
Abstract
Keywords
Plain language summary
Patients’ voices: what patients with Crohn’s disease and ulcerative colitis have to say and recommend to their doctors
Inflammatory Bowel Diseases (IBD), which include Crohn’s disease and ulcerative colitis, are chronic conditions causing ongoing intestinal inflammation. These diseases significantly affect patients’ quality of life, emphasizing the importance of the relationship between patients and their gastroenterologists. A recent qualitative study aimed to explore what IBD patients expect from their treating doctors.
The study involved 36 patients—19 with Crohn’s disease and 17 with ulcerative colitis. It used the DIPEx method, developed by the Health Experiences Research Group at Oxford University, to conduct in-depth interviews. Researchers analyzed these interviews to uncover common themes and expectations.
Patients highlighted three main areas as crucial: the expertise of doctors, the quality of the patient-doctor relationship, and the efficiency of healthcare organization. They stressed the need for doctors to have a thorough understanding of IBD and its symptoms, and to provide personalized care that addresses the specific needs and concerns of each patient. Respectful treatment, sensitive handling of potentially embarrassing situations, and fostering trust were identified as key elements of a good patient-doctor relationship.
Additionally, patients valued having sufficient time during medical appointments and emphasized the importance of including mental health support as part of their treatment. The ability of doctors to establish a professional yet friendly rapport was also considered essential for managing the unpredictable nature of IBD.
The study concludes that a collaborative, respectful patient-doctor dynamic is crucial and calls for systemic healthcare changes to better support this approach. It underscores the importance of listening to patient voices to enhance the effectiveness of care in managing IBD, advocating for personalized treatment plans and a more patient-centered healthcare system.
Introduction
Inflammatory bowel diseases (IBD) represent a diverse variety of chronic inflammatory intestinal conditions, with two major types: ulcerative colitis (UC) and Crohn’s disease (CD). The chronic nature of IBD impacts the lives of patients. 1 Key symptoms include pain, diarrhoea, stool urgency, high frequency, incontinence, passing of blood and mucus, flatulence, weight loss, and fatigue. Impacts on daily activities, social and leisure activities, treatment, and psychological effects are described in a conceptual model of the burden of IBD. 2 In the Czech Republic, the overall prevalence of patients with a history of IBD is approximately 98,000, with 27,977 patients with CD and 28,430 patients with UC receiving medical care. 3
The quality of life of patients with IBD is lower than that of the healthy population, both among adults and children. Additionally, during periods of active disease, quality of life deteriorates even further.4,5 In recent years, the role of healthcare providers, particularly treating gastroenterologists, has become increasingly recognised as a factor that significantly influences patients’ well-being. 6 Patient-centred personalised medicine models are more effective.7,8 As medication adherence is a concern in IBD care, 9 the focus on patient participation and shared decision-making has been proven to reduce non-adherence to treatment. 10 However, patients and their gastroenterologists may have differing perceptions of the quality of care.8,11
Previous research has highlighted that effective communication between IBD patients and their healthcare providers is crucial for improving patient outcomes and quality of care. Studies have shown that when healthcare providers engage in clear, empathetic communication and involve patients in shared decision-making, it can significantly enhance patients’ satisfaction with care and adherence to treatment plans.12–14 For instance, patients who feel heard and understood by their doctors are more likely to trust their healthcare providers and follow medical advice. 15 Additionally, shared decision-making in gastroenterology can improve the quality of care and patient satisfaction by enhancing communication and fostering a collaborative treatment approach between patients and providers.16–18 These findings underscore the importance of fostering a collaborative doctor-patient relationship to meet the complex needs of IBD patients. The Ulcerative Colitis Narrative Global Survey, a comprehensive international study conducted by Rubin et al. across multiple countries, identified gaps in optimal care, particularly in areas such as the need for more information at the initial diagnosis and better emotional support from physicians. 19
This study aimed to investigate the personal experiences of IBD patients with their treating physicians. By analysing these patients’ perspectives, this study aimed to gain insights into the communication dynamics and specific areas of improvement identified by patients within the context of collaborative and integrated models of care in IBD treatment.20,21 The focus is on understanding patients’ expectations, preferences, and suggestions to enhance the doctor-patient relationship in the context of IBD care. By highlighting these insights, this article aims to contribute to understanding effective doctor-patient communication and inform strategies for improving the quality of care provided to individuals with IBD.
