
Abstract
Although many previous studies have reported the relationship between GSTP1 rs1695 gene polymorphism and myelosuppression induced by platinum-based drugs, the conclusions are not consistent. The aim of the study is to evaluate the association between granulocytopenia and thrombocytopenia induced by platinum-based drugs and GSTP1 rs1695 gene polymorphism by meta-analysis. A literature search was performed using the Pubmed, Embase, CNKI, and Wanfang databases, and the odds ratio (OR) and its 95% confidence interval (CI) were used to evaluate the correlation. Finally,12 case-control studies comprising 1657 patients were included in our study. GSTP1 rs1695 gene polymorphism showed a significant correlation with granulocytopenia induced by platinum-based drugs (dominant genetic model: OR=1.60, 95% CI=1.19. 2.15, P=0.002; recessive genetic model: OR=3.72, 95% CI=1.73, 8.00, P=0.001; allelic genetic model: OR=1.76, 95% CI=1.34, 2.33, P=0.001). This gene polymorphism is not associated with thrombocytopenia (OR=0.87, 95% CI=0.47, 1.60, P=0.649). False-positive report probability showed that the association between polymorphism and adverse reactions is true. Sensitivity analysis showed that the results were stable. However, there was a certain publication bias in the included studies. In conclusion, the GSTP1 rs1695 gene polymorphism is associated with granulocytopenia induced by platinum-based drugs.
Introduction
Malignant tumors are the leading cause of deaths globally. In 2018, 1.7 million people in the US are expected to die of cancer. 1 Platinum-based drugs are the mainstay treatment for malignant tumors such as lung cancer and breast cancer. Myelosuppression includes granulocytopenia, thrombocytopenia, and anemia are the commonly seen adverse reactions associated with platinum-based drugs. According to statistics, the incidence of Grade 3–4 myelosuppression in patients receiving sufficient doses of cisplatin is around 20%. Although there are prophylactic methods, such as the use of colony-stimulating factors, myelosuppression often results in a failure to complete chemotherapy on time and reduces the efficacy of drugs. 2
In recent years, increasing numbers of pharmacokinetic studies have been performed to identify populations with a high incidence of chemotherapy-related adverse reactions. 3 For example, UGT1A1 gene polymorphism is widely used in predicting irinotecan-induced diarrhea. 4 Variations in drug target genes or gene polymorphisms in DNA repair enzymes and metabolic or detoxification pathways may affect myelosuppression induced by platinum-based drugs. Studies have shown that many gene polymorphisms are associated with the occurrence of myelosuppression induced by platinum-based drugs such as ERCC1/2, 5 XRCC3, 6 XRCC1, and DYPD. 7 To date, in-depth research on the relationship between GSTP1 rs1695 gene polymorphism and myelosuppression induced by platinum-based drugs have been performed.
Glutathione-S-transferase (GST) is a phase II enzyme and a superfamily containing many isoenzymes. These enzymes can catalyze the binding of cisplatin and other polar compounds to glutathione (GSH) to be converted into water-soluble substances that are excreted through urine or bile. 8 In humans, GST can be classified into eight classes, including α, μ, π, and θ, 9 according to the different encoded proteins. GST-π is encoded by GSTP1 and an immunoblot analysis revealed that GST-π is widely distributed throughout the body.
The GSTP1 gene is located on chromosome 11q13 and exhibits polymorphisms. An A/G single nucleotide mutation at rs1695 results in an amino acid substitution from isoleucine to valine (p.rs1695). This results in decreased substrate specificity, catalytic activity, and thermal stability in the encoded GSTP1 protein. 10 In the last 20 years, a large number of studies have investigated the relationship between GSTP1 rs1695 gene polymorphism and myelosuppression induced by platinum-based drugs (granulocytopenia, thrombocytopenia).11-22 However, the small sample sizes of these studies resulted in inconsistent conclusions. Therefore, we performed a meta-analysis on the relationship between GSTP1 rs1695 gene polymorphism and myelosuppression induced by platinum-based drugs to provide a new basis for predicting adverse drug reactions.
Materials and methods
Search strategy and inclusion/exclusion criteria
A literature search was performed using English databases (Pubmed and Embase) and Chinese databases (CNKI and Wanfang) from inception until January 31, 2018. The following search string was employed to search the Pubmed database: (myelosuppression OR leucopenia OR thrombocytopenia) AND (cisplatin OR oxaliplatin OR carboplatin) AND (GSTP1 OR rs1695 OR Ile105Val). In addition, a manual search of references in relevant review papers and included studies was carried out to supplement the data.
The primary inclusion criteria were: (a) study type: case-control studies; (b) study subjects: cancer patients undergoing treatment with platinum-based drugs; (c) exposure factors: GSTP1 rs1695 gene polymorphism; (d) outcome markers: myelosuppression (including granulocytopenia and thrombocytopenia) induced by platinum-based drugs (such as cisplatin, carboplatin, and oxaliplatin); and (e) studies providing different genotypes or number of patients who experienced myelosuppression.
