
Abstract
Introduction
Systemic lupus erythematosus (SLE) is an autoimmune and multisystemic inflammatory disease.1–3 The etiology of SLE remains unknown, and its clinical and laboratory manifestations exhibit significant variability, leading to diverse clinical courses and prognoses among patients. 4 Various risk factors have been identified as predisposing factors for inflammation and immune system stimulation. Genetic factors also play a role in the development of SLE.
Hormones, such as estradiol, progesterone, and prolactin, have been implicated in the occurrence and severity of SLE.1,5–7 SLE predominantly affects women of reproductive age, with approximately 80% of cases occurring in this population, particularly within the 20-40-years age group. Women are nine times more likely to be affected than men in this age range. Menstrual disorders, encompassing a range of abnormalities such as prolonged menstrual cycles, oligomenorrhea, amenorrhea, and temporary persistent amenorrhea, are relatively common among patients with SLE.8,9
Several studies have investigated the relationship between menstruation and autoimmune diseases, particularly SLE. In a prospective study of 36 patients with SLE who did not receive cyclophosphamide, menstrual changes were observed in 7.52% of cases, with SLE activity identified as a significant risk factor for menstrual changes in patients not treated with alkylating drugs. 9 Antimalarial drugs, including hydroxychloroquine, have been shown to alleviate mild disease manifestations, such as skin lesions, arthritis, and physical symptoms. Reduced consumption of hydroxychloroquine has been associated with increased disease recurrence, organ damage, and poor prognosis and survival rates.10–12 Corticosteroids are considered a mainstay of SLE treatment, effectively controlling mild symptoms or involvement of vital organs.13,14 Immunosuppressants, widely used in SLE treatment, exert suppressive effects on the immune system through multicellularity and induction of apoptosis in immune response cells. This action can extend beyond the immune system, affecting other organs, including the female reproductive system. 15 A study by Rodrigues et al. found a higher prevalence of menstrual changes in lupus patients compared to the general population, with a significant association between menstrual changes and the use of immunosuppressive agents in these patients. 16 Another study by Fatnoon et al. reported a higher risk of menstrual irregularities in patients treated with cyclophosphamide. 8
Understanding the prevalence of menstrual disorders in SLE and their relationship to clinical parameters is important for patient-centered management. Previous studies have shown that menstrual disturbances may influence quality of life and reproductive planning in women with SLE.9,17,18 Studying the association between menstrual disorders and specific treatments allows healthcare professionals to make informed decisions, minimizing adverse effects on reproductive health. Addressing the specific needs of patients with menstrual disorders further improves overall well-being and quality of life for individuals with SLE. This study aimed to determine the prevalence of menstrual disorders in patients with SLE and evaluate their association with immunosuppressive medications and disease activity (SLEDAI-2K).
Patients and methods
Study subjects and design
This cross-sectional pilot study was conducted from June 2022 to March 2023 at the Rheumatology Clinic, Golestan University of Medical Sciences, a tertiary care center in Iran. A total of 58 patients were initially recruited for this cross-sectional pilot study. Participant selection is summarized as follows: 68 individuals were screened, 58 were enrolled, and 50 were analyzed after exclusion of eight postmenopausal women. As this was a pilot study, no formal sample size calculation or power analysis was performed; all eligible patients meeting the inclusion criteria during the study period were consecutively enrolled. Participants were consecutively recruited from the rheumatology clinic of our tertiary center, comprising female patients with SLE (aged 16–51 years) who met the ACR/SLICC classification criteria and were willing to participate. Diagnosis and classification of SLE were based on the 2012 Systemic Lupus International Collaborating Clinics (SLICC) criteria, 19 a widely accepted classification scheme. However, 8 patients were subsequently excluded from the analysis due to their menopausal status, resulting in a final sample size of 50 patients. The inclusion criteria were patients with SLE who had a diagnosis of SLE, were referred to the medical department conducting the study, and were both eligible for and willing to participate in the cross-sectional pilot study. Additionally, exclusion criteria included patients without confirmed SLE diagnosis, male patients, postmenopausal females, known autoimmune or endocrine disorders affecting menstruation such as thyroid disease, polycystic ovary syndrome, premature ovarian failure (POF), and hyperprolactinemia, pregnant or breastfeeding patients, those declining participation, and patients unable to provide written informed consent.
