
Abstract
Pancreatic carcinoma is a highly malignant disease associated with an extremely poor prognosis, which is caused by late presentation, aggressive invasion and metastases, as well as the detection of pancreatic carcinoma in its advanced stages. Thus, better understanding of the tumour biology of this malignancy is sorely needed to improve the clinical outcome. A great challenge for the medical practice is finding a new biomarker of pancreatic carcinoma that will be helpful in diagnosis, in prognosis and in making clinical decisions, including the assessment of patients’ response to therapy. It is suggested that selected chemokines and their specific receptors play an important role in tumour progression, such as tumour growth, angiogenesis, proliferation and development of metastasis. In the present review, general characteristics of chemokines and their specific receptors as well as the significance of these molecules in tumour development are described. The crucial issue of this review is to summarise the importance of various chemokines and their specific receptors in pancreatic carcinoma. Understanding the role of chemokines in the pathogenesis of pancreatic carcinoma is extremely important since these proteins may be used as a potential tool in the diagnosis and prognosis of pancreatic carcinoma patients.
Keywords
Pancreatic cancer
Pancreatic cancer (PC) is a highly aggressive malignant tumour with a very poor prognosis. This neoplasm is the fourth leading cause of cancer-related death worldwide and the tenth in annual incidence among all malignancies (1, 2). PC is characterised by aggressive growth and a high metastatic rate. This malignancy metastasises predominantly to multiple lymph nodes and to more than one lymph node group. In addition, the most common sites for distant intra-abdominal metastasis are the peritoneum and the liver, while the extraperitoneal sites for metastases are located in the lung (3). Ductal adenocarcinoma of the pancreas is the most common epithelial exocrine pancreatic tumour and accounts for more than 85% of all malignant pancreatic neoplasms. About 80%–90% of PC are located in the head of the gland (3). The incidence of this malignancy is higher in individuals aged 65–75 (3). Moreover, the resection margin, metastatic nodes, blood-transfusion and grading independently influence patient prognosis (4). In addition, a study by Contreras et al. (5) demonstrated the association between lymph node retrieval and the survival of pancreatic adenocarcinoma patients undergoing pancreaticoduodenectomy. Therefore, it has been estimated that the one year survival rate is 13%, while the overall five-year survival rate is less than 5%. Some authors suggest that, within the next decade, PC will become the second leading cause of cancer-related death in the USA and other Western countries (6, 7). A lack of symptoms, even in advanced stages of the disease, is the main reason why potentially curative surgical tumour resection is appropriate only in 15%–20% of PC patients, while the remainder of patients are treated using adjuvant therapies (8). The symptoms of PC often include abdominal pain, loss of appetite and loss of weight.
PC remains a highly deadly disease. Therefore, there is an urgent need to improve the early diagnosis of PC. Current multiagent chemotherapy has improved the overall survival of PC patients. Unfortunately, this treatment has toxic side effects. The clinical course of PC is usually aggressive, with a high symptom burden that causes significant deterioration of the patient’s quality of life (7).
Diagnosis of patients with PC
Routine diagnosis and detection methods of PC in clinical practice continue to be based on endoscopic ultrasonography, computed tomography, endoscopic retrograde cholangiopancreatography, magnetic resonance imaging and magnetic resonance cholangiopancreatography. However, these techniques have limited usefulness due to their cost and invasiveness (9). Moreover, measurement of the concentration of the well-established biomarker for PC, such as cancer antigen 19-9 (CA 19-9) – the current gold standard blood-based marker, is not sufficiently specific to be used in early detection (10). It has been estimated that the sensitivity and specificity for the measurement of CA 19-9 levels in PC patients is 79% and 82%, respectively (11, 12). Serum levels of CA 19-9 have been found to be elevated in patients with benign pancreatic diseases, acute pancreatitis and chronic pancreatitis, and therefore discrimination between PC and benign pancreatic diseases is very difficult (11, 12). Thus, a non-invasive and accurate method for early detection of PC as well as novel approaches to diagnosing PC in patients, such as the establishment of other biochemical markers, are sorely needed to improve the management of PC patients.