The primary exclusion criteria were: (a) papers that were republished; and (b) papers in which the entire manuscript was unobtainable or data could not be extracted.
According to clinical correlation, the outcome marker was Grade 3 and above granulocytopenia or Grade 1 and above thrombocytopenia as defined by NCI-CTCAE. (Grade 3 and above granulocytopenia was defined as white blood cell count <2*109/L or neutrophil count <1*109/L. Thrombocytopenia was defined as platelet count <80*1012/L or the use of colony-stimulating factors.)
Data extraction
Two researchers (Lv and Song) were independently responsible for literature search and data extraction according to the aforementioned criteria. Discussions were carried out in ambiguous cases until a consensus was reached. The following data were extracted from the papers: first author, year of publication, race (Asian, non-Asian), study design, polymorphism detection method, sample size, type of tumor, chemotherapy regimen, and genotype frequency.
Quality assessment
This study employed the Newcastle–Ottawa Scale (NOS) 23 to assess study quality. The NOS quality assessment scale contains three parts: selection of study subjects (0–4 points), inter-group comparability (0–2 points), and evaluation of exposure or outcomes (0–3 points). A paper which scores 6 points and above is considered to have high study quality.
Statistical analysis
This study employed dominant, recessive, and allelic genetic models to evaluate the risk of myelosuppression. The Stata 11.0 software (StateCrop LP, College Station, TX, USA) was used for statistical analysis. The genotypes of the control group in the included studies were tested to see if they conform to Hardy–Weinberg equilibrium (HWE). Odds ratio (OR) and 95% confidence intervals (CI) were calculated from original data as effector markers. Heterogeneity in the results of the included studies was analyzed using X2 test (test level of α=0.1). This was combined with I2 quantitation to determine the degree of heterogeneity. If I2<50%, then statistical heterogeneity was acceptable (0<I2<25%: mild heterogeneity 25%<I2<50%: moderate heterogeneity). If the statistical heterogeneity between results of various studies was acceptable, a fixed effects model was used for the meta-analysis. If not, we further analyzed the source of heterogeneity. After eliminating the effects of significant clinical heterogeneity, a random effects model was then employed for the meta-analysis and a subgroup analysis was performed to investigate the source of heterogeneity.
The false-positive report probability (FPRP) was calculated for positive results to evaluate the true relationship between gene polymorphism and myelosuppression after chemotherapy.24,25 The FPRP was calculated from the P-value, a priori probability, and statistical power. We set the FPRP threshold to 0.2, the range of a priori probability to 0.25–0.01 and the statistical power based on computing power to detect OR=1.5.
Sensitivity analysis was employed to exclude the effects of individual studies on the total effects one by one for evaluating the stability of the results. A funnel plot and Egger’s method 26 were used to test for publication bias. All tests were two-tailed and a difference of P< 0.05 was considered statistically significant.
Results
Study characteristics
As shown in Figure 1, we initially screened 280 papers from Chinese and English databases. After screening layer by layer, 12 case-control studies comprising 1657 patients who fulfilled the inclusion criteria were selected. Among these papers, 10 were on granulocytopenia and included 1441 patients, while 4 papers were on thrombocytopenia and included 316 patients. The characteristics of the included studies are shown in Table 1. The sample size of these studies ranged from 40 to 600. The types of tumors in the studies included non-small cell lung cancer (NSCLC), gastric cancer, ovarian cancer, and bladder cancer. The drugs that were used in combination with platinum-based drugs included paclitaxel, epirubicin, and 5-fluorouracil.
