
Abstract
It is difficult to diagnose necrotizing fasciitis early. In addition, untimely or incorrect treatment worsens the disease, which may then develop into severe necrotizing fasciitis. A retrospective analysis of the clinical data of 35 patients with severe necrotizing fasciitis admitted to the Burn Department of Gansu Provincial Hospital from 1 January 2015, to 1 January 2020, and the etiology, causes and diagnosis of their aggravated conditions was performed. Thirty cases were directly or indirectly related to trauma, 4 cases were pressure sores caused by long-term paraplegia, and 1 case was from mosquito bites on the left side of the chest. The preliminary diagnosis of 24 patients was unclear, and these cases were misdiagnosed as cellulitis or skin infections; 11 patients were diagnosed at the early stage, but due to the incorrect treatment or failure of timely treatment, their condition was further aggravated and developed into critical necrotizing fasciitis. 1. The diagnosis of necrotizing fasciitis mainly depends on clinical manifestations, and early diagnosis is key; 2. When the patient has local trauma accompanied by local inflammation, fever or hypothermia, necrotizing fasciitis should be highly suspected, and a differential diagnosis should be made between necrotizing fasciitis and cellulitis. The affected tissue should be thoroughly debrided and drained to avoid necrosis spreading to the distal limb along the fascial space. 3. Necrotizing fasciitis should be treated with systemic comprehensive treatment, rational use of antibiotics, correction of water and electrolyte disturbance, early active and thorough debridement and effective wound closure.
Introduction
Necrotizing fasciitis (NF) are rapidly progressing and life-threatening bacterial infections that destroys the epidermis, dermis, subcutaneous tissue, fascia, and muscles. Hippocrates (500 BC) gave an early description as “diffused erysipelas caused by trivial accidents, [where] flesh, sinews, and bones fell away in large quantities, [leading to] death in many cases.”1–5 The term “necrotizing fasciitis” was first coined by Wilson in 1952 and is probably the most accurate term to describe the key features of the infection process. Necrotizing fasciitis (NF) is characterized by rapid disease progression, soft-tissue infection, subcutaneous tissue and deep fascia necrosis, and pain disproportionate to the physical presentation, 6 with necrosis reaching deep fascia. Therefore, patients frequently experience symptoms of sepsis, septic shock, and multiple organ failure. The disease lacks specific clinical manifestations in the early stages, so it is difficult to distinguish it from other soft-tissue infectious diseases, such as cellulitis and gas gangrene. Treatment is delayed due to the difficulty of early diagnosis. When the diagnosis is clear, most patients have experienced complications such as extensive fascial necrosis, electrolyte imbalance, anemia, hypoproteinemia, and multiple organ failure. The absence of preliminary pathological characteristics makes the diagnosis of necrotizing fasciitis extremely difficult. Therefore, we conducted a systematic retrospective analysis with the purpose of determining clinical characteristics as a means of aiding early diagnosis and treatment.
Methods
Clinical data
Retrospective analysis of patients admitted to the burn department of Gansu Provincial Hospital from January 2015 to January 2020. Inclusion criteria: Patients diagnosed with necrotizing fasciitis. Exclusion criteria: Patients who requested to be discharged before treatment was completed or patients with missing clinical information. The time from onset to initial admission ranged from 15 days to 1 month. All patients were transferred to our hospital from primary hospitals. By obtaining the patients' medical histories and consulting the data of primary hospitals, we learned that most of patients were misdiagnosed with cellulitis and skin infections and were given symptomatic treatment such as anti-infection medications and regular dressing changes on the wound.
Clinical manifestation
Most of the patients were admitted late, with obvious limb swelling accompanied by systemic symptoms, but the wound manifestations were not consistent. Some wounds expanded slowly and undetected in certain parts of the limb, and some developed by leaping along the long axis of a limb, forming multiple wounds. The skin between the wounds of necrotic fasciitis appeared basically intact. There were usually no obvious purulent secretions on the wounds, and the fasciitis was mainly characterized by fascial necrosis, accompanied by muscle necrosis in severe cases. Patients often experienced septic shock, sepsis, hypoproteinemia, severe anemia, and electrolyte disturbances, and some had hypothermia.
