
Abstract
Objectives:
Dihydrodiol dehydrogenase 2 (DDH2) plays an important role in pathogenesis of non-small-cell lung cancer (NSCLC). This study aimed to evaluate the value of serum DDH2 levels in NSCLC patients.
Methods:
Serum samples were obtained from 863 NSCLC patients and 439 healthy controls. The samples were randomly divided into a training set and a test set. Serum DDH2 levels were assayed by enzyme-linked immunosorbent assay (ELISA).
Results:
The levels of DDH2 in NSCLC patients were significantly higher than those in healthy controls (P < 0.001). The diagnostic use of DDH2 in lung adenocarcinoma was significantly greater than that of carcinoembryonic antigen, cytokeratin 19 fragment (CYFRA21-1), and carbohydrate antigen 125 (P < 0.001). Combining DDH2 with carcinoembryonic antigen, CYFRA21-1, and carbohydrate antigen 125 was more effective for lung adenocarcinoma diagnosis than DDH2 alone. In addition, the levels of DDH2 could contribute to the diagnosis of lung squamous cell carcinoma.
Conclusions:
The measurement of serum DDH2 is a valuable diagnostic marker for NSCLC patients.
Introduction
Lung cancer is the leading cause of cancer-related death worldwide. 1 Non-small-cell lung cancer (NSCLC) accounts for 80–85% of total lung malignancies. 2 On the basis of histology, the NSCLC can be subdivided into adenocarcinomas (ADC), squamous cell carcinomas (SCC) and large cell carcinomas. When patients are diagnosed with early stage disease, their 5-year survival rate is nearly 60%. Unfortunately, the majority of patients are at an advanced stage of disease and the overall 5-year survival rate is only 15%. 3 Lung cancer survival mainly depends on the disease stage at diagnosis.4,5 Therefore, it is necessary to explore new biomarkers to diagnose early lung cancer.
The potential uses of tumor markers include aiding early diagnosis, monitoring cancer progression, and determining prognosis. 6 Tumor markers that are currently available for lung cancer, such as carcinoembryonic antigen (CEA), cytokeratin 19 fragment (CYFRA21-1), and carbohydrate antigen 125 (CA125) are not satisfactory for diagnosis at an early stage due to their low sensitivity and specificity.7,8 For more effective lung cancer diagnosis, we need to find higher specificity and sensitivity biomarkers.
Dihydrodiol dehydrogenase 2 (DDH2) is a member of aldo-keto reductase superfamily. 9 Previous studies showed that DDH was overexpressed in various types of tumors, such as ovarian cancer, uterine cervical cancers, and so on.10-15 Recent studies have reported that the serum DDH2 level was evaluated in NSCLC patients.16,17 However, the diagnostic value of the serum DDH2 level in these patients has not been fully assessed.
Therefore, we measured the levels of serum DDH2, CEA, CYFRA21-1, and CA125 in a large clinical population to investigate the diagnostic efficiency of these markers in NSCLC patients.
Patients and methods
Patients
A total of 863 NSCLC patients and 439 healthy individuals were enrolled at the Nanjing Chest Hospital from January 2012 to May 2016. The patients and healthy individuals were enrolled according to the following criteria: patients had no antineoplastic therapy, radiotherapy, or chemotherapy before the collection of the samples; healthy controls had not received a diagnosis of malignancy or benign tumors after routine examinations including chest X-rays, blood biochemical analysis, or tumor markers analysis. NSCLC was defined on the basis of computed tomography (CT) and confirmed by histopathology according to the World Health Organization Classification of Tumors of the Lung. 18 Tumors were staged pathologically according to the Union for International Cancer Control (UICC-7) staging system for lung cancer. 19 All samples were randomly separated into a training set and a test set.
The study protocol was approved by the ethics committee of Nanjing Chest Hospital. All patients provided written informed consent before enrollment.