Materials and methods
The data presented in this article represent a subgroup of data from a broader study focusing on patients’ experiences: “Health Talk Czech – Experiences With IBD” supported by Palacky University [IGA_CMTF_2023_002]. This study analysed the messages and recommendations given to medical professionals. Owing to the qualitative nature of the research, the results show the original representative quotes of patients.
Design
From May 2017 to April 2023, 36 in-depth, semi-structured interviews were conducted with 19 patients with Crohn’s and 17 patients with ulcerative colitis living in the Czech Republic. The study was carried out using the Database of Personal Experiences of Health and Illness (DIPEx) method developed by the Health Experiences Research Group at the University of Oxford. This database thoroughly analyses narrative interviews of people with particular conditions chosen to represent the broadest range of experiences. 22
The DIPEx methodology, with its solid grounding in rigorous qualitative research, provides access to an “increasingly rare commodity: diversity of perspective and experience.” 23 The research methodology has expanded to 14 countries and was standardised also for the Czech Republic. 24 This design is used to study the experiences of people with various illnesses and disabilities.25,26 DIPEx studies aim to inform patients, educate healthcare professionals, and offer a patient-centred perspective to researchers and those who manage health services. 27
Researchers and other professionals
Numerous researchers have collaborated on various aspects of the projects. The main interviewer (HB), who specialises in the psychological well-being of patients with IBD, conducted most of the interviews. One student conducted seven interviews under supervision. The data analysis was led by HB and KG (a social worker experienced in social health research) alongside ZZ (a gastroenterologist) and ZM (a psychotherapist). All researchers were trained in qualitative research and had no prior relationships with the participants. Participants were informed about the researchers’ professional backgrounds and the study’s objectives, but no personal goals or motivations for conducting the research were disclosed. An academic supervisor (PT), well-versed in psychology and health research, meticulously reviewed the data and provided guidance to ensure rigour. The authors were 3 females (all three PhD, one MD) and 2 males (ZM – PhD, PT – prof.) Medical supervisors, including three gastroenterologists and one IBD nurse, supported the project’s validity. Advisory Panel meetings were convened on three occasions throughout the project. During these meetings, researchers and medical supervisors engaged with additional experts from the patients’ organisations and two patients to ensure a comprehensive perspective.
Data collection
Participants were recruited through organisations working with the target group (Pacienti IBD, ILCO – Voluntary Association of Ostomies), Advisory Panel, and support groups, including virtual communities on social networks. Purposive sampling was based on two key concepts: maximum variation and theoretical saturation. Participants included in the study were adults aged 18 and above with a confirmed diagnosis of Inflammatory Bowel Disease (IBD), specifically Crohn’s Disease or Ulcerative Colitis, living in the Czech Republic. They had to provide written informed consent and be able to speak and understand Czech. Exclusion criteria involved individuals with major comorbidities that could influence their IBD experiences, those unable to communicate effectively due to cognitive impairments or severe physical illness, and any potential participants who did not provide informed consent. Furthermore, participants were purposively selected to fulfil the requirements of a maximum variation sample. Maximum variation involved identifying variables that could impact the experience (such as age, gender, region, size of the town/village, living arrangement, family background, condition-specific factors, etc.) and ensuring these variations are represented in the sample. Maximum variation was defined before the data collection in accordance with the DIPEx methodology.28,29 IBD-specific factors were determined based on a literature review and discussions with experts from the Advisory Panel. These factors include different stages of the disease, different medications and treatments, age, age at diagnosis, and distance of residence from the gastroenterology medical facility.
Theoretical saturation in the study was reached when no additional issues or insights were identified, and data began to repeat, making further data collection redundant and indicating that an adequate sample size had been reached. This saturation was evaluated after achieving maximum variation and continuously assessed during data collection and analysis.
Part of the interview guide related to messages or recommendations.

Data analysis
The interviews were digitally recorded (in audio or video format according to the participant’s preference), then transcribed verbatim and checked for the correctness of the transcription; the anonymised transcripts were then sent to the participant for approval. The participants could clarify the details or delete part of the interview. All participants provided written informed consent to use the data for research.