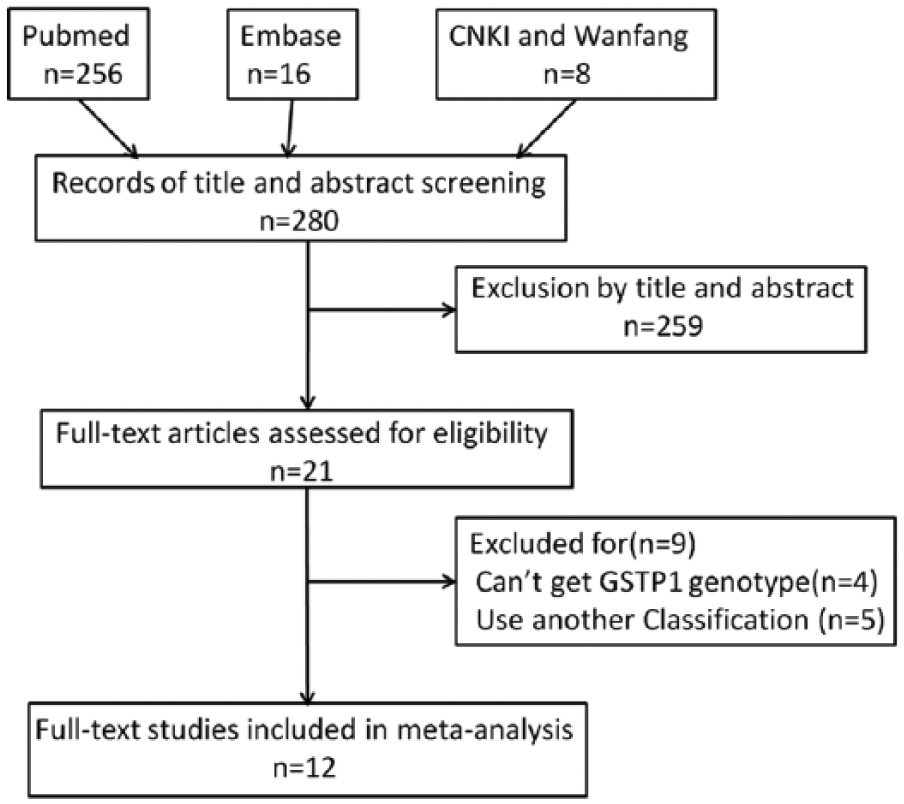
Flow chart of literature search and selection progress.
Characteristics of studies included in meta-analysis.
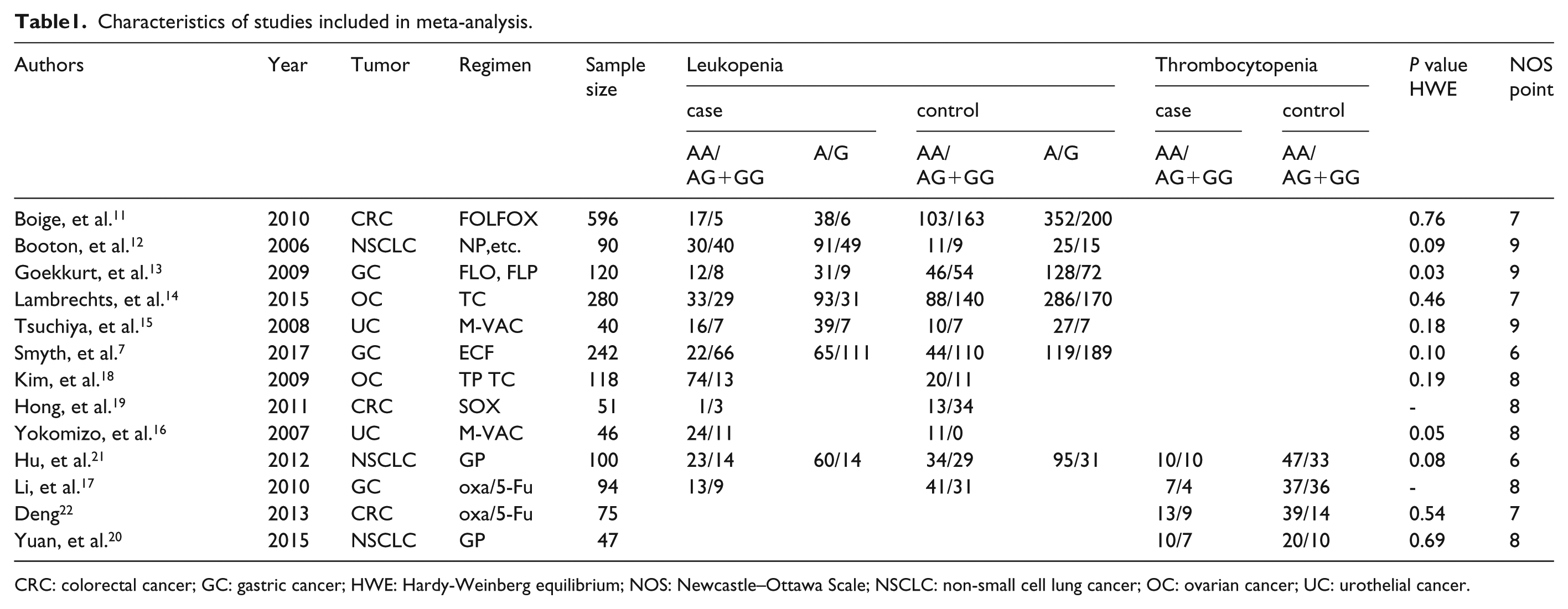
CRC: colorectal cancer; GC: gastric cancer; HWE: Hardy-Weinberg equilibrium; NOS: Newcastle–Ottawa Scale; NSCLC: non-small cell lung cancer; OC: ovarian cancer; UC: urothelial cancer.
Quality assessment
As shown in Table 1, we employed the NOS to evaluate study quality according to the year of publication, race, study design, sample size, tumor type, chemotherapy regimen, and others.