Serum collection and determination of DDH2, CEA, CYFRA21-1, and CA125 levels
Serum samples from each individual were obtained at the time of diagnosis, before any therapeutic measures were started (surgery, chemotherapy, or radiation). Samples were centrifuged at 3000 rpm for 10 min at −4°C. The supernatant were stored at −80°C until testing. The levels of DDH2 were determined by enzyme-linked immunosorbent assay (ELISA). The tumor markers CEA, CYFRA21-1 and CA125 were measured electrochemiluminescence immunoassays on Roche Elecsys 1010 analyzer (Roche Diagnostics; Mannheim, Germany). All assays were run in duplicate, with dilutions as appropriate, and laboratory personnel were blinded to the identities of the samples. The upper normal limits for the tumor markers are 5 ng/mL for CEA, 3.3 ng/mL for CYFRA21-1, and 35 U/mL for CA125.
Statistical analysis
Statistical software (SPSS for Windows, version 18) was used for data analysis, and all values are given as mean ±SD. The Mann–Whitney U test was used to compare between serum sample groups, and the Kruskal–Wallis test was used to compare several groups. Receiver operating characteristic (ROC) curves were plotted to assess the sensitivity, specificity, and areas under the curves (AUC) with a 95% confidence interval (CI). The optimum cutoff value for diagnosis was determined by maximizing the specificity at 95% in the training set. Binary logistic regression was used to assess whether the diagnostic efficiency of DDH2 in combination with CEA, CA125, and CYFRA21-1 was superior to that of the four individual biomarkers alone. Differences were considered statistically significant when the P value was lower than 0.05.
Results
Clinical characteristics of patients
The mean age of the NSCLC patients (61 years) was not obviously different from the controls (60 years). The proportion of male gender accounted for 41.9% of the NSCLC patients and 52.3% of the controls, with no significant difference. Among the NSCLC patients, 417 had lung SCC and 446 had lung ADC. The patient’s characteristics are presented in Table 1.
Serum levels of DDH2, CEA, CYFRA21-1 and CA125
In the training set (n=432), the serum DDH2 levels in NSCLC patients were higher than those in the controls (9.24 ± 1.51 ng/mL vs. 1.31 ± 0.58 ng/mL, P < 0.001, Figure 1(a)). In the test set (n=431), the serum DDH2 levels in NSCLC patients were also higher than those in the controls (9.15 ± 1.59 ng/mL vs. 1.35 ± 0.73 ng/mL, P < 0.001, Figure 1(b)). In the whole set (n=863), the serum DDH2 levels in NSCLC patients were significantly higher than those in the controls (9.18 ± 1.65 ng/mL vs. 1.34 ± 0.59 ng/mL, P < 0.001, Figure 1(c)). In addition, the levels of serum CEA, CYFRA21-1, and CA125 in NSCLC patients were significantly higher than those in the controls (Table 2).
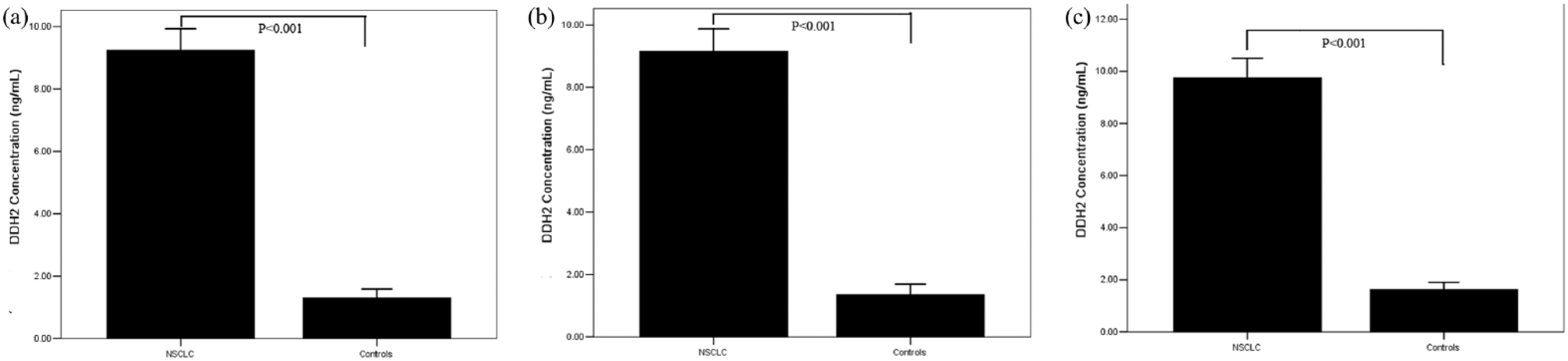
The serum DDH2 levels from individuals in the training, test, and whole sets. Serum DDH2 levels in the training set (a). Serum DDH2 levels in the test set (b). Serum DDH2 levels in the whole set (c).
