA to create mixtures. SFRP2 MethyLight assays were performed in 24 replicates at each DNA concentration.
Data analysis
∆Cp was used to determine the methylation status of SFRP2; ∆Cp was defined as the difference between the Cp values for the target (SFRP2) and the internal control gene (ACTB). Serum specimens were “not detected” if the SFRP2 Cp was not measurable or was ⩾ 41.0 cycles and the ACTB Cp was ⩾ 36.0 cycles. Data were subjected to statistical analysis by using IBM SPSS for Windows Version 22.0, and the t-test was used for comparison between two samples at the significant level of P<0.01. Data from sensitivity and specificity were used to plot the receiver operating characteristic (ROC) curve. Because most Cp values from normal individuals were not detected in the qPCR reaction, we had to set the Cp values to 50 (the maximal number of PCR cycles) for those not detected samples, to plot the curve. 11
Results
The analytical performance of the SFRP2 MethyLight assay
To evaluate the analytical performance of the SFRP2 MethyLight assay, mixtures of different ratios of bisulfite-treated genomic DNA were each tested for 24 replicates. As shown in Table 2, SFRP2 MethyLight assay could detect as low as 12.5pg fully methylated genomic DNA (~ 3.8 copies of human genome), and no SFRP2 signal was detected in the negative control. For the analytical sensitivity of the assay, LoD was defined as the target concentration that produces positive results in more than 95% of the replicate experiments. 12 As such, the LoD of SFRP2 MethyLight assay was about 200 pg (~ 60 copies of human genome) per PCR reaction, which means that each PCR reaction contained 200 pg genomic DNA as a template.
The analytical performance of SFRP2 MethyLight assay.
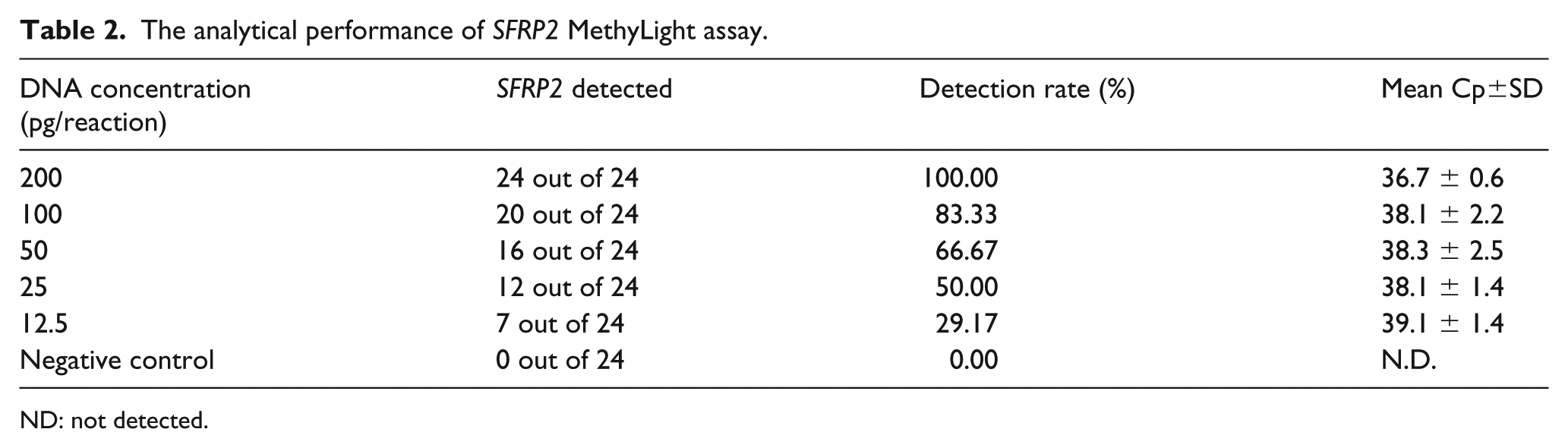
ND: not detected.
Methylation levels of the SFRP2 gene in CRC tissues
SFRP2 MethyLight assay was used to quantify methylation levels of SFRP2 gene in 17 CRC tissues. The ROC curve was constructed to evaluate the performance of this assay for detecting CRC. The SFRP2 methylation levels were higher in 94.1% (16/17) of cancer tissues than in their paired adjacent paracancer tissues (P < 0.001, Figure 1(a)), and the area under the ROC curve was 0.95 (95% confidence interval (CI) 0.86, 1.00, Figure 1(b)) for cancer when compared to paired adjacent paracancer tissues.