GSTP1 rs1695 gene polymorphism and granulocytopenia after chemotherapy
Ten papers reported data on the correlation between GSTP1 dominant genetic models and myelosuppression after chemotherapy, six papers reported correlation data between GSTP1 recessive and allelic genetic models and myelosuppression after chemotherapy. The heterogeneity test results showed that moderate statistical heterogeneity exists between the results of the included studies in various models (dominant genetic model: P=0.074, I2=42.6%; recessive genetic model: P=0.461, I2=0.0%; allelic genetic model: P=0.461, I2=0.0%) and the heterogeneity was acceptable. A fixed effects model was used for the meta-analysis. Results showed that a correlation exists between GSTP1 rs1695 gene polymorphism and granulocytopenia after chemotherapy in dominant, recessive, and allelic genetic models (dominant genetic model: OR=1.60, 95% CI=1.19, 2.15, P=0.002, Figure 2; recessive genetic model: OR=3.72, 95% CI=1.73, 8.00, P=0.001, Supplementary Material 1; allelic genetic model: OR=1.76, 95% CI=1.34, 2.33, P=0.001, Supplementary Material 2).
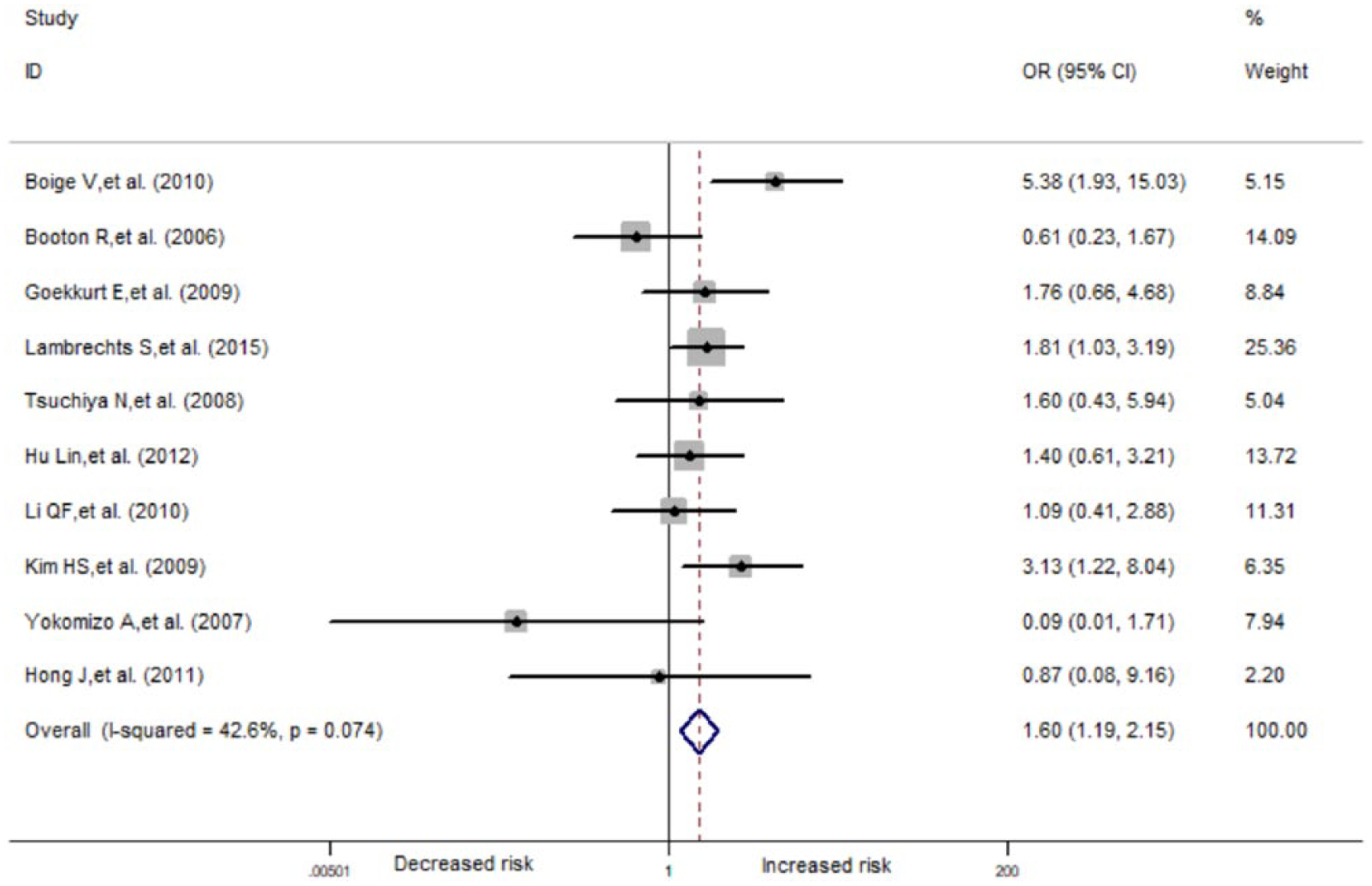
Forest plots of leukopenia associated with GSTP1 Ile105Val polymorphism (dominant model).