The data were then coded systematically using NVivo12 software. Five transcripts were first coded independently by two researchers to develop a coding framework, and the framework was then discussed with the entire team and modified according to the comments received. After the coding framework was established, researchers coded the remaining transcripts. Cross-coding was performed on the first five interviews as well to ensure reliability. This approach allowed us to refine the coding framework collaboratively. When a new theme emerged, the previous transcripts were re-examined to ensure the theme was not missed. Throughout the study, all changes and decisions in the coding process were meticulously documented in a shared coding diary, providing transparency and traceability. Thematic analysis was applied, incorporating constant comparison and exploration of deviant cases.30,31 These included emergent and anticipated themes, which were then categorised. The categories were combined into individual topics using a thematic analysis. For the purpose of this manuscript, the “one sheet of paper” (OSOP) technique was used, 22 in which the researchers analysed all sections of data that fall under the codes “messages” and “recommendations.” The researchers wrote relevant data on a piece of paper with the participant’s ID. Common elements and differences were then searched. Each theme was defined and named to capture the essence of the data it represented. The team worked collaboratively to ensure the themes and definitions were clear and accurately reflected the data. For instance, when a participant expressed concerns about care availability, it was coded as “availability.”
The final step involved weaving together the thematic analysis into a coherent narrative. For example, themes labelled as “availability,” “changing doctors,” “seeking care,” “geographical distance”, and similar were combined into the chapter “Access to care” and described. This included selecting vivid, compelling quotes from the participants to illustrate each theme and ensuring a clear, logical flow in the presentation of findings.
The interviews and analyses were conducted in the Czech language. The results were then translated into English for the purpose of this manuscript (the DeepL translator was used for translations).
Results
Sample description
Sociodemographic factors.
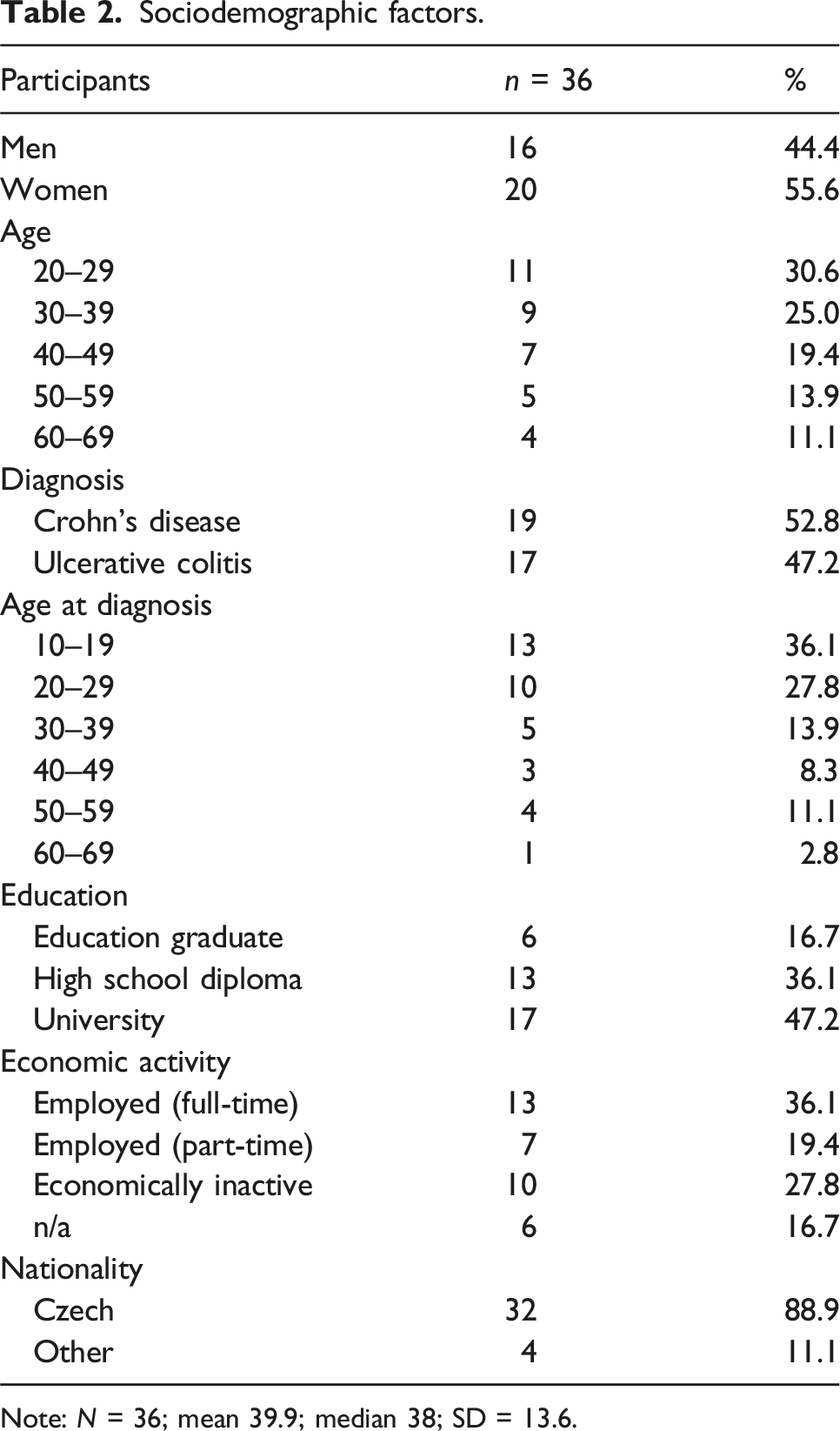
Note: N = 36; mean 39.9; median 38; SD = 13.6.
Findings
Results – patients’ recommendations and messages to physicians.

Expertise
Information and explaining
Participants’ recurring requirement for information directly from their medical practitioners was consistently underscored. This necessitates maintaining professionalism to impart essential information to patients regarding their medical status and subsequent treatment.
Information, information, information… (participant 02)
To get maximum information from my doctor. (participant 33)
Patients expressed a desire for healthcare professionals to respond without irritation when they posed questions that might seem unrelated or trivial.
Also, the important thing is not to get angry if the patient asks stupid questions. Or bullshit, from the medical perspective. Patients don’t have the education. They need to know the details. (participant 22)