The levels of serum DDH2, CEA, CYFRA21-1, and CA125.
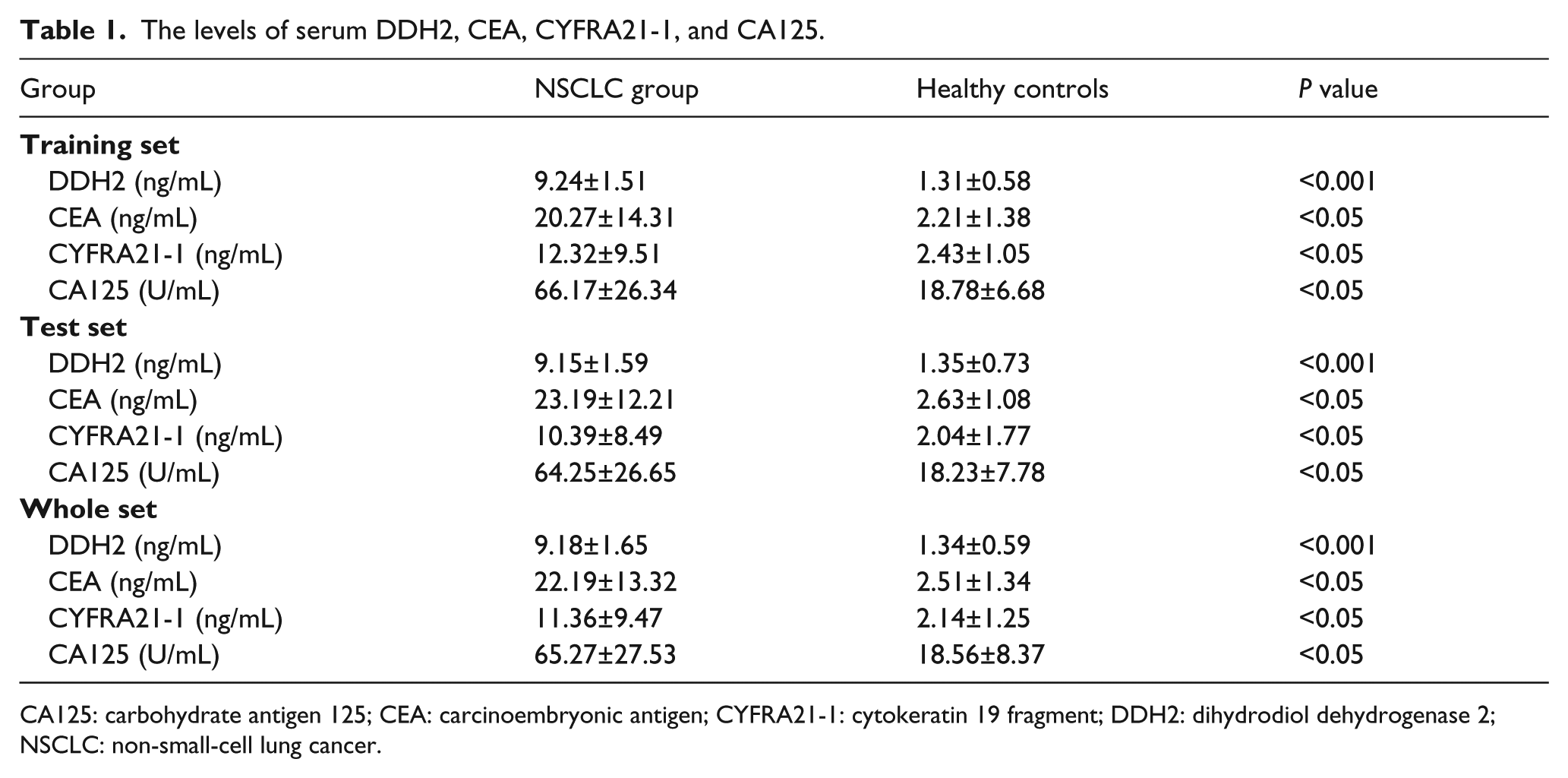
CA125: carbohydrate antigen 125; CEA: carcinoembryonic antigen; CYFRA21-1: cytokeratin 19 fragment; DDH2: dihydrodiol dehydrogenase 2; NSCLC: non-small-cell lung cancer.