Microbiological detection
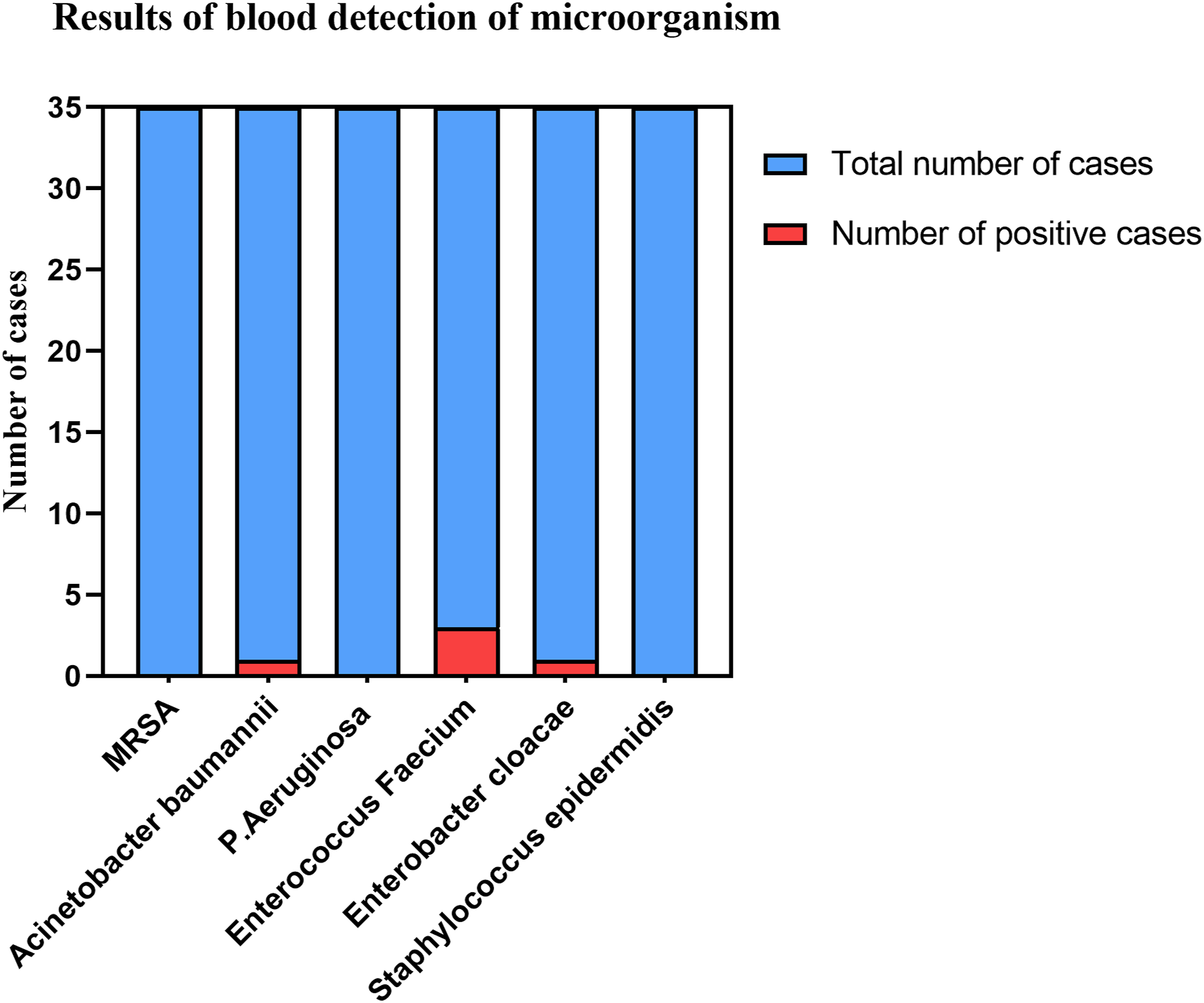
All patients underwent more than two microbiological tests after admission, including blood culture and wound culture. The bacteria examined generally included common gram-positive and gram-negative bacteria such as MRSA, Acinetobacter Baumann Pseudomonas aeruginosa, and Cococobacteria enterococcus faecium. Antibiotics were adjusted in a timely manner according to the results of bacterial culture (Figures 1 and 2). Results of wound detection of microorganism. Results of blood detection of microorganism.