Chemokines and their specific receptors – general characteristics and their role in tumour progression
Chemokines are a family of structurally related low-molecular-weight proteins, and most of them are produced under pathological conditions by tissue cells and infiltrating leukocytes. Over 50 chemokines have been identified and grouped into four classes: CC, CXC, CX3C and XC. This classification is based on the positions of key cysteine residues (13). Chemokines can also be divided on the basis of their function into homeostatic, inflammatory or dual function chemokines. In general, homeostatic chemokines are involved in controlling cell migration, while inflammatory chemokines are activated during an immune response (14).
Chemokines act through their cognate G-protein coupled specific receptors to cause a response from cells, such as adhesion, migration and chemotaxis (15, 16). Chemokine receptors are seven-transmembrane receptors consisting of the N-terminus outside the cell surface, three extracellular and three intracellular loops as well as the C-terminus in the cytoplasm (17, 18). Approximately 20 chemokine receptors have been investigated to date.
Chemokines and their specific receptors are known to play important roles in the regulation of leukocyte functions such as growth, differentiation and activation (15, 19). They regulate inflammatory, infection and immunity processes, as well as tissue injury reactions. However, chemokines might be involved in a number of pathological processes including the development of cardiovascular and malignant diseases, such as PC (15, 19).
Uncontrolled inflammation has been associated with the development of various malignancies, including PC (20-25). Inflammatory mediators within the tumour microenvironment are involved in a complex signalling process which facilitates tumour progression via the migration of neoplastic cells through the stroma. Local and systemic inflammatory responses might also be induced by the developing malignancy (20, 21). Some clinical investigations have proved that various inflammatory mediators, including