The relationship between DDH2 levels and clinicopathological characteristics
The relationships between serum DDH2 levels and clinicopathological characteristics of NSCLC patients are shown in Table 1. In the training set, the levels of serum DDH2 in the ADC patients were significantly higher than those in the SCC patients (P < 0.01). In the test set, the serum DDH2 levels of ADC patients were also higher than those in the SCC patients (P < 0.01). These results indicate that serum DDH2 has a better diagnostic efficacy for identifying ADC patients than SCC. In addition, both in the training and test sets, the serum levels of DDH2 were significantly correlated with tumor, node, metastasis (TNM) stage (P < 0.01), lymph node metastasis (P < 0.05) and distant metastases (P < 0.01). These results indicated that serum DDH2 levels increased in NSCLC patients, and are associated with the progression and metastasis of NSCLC, which serve as a potential biomarker to differentiate NSCLC patients from healthy controls.
The relationship between serum DDH2 levels and clinicopathological characteristics in NSCLC patients.
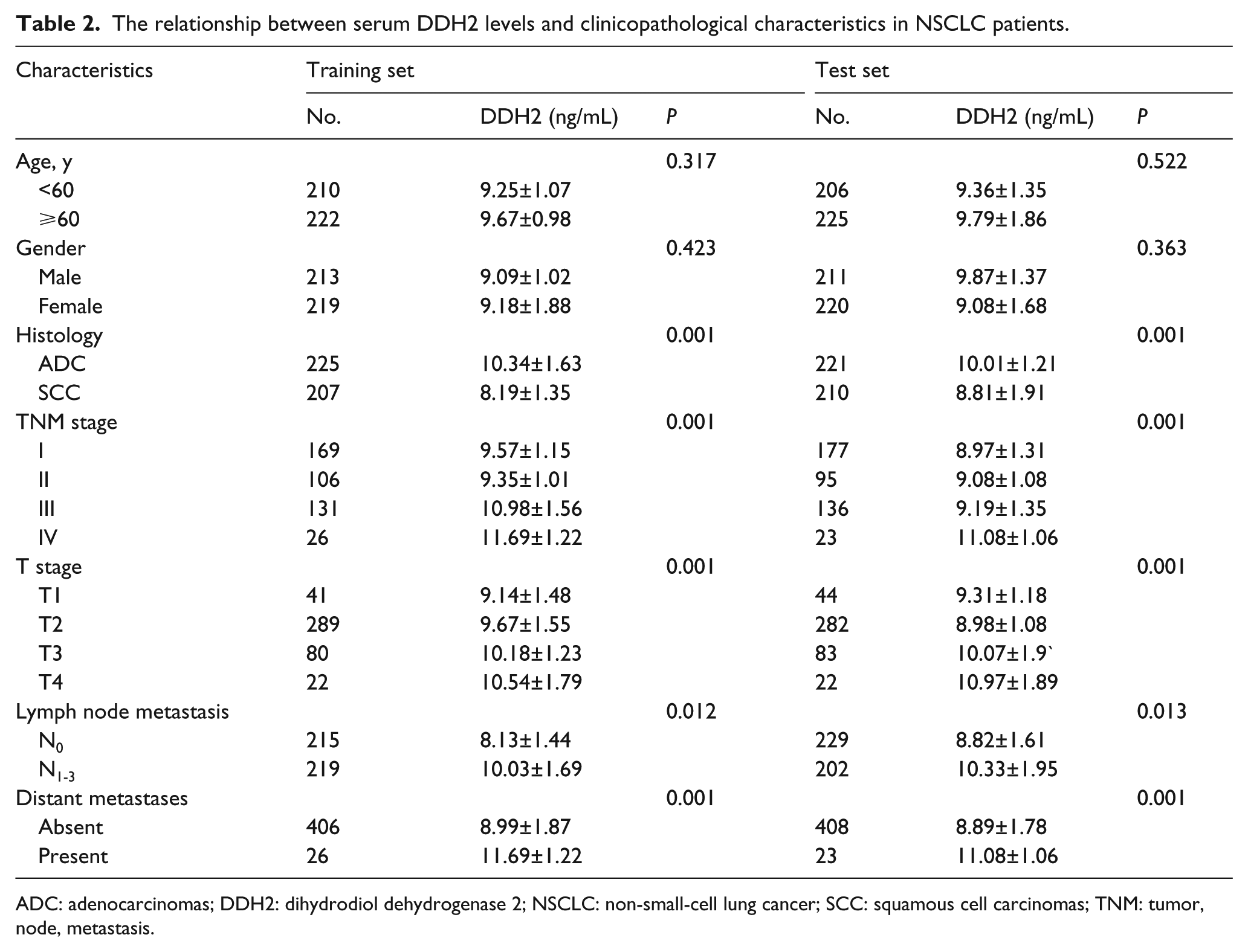
ADC: adenocarcinomas; DDH2: dihydrodiol dehydrogenase 2; NSCLC: non-small-cell lung cancer; SCC: squamous cell carcinomas; TNM: tumor, node, metastasis.
The Diagnostic Value of DDH2, CEA, CYFRA21-1, and CA125