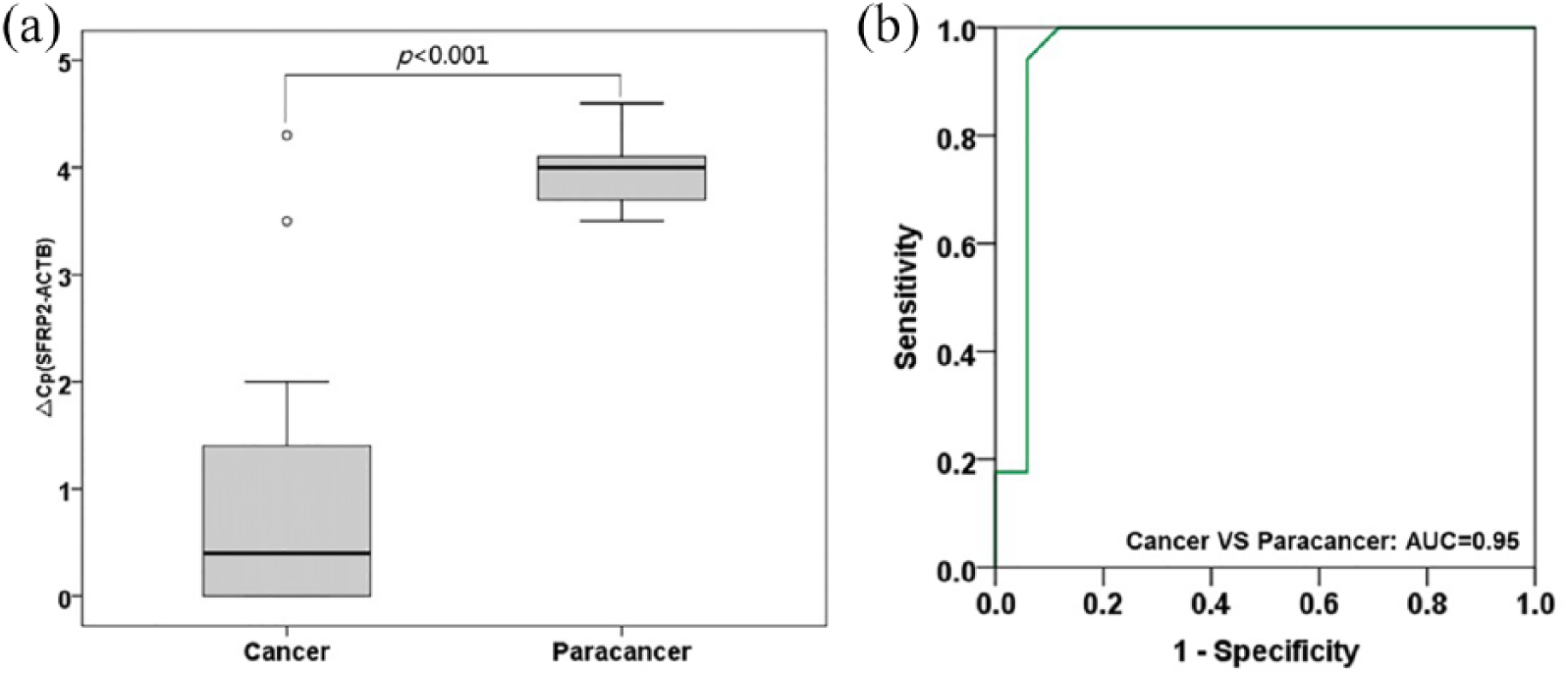
SFRP2 methylation in tissue samples. (a) Methylation levels of the SFRP2 gene in colorectal cancer tissues and paracancer tissues assessed by SFRP2 MethyLight assay. (b) ROC curve for SFRP2 methylation levels in colorectal cancer versus paracancer tissues. ∆Cp was defined as the difference between the Cp values for the target (SFRP2) and the internal control gene (ACTB). ROC: receiver operating characteristic.