cytokines, matrix metalloproteinases and chemokines are involved in tumour cell growth, proliferation, migration and angiogenesis of tumour cells, including PC (16, 20). The significance of selected chemokines and their specific receptors has been reported in a series of human gastrointestinal malignancies, including gastric, colorectal, oesophageal cancer and hepatocellular carcinoma (26-37) (Tab. I). The investigations proved the significance of various chemokines in tumour progression although the clinical utility of these molecules in PC and its potential usefulness in the diagnosis of patients remains unclear. Evidence from previous studies suggests that selected chemokines and their specific receptors are able to facilitate tumour dissemination at every stage of progression, including adherence of tumour cells to the endothelium, extravasation from blood vessels, proliferation and angiogenesis (20, 24-26). These molecules might also simplify communication between neoplastic cells and non-neoplastic cells within the tumour microenvironment, stimulating the activation of neutrophils and tumour-associated macrophages.
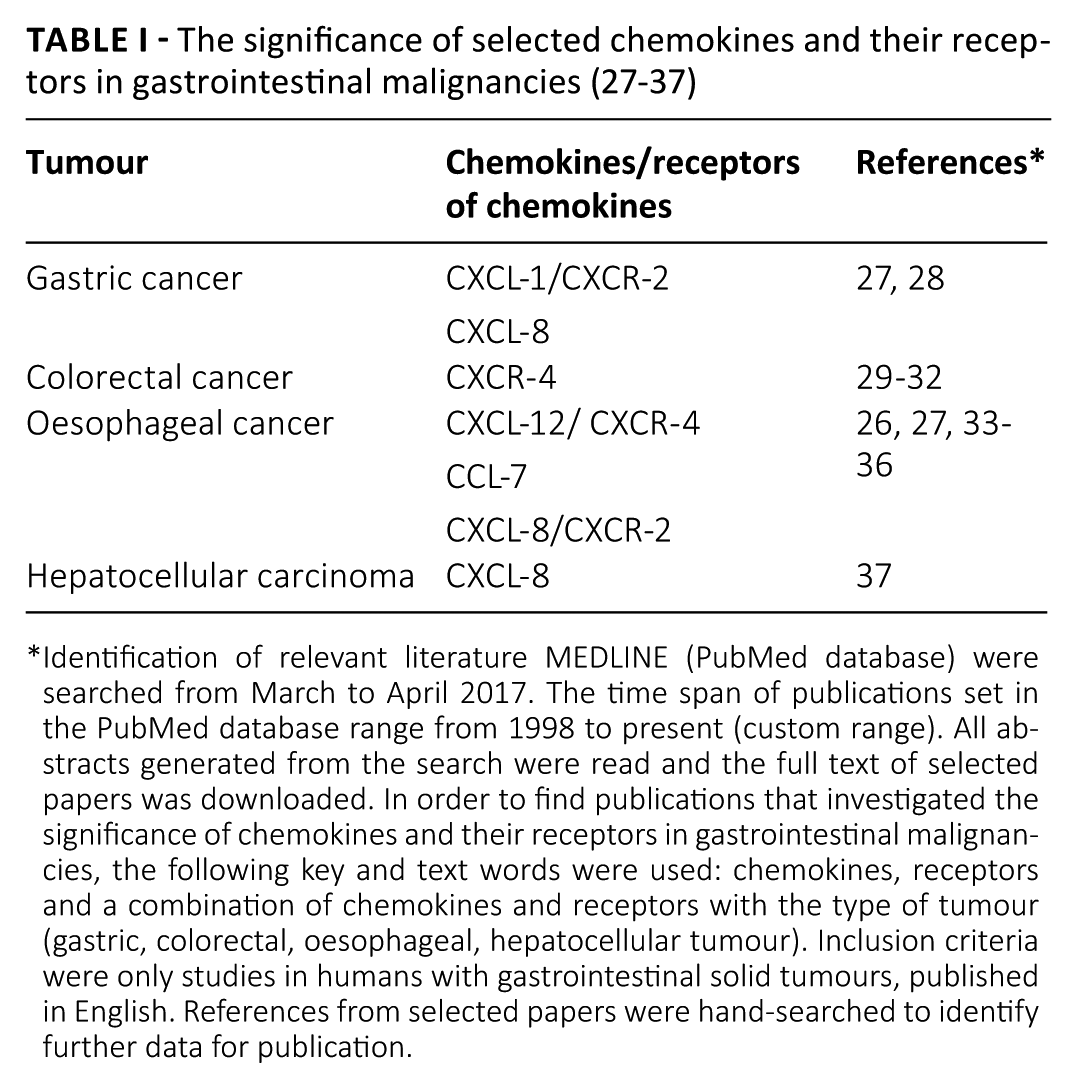
Identification of relevant literature MEDLINE (PubMed database) were searched from March to April 2017. The time span of publications set in the PubMed database range from 1998 to present (custom range). All abstracts generated from the search were read and the full text of selected papers was downloaded. In order to find publications that investigated the significance of chemokines and their receptors in gastrointestinal malignancies, the following key and text words were used: chemokines, receptors and a combination of chemokines and receptors with the type of tumour (gastric, colorectal, oesophageal, hepatocellular tumour). Inclusion criteria were only studies in humans with gastrointestinal solid tumours, published in English. References from selected papers were hand-searched to identify further data for publication.
Selected chemokines and their specific receptors in PC
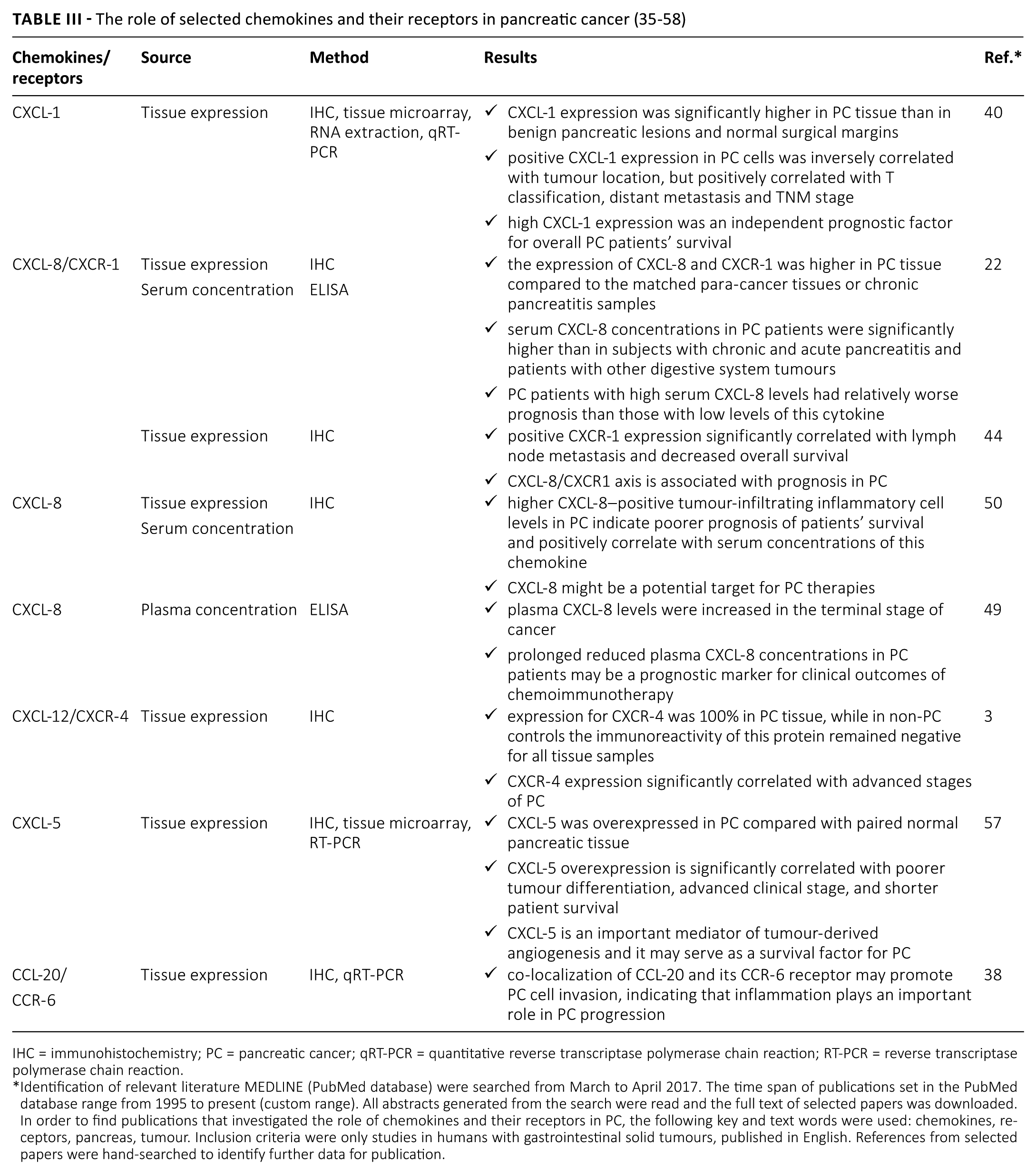