Clinic treatment
Based on the results of the laboratory examination on admission, the overall physical condition of the patient was preliminarily assessed, corresponding anti-infection and fluid rehydration treatments were given, and the patient was actively stabilized. If the patients were suffering from septic shock, while they were being stabilized and given anti-shock treatment, surgical treatment was performed as soon as possible, and the wound was thoroughly debrided and drained (Figure 3). After the operation, vacuum sealing drainage (VSD) was placed on the wound, and 30 U insulin, 100 mg lidocaine and 7500 U external recombinant human acidic fibroblast growth factors were administered via 1000 mL sodium chloride saline. The wound was washed twice a day. Four to 5 days after the operation, the VSD of the wound was opened, and the condition of the wound was observed. If there was more necrotic tissue, another operation was undertaken to remove the necrotic tissue, and the VSD was replaced after the operation until there was no necrotic tissue on the wound and fresh tissue appeared. At this time, the wound was sutured. If the wound was too large to be sutured directly, medium thickness skin was transplanted to try to close the wound as soon as possible (Figure 4). When anti-infection treatment was ineffective, the wound debridement and drainage were not completed, and reoperation was performed as soon as possible (Figure 5). When the diagnosis was not clear, surgery was performed as soon as possible, a diagnostic incision was made on the wound surface, and after the etiology was determined, the corresponding treatment was administered (Figure 6). A 45-year-old male patient was admitted to the hospital due to a high fever for 3 days and a coma for 1 day (a) The patient was admitted with swelling of the left lower limb with marked inflammation and a small wound on the lateral thigh. (b) Intraoperative exploration showed a large amount of necrotic tissue and complete debridement. (c) After complete debridement, VSD was given for continuous suction, and fresh granulation tissue could be seen after rinsing with 2000 mL normal saline every day for a week. (d) Wound 2 weeks after surgery. (e) Six months after the operation, the patient’s wound had recovered well, and function was good. A 32-year-old male patient was admitted to the hospital due to persistent fever for 1 day. The patient underwent small window drainage in the primary hospital. (a, b) The figure shows that 7 days after the patient received small incision drainage of the left lower extremity in another hospital, necrotic tissue and purulent secretions could be seen around the incision due to incomplete incision drainage and insufficient drainage, resulting in the necrosis spreading to the distal extremity along the fascia. (c, d) Intraoperative exploration revealed a large amount of necrotic tissue, edema granulation tissue and edema synovial membrane in the left lower limb. (e) One week after debridement and skin grafting, the grafted skin survived well, and there was no obvious inflammatory reaction in the skin margin. A male patient was admitted to the hospital due to paraplegia for 1 year and continuous fever for 5 days. (a) The patient had sacrococcygeal decubitus sores, swelling of the right lower limb with a fetid odor, and hypothermia. (b–d) Intraoperative exploration revealed foul-smelling pus outflow from the right lower limb. (e) After the first operation, the wound was fixed with dense iodovolt gauze. (f) Fresh granulation tissue was observed at the wound 10 days after the operation. (g) The second operation covered the wound with a medium-thickness skin graft. (h) The wound was basically healed 15 days after skin grafting. A 33-year-old female patient was admitted to the hospital due to redness and swelling in the right lower extremity with pain for 10 days, progressive worsening, and coma for 3 days. (a) Swollen right lower extremity with low skin temperature and foul odor. A diagnostic incision was made in the right calf, and the picture shows the necrotic fasci. (b) First operation, debridement of the thigh and exploration of the necrotic tissue in the fascial space. (c, d) During the second operation, there was an obvious foul pus outflow to the right lower extremity, and a large amount of necrotic tissue was seen at the knee joint in addition to myofascial inflammation. After the wound was debrided completely, VSD was placed and rinsed with 2000 mL normal saline for 1 week every day. (e) In the third operation, the necrotic tissue was reduced, but the necrotic fascia was visible to the knee joint. VSD was placed after debridement. (f) In the fourth operation, necrotic tissue was found at the knee joint, and it was fully debrided. A large autologous medium-thick skin patch was transplanted to cover the wound, and the VSD was placed. (g, h) Patients were followed up for half a year after discharge. They had no significant obstacles with respect to knee movement or walking.