ROC curves were plotted to determine the diagnostic efficiency of serum DDH2 levels for NSCLC. The efficiency of CEA, CYFRA21-1, and CA125 in distinguishing NSCLC from healthy controls was also included. The measurements of the different individual markers and their predictive value in the diagnosis of NSCLC are summarized in Table 3. Among the four biomarkers, DDH2 displayed the highest AUC (Figure 2(a), training set: 0.813, 95% CI 0.802, 0.944; test set: 0.810, 95% CI 0.725, 0.896; Table 3) and satisfactorily discriminated patients with ADC from healthy controls. CYFRA21-1 displayed the highest AUC in differentiating patients with SCC from healthy controls (Figure 2(b), training set: 0.840, 95% CI 0.753, 0.926; test set: 0.844, 95% CI 0.762, 0.927; Table 3). DDH2 and CA125 had similar moderate capacities for differentiating patients with SCC from healthy controls (P = 0.138; Table 3). CEA exhibited a low discriminatory capacity for both ADC and SCC, with AUC ranging from 0.519 to 0.602 (Figure 2(a) and (b); Table 3). DDH2 exhibited optimal efficacy for the diagnosis of all NSCLC (Figure 2(c), training set: 0.829, 95% CI 0.738, 0.920; test set: 0.798, 95% CI 0.711, 0.886; Table 3).These results show that the diagnostic efficacy of DDH2 in ADC and NSCLC overall was greater than that of CEA, CYFRA21-1, and CA125 (P < 0.001; Table 3). CYFRA 21-1 was the most efficient for the diagnosis of SCC but displayed a lower efficacy than DDH2 for NSCLC (training set: sensitivity 48.6%, specificity 87.3%; Table 3).
The diagnostic efficiency of models in differentiating NSCLC patients and the controls.