Clinical investigations have suggested that chemokines and their receptors might also play a role in the pathogenesis of PC (20, 24, 25). The classification of selected chemokines and their receptors, which play a potential role in PC, is presented in Table II (38-58). Chemokine CXCL-1 (C-X-C motif chemokine ligand 1) belongs to the CXC chemokine family and is known to play a role in inflammation, angiogenesis and wound healing, as well as in tumorigenesis via the regulation of tumour progression, such as tumour growth, angiogenesis, proliferation and the development of metastasis (40). The role of selected chemokines and their receptors in PC is presented in Table III. Lian et al. (40) assessed the clinical significance of CXCL-1, known as growth-regulated oncogene-alpha (GRO-α), in PC by determining the expression of this protein in PC tissue using the immunohistochemical technique, tissue microarray construction, RNA extraction and quantitative reverse transcriptase polymerase chain reaction (qRT-PCR) analyses. The authors revealed that the frequency of increased CXCL-1 protein expression in the cytoplasm of cancer cells and stroma was significantly higher in PC in comparison with benign pancreatic lesions and normal surgical margins. It has been shown that positive CXCL-1 expression in the cytoplasm of cancer cells was inversely correlated with tumour location, but positively correlated with T classification, distant metastasis and TNM stage. Furthermore, high CXCL-1 expression in the cytoplasm of cancer cells or stroma, TNM classification, T classification and lymphatic metastasis were independent prognostic factors for the overall PC patients’ survival, which was confirmed by multivariate regression analysis. The authors also demonstrated that PC patients with positive CXCL-1 expression in cancer cells had significantly poorer survival compared to those with negative expression of this cytokine, which was assessed using Kaplan–Meier survival curves. These findings indicate the potential usefulness of CXCL-1 as a prognostic biomarker of PC (40).