The need for relevant and sufficient information was repeatedly emphasised during the interviews. Some participants urged doctors to place a greater emphasis on providing initial information to new patients. This recommendation was particularly mentioned by those who felt they did not receive sufficient information at the beginning of their treatment, leading to uncertainty.
So, mainly to spend enough time, especially in the beginning, explaining not only the immediate but the more far-reaching context of the disease. Explaining all that, all that it means right now, but also what it may mean in the future in terms of life change. (participant 36)
One participant suggested hospital doctors should allocate more time during visits to answer patients’ questions and explain the details.
It would have been awfully nice if someone had told me at the beginning it’s not always going to be as unpleasant as it is now. You're not going to feel as humiliated and as stigmatised as you do at the beginning. The beginning is very hard. Just in terms of accepting that something is happening medically and the examinations at the beginning. It’s not pleasant, of course it’s not. And for a young woman, especially. But on the other hand, it doesn’t make the world fall apart, and you can live with it. (participant 07)
Not underestimating symptoms
Participants conveyed a message to doctors and other healthcare professionals, urging them to listen more attentively and never trivialise a patient’s difficulties under any circumstances.
What’s my message? Trust the patient. Because I sometimes felt like the doctor thought I was like exaggerating, making it worse, making things up. When the doctor really makes you feel like you’re making things up or like I’m some kind of simulacrum, that was probably the worst thing I’ve ever experienced. (participant 21)
First, they mentioned that it is crucial not to underestimate the symptoms experienced by patients.
Don’t underestimate the first symptoms. If someone comes to you with a problem, don’t underestimate just what the person is saying, take it a little bit seriously. I think you can distinguish a problem like that from, I don’t know, a viral disease or salmonellosis or something like that. (participant 14)
Unlocking exceptional care
Participants’ messages were related to their quality of care. The most crucial requirement expressed by the participants was high-quality and appropriate health care. Providing the best possible care and considering all symptoms are paramount for achieving positive outcomes. Adequate treatment is vital in ensuring patients feel well and experience relief from symptoms.
The specialist should definitely be an expert in the whole field. That he’s just really giving his patient his best. And if, like me, the biological treatment just doesn’t work, he tries to find a way to give me the best. (participant 15)
Clinical outcomes versus patient-reported outcomes disparity
Patients expressed the need to discuss with their physician if there was a difference between what the clinical results were and how they felt. They experienced incongruity between objective clinical measures and subjective symptoms or feelings reported by the patient. They considered the professional attitude of doctors to recognise this disparity.