GSTP1 rs1695 gene polymorphism and thrombocytopenia after chemotherapy
Four papers reported data on the correlation between GSTP1 dominant genetic models and thrombocytopenia after chemotherapy. Heterogeneity test results showed that there was no statistical heterogeneity in the results of the included studies (P=0.718; I2=0.0%). A fixed effects model was used for the meta-analysis, and the results showed that there was no correlation between GSTP1 rs1695 gene polymorphism and thrombocytopenia after chemotherapy in a dominant genetic model (OR=0.87; 95% CI=0.47, 1.60; P=0.649; Figure 3).
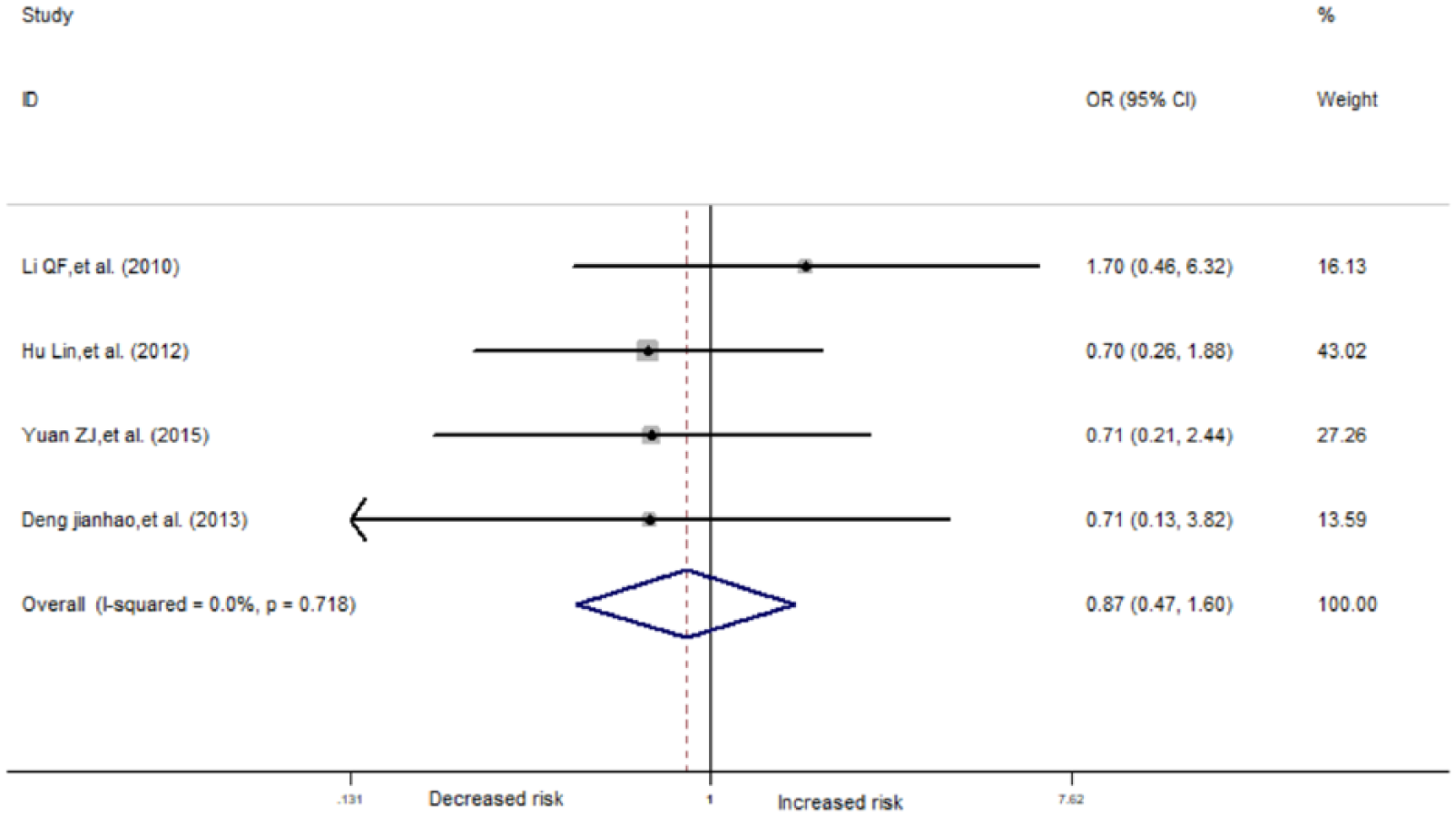
Forest plots of thrombocytopenia associated with GSTP1 Ile105Val polymorphism (dominant model).