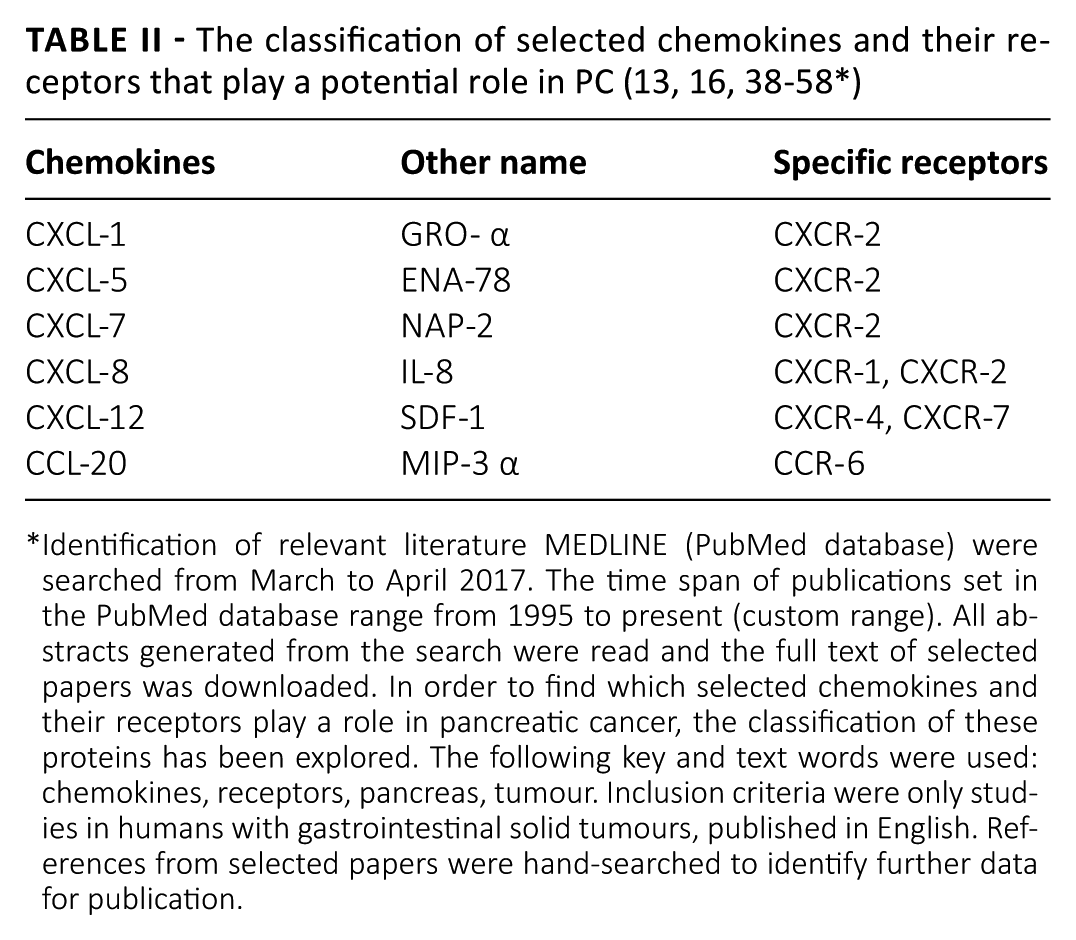
Identification of relevant literature MEDLINE (PubMed database) were searched from March to April 2017. The time span of publications set in the PubMed database range from 1995 to present (custom range). All abstracts generated from the search were read and the full text of selected papers was downloaded. In order to find which selected chemokines and their receptors play a role in pancreatic cancer, the classification of these proteins has been explored. The following key and text words were used: chemokines, receptors, pancreas, tumour. Inclusion criteria were only studies in humans with gastrointestinal solid tumours, published in English. References from selected papers were hand-searched to identify further data for publication.