I need my doctor to say – for example: “It looks like you’re getting good results. I believe you’re not feeling well, but just these results here are good. It can be like that.” I think it’s been said a couple of times, even at these patients’ conferences, that it happens. Like, there are people who have crazy results, and they’re doing well, and then there are people who have good results, and they’re doing terrible. And that’s what these diseases can be. (participant 21)
Lifelong learning
Another finding emphasised the importance of having educated and knowledgeable healthcare staff. A competent healthcare professional should stay informed about the latest trends in IBD treatment, be well-versed in the available treatment options, and remain up-to-date with new developments in the field. This knowledge allows them to make appropriate recommendations and provide optimal patient care. Continuous education has been highlighted as a crucial aspect of the ongoing development of healthcare professionals. Advancements in IBD research and treatment are vital for delivering the best possible care to patients. Regular training and staying informed about the latest scientific findings will contribute to improved patient outcomes.
So that at the moment when the disease shows its worse side, he can help that patient or that person with some adequate treatment. I think that the experts should probably keep on educating themselves. But that’s probably a matter of course, I think, for all doctors. (participant 23)
Furthermore, some participants recognised the value of consulting colleagues and seeking input in complex cases. Collaboration with other healthcare professionals can provide valuable insights and contribute to more comprehensive and effective treatment strategies.
He should probably be able to communicate with other medical practitioners, as well. I think it’s good that they can discuss something with each other. (participant 15)
The physician-patient relationship
Most participants recommended a humanistic, empathetic, tolerant, humble, personal, willing, understanding, and compassionate approach. The important themes of the need for individualised care and applying a holistic approach to the person, beyond just the medical aspect, emerged.
To treat the patient as a person, not as a diagnosis
The messages, recommendations, and sometimes even criticisms directed towards doctors were most frequently related to their approach towards patients with IBD. Some participants mentioned their negative experiences, feeling like they were merely seen as “guts,” a “chemical laboratory,” or reduced to labels and diagnoses. Providing care to them felt akin to “fixing a car” or “working on an assembly line.”
What would I tell them (doctors)? I mean, I had that doctor, and she was great. She was great. But sometimes you come across a doctor who’s not great, but he treats it like a regular job. It’s like going to a mechanic’s shop to get your car fixed. He doesn’t ask you any questions. He just plugs it into the diagnostic and doesn’t ask you any questions. (participant 13)
Expertise and professionalism are necessary for participants, but it is important to treat patients personally as people.
I think it would be so ideal if like the person had the disease, too. (Laughs) I know it’s stupid and silly, but I feel like everybody just takes me like there’s a machine that comes in at 9:30, and at 10:30, there’s a second machine, and at 11:00 there’s a third machine, and then we take a break, and then it’s back to the fourth machine. That they should treat patients more like people who have a lot of other problems and not just treat it like a machine off the production line. And yet, even though the person may be the best professional, they should treat these people better. (participant 05)
To face shame and embarrassment together
The theme of doctor-patient communication has emerged as an important topic in patient messages. According to the participants, communication should be open and friendly, creating a relaxed atmosphere that helps patients overcome shyness and embarrassment. Respect helps with shyness and embarrassment.
Because some people don’t have the guts to ask. It’s good to be more sensitive because the moment you look at the anus, for example, you’re very embarrassed. And so you pull everything up, the curtains and everything. Which is pretty much how it’s normally done now, respecting privacy. (participant 22)
Another participant explained how the openness of a physician helped him be more comfortable with these embarrassing themes.
I was actually kind of shy about talking about some of those things in the early days of this disease, as well, because there are definitely some uncomfortable things that are kind of taboo, especially about diarrhoea and things like that, so it’s not always everybody’s thing. I would encourage them to ask about those things themselves because they know that there’s that kind of shyness with people. And actually, my doctor, my gastroenterologist, by actually asking me about those things, even though they were quite uncomfortable at first, it was difficult for me to talk about them, but actually, by him asking me about them all the time, it became like such a normal thing for me. (participant 03)
Embracing a friendship-like approach
Participants’ need to bridge the gap between physicians and patients was repeatedly raised. Some participants emphasised the need to establish a relationship with the physician based on friendship, trust, and mutual sympathy. This includes talking about life and understanding, small talk, and a friendlier approach.