Female patients diagnosed with SLE who were referred to our medical center and met the criteria for participation in the study were asked to complete a questionnaire assessing lupus disease activity, as measured by the Systemic Lupus Erythematosus Disease Activity Index (SLEDAI-2K).2,8,9,20,21 The menstrual disorder questionnaire was not formally validated but was adapted from previously used tools for similar studies. The questionnaire included items on dysmenorrhea, polymenorrhea, and menorrhagia, with definitions aligned with standard clinical criteria (dysmenorrhea: painful menstruation occurring for ≥50% of cycles over the past year; polymenorrhea: cycles <21 days; menorrhagia: excessive bleeding requiring sanitary product change every 2 h). The items were adapted from the Menstrual Symptom Questionnaire (MSQ) used in prior SLE studies 9 and the Menstrual Distress Questionnaire (MDQ). 22 The adapted items are based on non-copyrighted, publicly available instruments, and no formal permission was required. The full questionnaire is provided as Supplement Material 1. Activity categories have been defined based on SLEDAI-2K scores: no activity (SLEDAI-2K = 0), mild activity (SLEDAI-2K = 1 to 5), moderate activity (SLEDAI-2K = 6 to 10), and severe activity (SLEDAI-2K = 11 to 19). The questionnaire included specific inquiries about symptoms related to menstrual disorders. Disease activity was scored by rheumatologists using the SLEDAI-2K version. 23 Patients did not self-score disease activity; questionnaires addressed menstrual disorder symptoms only. Additionally, information regarding the classification and duration of medications used for SLE management since the time of diagnosis was recorded.
Efforts to minimize bias included consecutive recruitment, standardized questionnaires, and uniform timing of blood sampling (day 3–5 of the cycle where feasible). Missing data for hormonal values or medication doses were excluded listwise without imputation. Furthermore, a venous blood sample was obtained from each participant to evaluate levels of follicle-stimulating hormone (FSH), luteinizing hormone (LH), and anti-Mullerian hormone (AMH).
The reporting of this study conforms to the STROBE guidelines. 24 The completed STROBE checklist is provided as Supplement Material.
Statistical analysis
After assembling the study participants’ information, the data were entered into SPSS software version 16 and the information was summarized and reported in tables and statistical charts. Regarding the measured hormones, the distribution of the variables was checked using the Kolmogorov-Smirnov test, and due to abnormal distribution, the non-parametric Mann-Whitney test was used to check their correlation with menstrual disorders. To investigate the relationship between the variables, the chi-square test was used for qualitative data with menstrual disorders. The distribution of SLEDAI categories was uneven (5 severe vs 45 mild/moderate cases). Given the small sample size in the severe category, the Chi-square test may not have been appropriate for detecting associations. Future studies should use more balanced groups or alternative statistical methods, such as Fisher’s exact test or logistic regression. In addition, the significance level of the study was considered to be 0.05.
Ethical approval and consent to participate
The study and all experimental protocols were approved by the Professional Ethics Committee of the Golestan University of Medical Sciences with the ethical code of ir. goums.rec.1396.85. Written informed consent was obtained from all patients for the implementation of this project. This study was conducted in accordance with the Declaration of Helsinki (1975), as revised in 2024.
