
Abstract
Colorectal cancer (CRC) is one of the leading causes of cancer-related death. It is the second most frequently diagnosed malignancy in Europe and third worldwide. Colorectal malignancies diagnosed at an early stage offer a promising survival rate. However, advanced tumors often present distant metastases even after the complete resection of a primary tumor. Therefore, novel biomarkers of CRC are sorely needed in the diagnosis and prognosis of this common malignancy. A family of chemokines are composed of small, secreted proteins. They are best known for their ability to stimulate the migration of several cell types. Some investigations have indicated that chemokines are involved in cancer development, including CRC. This article presents current knowledge regarding chemokines and their specific receptors in CRC progression. Moreover, the prime aim of this review is to summarize the potential role of these proteins as biomarkers in the diagnosis and prognosis of CRC.
Introduction
Colorectal cancer (CRC) is considered a serious global problem since it represents the second most commonly diagnosed malignancy in Europe and third worldwide. 1 Recently, a marginal increase in its incidence has been observed in Central and Eastern Europe. 2 The global incidence and mortality rates are, in principle, lower for females than for males. 3,4 Unless genetically determined, CRC very rarely occurs in patients younger than 40 years. Therefore, the majority of screening programs are targeted at individuals older than 50 years. 1,5 Structurally, CRC is a highly heterogeneous disease which may occur in the rectum as well as the colon. 6 A tumor may develop in the right- or left-side of the colon, causing different systemic symptoms. Patients diagnosed with right-sided CRC usually complain of abdominal pain and weight loss. They may also experience occult gastrointestinal bleeding, confirmed by a positive fecal occult blood test, which often results in iron-deficiency anemia. 7 By contrast, left-sided colon cancer frequently produces symptoms such as overt bleeding from the lower intestine and a change in defecation rhythm, for example, diarrhea or constipation. 7 Tumor stage at the time of diagnosis is considered to be one of the most significant prognostic factors for this malignancy. The 5-year survival rate depends, among other factors, on the presence or absence of distant metastases. It ranges from 90% for early-stage disease without distant or regional metastases to 10% for advanced-stage cancer with distant metastases. 8
Risk Factors, Prevention, and Screening
Since there is no single, obvious cause of this malignancy, several risk factors in CRC development have been investigated. They have been divided into 2 groups: modifiable and nonmodifiable. Obesity, poor diet, tobacco or alcohol use, as well as a lack of physical activity are factors which can be modified. 9 The relationship between diet and CRC development has been investigated several times. It has been demonstrated that increased red meat consumption as well as a low fiber intake may raise the risk of developing CRC. 10 By contrast, a high intake of fish, green leafy vegetables, vitamin D, and calcium has been shown to have protective properties against CRC. 6,11 Other risk factors such as familial or personal history of CRC as well as colorectal polyps, Lynch syndrome, and the presence of type 2 diabetes are nonmodifiable factors. 11,12 However, the majority of cases with CRC are associated with an unhealthy lifestyle and therefore, in order to diminish the risk of CRC, it is recommended that the intake of red meat is reduced, excessive alcohol consumption avoided, and the duration and frequency of physical activity increased. 11,13 Factors contributing to an increase or decrease in CRC incidence are presented in Figure 1.