Now I have a doctor who asks if I went on vacation, if I’m going somewhere, and deals with things outside the box with me. If I have any problem, he will give me advice. (participant 30)
One participant mentioned that with a gastroenterologist, it is a relationship for life, and patients need to feel reassured.
I’ve since learned to get along with him, and we have a good relationship. We just, he knows my case, I know, like we even talk sometimes about things outside. And you guys, ideally, I think, should have some kind of relationship like that. A patient-physician kind of relationship, but maybe on a higher level, because you already know each other and you know what to expect from each other. Be tolerant of the doctor, and the doctor should be tolerant of you. (participant 08)
Trust, to feel secure with the physician
The concept of trust emerged as being highly important in the analysis. Good professional care and the possibility of establishing an individual relationship lead to trust, which is a vital aspect of treatment.
What do I need from him? Well, I need him to treat me well. To make me feel good. And I have a doctor who can talk to me. So, I’m not complaining. So, even before that, we pretty much understood each other internally. So, that is quite important, trust as a doctor-patient. That’s for sure. So that’s important. (participant 30)
Patients with IBD need to feel secure in their relationship with their physician, especially because of the uncertainty of their disease.
The sense of security that the doctor is supposed to give is very important. Like I can really rely on him, and that there’s some kind of concern. I’m sure sympathy plays a part, but also the doctor’s attitude. If there’s a mutual trust, that’s definitely important. If he gives me a solution or some medication, and I don’t trust it, I’ll go ask someone else what they think because I don’t think it’s right. So, I know that what they’re recommending is good. (participant 28)
If the patient perceives support from their doctor, feelings of gratitude and security can be very strong and helpful in coping with challenging situations with a chronic illness.
I can say that my gastroenterologist is totally, I think, awesome. I know he may not be a good fit for some people, but he’s a great fit for me. I know that whenever I just need something, I can count on him. So that doctor, he helped me a lot, he really did. He really, really, I was still so bad about it, about the surgery, but he really, really reassured me that everything was going to be okay, explained everything to me, and I am really grateful for that. (participant 19)
The healthcare system
We decided to include this third group of analyses in the results because the realisation that the overall healthcare system needs to change has occurred repeatedly. Although seemingly unrelated directly to physicians and patients, it significantly affects the treatment outcome and quality of life for both patients and medical professionals.
To have enough time
Another theme that surfaced in patients’ recommendations and messages was the time constraint for doctors, their excessive workload, and overall busyness.
I know what the doctor and nurse staffing is, or the workload and so forth, okay? That maybe there’s a shortage, or what all that doctor has to do, how many different things he’s got to do, that it’s not just surgeries, now these different outpatient clinics, but he’s doing procedures, yeah? Then he goes to different congresses, and so on, he gives lectures and so on, so if he is so busy, then he can’t have as much space in the consulting room for the patient as he would like to, right? So, then, the check-up is just a short-term check-up. (participant 09)
Patients were aware that doctors were also interested in attending to them, but the health system did not give them the space to do so.
And, like, more time with the patient, yeah. It’s just so obvious that if the doctor is good, he doesn’t have time. But that’s just the way the healthcare system is set up in general. (participant 06)
Some participants perceived that if a doctor is dedicated, it is not possible in the current health system for him/her to do everything within his/her working hours.
Well, as long as he has time for me. And I’m lucky enough to have a doctor who’s really dedicated to us, but he’s not keeping up. (participant 04)
Availability of care
One aspect highlighted by some participants was the possibility of choosing quality healthcare. However, such options may not be available everywhere. Other participants reported changing doctors and seeking care elsewhere where they believed they would receive better care. Access to high-quality care is essential for effective management of IBD.
They sent me to another town. And there, the doctor didn’t know based on the results either, so he immediately sent me to a bigger town for biological treatment. Which is quite a stretch. Because it’s a three-hour drive. (participant 26)
There is differential access to healthcare in large settlements (with IBD centres) and places further away from IBD centres.