False-positive report probability
A false-positive relationship between GSTP1 rs1695 gene polymorphism and granulocytopenia after chemotherapy may result in mixed effects. Therefore, FPRP was used to evaluate this effect, and the results are shown in Table 2. In the three positive correlation models, the FPRP value was lower than the predetermined value of 0.2. Therefore, it can be determined that a true relationship exists between GSTP1 rs1695 gene polymorphism and granulocytopenia after chemotherapy.
FPRP values of SNPs associated with leukopenia.
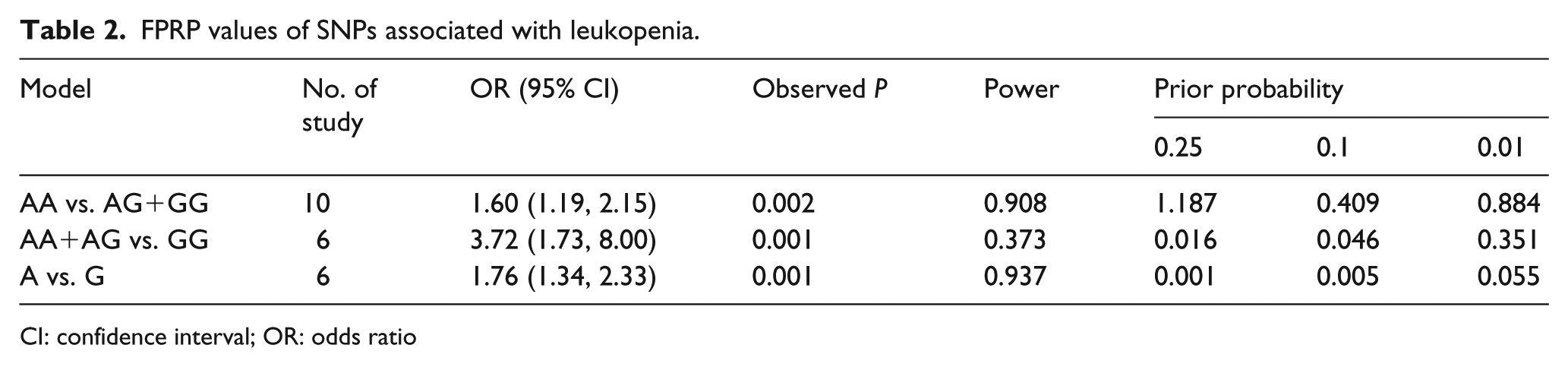
CI: confidence interval; OR: odds ratio
Sensitivity analysis and publication bias
One study that did not conform to HWE was excluded, 13 and the meta-analysis was repeated. Results showed that there were no significant changes in the combined effects between GSTP1 rs1695 gene polymorphism and granulocytopenia in the three models (data not shown). This shows that our meta-analysis results are stable (Figure 4, Supplementary Material 3 and 4).
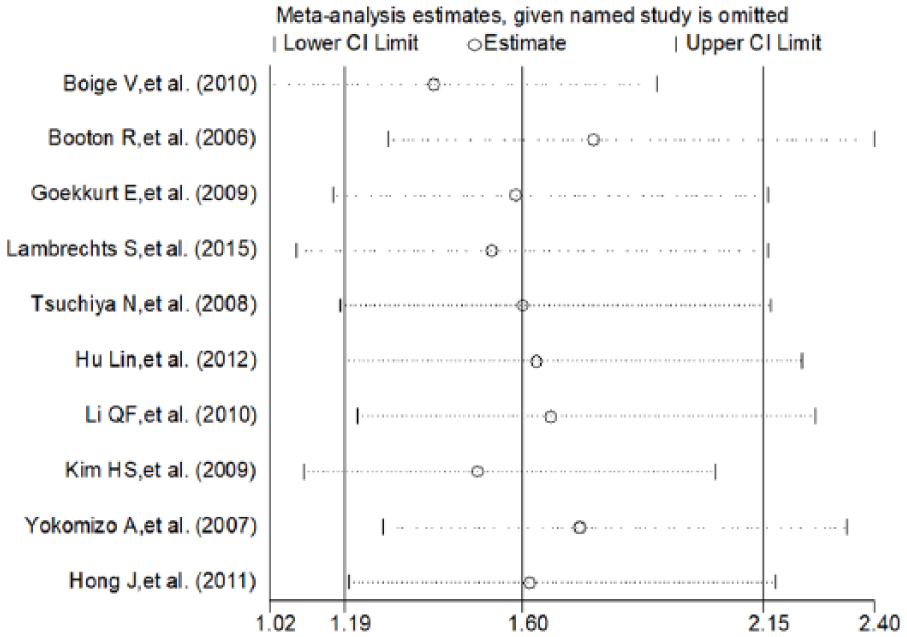
Sensitivity analysis by excluding any single study (dominant model).