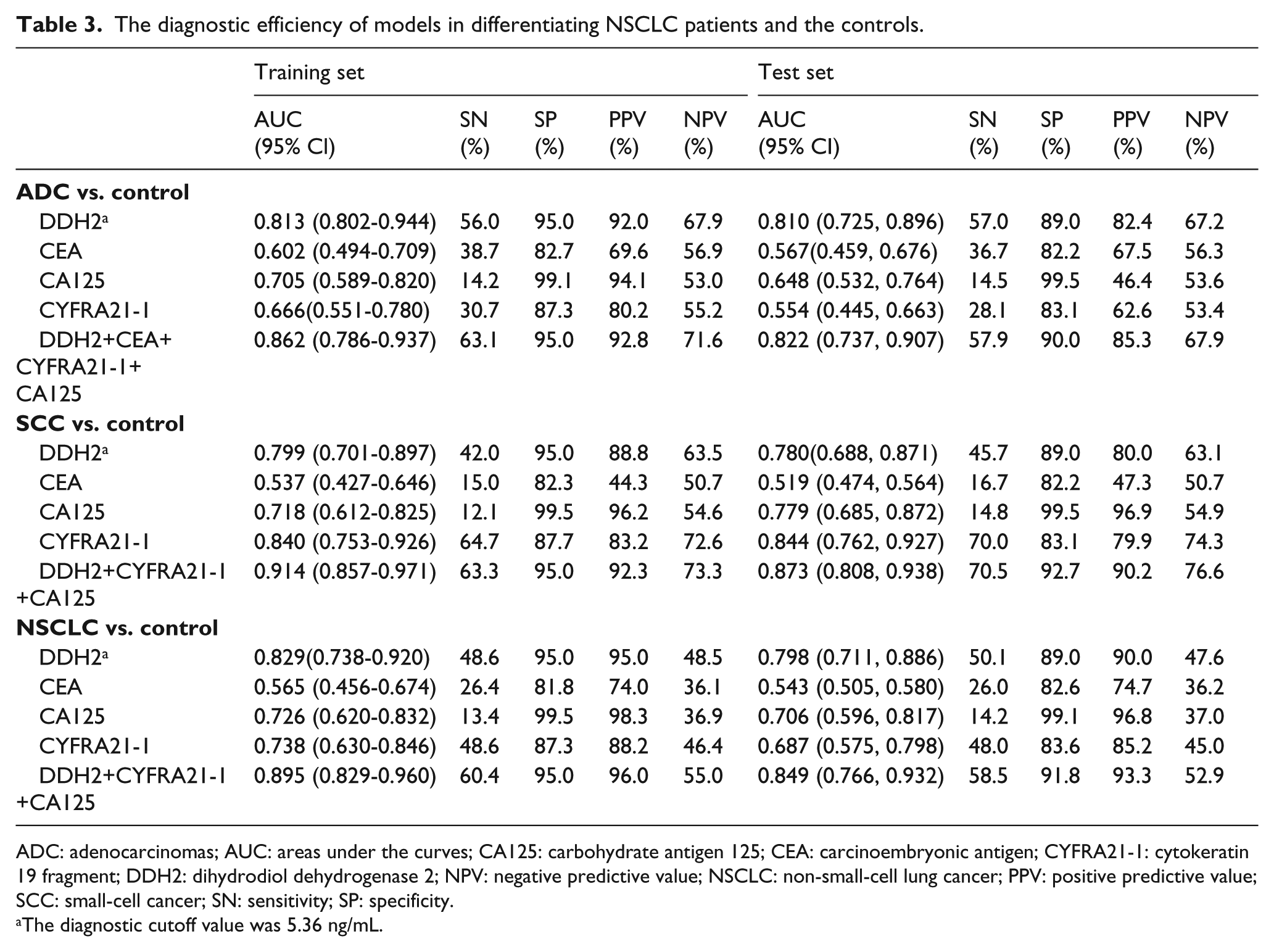
ADC: adenocarcinomas; AUC: areas under the curves; CA125: carbohydrate antigen 125; CEA: carcinoembryonic antigen; CYFRA21-1: cytokeratin 19 fragment; DDH2: dihydrodiol dehydrogenase 2; NPV: negative predictive value; NSCLC: non-small-cell lung cancer; PPV: positive predictive value; SCC: small-cell cancer; SN: sensitivity; SP: specificity.
The diagnostic cutoff value was 5.36 ng/mL.