IHC = immunohistochemistry; PC = pancreatic cancer; qRT-PCR = quantitative reverse transcriptase polymerase chain reaction; RT-PCR = reverse transcriptase polymerase chain reaction.
Identification of relevant literature MEDLINE (PubMed database) were searched from March to April 2017. The time span of publications set in the PubMed database range from 1995 to present (custom range). All abstracts generated from the search were read and the full text of selected papers was downloaded. In order to find publications that investigated the role of chemokines and their receptors in PC, the following key and text words were used: chemokines, receptors, pancreas, tumour. Inclusion criteria were only studies in humans with gastrointestinal solid tumours, published in English. References from selected papers were hand-searched to identify further data for publication.
Chemokine CXCL-8 is a pro-inflammatory factor that belongs to the CXC chemokine family. This molecule is a chemotactic activator of granulocytes in inflammatory and immune reactions. However, CXCL-8 might play a role in cancer invasion, angiogenesis and metastasis, as well as be a component of the tumour microenvironment (22, 41-43). It has been shown that stromal cells can produce CXCL-8 to influence the ability of invasion and metastasis of tumour cells. Moreover, tumour cells may also secrete this chemokine in an autocrine or paracrine manner in a number of malignancies including PC (42, 44). It has been shown that the most critical effect of this chemokine on tumour cells is its considerable angiogenic potential and its ability to promote invasion and metastasis (42, 45, 46). Chen et al. (22) investigated the clinical significance of CXCL-8 in PC prognosis by examining the expression and serum concentration of CXCL-8 in PC. The expression of CXCL-8 and CXCR-1 proteins was higher in PC samples compared with the matched para-cancer tissues, suggesting that this cytokine might be produced by PC cells. PC cell lines showed high levels of CXCL-8 in the supernatant and mRNA expression, which has also been confirmed by other authors (47). In addition, it has been shown in this latter study that serum CXCL-8 levels in PC patients were significantly higher than in patients with other digestive system tumours or with chronic and acute pancreatitis (28, 48). Thus, the authors suggested that PC cells had a higher ability to produce chemokines than inflammatory cells and function in an autocrine manner (22, 48). Moreover, PC patients with high serum CXCL-8 levels had a relatively poorer survival outlook compared with those with low concentrations of CXCL-8 (22). The authors concluded that this chemokine might be a sensitive marker in predicting prognosis and monitoring disease progression in PC patients. In addition, patients with high serum CXCL-8 concentrations should receive more active treatment due to the more aggressive biology of this malignancy. This study represents a promising target for the development of adjuvant therapies for PC (22), which has been confirmed by other authors (49, 50). The concentrations of CXCL-8 in the sera of PC patients were also investigated by Kim et al. (51), although the authors failed to demonstrate if this cytokine was correlated with inflammatory markers, and whether it may predict the tumour progression pattern.
CXCR-1 is a G-protein coupled receptor that binds chemokine CXCL-8 with high affinity. This receptor is expressed primarily in neutrophils (52). However, it has been suggested that CXCR-1 may also play a role in tumorigenesis, including PC. The study of Chen et al. (44) indicated that positive CXCR-1 expression significantly correlated with lymph node metastasis. In addition, the authors showed that multivariate analysis confirmed a significant association between positive CXCR-1 expression and a decreased overall survival, concluding that the CXCL-8/CXCR1 axis is associated with the prognosis in PC (44).