Statistical analysis
Results of wound detection of microorganism.

Results of blood detection of microorganism.

Early characteristics of the disease.

Results of laboratory tests.

Results
All 35 cases of necrotizing fasciitis survived, and the average hospitalization cost was more than 100,000 yuan. Hospitalization lasted more than 30 days on average. Twenty-one patients were re-examined regularly after discharge. No recurrence was observed after 1 year of follow-up. Fourteen patients were not re-examined after discharge. All 35 patients underwent surgery, and 22 patients underwent more than one operation. Thirty cases were directly or indirectly related to trauma, 13 patients had a history of paraplegia, 4 cases were pressure sores caused by long-term paraplegia, and 1 case was the result of mosquito bites on the left side of the chest. The preliminary diagnosis of 24 patients was unclear, and these cases were misdiagnosed as cellulitis or skin infection; 11 patients were diagnosed in the early stage, but due to incorrect treatment or failure to obtain timely treatment, their condition was further aggravated and developed into critical necrotizing fasciitis. All 35 patients showed typical symptoms of inflammatory reactions in the early wound (redness and high skin temperature around the wound). Most of the patients’ early wounds had tension blisters, pain around the wound, a peculiar smell and crepitus, accompanied by hypotension and an abnormal body temperature (Figure 7). Early laboratory testing of the patients was not specific and could not provide effective evidence for clear diagnoses (Figure 8). Early characteristics of the disease. Results of laboratory tests.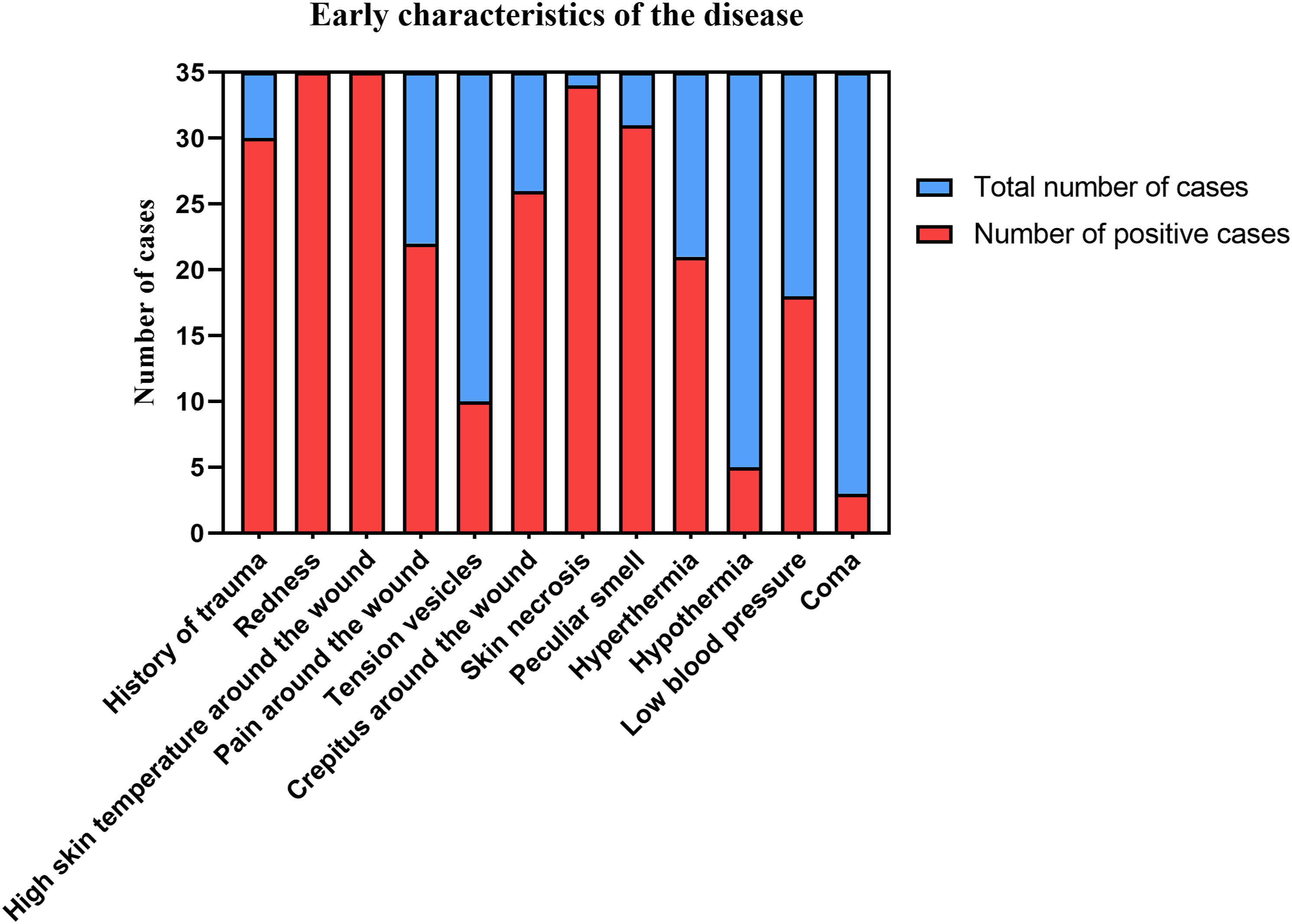

Discussion
Necrotizing fasciitis is a disease characterized by necrosis of the skin, subcutaneous tissue, and superficial fascia. It rarely involves muscles and generally occurs in places with loose tissue. Most cases spread quickly to local tissue. If not handled properly, patients often develop sepsis and die of septic shock; later stages of the disease are usually accompanied by multiple organ failure.7,8 The common causes are a lack of unnoticed body puncture, care-related bedsores of paraplegic patients, and delayed medical treatment. This leads to a critical dilemma as patients generally have advanced symptoms, such as swollen limbs or severe systemic issues, by the time they are admitted to the hospital. Therefore, patients often experience septic shock and complications such as sepsis, hypoproteinemia, anemia, and electrolyte imbalance.
Thus, early diagnosis is very important to the treatment of the disease, but necrotizing fasciitis is easily misdiagnosed and missed in the early stage. We conducted a retrospective analysis and found that early necrotizing fasciitis shares some common characteristics: (1) Small trauma, such as mosquito bites, pressure sores, or localized wounds, are present. (2) Patients who suffered from minor trauma did not receive regular treatment in a timely manner. Instead, they