Results
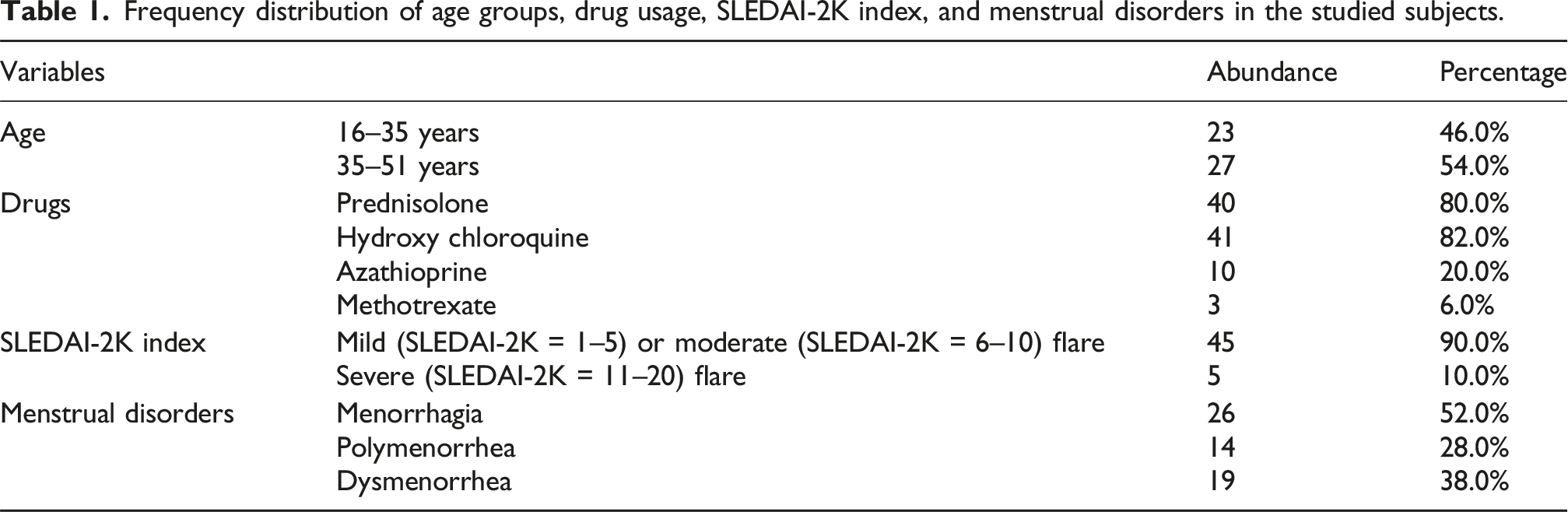
The study included 50 female patients diagnosed with SLE. The median age was 35–40 years (SD = 8.88) with patients divided into 16-35 years (n = 23, 46%) and 36–51 years (n = 27, 54%) age groups.
Frequency distribution of age groups, drug usage, SLEDAI-2K index, and menstrual disorders in the studied subjects.
Frequency distribution (%) and counts of dysmenorrhea, polymenorrhea, and menorrhagia according to age, medication use, and SLEDAI-2K category. Percentages are column-based within each disorder category; p-values correspond to Chi-square tests. Missing values in some categories are due to incomplete data or non-response. Missing values in some categories are due to incomplete data or non-response.

Hydroxychloroquine users had a higher prevalence of menstrual disorders, including dysmenorrhea (94.7% vs 85.7%), but this difference was not statistically significant (p-value = 0.066). Conversely, the azathioprine group showed a numerically lower frequency of menstrual disorders. This discrepancy may be due to sample size limitations and requires further investigation in larger studies.
Mild disease activity (SLEDAI-2K index 1–5) occurred in 28 patients, moderate activity6–9 in 17 patients, and severe activity10–19 in five patients.
Mean, standard deviation, and standard error of FSH, LH, and anti-mullerin hormone according to dysmenorrhea, polymenorrhea, and menorrhagia, respectively.

Prednisolone usage showed an association with higher dysmenorrhea prevalence in this pilot cohort, although causality cannot be inferred. Dysmenorrhea was observed to be more frequent in the older group (36–51 years) with a prevalence of 63% compared to 39% in the younger group (16–35 years). However, this difference was not statistically significant (p-value = 0.15), suggesting that age may not be a strong predictor of dysmenorrhea in this population. Also, no patient had received cyclophosphamide in the last 2 years; four patients had historical use and were excluded from hormonal analyses.
Discussion
The purpose of this study was to investigate menstrual disorders in patients with SLE. Although prior studies have examined menstrual disorders in SLE, this pilot study uniquely evaluates concurrent hormonal profiles (FSH, LH, AMH) alongside medication use, providing granular insights despite its modest sample size. The distribution of the frequency of dysmenorrhea, polymenorrhea, and menorrhagia in the studied subjects was assessed according to the age groups. Dysmenorrhea appeared numerically more frequent among participants aged >35 years, consistent with previous reports,8,16 though this difference did not reach statistical significance. In a 2008 study, Fatnoon et al. 8 investigated the prevalence and types of menstrual disorders in patients with SLE and identified the factors that cause them to develop. The mean age and standard deviation for the study group were 33.23 ± 10.96 years. The prevalence of menstrual irregularities was 49% with a higher risk in the older age group (more than 30 years old) and those who used cyclophosphamide, especially if the dose was more than 10 g. Like these results, disorders in our study occurred more in the older age group, with no statistically significant relationship. Previous studies, including Pasoto et al. 9 and Mandal et al. 17 have reported associations between corticosteroid use and menstrual disturbances, supporting our observed trends. Although statistical significance was not reached, dysmenorrhea, polymenorrhea, and menorrhagia were numerically more frequent among Hydroxy chloroquine and prednisone users compared to Azathioprine users, suggesting possible clinical relevance.