Diagnosis of CRC is a complex process involving a number of investigations. It normally commences with laboratory tests, including carcinoembryonic antigen (CEA) concentration determination. However, this marker is not sufficiently sensitive and specific and therefore, it is useful primarily in monitoring the treatment. Other important examinations in CRC diagnosis include a colonoscopy/sigmoidoscopy and imaging tests. Nevertheless, the final diagnosis is confirmed by histopathological examination, which is an invasive procedure. 8,14
Screening options for CRC used at present include several tests which have both advantages and limitations. However, the most important parameters of a test are diagnostic sensitivity and specificity, which define its accuracy. 15 Colonoscopy, which is currently the most sensitive method for CRC screening, is recommended every 10 years for individuals aged 50 years or older, who are considered an average-risk group for developing this type of cancer. 16 Importantly, the examination can detect both precancerous and cancerous lesions, which may be removed at the time of detection. 17 Another test is a semi-invasive sigmoidoscopy, which is similar to colonoscopy besides the fact that only the distal half of the colon is examined. However, it is performed less frequently. Computed tomography colonography, which does not require sedation, is another method used in CRC diagnosis. It can assist in detecting both proximal and distal lesions but does not offer the possibility of lesion removal. 9,17 Diet may also interfere with test results, for example, a high intake of vitamin C may provide false-negative results since it inhibits the activity of peroxidase used in FOBT, while hemoglobin found in red meat can lead to false-positive results. 17,18
Biomarkers for Early Diagnosis of CRC
Inherited mutations are responsible of approximately 20% to 30% of CRC. Due to next generation sequencing with potential future therapeutic implications, genomics of CRC has been recently under extensive investigation. The predictive significance of various blood cell ratios in CRC has been studied by many authors, who indicate the potential role of the fractional albumin rate (FAR = 100 × fibrinogen/albumin), fibrinogen to prealbumin ratio (FPR = fibrinogen/prealbumin), and the neutrophil–lymphocyte ratio (NLR) in early CRC. It is suggested that increased FAR, FPR, and NLR have been reported in early CRC in comparison to healthy controls in the prognosis and survival of patients with CRC. 19 Moreover, low lymphocyte–monocyte ratio (LMR) is related to more advanced and poorly differentiated disease, whereas high LMR was associated with early stages and improved overall survival. Some clinical investigations have indicated that the diagnostic utility of FAR and FPR was higher than NLR, and the combination of FPR, CEA, and CA19-9 could optimize the discrimination ability of CRC from benign disease, what may suggest that these biomarkers can be implemented for early diagnostics of patients with CRC. 19 However, due to the variety of patients’ population, analytical techniques, and timing of specimen collection, future studies are sorely needed.
Some clinical investigations have suggested the role of circulating tumor cells (CTCs) and circulating tumor DNA (ctDNA—cell-free DNA) as an noninvasive biomarkers for early diagnosis; ctDNA refers to small DNA fragments that are released by the tumor into the bloodstream and contribute complementary information for clinical decision. These potential biomarkers allowed for high-yield isolation directly from a small volume of unprocessed plasma. The assessment of CTCs and ctDNA-based liquid biopsies hold promise for early diagnosis of CRC, however their detection may not be widely adopted for routine practice until accuracy and reliability of these tests are validated on large, independent studies. 20
The analyses of methylation of the promoter of Septin9 DNA have been also suggested as biomarker for early diagnosis of CRC. The authors indicate the significance of detection of methylated Septin9 DNA using a qualitative assay for the polymerase chain reaction in the early detection of CRC. This stool-based test is useful in the discrimination between patients with CRC and healthy controls. 21 Moreover, the biomarkers of microsatellite instability has been also suggested as useful tools in the early diagnosis of CRC and may serve as screening markers for Lynch syndrome and detection of mutated DNA in stools. 22
Chemokines—General Informations
Chemokines are a family of small, structurally related proteins involved in many processes including angiogenesis 23 and lymphoid tissue development. 24 Their functional activity is induced by binding to specific G protein-coupled receptors, which are found on the surface of targeted cells. Research studies have revealed that one chemokine can bind to many receptors and one receptor may be activated by a number of ligands. 25 Approximately 50 chemokines and 20 chemokine receptors have now been acknowledged to be responsible for several aspects of intercell interactions. 26 Thus, they are known for inducing chemotaxis in a variety of cells such as lymphocytes, neutrophils, eosinophils, and fibroblasts. However, chemokines also play an important role in many pathological processes, including artherosclerosis, HIV infection, autoimmune diseases, and even cancer. 27,28 It has been indicated that some of these proteins may support tumor development and metastatic spreads via different mechanisms. 29
