
Abstract
BACKGROUND:
Blood-circulating miRNAs have been reported to act as potential biomarkers in various cancers including non-small cell lung cancer (NSCLC).
OBJECTIVE:
This study was to assess serum miR-98 levels in NSCLC patients and explore its potential prognostic value.
METHODS:
The relative expression levels of miR-98 were detected by quantitative RT-PCR in the sera of 127 NSCLC patients and 60 healthy controls.
RESULTS:
Our results showed that serum miR-98 expression was down-regulated in NSCLC patients compared with healthy controls. Receiver operating characteristic (ROC) curve analysis suggested that serum miR-98 could be used as a potential marker in the diagnosis of NSCLC. In addition, decreased serum miR-98 was positively correlated with worse TNM stage, lymph node metastasis, as well as unfavorable overall survival. Multivariate Cox regression analysis confirmed that serum miR-98 expression was an independent prognostic factor for NSCLC.
CONCLUSIONS:
Therefore, serum miR-98 might be useful as a promising biomarker for prognosis prediction of NSCLC.
Introduction
Non-small cell lung cancer (NSCLC), which accounts for approximately 80%–85% cases of lung cancer patients, is one of the leading fatal malignancy around the world [1, 2]. Although huge progress has been made in the treatment of this deadly disease over the past decades, the 5-year overall survival rate of NSCLC patients remains dismal [3, 4, 5]. Therefore, it is extremely urgent to identify potential novel biomarkers to improve the prognosis of patients with NSCLC.
MicroRNAs (miRNAs) are a subset of small, non-coding RNAs consisting of 19–25 nucleotides. MiRNAs can negatively modulate target genes expression by binding to the 3
MiR-98 belongs to the let-7/miR-98 family which is highly evolutionally conserved [12, 13]. Recently, miR-98 had been reported to play critical roles in the development of various cancers such as glioma [14], prostate cancer [15], head and neck squamous cell carcinoma [16] and NSCLC [17, 18]. However, the diagnostic and prognostic significance of serum miR-98 in NSCLC patients was still unknown. This study was to detect serum miR-98 level in NSCLC patients and explore its potential clinical value.
Materials and methods
Patients and sample collection
A total of 127 NSCLC patients prior to any treatment were enrolled in this study. The patient group included 79 men and 48 women aged between 38 to 72 years old (median age
Blood samples were collected from patients with NSCLC and healthy controls early in the morning. Up to 5 ml of fasting venous blood was collected in a serum separator tube from every participant. The blood samples of healthy controls were not mixed with those of tumor patients. All blood samples were centrifuged at 2800 g for 10 min within half an hour after collection. Then the separated supernatant was stored in 1.5-mL tubes at
Total RNA isolation and quantitative RT-PCR
Total RNA was extracted from serum samples using a miRVana PARIS Kit (Applied Biosystems, Foster City, CA, USA) in accordance with the manufacturer’s protocols. RNA purity and concentration was determined using a NanoDrop ND-1000 spectrophotometer (NanoDropTechnologies, Wilmington, DE). Reverse transcription reaction was performed using a TaqMan MicroRNA Reverse Transcription Kit (Applied Biosystems, Foster City, CA, USA). Subsequently, Quantitative RT-PCR was carried out using the Maxima SYBR Green qPCR Kit (Thermo Scientific, CA, USA) on an ABI 7500 fast real-time PCR system (Applied Biosystems, Foster City, USA) according to the manufacturer’s instructions. The PCR cycling conditions were as follows: 95
Statistical analysis
Statistical analysis was performed using GraphPad Prism v5.0 software (GraphPad Software, Inc., San Diego, CA). The data was not subjected to normal distribution. Therefore, the median value of serum miR-98 in this NSCLC cohort was used as a cut-off point to divide the patients into two groups namely high serum miR-98 group and low serum miR-98 group. The difference in serum miR-98 levels between two groups was compared by Mann-Whitney U test. The Pearson’s chi-squared test was used to evaluate the association between serum miR-98 levels and clinical parameters. Survival curves were constructed using the Kaplan-Meier method and compared by log-rank test. The Cox proportional hazards model was used for multivariate analyses of the independent prognostic factors. Receiver-operating characteristic (ROC) curve was constructed to determine the diagnostic value of serum miR-98 for NSCLC.
Association between serum miR-98 expression and clinicopathological characteristics of NSCLC patients
Association between serum miR-98 expression and clinicopathological characteristics of NSCLC patients
Serum miR-98 expression was significantly decreased in patients with NSCLC.