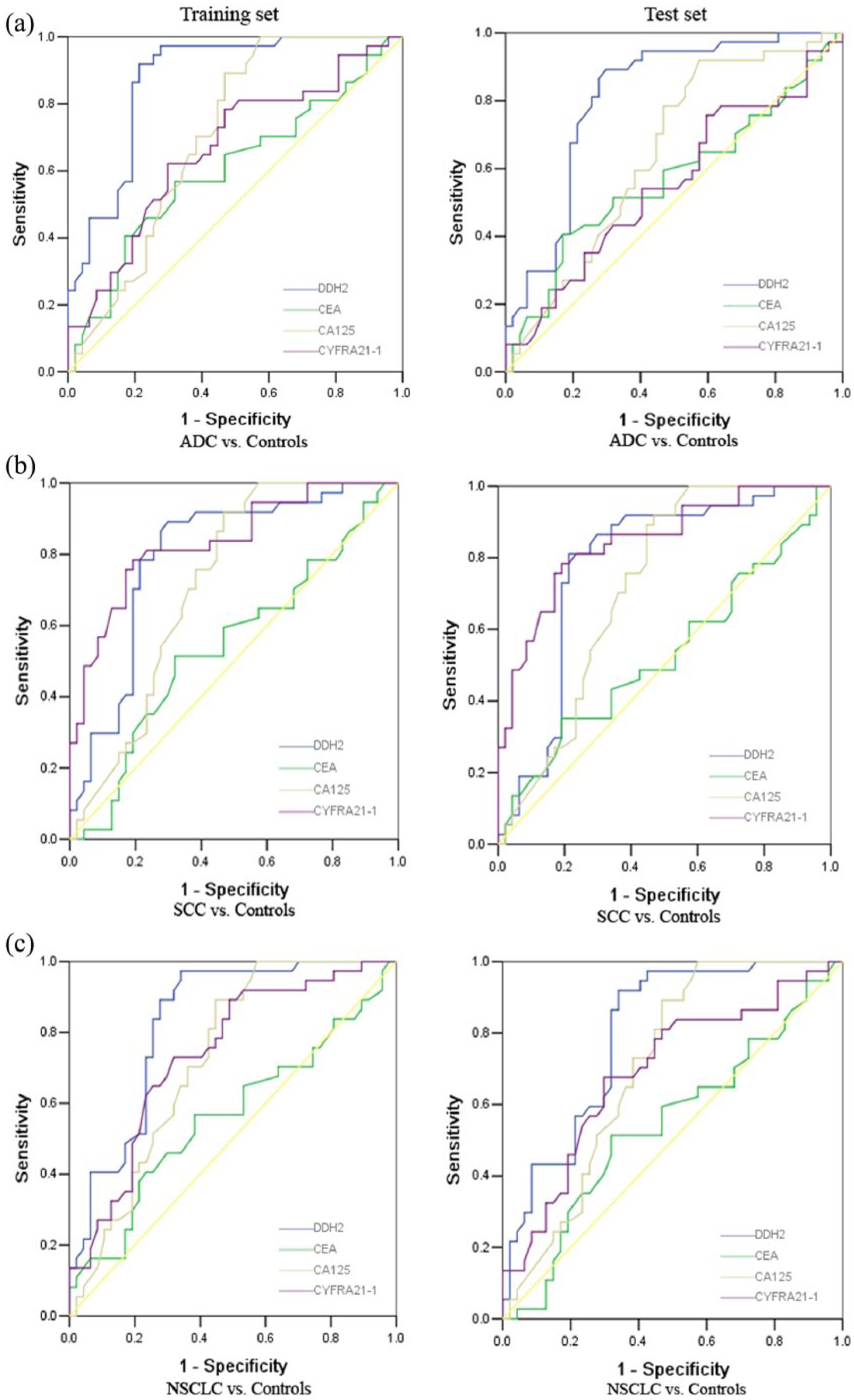
ROC curve analyses of the use of DDH2, CEA, CYFRA21-1, and CA125 to differentiate NSCLC patients and controls. (a) ROC curves for DDH2, CEA, CYFRA21-1, and CA125 for patients with ADC versus controls in the training (left) and test sets (right), respectively. (b) ROC curves for DDH2, CEA, CYFRA21-1 and CA125 for patients with SCC versus controls in the training (left) and test sets (right), respectively. (c) ROC curves for DDH2, CEA, CYFRA21-1, and CA125 for patients with NSCLC versus controls in the training (left) and test sets (right), respectively.