Well, there’s a big difference because, in eastern Bohemia, there’s a problem with doctors. Here in Prague, there is one internist who helped me a lot, and she got me to doctors who started to look into it more, and they really found a solution. (participant 34)
To integrate mental health and psychological interventions into the treatment process
Psychosomatic connections with IBD have been repeatedly mentioned. This interdisciplinary approach promotes better outcomes and enhances the quality of patient care.
And it’s the psychological part, yeah, that should be, in my opinion, a much better set-up. It should be much better; much more attention should be paid to it, to those patients, because a lot of research shows that quality of life is greatly reduced often, yeah? And I personally don’t really get it; why do they keep doing research on that quality of life? They keep showing that it’s still the same, right? They’re being done probably because of the fact that different practices in that medicine are changing. Unfortunately, the psychological treatment in this is quite backward. (participant 08)
One participant suggested that a gastroenterologist should also be a psychologist to comprehend all causes and circumstances of the healthcare relationship.
I think, ideally, the psychologist and the doctor should be in one person. I think that the division between the chemical part and the psychological part is so marked that medicine will never be able to cure, to cure the disease comprehensively, without looking at it from the perspective of the whole person. (participant 01)
Discussion
This study aimed to investigate the messages and recommendations provided by patients regarding their experiences with doctors in the context of Inflammatory Bowel Disease (IBD). This study reveals the critical facets of patient experiences and offers valuable insights for practitioners and stakeholders. This is the first extensive qualitative study of IBD patients’ needs in the Czech Republic. Patients actively engaged in their treatment bring novel perspectives, emphasising the importance of a partnered, respectful patient-physician relationship. Realising this approach necessitates systemic healthcare changes, as underscored by this study.
Effective doctor-patient communication is crucial in providing optimal care for patients with IBD.7,13,16,19 Participants emphasised the need for open and friendly communication that creates a relaxed atmosphere, enabling patients to overcome shyness and receive necessary information about their condition and treatment. It is recommended that doctors establish a balanced dialogue and address patients’ questions patiently. Providing relevant and sufficient information, particularly during the early stages of treatment, has been emphasised to alleviate uncertainty and anxiety. Participants suggested allocating more time during visits for detailed explanations and emphasised that early information is important.
Linked to this is the need for more time during regular doctor appointments. The Ulcerative Colitis Narrative Global Survey also confirmed the need for both patients and physicians to have longer appointments. 19 In another, population-based study, patients with IBD were twice as likely to report unmet healthcare needs compared to the general population. 32
Access to care varied according to place of residence in our study. It is easier to access adequate care in large cities with IBD centres. Getting a routine check-up with a gastroenterologist in smaller settlements is sometimes longer and more challenging.
Participants stressed the significance of a humanistic approach emphasising individualised care and holistic understanding. They wanted doctors to view them as humans and not just as medical cases. Time constraints, heavy workloads, and patients feeling like they were on a “conveyor belt” were highlighted as challenges to patient-centred care. Quality care, education of healthcare professionals, a pleasant environment, and the value of continuous learning and collaboration were identified as essential factors in achieving optimal care outcomes for patients with IBD. It is important to note that perceptions of care quality can vary between patients and gastroenterologists.8,11 For instance, Vaucher found that the critical components for patients are quality of life and social outcomes. 8
Other previous studies revealed that adequate physician-patient communication enhanced patient satisfaction with treatment decision-making and patient trust in physicians.11,14,15 The patient’s trust in the doctor is formed by the doctor’s level of expertise and communication with the patient, leading to cooperation in treating IBD. Moreover, strong satisfaction with care quality correlates with treatment adherence, particularly when treatment strategies are mutually agreed upon. 10
The Ulcerative Colitis Narrative Global Survey of in-office visits in the United States and Europe 19 showed that physicians had the goal of endoscopic remission, which the patient rarely articulated. The patient’s goal may be different: to feel better. However, the emotional impact of this disease has rarely been discussed. It is important to discuss common goals from the perspectives of both sides. This is consistent with our study, in which patients proposed to address this discrepancy.