We investigated the distribution of the frequency of dysmenorrhea in the studied subjects according to the use of prednisolone, and in the subjects with dysmenorrhea, the frequency of prednisolone users was significantly higher compared to non-users of prednisolone (94.7% vs 5 3.3%), and statistically, there was a significant difference between the two groups, while there was no difference between the two groups in the case of polymenorrhea and menorrhagia. Similar to these results have been obtained in Pasoto et al. study 9 which showed the prevalence of menstrual cycle disorders and clinical, hormonal, and therapeutic dependencies in patients with SLE. Azathioprine usage was not associated with menstrual cycle disorders. The percentage of commonly used prednisone (p-value = 0.3), the average dose (p-value = 0.062), and the percentage of patients with high doses (≥30 mg/day; p-value = 0.09) were comparable in patients with or without menstrual alterations.
In our study, the distribution of the frequency of dysmenorrhea, polymenorrhea and menorrhagia according to the consumption of hydroxychloroquine was investigated, and the frequency of these menstrual disorders was significantly higher in hydroxychloroquine users, with no significant difference between the two groups. The frequency distribution of dysmenorrhea, polymenorrhea and menorrhagia in the studied subjects was investigated according to the usage of Azathioprine, and in the subjects with these disorders, the frequency of hydroxychloroquine users was lower compared to non-users, however there was no significant difference between the two groups.
Mandal et al. 17 conducted a study about the association between menstrual disorders and SLE. They examined a study population with SLE and identified several factors related to abnormal menstrual cycles, including higher SLEDAI-2K scores, longer disease duration, elevated thyroid-stimulating hormone (TSH) levels, higher levels of LH and prolactin, altered ovarian Doppler parameters, and higher cumulative dose of steroids. Like our study, they highlighted the presence of menstrual disorders in patients with SLE and suggested multiple factors, including medication usage and disease activity, as potential contributors. Further research is needed to better understand the underlying mechanisms and optimize management strategies for menstrual disorders in patients with SLE. Age at menarche and its potential influence on current menstrual dysfunction were not assessed, which could be a confounding factor.
Overall, similar to our results, prior studies imply that both immunosuppressive medication exposure and disease activity may jointly influence menstrual patterns.25,26 Because we did not formally test interaction terms between SLEDAI and medication use, attributing menstrual changes solely to drug effects would be premature.
The study by Pasoto et al. 9 evaluated 36 patients with SLE without alkylating therapy and aimed to determine the prevalence of menstrual disturbances and their associations with clinical and hormonal factors. The findings revealed that disease activity, measured by SLEDAI-2K scores, was significantly higher in patients with irregular cycles. Interestingly, the use of azathioprine, another SLE medication, was not associated with menstrual disturbances. Overall, this study showed an association between prednisolone use and dysmenorrhea but no significant association with polymenorrhea or menorrhagia.
Dejan Rodrigues et al. 16 found a significant relationship between menstrual changes within the usage of immunosuppressive agents. Similar to what has been observed in other publications on SLE treatment, the frequency of menstrual changes was higher in these patients compared to the general population. The higher frequency of menstrual changes in patients with SLE was remarkably dependent to the usage of the immunosuppressive agents. Similar to these results, the cases of menstrual disorders in our study were more in patients with other medications application, but there was a considerable correlation only in the case of dysmenorrhea and the use of prednisolone.
In addition, the distribution of the frequency of dysmenorrhea, polymenorrhea and menorrhagia in our studied subjects was investigated according to the SLEDAI-2K index, and the frequency of subjects with mild or moderate flare activity was higher than those with severe flare, but statistically there was no significant difference between the two groups. In the study of Pasoto et al. 9 the mean levels of SLEDAI-2K (p-value = 0.02) and the frequency of patients with SLEDAI-2K ≥8 (p-value = 0.008) were higher in patients with irregular cycles, while in our research, dysmenorrhea, polymenorrhea and menorrhagia were more in the group with mild or moderate flare activity, which could be related to the larger number of these cases.
Also, in our study, the mean, standard deviation, and standard error of FSH, LH, and AMH values were examined according to the presence or absence of dysmenorrhea, polymenorrhea, and menorrhagia, and the mean values were not significant in any of the cases among the two groups. In this regard, J Mayorga and his colleagues evaluated the prevalence of POF and its related factors in patients with SLE and did not find any significant relationship between POF and autoimmune endocrine diseases. Also, in the study of Shabanova et al. 18 regarding the investigation of ovarian function and disease activity in patients with SLE, they concluded that the increase in FSH and LH values was seen only in a small number of patients with menstrual disorders.