The role of chemokine CXCL-12, known as stromal cell derived factor 1 (SDF-1), and its specific receptor type 4 (CXCR-4) in tumour development has been suggested by many authors (3, 28, 53-56). It has been shown that gastrointestinal tumours co-expressed CXCL-12 and its specific receptor CXCR-4 in an autocrine and paracrine fashion (53). The activation of CXCR-4 by CXCL-12 might induce the migration, invasion and angiogenesis of tumour cells (3, 54). The study of Wehler et al. (3) evaluated the expression of CXCR-4 in PC tissue and PC cell lines, using immunohistochemical technique and Western blot analysis. Moreover, the authors compared levels of these molecules with the clinicopathological parameters of the tumour. In PC tissue, the respective expression rate for CXCR-4 was 100%, while in non-PC controls the immunoreactivity of this protein remained negative for all tissue samples (3). CXCR-4 expression significantly correlated with the advanced stages of cancer and indicated a strong trend towards haematogenous dissemination and progressed local disease, while no correlation was established for lymphatic dissemination. However, the over-expression of CXCR-4 was not significantly correlated with the decreased survival of PC patients. The authors concluded that the strong expression of CXCR-4 was significantly associated with advanced PC and confirmed that this protein was linked to tumour dissemination and poor prognosis (3). Thus, the inhibition of PC progression by CXCR-4 antagonists might be a promising therapeutic tool (3). Similar findings were shown by Saur et al. (56) who demonstrated that CXCR-4 expression might mediate the metastases of PC cells, which was evaluated using murine in vivo studies.
Other chemokines from the CXC chemokine family that might have significance for the development of PC are CXCL-5 and CXCL-7 (57, 58). A study by Li et al. (57) demonstrated that CXCL-5 was overexpressed in PC tissue compared to normal pancreatic tissue. In addition, CXCL-5 overexpression was significantly correlated with poorer tumour differentiation, advanced clinical stage and shorter patient survival. The authors concluded that CXCL-5 might be an important mediator of tumour-derived angiogenesis and may serve as a survival factor for PC patients. The role of CXCL-7 as a novel biomarker in PC was presented by Matsubara et al. (58) who compared the diagnostic significance of CXCL-7 with a classical tumour marker for PC – CA 19-9. The authors indicated a significant decrease in plasma CXCL-7 levels in PC patients and concluded that the combined analysis of CXCL-7 and CA19-9 may improve the discriminatory power of the former in PC.
The C-C motif chemokine CCL-20, known as macrophage inflammatory protein-3 alpha (MIP-3α), is a chemotactic cytokine involved in inflammatory cell migration via its binding to the highly specific transmembrane receptor CCR-6. It is suggested that this protein might play a role in neoplastic processes. It has recently been shown that CCL-20 may promote tumour cell migration and invasion in PC (38). The immunohistochemical staining and qRT-PCR confirmed the co-localization of CCL-20 and its specific receptor CCR-6 in PC. Immunoreactivity of this cytokine was also positive within the stromal cells adjacent to cancer cells in PC tissue, while qRT-PCR confirmed the presence of CCL-20 messenger RNA within PC cell lines (38). The authors concluded that the co-localization of CCL-20 and its CCR-6 receptor may promote PC cell invasion, indicating that inflammation plays an important role in PC progression. Therefore, therapies targeting the inflammatory process could be helpful in the prevention of PC invasion and metastasis (38).
Conclusion
PC is the fourth leading cause of cancer-related death in Western countries. It has been estimated that within the next decade PC will become the second leading cause of cancer-related death in the USA and other Western countries. Therefore, non-invasive and accurate methods for early detection of PC as well as novel approaches to diagnosing PC in patients, such as the establishment of biochemical markers, are sorely needed to improve the management of PC patients. A variety of chemokines and their specific receptors have been suggested recently to distinctly contribute to tumour growth, dissemination and local immune escape in the pathogenesis of many malignancies, including PC. In our review, we performed a comprehensive literature search using the PubMed database to identify original articles that investigated whether chemokines and their receptors might play a role in PC. In summary, our review indicates potential significance of selected chemokines and their specific receptors in the progression of PC as well as in patient prognosis. However, little is known about serum levels of these proteins in PC patients and their diagnostic usefulness in the disease. Therefore, further investigations are needed to clarify the significance of chemokines and their receptors as potential candidates for tumour markers for PC.
Footnotes
Disclosures
Financial support: The present project was supported by the Medical University of Bialystok, Poland (N/ST/ZD/17/001/1198). BM is supported by funds from the Leading National Research Centre (KNOW).
Conflict of interest: None of the authors has financial interest related to this study to disclose.