Our study demonstrates that in consultations with a gastroenterologist, inquiring about quality of life and psychological well-being is paramount for patients. The Ulcerative Colitis Narrative Global Survey showed that the gastroenterologist asked patients about their disease’s quality of life or emotional impact in 23% of visits. 19 Treating the person as a whole, not just the diagnosis, was taught by the key message of our participants. A Greek study highlighted a similar phenomenon in that most doctors focus on treating the disease and not the patient as a whole. 33
Psychological care can improve a patient’s quality of life and integrate work into routine management. Psychological screening was well accepted, with 68% of patients participating in a study by Lores et al. 34 Psychological care was needed for those scoring highly in anxiety, depression, or general distress. Participants in our study repeatedly expressed an interest in integrating psychological aspects into IBD care.
We opted for qualitative research in line with studies highlighting the importance of including patients in research to bridge the gap between researchers and research, as well as between healthcare commissioners and research outcomes.35,36 We see the importance of the study, particularly in the confirmation of the predominantly quantitative results by the word-of-mouth of patients and the need for practical changes to the whole healthcare system. This is in line with the work of researchers working on the integrative care of IBD patients.20,21
Limitations
Several limitations of this study should be considered when interpreting the results. The sample of participants was heterogeneous, reducing the qualitative analysis’s scientific rigour. Some participants grounded messages on the long-term medical care experience, so they may not be relevant for recently diagnosed patients when some medical procedures may have already been innovated. This is particularly relevant to the holistic approach to a person who is gradually being incorporated into the care of most hospital settings. The participants were from different regions and circumstances, with different disease severity, age, age at diagnosis, and other sociodemographic factors. Another limitation of the sample was that we did not succeed in recruiting more patients from minority and socially disadvantaged environments. The study included patients willing and motivated to comment on the topic, which is not indicative of the entire population of IBD patients. Additionally, a formal sample size or power analysis was not performed for this qualitative study. This approach aligns with the objectives of qualitative research, which prioritise depth and richness of data over numerical representativeness. Furthermore, the interview guide was not formally validated; however, it was reviewed and revised after conducting three of the 36 interviews. Experts from the Advisory Panel collaborated on this process to ensure the relevance and comprehensiveness of the questions.
Conclusions
These findings contribute to knowledge about the key themes about physician-patient communication and the approach of healthcare providers, with a particular focus on the need for a friendly and humanistic approach, delivery of high-quality care, and the significance of lifelong education in health care. By identifying and analysing these topics, this study aimed to deepen the understanding of effective communication strategies, the importance of patient-centred care, and the continuous professional development required to meet the evolving healthcare needs of patients. The findings sought to provide valuable insights and inform healthcare professionals and policymakers in their efforts to enhance physician-patient interactions, improve the provision of quality care, and promote ongoing education within the healthcare field. Subsequent qualitative research could bring the voices of healthcare workers’ needs to the healthcare system.
Supplemental Material
Supplemental Material - Inflammatory bowel disease patients’ expectations of care: Insights from a qualitative study
Supplemental Material for Inflammatory bowel disease patients’ expectations of care: Insights from a qualitative study by Hana Bednarikova, Kristyna Gabova, Zuzana Zelinkova, Zdenek Meier and Peter Tavel in European Journal of Inflammation.
Supplemental Material
Supplemental Material - Inflammatory bowel disease patients’ expectations of care: Insights from a qualitative study
Supplemental Material for Inflammatory bowel disease patients’ expectations of care: Insights from a qualitative study by Hana Bednarikova, Kristyna Gabova, Zuzana Zelinkova, Zdenek Meier and Peter Tavel in European Journal of Inflammation.
Supplemental Material
Supplemental Material - Inflammatory bowel disease patients’ expectations of care: Insights from a qualitative study
Supplemental Material for Inflammatory bowel disease patients’ expectations of care: Insights from a qualitative study by Hana Bednarikova, Kristyna Gabova, Zuzana Zelinkova, Zdenek Meier and Peter Tavel in European Journal of Inflammation.
Footnotes
Author contributions
HB: recruitment, data collection, analysis of results, draft of the paper, final approval; KG: data extraction, analysis of results, draft of the paper, revising the article, final approval; ZZ: interpretation of data, revising the article, final approval; ZM: interpretation of data, revising the article, final approval; PT: conception and design of the study, revising the article, final approval. All authors contributed to drafting or revising the article critically for important intellectual content. All authors provided final approval of the version to be submitted and agreed to be accountable for all aspects of the work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by Palacky University [IGA_CMTF_2023_002].
Ethical statement
Data availability statement
The data underlying this article are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.