It is noteworthy that the majority of the aforementioned studies corroborate each other’s findings, indicating consistency in the reported results. However, it is important to acknowledge that the observed differences among these studies may stem from variations in study design and the specific drug regimens investigated in each study.
Although prednisolone usage was associated with dysmenorrhea, it is important to emphasize that this study is cross-sectional and therefore cannot establish a causal relationship. The observed association should not be interpreted as a definitive cause-and-effect link, and further prospective studies are needed to test such mechanisms.
Study limitations
This study has several limitations. The sample size was modest and drawn from a single tertiary center, which may limit the generalizability of our findings to other geographic and clinical settings. Participants were predominantly of Middle Eastern descent, and ethnic variation may affect hormonal profiles and SLE manifestations. Known cross-ethnic differences in SLE disease severity and medication response should be considered when interpreting the findings, as the generalizability of the results to non-Middle Eastern populations may be limited. While we excluded postmenopausal women, it is important to note that some perimenopausal women may have hormone values that do not reflect those of younger women. This could introduce bias in our hormonal assessments, and stratification by menopausal status could have helped to reduce this potential source of confounding. As a pilot study, no formal sample size calculation or power analysis was performed, and the cross-sectional design restricts causal inference regarding medication effects. Recall bias may have influenced responses to the menstrual questionnaire, as data relied on patient self-reporting. Measurement bias is possible because hormonal assays were not repeated across cycles. Although hormonal measurements were obtained between day 3 and day 5 of the menstrual cycle for most patients, precise cycle phase documentation was not available for all, potentially affecting hormone level interpretation. Uncontrolled confounding factors such as disease duration, cumulative steroid dose, and comorbidities may also have influenced the observed associations. These limitations should be considered when interpreting the results. No post hoc power or sensitivity analysis was performed; thus, the study may have been underpowered to detect modest associations, particularly for non-prednisolone drugs or hormone variations. All non-significant results should therefore be viewed as preliminary.
Conclusion
This cross-sectional study found a significant association between prednisolone use and dysmenorrhea in women with SLE. The higher frequency of dysmenorrhea in prednisolone users versus non-users suggests these medications may contribute to menstrual disorders in some patients. However, given the study design, it is difficult to ascertain a definitive causal relationship due to limitations in controlling for potential confounding factors. Other variables like age, disease severity, and use of other medications may impact dysmenorrhea risk. Additionally, the sample size of 50 patients with SLE from a single center may limit generalizability. Further research using larger sample sizes, prospective cohorts, and controlled analyses is warranted to better characterize the effects of glucocorticoids and immunosuppressants on menstruation in SLE. While an association exists, disease duration at the time of recruitment was not systematically recorded, which may influence menstrual patterns and medication effects. Making firm conclusions about prednisolone as the sole driver of dysmenorrhea in this population is difficult given the inability to fully account for confounding variables in this preliminary study.
Supplemental material
Supplemental Material - Menstrual disorders in systemic lupus erythematosus patients; A cross-sectional pilot study
Supplemental Material for Menstrual disorders in systemic lupus erythematosus patients; A cross-sectional pilot study by Hedieh Nirouei, Alireza Fatemi, Nafiseh Abdolahi, Mehrdad Aghaei, Mahboubeh Azaderah, Yasmin Yazdooei in European Journal of Inflammation.
Footnotes
Acknowledgment
Special thanks to all the fellow authors who contributed to this article.
Ethical considerations
The study and all experimental protocols were approved by the Professional Ethics Committee of the Golestan University of Medical Sciences with the ethical code of ir. goums.rec.1396.85.
Consent to participate
The informed consent was also obtained from all patients for the implementation of this project. All methods were performed in accordance with the relevant guidelines and regulations. Written informed consent was obtained from all subjects before the study.
Authors contribution
H.N: Design of the work and Manuscript writing.
A.F., and Y.Y: Manuscript writing and Data entry.
M.A., and N.A.: Data interpretation and substantial manuscript revision.
M.Az.: Gynecological assessment.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data supporting the findings of this study are available from the corresponding author, but restrictions apply to the availability of these data, which were used under license for the current study, and are therefore not publicly available. However, the data is available in the form of an Excel file from the authors upon reasonable request and with the permission of Alireza Fatemi.
Trial registration
This randomized clinical trial was not registered because it was not a randomized clinical trial.
Role of the Funder/Sponser
The funder had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Guarantor
Alireza Fatemi.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.