went to the hospital and were misdiagnosed with cellulitis despite symptoms of advanced stage necrotizing fasciitis, including local redness, pain, and dysfunction. (3) Paraplegic patients had sacrococcygeal pressure ulcers with or without inflammation, whole-body or low-grade fever, spreading redness and swelling in lower limbs. (4) Patients had wounds that could not be debrided in a timely and effective manner. Incomplete incision and drainage caused the necrosis to spread along the fascia to the distal limbs.
Early and thorough debridement after correction of the internal environment is a key step in the treatment of necrotizing fasciitis. A retrospective analysis found that some patients had a clear diagnosis in the primary hospital, but the surgical treatment failed to fully open and drain, causing the necrosis to spread continuously along the fascial space to the distal limbs. Therefore, perioperative systemic comprehensive treatment is key to combating necrotizing fasciitis. Patients with a prolonged disease course often experience severe anemia, hypoalbuminemia, and electrolyte disorders, which should be actively corrected. However, most of these patients have a long history of being bedridden, so they often have poor cardiopulmonary function, which makes treatment of these patients very difficult. Patients with septic shock and hypoalbuminemia have poor cardiopulmonary conditions and need to limit fluid replacement. Thus, this group of patients with septic shock were treated with Picco’s effective detection of blood flow to maximize the time for treatment. 9 Due to the disease characteristics of necrotizing fasciitis, surgical debridement should focus on the breadth and depth of debridement. Limb necrotizing fasciitis rarely involves muscles, but it can encroach on the deep fascia. In general, the deep fascia of long-term and critically ill patients is often affected and needs to be removed. The breadth refers to the extent of the wound margin. Sneak creep is a characteristic of the disease. According to clinical experience, it is necessary to remove at least 1 cm of skin and subcutaneous tissue at the wound margin, especially the edges of both sides of the long axis of the limb, until necrotic tissue is not directly visible. Even so, it is difficult to debride patients with a critical or prolonged disease course to in a single treatment; most patients need three or more operations to completely debride and cover the wound. This also indicates that the range of necrotizing fasciitis infection or necrosis exceeds the range estimated under direct vision.9–11 If the patient’s wound still has excessive secretions or the patient continues to have a high fever after surgery, a second surgical treatment should be performed immediately under relatively stable internal conditions. If the patient’s necrotic tissue cannot be productively removed, its symptoms cannot be effectively improved. Thorough debridement is the key to treating necrotizing fasciitis because it can address the problem at the source.