Funnel plot and Egger’s plot were used to evaluate publication bias. Results showed that bias is not statistically significant (P>0.05, Figure 5, Supplementary Material 5).
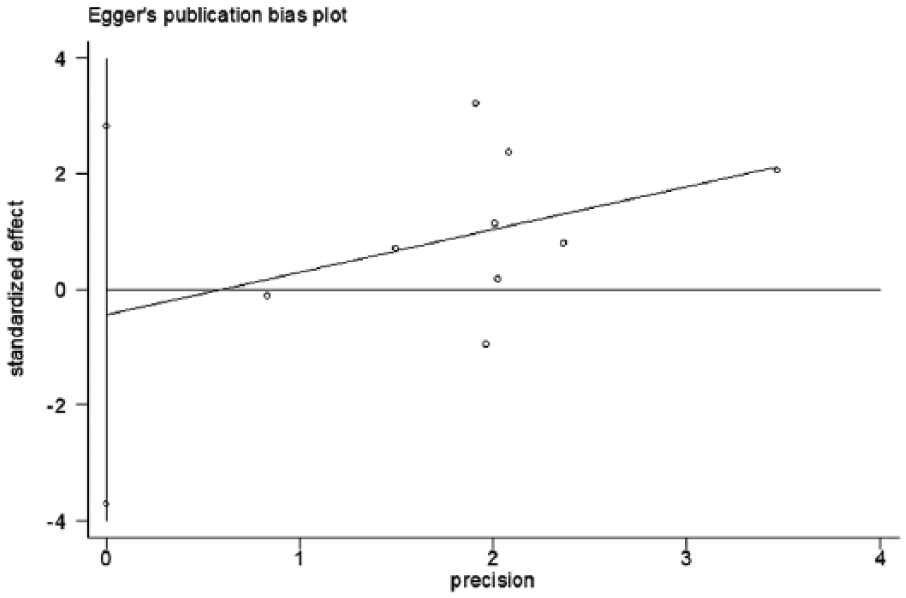
Egger plots to detect potential publication biases.
Discussion
Platinum-based chemotherapy drugs, including first-generation drugs cisplatin and carboplatin, and the third-generation drug oxaliplatin, are commonly used for many solid tumors. Myelosuppression induced by platinum-based drugs not only delays treatment and affects therapeutic efficacy, but also can cause serious complications and pose a threat to the life of patients. Therefore, there is an urgent need to identify biomarkers that can predict myelosuppression associated with platinum-based drugs and other adverse reactions. Single nucleotide polymorphisms (SNPs) refer to the insertion, loss, or substitution of single nucleotide bases in a genetic sequence, resulting in polymorphism in the nucleotide sequence. Many studies have examined the relationship between GSTP1 rs1695 gene polymorphism and adverse reactions after chemotherapy with platinum-based drugs. A study by Carron et al. 27 on 88 head and neck squamous cell carcinoma patients receiving concomitant radiochemotherapy with cisplatin found that the probability of moderate or severe vomiting is higher in patients with the GSTP1 AA/AG genotype. In addition, another study showed that polymorphism at this locus is associated with cisplatin ototoxicity in children. 28 A previous meta-analysis investigated the relationship between GSTP1 rs1695 gene polymorphism and oxaliplatin-induced peripheral neuropathy, 29 and the results showed that polymorphism at this locus was not associated with peripheral neuropathy. In recent years, many studies on the relationship between GSTP1 rs1695 gene polymorphism and myelosuppression induced by platinum-based drugs have been performed. However, the conclusions were not consistent. Small sample size and poor test power are the possible reasons for the inconsistency in results. Therefore, there is a need to employ a meta-analysis to expand the sample size.
To the best of our knowledge, our study is the first meta-analysis on the relationship between GSTP1 rs1695 gene polymorphism and myelosuppression induced by platinum-based drugs. Our study included 12 case-control studies containing 1657 patients with cancer who received a regimen containing platinum-based drugs. Results showed that GSTP1 rs1695 gene polymorphism showed a significant correlation with granulocytopenia after chemotherapy under the dominant, recessive, and allelic genetic models. However, there was no correlation between GSTP1 rs1695 gene polymorphism and thrombocytopenia after chemotherapy. We employed FPRP to exclude interference from false positives on the authenticity of the relationship. Sensitivity analysis showed that our study results were stable and reliable, while Egger’s method showed that there was some publication bias in the included studies.