Structurally, chemokines have been divided into 4 subfamilies including CXC, CC, CX3C, and C. This classification is based on the position of N-terminal cysteine residues. 30 Moreover, the CXC group can be subdivided according to the presence or absence of the ELR motif, which is a sequence of 3 consecutive amino acids Glu-Leu-Arg. However, chemokines can also be classified as inflammatory, homeostatic, or dual function according to their function in the immune system and inflammatory response. 31 Homeostatic chemokines such as CC-chemokine ligand (CCL) 19 and CCL20 are produced constitutively. They participate in the migration and progression of various cells responsible for functioning of the immunological system. 32 By contrast, inflammatory chemokines such as CXC motif chemokine ligand (CXCL) 8 and CCL2 are produced by tissues and migrating leukocytes in response to bacterial toxins and proinflammatory cytokines, for example, interleukin (IL) 1 or tumor necrosis factor α (TNF-α). 33 Furthermore, they play an important role in cell activation, which promotes wound healing. 34 Chemokine receptors are structurally similar to chemokines. Their name is derived from the chemokine ligand with which they interact. They are divided into 4 groups: CXC chemokine receptor (CXCR), CC-chemokine receptor (CCR), CX3CR, and XCR. 35
Chemokines in Cancer
Inflammation is a multistep process associated with molecular and cellular alterations. 36 Previous investigations have demonstrated that controlled inflammation is a necessary process, which helps the body defend against various pathogens and repair damaged tissue, while uncontrolled inflammation is implicated in a number of pathological processes such as the development of neoplasms. 37 Inflammation has been acknowledged to be one of the features of many pathological processes including malignancies. Some studies suggest that chemokines may play a critical role in cancer. 38
Despite the fact that chemokines were initially recognized as important immune cell migration mediators, new evidence indicates that they are also involved in the biology of nonimmune cells, which play a significant role in tumor development, growth, and progression. 39 They coordinate all intercell interactions and thus exert a considerable impact on tumor promotion. 40 These chemotactic cytokines are able to induce cancer cell proliferation and survival in a number of ways. Research studies have demonstrated that tumor cells can acquire the ability to express chemokine receptors and produce chemokines which promote tumor growth. 41 Angiogenesis is an important step in tumor progression. Cancer cells acquire the ability to form new vessels from pre-existing blood vessels to deliver oxygen and necessary nutrients as well as to eliminate waste. This process is regulated by several angiogenic factors, lipids, and enzymes. 42 Many members of the chemokine superfamily may act proangiogenically by supporting the formation of new vessels, while others are angiostatic—responsible for inhibiting these activities. 43 It has been established that melanoma expresses several chemokines such as CCL2, CCL5, CXCL1, CXCL2, CXCL3, and CXCL8, which are associated with both tumor growth and progression. 44 In addition, CXCR4, normally not expressed on breast epithelial cells, is frequently found on breast cancer cells. 45 Some investigators have demonstrated that the CXC-chemokine/CXCR2 axis may promote tumor-associated angiogenesis in pancreatic cancer. They have demonstrated that the ELR+ CXC-chemokines concentrations are significantly higher in patients with cancer compared to healthy individuals. 46 The potential role of CXCL8, which is san angiogenic CXC-chemokine, in ovarian cancer biology has been investigated since its enhanced expression was observed in ovarian cancer cell lines. 47
Another important process in tumor progression is metastasis, which refers to the migration of malignant cells to areas distant from the site of a primary tumor. 48 Since the majority of cancer deaths are caused by distant metastasis rather than the excessive growth of a primary tumor, it is important to understand this multistep process in cancer biology as well as cancer treatment. 49,50 Metastasis comprises many independent processes and complex interactions including, inter alia, local invasion, tumor cell dissemination, colonization, and angiogenesis. 50,51 A number of studies have indicated that chemokines play a key role in metastasis. Tumor cells are able to express specific chemokine receptors which help to direct malignant cells to several anatomic sites to form metastases. 52 These metastatic sites start producing selected chemokines which attract CTCs to a supporting microenvironment. 53 The most thoroughly researched pair of proteins associated with metastasis is CXCR4 (CXC chemokine receptor 4) and its ligand CXCL12. It has been demonstrated that blocking this axis may suppress breast cancer lung metastasis. 24,54 However, its involvement in metastatic processes has also been observed in other cancers such as prostate cancer, lung cancer, and CRC. 55 -57
The Involvement of Chemokines and Their Receptors in CRC
A link between inflammation and cancer was suggested a number of years ago, based on the presence of inflammatory cells in tumor samples collected during biopsies. Furthermore, it was discovered that tumors frequently arise at sites of inflammation. 58 Since chronic inflammation is one of the key risk factors for CRC, it has been suggested that proinflammatory chemokines in particular may be involved in the development, progression, and metastasis of several types of cancer including CRC. 24 Evidence from a number of investigations demonstrates that selected chemokines and their specific receptors are involved in several stages of CRC development. However, the majority of the studies were based on the analysis of their expression levels in tissue samples. 59