Methylation levels of the SFRP2 gene in CRC serum
The positive detection rate for each stage is shown in Figure 2(a), the overall sensitivity for CRC and AA were 69.4% (95% CI 56.2, 80.1%) and 42.9% (95% CI 11.8, 79.8%) with a specificity of 87.3% (95% CI 74.9, 94.3%) for CRC and AA. Sensitivities for different stages of CRC were 46.2% for stage I (6/13), 74.1% for stage II (20/27), 70.6 % for stage III (12/17), and 100% for stage IV (5/5) (Figure 1 (a)). The ROC curve for SFRP2 MethyLight assay detecting CRC in serum is shown in Figure 2(b), and the area under the curve (AUC) was 0.821 (95% CI 0.744, 0.898) indicating a good performance in distinguishing the CRC subjects from normal subjects. Furthermore, there was no significant difference in the positive rates of SFRP2 between different genders, the location, or the size of the tumors (Table 3). Although there is a significant difference in the detection rate of colorectal cancer at different ages (P < 0.05), this may be due to the bias caused by insufficient sample size.
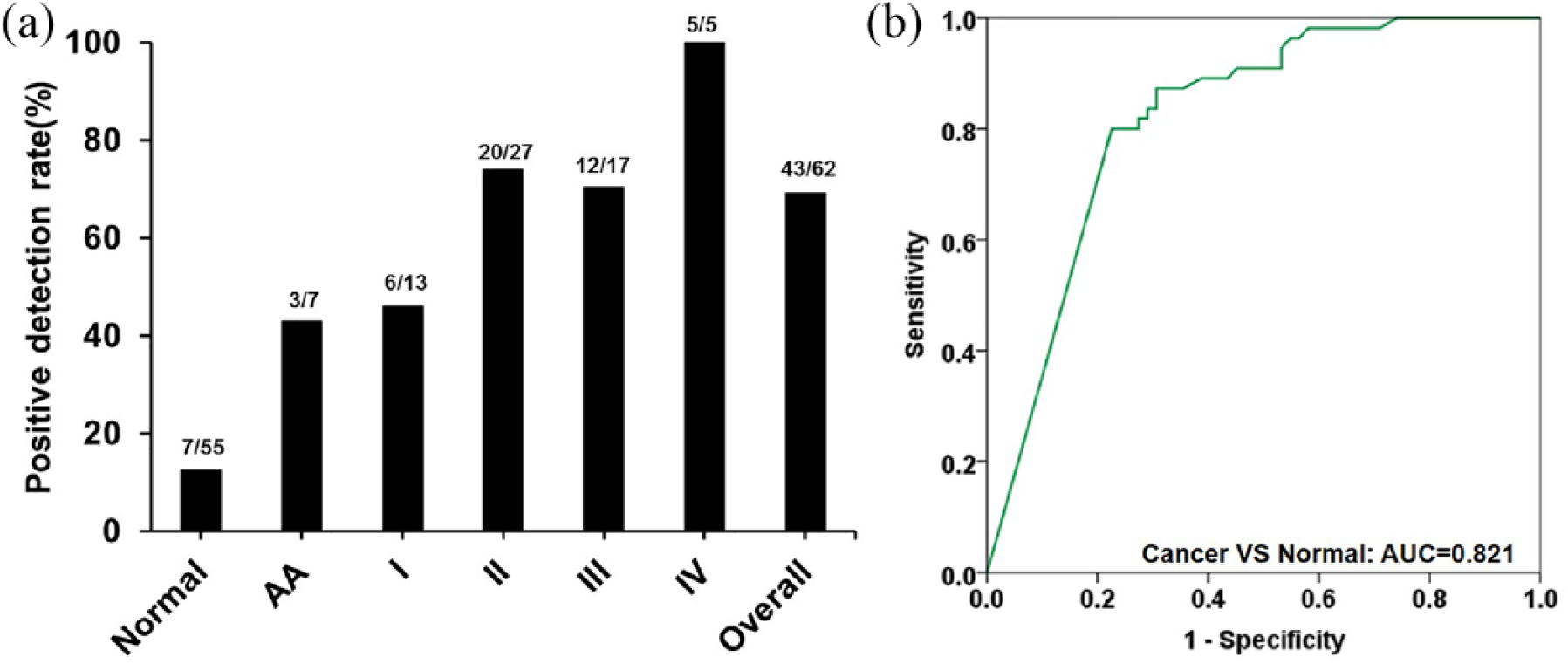
Sensitivity of SFRP2 MethyLight assay in detecting colorectal cancer across stages I–IV. (a) Positive detection rates for normal, AA, and all stages of colorectal cancer. (b) ROC curve for the SFRP2 MethyLight assay in detecting colorectal cancer. AA: advanced adenoma; ROC: receiver operating characteristic.