When patients are admitted without direct bacteriological support, based on clinical experience, treatment with broad-spectrum antibiotics is an important auxiliary method. However, since the disease is rarely diagnosed in the early stages, most patients take multiple antibiotics for a long time until a definite diagnosis is made. This potentially increases antibiotic resistance. Even so, the use of broad-spectrum antibiotics should be used in the perioperative period. We believe the medication still has a more positive effect on patient outcomes. In this group of patients, imipenem is generally selected for treatment during the perioperative period. After the wound and blood culture results were obtained, sensitive and relatively narrow-spectrum antibiotics were selected. In patients with necrotizing fasciitis, when there is no obvious systemic inflammatory response, debridement should be given priority, and antibiotics should only be used as an auxiliary treatment. Therefore, it is worthwhile for clinicians to consider the indication, the consequence, and the strategy of applying powerful broad-spectrum antibiotics when facing the spread of necrosis.
Bacteriological examination has important clinical significance in the treatment of infectious diseases. However, the current detection rate of anaerobic bacteria in the clinic is low, which greatly reduces its significance in guiding clinical treatment. Necrotizing fasciitis is usually caused by anaerobic and aerobic bacterial infections,8,12 but bacterial culture often does not help diagnose the disease. Because the bacterial culture period is long, the detection rate of anaerobic bacteria is low. Most of the patients in this group have been treated in more than two hospitals and for seven or eight detected bacteria. Antibiotics have been given according to drug sensitivity experiments, but the effect is far from satisfactory. Therefore, treatment of the disease cannot be overly dependent on the results of bacterial drug sensitivity tests but should be based on clinical manifestations and surgical treatment, with bacteriology testing only as a reference for treatment. This study was a retrospective analysis, single-center and with a small sample size, and no sample size estimation was performed. Therefore, the sample size should be increased and a multicenter study should be performed to obtain more accurate data. The incidence of necrotizing fasciitis is decreasing year by year, and in addition, when patients suffering from this disease are diagnosed, their condition is already critical and must be treated immediately and urgently, and can only be empirically summarized after the patient has completed treatment. Therefore, this study lacks a control group as well as a comparison of treatment effects. We only summarize the early features and causative factors of necrotizing fasciitis and empirically summarize the treatment of the disease, and cannot compare the therapeutic effect with other treatment methods.
In summary, early and thorough debridement after correction of the internal environment has a key role in the treatment of necrotizing fasciitis. Systemic comprehensive perioperative treatment is important for better outcomes in the treatment of necrotizing fasciitis.
Conclusions
1. The diagnosis of necrotizing fasciitis mainly depends on clinical manifestations, and early diagnosis is key. 2. When the patient has local trauma with local inflammation and fever or hypothermia throughout the body, necrotizing fasciitis should be highly suspected, and a differential diagnosis should be made with cellulitis. When it is difficult to distinguish, a diagnostic surgical incision can be performed. 3. The affected tissue should be thoroughly debrided and drained to avoid necrosis spreading to the distal limbs along the fascial space. 4. Necrotizing fasciitis should be systemically and comprehensively treated, with rational use of antibiotics, correction of water and electrolyte disorders, early active and thorough debridement, and effective sealing of the wound.
Footnotes
Author contributions
XY and ZG contributed to the conception and design of the study, acquisition of data, analysis and interpretation of data, and drafted the article. XY, ZG, MZ, QF, and JZ make critical revisions to important intellectual content and final approval of the version to be submitted. All authors have read and approved the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval for this study was obtained from the ethics committee of Gansu Provincial Hospital (APPROVAL NUMBER 2020-104). We have obtained written informed consent from all study participants. All of the procedures were performed in accordance with the Declaration of Helsinki and relevant policies in China.
Informed consent
For any people individually identifiable within this publication, Written informed consent for their use in the publication was obtained from all subjects before the study.