CXCL12, also known as stromal cell-derived factor 1, and its receptor CXCR4 (fusin) have been recognized as a representative pair involved in cancer metastasis. 54 In the liver, which is the most common CRC metastasis site, CXCL12 is normally secreted by Kupffer cells and endothelial cells. 60 CRC cells are also capable of expressing this chemokine ligand, although the process is fairly controversial since the expression is bidirectional—tumor suppressive 61 and tumor promotive. 62 Clinical studies have revealed that in CRC, the expression of CXCR4 correlated with poor survival rates and liver metastasis. 63,64 In addition, the enhanced expression of this receptor has been observed under hypoxia via the activity of hypoxia-inducible factor 1-α. 65 Another receptor that interacts with CXCL12 is CXCR7, which has also been found to be expressed by CRC cells. Wang et al 66 assessed the expression of CXCL12, CXCR4, and CXCR7 in CRC and lung metastasis tissue samples and found that the expression of both CXCL12 and CXCR7 was significantly higher in metastasis samples in comparison to those of primary lesions. Moreover, significantly higher expression of CXCL12 was observed in lung tissue with malignant changes when compared to tissue with benign lesions. 67
Another important pair in CRC is CCL20 and its specific receptor CCR6. CCL20, also known as liver and activation-regulated chemokine or macrophage inflammatory protein-3a, has been found to be expressed in several human tissues. 68 It has been indicated that this molecule might be involved in neoplastic processes. The expression of this chemokine ligand has been detected, inter alia, in liver, and lung tissues but not in bone marrow or spleen. 69 -72 The CCL20 expression has been found to be elevated in both CRC and CR liver metastasis in comparison to non-malignant tissue. 73 Interestingly, CCR6 has been found to be overexpressed in CRC. Additionally, stimulation of its physiological ligand (CCL20) has been demonstrated to promote the proliferation and migration of this type of cancer in in vitro studies. 74 Some studies have revealed that CCR6 expression is significantly higher in both CRC and CR liver metastases. 75 -77 Hu et al 78 demonstrated elevated CCR6 expression in CRC, but it was strongly linked with distant metastases to either lung or liver. However, it was also revealed that the observed overexpression was not organ-specific and thus there was no differentiation between lung and liver metastases. Significantly, research performed by Dellacasagrande et al 79 demonstrated that higher CCR6 expression was observed in small CRC metastatic tumors in comparison to the surrounding tissue, which suggests the impact of this receptor on the development of liver metastases. Conversely, lower CCR6 expression has been observed in large, existing metastatic tumors in comparison to primary tumors, which might imply that the expression of this receptor is not required by the CRC cells which have already formed distant metastases. 80
Another extensively researched receptor is CXCR3 (CXC chemokine receptor 3), which has been found to be expressed on several cells including CRC cells. 57 The receptor was found to promote metastases to lymph nodes when both ligands for the receptor–CXCL9 (CXC motif chemokine 9) and CXCL10 (CXC motif chemokine 10)—were expressed at elevated levels. 81 In addition, some studies have revealed that at stage II or/and stage III of CRC, the expression of CXCL10 can be considered an independent prognostic factor for cancer recurrence, 82 while other researchers have demonstrated that the coexpression of both CXCR3 and CXCL10 in CRC is linked to poorer prognosis and metastatic recurrence. 83 In addition, elevated CXCL10 levels in the sera of patients with CRC have been found to be associated with advanced stages of the disease. Furthermore, the same study identified increased serum CXCL10 concentration as well as the presence of distant metastases as independent factors of poor prognosis. 84
CXC motif chemokine 8, also known as IL8, is a factor responsible for granulocyte activation in immune responses during inflammation. Some authors suggest that the expression of CXCL8 is regulated by various stimuli such as steroid hormones (eg, oestrogens and androgens), environmental and chemical stress (eg, hypoxia), as well as inflammatory signals (eg, TNF-α). 85 It has been proven that this protein plays a key role in cancer invasion, progression, angiogenesis, and metastasis formation. 86 CXCL8 has been reported to be linked with metastatic potential. 87 Its specific receptor—CXCR2 (IL8 receptor β) may promote angiogenesis via interaction with ELR + CXC chemokines such as CXCL5 (CXC motif chemokine 5), CXCL2 (CXC motif chemokine 2), and CXCL1 (CXC motif chemokine 1). 88 In a knockout mouse model of tumor microenvironment, a lack of the CXCL8-CXCR2 axis has been observed to act against CRC growth and distant metastases. 89 In addition, CXCR1 and CXCR2 antagonists have inhibited CRC metastasis through the induction of tumor cell apoptosis. 90 The elevated serum concentration of chemokine CXCL8 has been found to be associated with advanced stages of CRC as well as the presence of distant metastases. 91
Serum concentrations of CXCL5 (CXC motif chemokine 5) were assessed by Yildirim et al who demonstrated that in patients with CRC, the level of the chemokine was significantly higher in comparison to healthy volunteers. 92 The study also evaluated the diagnostic sensitivity and specificity of CXCL5. However, due to the statistically insignificant results obtained, CXCL5 cannot be recognized as a potential marker in CRC screening. Matsushita et al 93 studied the concentrations of CXCL15 (CXC motif chemokine 15) in the sera of patients with CRC and discovered that serum CXCL15 levels were elevated in the cancer group in comparison to healthy controls. The concentrations increased with disease stage and correlated with poor survival. The chemokines as well as their specific receptors involved in CRC have been presented in Table 1.