Down-regulation of serum miR-98 in NSCLC patients and its diagnostic value
qRT-PCR was used to detect the levels of serum miR-98 in 127 NSCLC patients and 60 healthy controls. The results showed that serum miR-98 expression was greatly lower in NSCLC patients than that in healthy control (
fAs shown in Fig. 3, ROC curve analysis revealed that serum miR-98 was an accurate indicator for discriminating NSCLC patients from healthy controls. The area under the curve (AUC) was 0.857, and the sensitivity and specificity were 80.3% and 81.7%, respectively.
Association between the relative miR-98 expression and TNM stage as well as lymph node metastasis of NSCLC patients.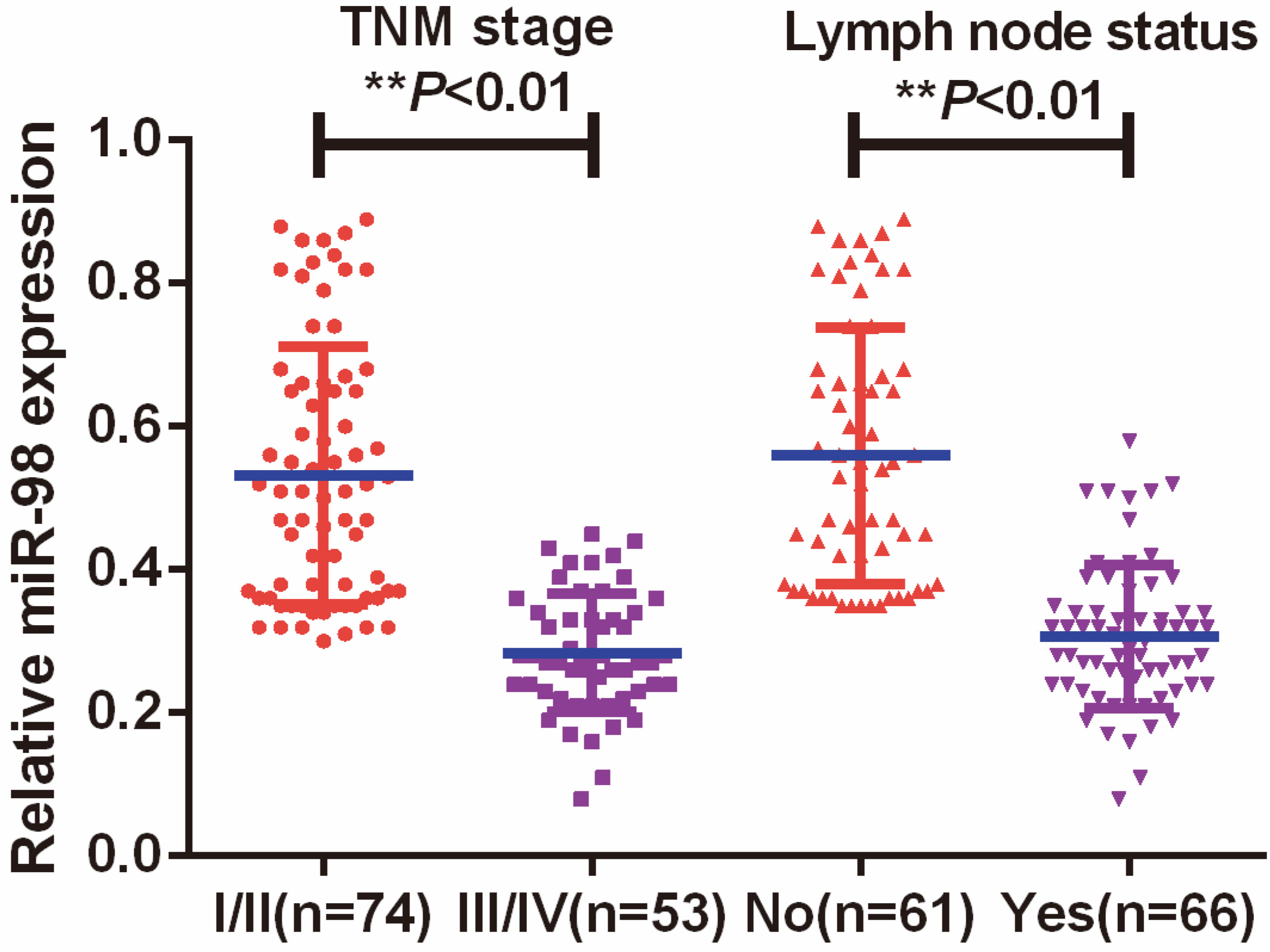
Univariate and multivariate analysis for OS in NSCLC patients by Cox regression model
ROC curve analysis of the serum miR-98 to distinguish NSCLC patients from healthy controls.