Results of methylated SFRP2 in identifying CRC between different ages, genders, and tumor locations.
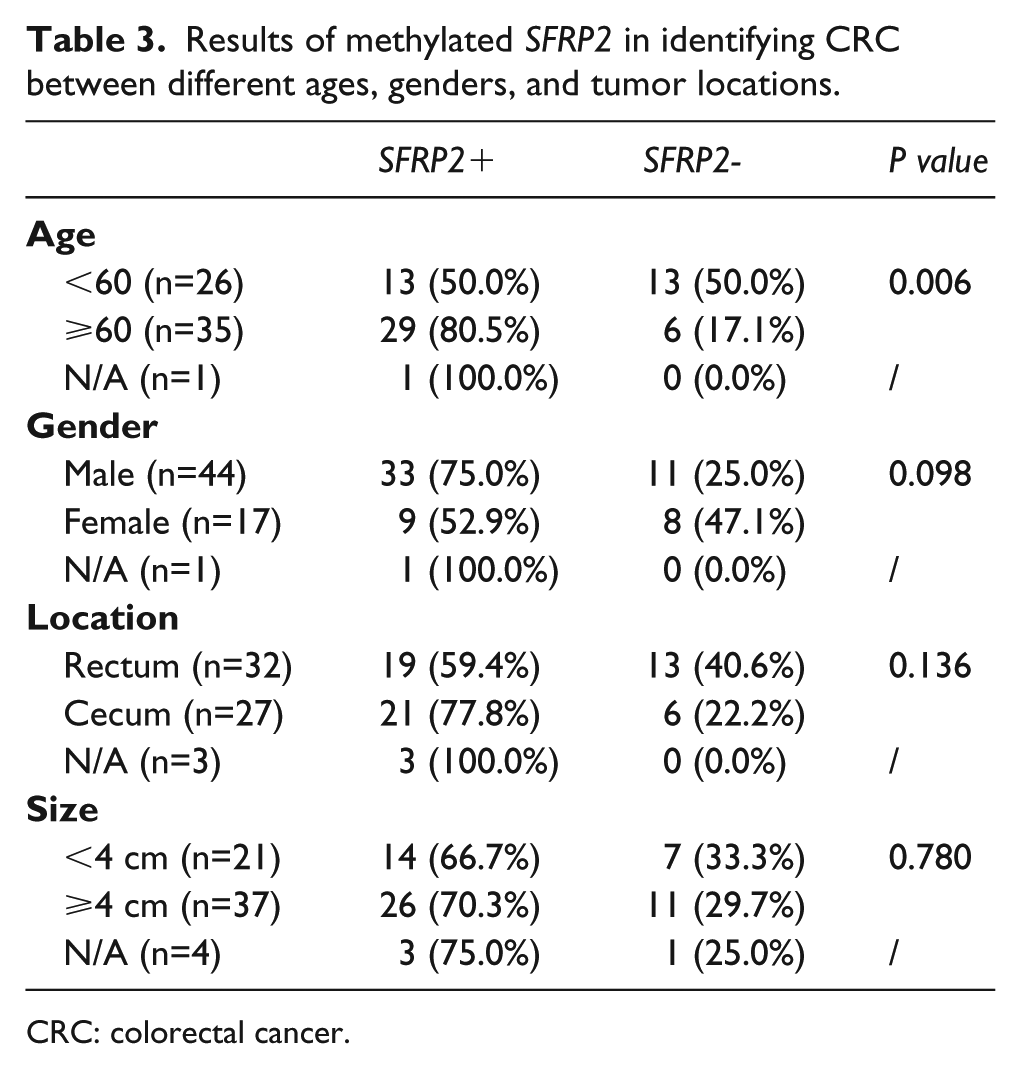
CRC: colorectal cancer.