Chemokines and Their Receptors Involved in CRC.
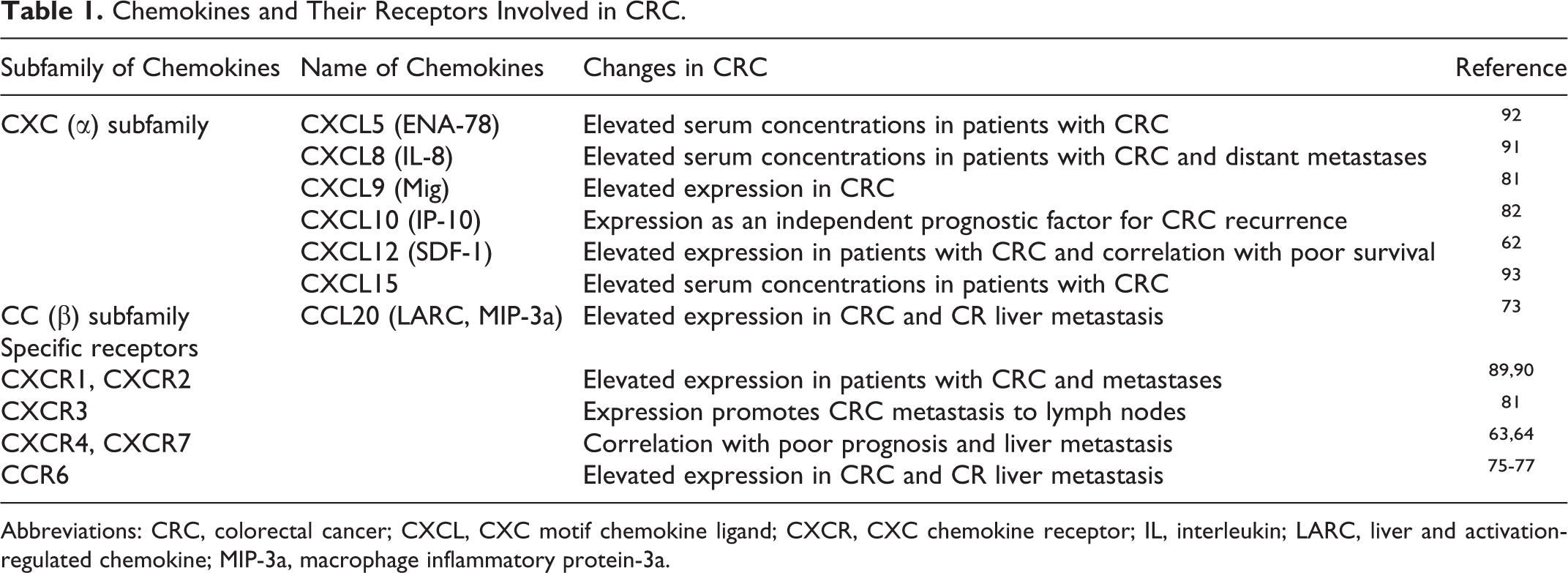
Abbreviations: CRC, colorectal cancer; CXCL, CXC motif chemokine ligand; CXCR, CXC chemokine receptor; IL, interleukin; LARC, liver and activation-regulated chemokine; MIP-3a, macrophage inflammatory protein-3a.
The potential utilization of serum chemokines in targeted cancer therapy has been evaluated by a number of researchers, 94,95 but there is scant knowledge regarding serum concentrations of selected chemokines as biomarkers in the diagnosis of CRC.
Conclusions
Colorectal cancer has been the focus of worldwide research efforts. The thought-provoking, stable incidence rate of CRC as well as a great number of CRC-related deaths each year necessitate the enhancement of diagnostic and screening methods. Chemokines play a critical role in a number of both physiological and pathological processes, including tumor development and progression. Recently, a number of chemokines and their receptors have been suggested to be involved in CRC. As presented in this review, the expression of several chemokines is enhanced in CRC. Published research results indicate that the increased expression of selected chemokines and/or their specific receptors is linked to poorer prognosis and metastatic recurrence. Moreover, elevated levels of these proteins have been demonstrated to correlate with the advanced stage of the disease and poor survival rates of patients with CRC. Chemokines and their specific receptors have been suggested as potential tumor markers but more research investigating serum levels of these proteins is needed.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.