GSTP1 is the most important detoxification enzyme in the body. GSTP1 105 Ile is located in the active site. Gene polymorphisms will result in amino acid mutants, which in turn will lead to reduced GSTP1 stability, decreased catalytic activity, and reduced metabolism of platinum-based drugs. This may be one of the mechanisms by which GSTP1 rs1695 gene polymorphism affects adverse reactions caused by platinum-based drugs. The study by Ishimoto et al. 30 showed that GSTP1 A alleles decrease cytoprotection abilities. Watson et al. 31 showed that GSTP1 catalytic activity is decreased by approximately one-third in the GSTP1 GG genotype compared with the AA genotype (GG genotype: 52.5 mmol/ng min, AA genotype: 74.9 mmol/ng min). Besides substrate specificity for removal of toxic substances, GSTP1 can also regulate signaling pathways, such as the JNK pathway 32 and STAT3 pathway, 33 through non-substrate ligand methods. This affects processes such as cell proliferation and apoptosis. Further research is warranted to investigate whether GSTP1 polymorphism can affect adverse reactions through this pathway. However, it must be pointed out that the effects of SNP on adverse reactions after chemotherapy are dependent on complex genetic backgrounds. The synergistic effects of other genes and proteins will amplify or mask the effects produced by GSTP1 SNPs. Therefore, the conclusion of this study should be carefully evaluated.
The limitations of this study are: (a) The presence of a relatively large publication bias as some negative results were not published or some raw data on GSTP1 rs1695 gene polymorphism and myelosuppression in clinical studies were not listed; also, current literature usually reported only the results for genetic models with most significance. Therefore, the level of evidence may not be sufficient, and the results of this study should be carefully evaluated. The pooled analysis should have been a method of extensive research, but limited to the cost we failed to carry out. (b) The sample size of most included studies was less than 300, and there is still some gap in the requirements for genetic association studies. Of the 12 included studies, only 4 reported the relationship between gene polymorphism and thrombocytopenia. Differences in study design, tumor type, and concomitant drugs may have affected the study results. (c) Previous studies showed that age is also a factor affecting myelosuppression. 34 However, as the raw data did not provide relevant information, we were unable to determine the relationship between age, polymorphism, and myelosuppression according to age subgroups. (d) Myelosuppression induced by chemotherapy agents is a multifactorial, multi-effector, complex process. This study only considered the relationship between GSTP1 rs1695 gene polymorphism and myelosuppression and did not consider the relationship between genes and genes, and that between genes and environmental factors. We believe that a large sample, prospective study should be carried out to further improve the relationship between gene polymorphism and myelosuppression after chemotherapy.
In summary, there is a significant correlation between GSTP1 rs1695 gene polymorphism and myelosuppression induced by platinum-based drugs. Owing to the above limitations, the conclusion of this study requires further validation using high-quality experiments.
Supplemental Material
Supp.Mat.1 – Supplemental material for Relationship between GSTP1 rs1695 gene polymorphism and myelosuppression induced by platinum-based drugs: a meta-analysis
Supplemental material, Supp.Mat.1 for Relationship between GSTP1 rs1695 gene polymorphism and myelosuppression induced by platinum-based drugs: a meta-analysis by Fei Lv, Yanju Ma, Ye Zhang and Zhi Li in The International Journal of Biological Markers
Supplemental Material
Supp.Mat.2 – Supplemental material for Relationship between GSTP1 rs1695 gene polymorphism and myelosuppression induced by platinum-based drugs: a meta-analysis
Supplemental material, Supp.Mat.2 for Relationship between GSTP1 rs1695 gene polymorphism and myelosuppression induced by platinum-based drugs: a meta-analysis by Fei Lv, Yanju Ma, Ye Zhang and Zhi Li in The International Journal of Biological Markers
Supplemental Material
Supp.Mat.3 – Supplemental material for Relationship between GSTP1 rs1695 gene polymorphism and myelosuppression induced by platinum-based drugs: a meta-analysis
Supplemental material, Supp.Mat.3 for Relationship between GSTP1 rs1695 gene polymorphism and myelosuppression induced by platinum-based drugs: a meta-analysis by Fei Lv, Yanju Ma, Ye Zhang and Zhi Li in The International Journal of Biological Markers
Supplemental Material
Supp.Mat.4 – Supplemental material for Relationship between GSTP1 rs1695 gene polymorphism and myelosuppression induced by platinum-based drugs: a meta-analysis
Supplemental material, Supp.Mat.4 for Relationship between GSTP1 rs1695 gene polymorphism and myelosuppression induced by platinum-based drugs: a meta-analysis by Fei Lv, Yanju Ma, Ye Zhang and Zhi Li in The International Journal of Biological Markers
Footnotes
Acknowledgements
Thank you to Zhi Li and Ye Zhang for their statistical support, and thank you to Ma Yanju for his guidance in the writing of the thesis. I also sincerely thank Huicong Song for his support in data extraction.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Natural Science Foundation of China (No. 81270036, 30901736), the Plan to Focus on Research and Development from Science and Technology project of Liaoning Province (No. 2017225029), Science and Technology Plan Project of Shenyang City (No. 18-014-4-11), and Fund for Scientific Research of The First Hospital Of China Medical University (No. FHCMU- FSR).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.