subSerum miR-98 correlated with clinical characteristics in NSCLC patients
All the 127 NSCLC patients were divided into high miR-98 expression group (
The Kaplan-Meier method and log-rank test demonstrated that the NSCLC patients in low serum miR-98 expression group had shorter OS than those in high serum miR-98 expression group, suggesting that lower serum miR-98 expression was correlated with worse prognosis of NSCLC (
Overall survival analysis of clinical variables in NSCLC patients.
Besides, univariate cox regression analysis found out that serum miR-98 expression (HR
In this study, a significant decrease in serum miR-98 expression was detected in NSCLC patients when compared to healthy controls. Moreover, ROC curve analysis suggested that serum miR-98 could effectively discriminate NSCLC patients from healthy controls. Furthermore, a positive correlation was observed between down-regulated serum miR-98 expression and poor clinical features as well as unfavorable OS. Finally, serum miR-98 expression was confirmed to be an independent prognostic factor for NSCLC. These findings indicated that miR-98 might serve as a tumor suppressor in NSCLC. Consistent with previous studies, Ni et al showed that miR-98 was down-regulated in both NSCLC tissues and cells. Ectopic miR-98 expression suppressed the oncogenic potential of NSCLC cells in vitro and in vivo [17]. Similarly, decreased miR-98 expression markedly stimulated NSCLC cell proliferation and invasion by regulating P21-activated protein kinase 1 [18]. Du et al. found that miR-98 could downregulate the expression of tumor suppressor gene FUS1 in lung cancer cell lines. However, they also showed that the expression level of miR-98 was lower in NSCLC cell line compared with normal bronchial epithelial cell line. In addition, no correlation was found between miR-98 and FUS1 expression levels in the lung cancer specimens [19]. Therefore, these data does not indicate miR-98 plays an oncogenic role in NSCLC.
MiR-98 was also found to exhibit a tumor suppressive role in other types of cancers. For instance, miR-98 was significantly reduced in hepatocellular carcinoma and decreased miR-98 levels were associated with unfavorable clinicopathological parameters. Overexpression of miR-98 inhibited hepatocellular carcinoma cell proliferation, migration, invasion and epithelial-mesenchymal transition through down-regulating SALL4 [20]. In esophageal squamous cell carcinoma (ESCC), reduced miR-98 was associated with various clinical features such as pathological grade, tumor stage and lymph node metastasis. In addition, ectopic expression of miR-98 inhibited the migration and invasion capacity of ESCC cells by targeting EZH2 [21]. MiR-98 levels were decreased in both oral squamous cell carcinoma (OSCC) tissues and cell lines. Moreover, upregulation of miR-98 repressed OSCC cell growth and migration via inversely regulating IGF1R [22]. Liu and colleagues showed that miR-98 level was dramatically down-regulated in salivary adenoid cystic carcinoma tissues. In addition, restoration of miR-98 suppressed cell proliferation, migration and invasion in vitro [23]. Enforced miR-98 expression reduced melanoma cell migration in vitro and suppressed metastatic tumor size in vivo by a negative feedback loop with IL-6. Additionally, increased miR-98 expression reduced tumorigenicity and enhanced survival in part by down-regulating IL-6 levels [24]. Up-regulation of miR-98 strongly inhibited glioma cell migration and invasion through degrading I
Interestingly, miR-98 was found to act as an onco-miRNA in breast cancer. Deng et al. revealed that higher miR-98 levels were observed in breast cancer tissues in comparison with cancer free controls. Furthermore, miR-98 was proved to serve as serum marker for discriminating breast cancer patients from healthy controls, indicating that over-expression of miR-98 contributed to carcinogenesis of breast cancer [25]. One possible reason is that the biological function of miR-98 is tissue specific. Further exploration of the hidden molecular mechanisms and downstream targets accounting for the role of miR-98 in tumorigenesis is required.
In conclusion, this study revealed that serum miR-98 expression was greatly down-regulated in patients with NSCLC. Moreover, downregulated miR-98 level was significantly associated with poor clinical outcome of NSCLC. Therefore, our findings demonstrate that serum miR-98 might serve as a promising biomarker for prognosis prediction of NSCLC.
Conflict of interest
None.