Discussions
SFRP2 is one member of the SFRP gene family participating in Wingless/Wnt signaling pathway. 13 The genes play an important role in cell growth, apoptosis, and regulation of cell differentiation. It is often methylated in human cancers, such as prostate, 14 hepatocellular, 15 and CRC.13,14 Its down-regulation is closely related to Wnt signaling activity and tumor progression. 16 SFRP2 methylation has been studied extensively in CRC and is suggested as a non-invasive biomarker for CRC screening. Tang et al. 17 examined the performance of methylated SFRP2 for detecting CRC in 0.2 mL serum by an agarose gel-based MSP approach. The assay sensitivity was 66.9% for CRC, 6.4% for adenomas, and the specificity was 98.7%. Using a similar approach with 0.2 mL of input plasma, Zhang et al. 18 showed that SFRP2 was methylated in 54.4% of CRC, and 40.0% of adenomas, with a specificity of 72.4%. Switching to a nested PCR-based SFRP2 qMSP assay with 3.5 mL plasma as the starting material, Barták later reported that the sensitivity of SFRP2 methylation was 72.3% and 83.8% for detecting CRC and colorectal adenoma, respectively, and the specificity was 97.3%.7
In the present study, SFRP2 was shown to be heavily methylated in CRC tissues when compared to paired paracancer tissues (P<0.001). Serum SFRP2 methylation showed 69.4% sensitivity for detecting CRC and 42.9% for AA with an 87.3% specificity in distinguishing CRC subjects from normal subjects, thus demonstrating similar sensitivity and specificity to those reported in previous studies. However, as a one-step qMSP assay is much easier to perform, the SFRP2 MethyLight assay has a clear advantage over agarose gel-based MSP17,18 and nested PCR-based qMSP 7 assays.
The SFRP2 MethyLight assay is non-invasive, is easier for the patients to comply with, and is easier for doctors to perform than a colonoscopy. In recent years, other non-invasive methods, such as stool DNA (CologuardTM) and methylated SEPT9 (Epi proColon 2.0) tests, have been approved by the US Food and Drug Administration for CRC screening.7,19 However, with the high price ($603 per test) and cumbersome procedure of CologuardTM, 5 it is not suitable for developing countries, such as China. While SEPT9 methylation showed similar sensitivity (68.2~80.6%) and specificity (80~99.3%) for CRC20,21 to SFRP2 MethyLight assay, its sensitivity for detecting AA was only about 20%. 22 Most CRC develop from adenomas, among which AA are considered to be the clinically relevant precursors of CRC. 23 Therefore, the screening and intervention for AA has been considered as a primary strategy for the prevention and early screening of CRC. 24 In the present study, the 42.9% sensitivity of SFRP2 methylation for AA detection was comparable to that of CologuardTM, 19 indicating that serum SFRP2 methylation could be a viable biomarker for detecting precursor lesions. The Epi proColon 2.0 test uses 3.5 mL plasma and is performed as triplicate qPCR reactions. Its sensitivity for CRC detection could be improved by using a large sample volume or when an SEPT9 result was considered positive if the results of at least one out of three replicate reactions were positive. 25 In contrast, SFRP2 MethyLight assay only used 0.5 mL serum and was performed as a single qPCR reaction. Therefore, its sensitivity for CRC detection also may be improved by increasing the input sample volumes and performing more replicate experiments per sample.
Conclusion
We developed a new MethyLight assay for detecting methylated SFRP2 in serum. Its sensitivity and specificity for CRC detection were 69.4% and 87.3%, respectively. Therefore, with further optimization, SFRP2 MethyLight assay may become a valuable tool for the non-invasive detection of colorectal neoplasms and precursor lesions.
Footnotes
Authors’ contributions
HL, ZW and GZ performed the statistical analyses, drafted the manuscript, and contributed equally to this work. MZ, YM, YC, and QX participated in data analysis. HL, ZW, GZ, MZ, and SF conceived of the study and participated in the design and coordination of the study. All authors read and approved the final manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by “Hundred Talents Program” of Chinese Academy of Sciences (Grant No. Y521051102), Key Technologies R & D Program for Social Development of Jiangsu Province (Grant No. BE2016685) and Suzhou Leading Talent Project (Grant No. ZXL2014128).