We used binary logistic regression to investigate whether combining the markers could improve diagnostic accuracy. The combination of DDH2, CEA, CYFRA21-1, and CA125 improved the classification capacity and yielded a better optimal diagnostic efficacy for ADC patients (training set: AUC 0.862; 95% CI 0.786, 0.937; test set: AUC 0.822; 95% CI 0.737, 0.907; Table 3) than did DDH2 alone (P < 0.01). For SCC patients, the combination of DDH2, CYFRA21-1, and CA125 had an AUC of 0.914 value (95% CI 0.857, 0.971) in the training set and 0.873 (95% CI 0.808, 0.938) in the test set, which was superior to CYFRA21-1 alone (P < 0.01). In addition, the combination of DDH2, CYFRA21-1, and CA125 represented a more efficient diagnostic modality (training set: AUC 0.895; 95% CI 0.829, 0.960; test set: AUC 0.849; 95% CI 0.766, 0.932; Table 3) for NSCLC than DDH2 or CYFRA21-1 alone (P < 0.01).
Discussion
DDH2 is overexpressed in various types of cancer tissues. Previous studies have mainly focused on detecting DDH2 in tumor tissue by the use of immunohistochemical study.10,11,15,16 Until now, only one study indicated that the serum DDH level is significantly higher in NSCLC patients than in healthy controls. 17 However, the sensitivity and specificity of DDH2 in NSCLC diagnosis was not further investigated. To our knowledge, this study is the first to investigate the serum DDH2 level in a large patient population to evaluate its clinical significance in NSCLC patients.
In the present study, we showed that the serum DDH2 levels were significantly elevated in NSCLC patients compared to the controls. These results indicate that serum DDH2 can be used as a biomarker for the diagnosis of lung cancer. We also tested CEA, CYFRA21-1, and CA125 levels and compared their diagnostic efficacy to that of DDH2. The results indicated that the combined detection of these four markers had a better diagnostic value than that of a single marker for the discrimination of NSCLC from healthy controls. This may offer a new method in differentiating NSCLC patients from healthy controls.
There are several good markers for the diagnosis of lung SCC, whereas good markers for ADC are lacking. 20 CYFRA21-1 was shown to have a good diagnostic value of SCC patients, with a high sensitivity but a low efficacy. 21 Therefore, we focused on ADC markers such as CEA and CA125. Both CEA and CA125 were useful for evaluating prognosis in NSCLC, but only performed moderately in diagnosing NSCLC. 22 Our results showed that CYFRA21-1 is a good marker for SCC diagnosis, with a much better sensitivity than DDH2, CEA, or CA125. In contrast, DDH2 indicated higher sensitivity than CEA, CYFRA21-1, or CA125 for ADC diagnosis. In the training set, the combination of DDH2 with CEA, CYFRA21-1, and CA125 improved the diagnostic sensitivity to 63.1% in ADC, 63.3% in SCC, and 60.4% in NSCLC. These results were validated in the test set. Our analyses of a large cohort of NSCLC patients showed that DDH2 is a highly effective diagnostic marker for ADC.
Several limitations of our study warrant discussion. First, serum samples were obtained from only the Asiatic population. Second, the used cutoff for CEA, CA125, and CYFRA21-1 are not universally recognized, with little difference in upper limits between laboratories. Third, the sensitivity and negative predictive value of DDH2 for ADC and NSCLC diagnosis is low.
In conclusion, our data suggest that serum DDH2 could be used to assist the diagnosis of NSCLC, particularly ADC.
Footnotes
Authors’ contributions
Chun-Hua Xu and Ding-Yu Ren contributed equally to this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.