
Abstract
This study aims to analyze the clinical effect of dexamethasone in the treatment of tuberculous meningitis and its effect on MyD88 and TLR4 expression in monocytes. In total, 60 tuberculous meningitis patients were divided into two groups: observation group and control group. Of them, 36 patients were treated with conventional anti-tuberculosis treatment combined with dexamethasone in the observation group, while patients in control group were treated with anti-tuberculosis alone, and the clinical efficacy and expression of TLR4 and MyD88 in peripheral blood monocytes in both the groups were analyzed. The total effective rate in the combined treatment group was 91.67%, which was significantly better than the control group (χ2 = 5.17, P < 0.05). This revealed that dexamethasone treatment can significantly reduce the expression levels of TLR4 and MyD88. Anti-tuberculosis treatment combined with dexamethasone can significantly improve treatment efficacy. Furthermore, the TLR4-MyD88 pathway plays an important role in the dexamethasone treatment of tuberculous meningitis.
Introduction
Tuberculous meningitis (TBM) is a nonsuppurative inflammatory disease caused by Mycobacterium tuberculosis traveling through the blood or other ways into the subarachnoid space, which affects the spinal meninx and meninges, resulting in high mortality and disability.1–3 In recent years, the increase in resistant strains and the prevalence of AIDS have resulted in the increased incidence of TBM, 4 which seriously threatens the life and health of patients. Early diagnosis and active treatment are the premise of good prognosis and the prevention of complications. 5 Toll-like receptors (TLRs) are a kind of important recognition receptors in innate immunity. Among them, TLR4 is distributed in antigen-presenting cells. TLR4 signals can be transduced through the MyD88-dependent downstream pathway and promote the secretion of inflammatory cytokines.6–9 Dexamethasone bidirectionally regulates these immune responses. It can induce the expression of TLR4 in resting T cells and inhibit the expression of TLR4 in activated T cells. 10 Based on the TLR4/MyD88 signaling pathway, we explore a possible mechanism, in which dexamethasone reduces this excessive immune reaction in TBM patients, in order to provide experimental reference for clinical application.
Materials and methods
General information
A total of 60 patients diagnosed with TBM by the modified acid fast staining method in the Neurology Department of our hospital from July 2013 to April 2015 were enrolled in this study. Among them, 36 patients were classified as the observation group and treated with conventional anti-tuberculosis combined with dexamethasone (Southwest Medicine, National Medicine H50021462; 1 mL:5 mg) treatment, while 24 patients were classified as the control group and treated with conventional anti-tuberculosis treatment. All patients in both groups provided signed informed consent. There was no significant difference in terms of age, disease, and all other aspects between the two groups (P > 0.05).
Therapeutic methods
Patients in the control group were treated by anti-tuberculosis therapy including anti-tuberculosis treatment, reduction of intracranial pressure and cerebral edema, and so on. Drugs used are as follows: rifampicin 1.45–0.6 g/day, isoniazid 0.6 g/day, ethambutol 0.75 g/day, and pyrazinamide 1.0–1.5 g/day. The 3-month strengthened treatment was followed by 7 months of consolidation therapy (oral administration, one time/day). In addition, 20% of mannitol was administrated by injection according to the weight of each patient within 1 h. Compared with the treatment in the control group, 10 mg/day of dexamethasone was intravenously injected in patients in the observation group.
Detection indices and methods
Clinical curative effect judgment
Excellent effective. Temperature returns to normal, symptoms are relieved, consciousness becomes clear, and cerebrospinal fluid (CSF) routine and biochemical indices significantly improve;
Effective. Normal temperature, symptoms are partly relieved, and CSF routine and biochemical indices improve;
Ineffective. No improvement or even the deterioration of the indicators and symptoms; death.
Separation of peripheral blood monocytes
A total of 5 mL of elbow vein blood was collected before anti-tuberculosis treatment and at 1 and 2 weeks after anti-tuberculosis treatment. The collected blood was placed in anticoagulant tubes, and heparin was added and mixed evenly. Peripheral blood monocytes were separated using HISTOPAQUE-1077 lymphocyte separation liquid (Gibco-BRL), according to the manufacturer’s instructions.
Detection of TLR4 and MyD88 messenger RNA expression in peripheral blood monocytes by reverse transcriptase–polymerase chain reaction
The total RNA of peripheral blood monocytes was extracted according to TRIzol reagent kit instructions (Shanghai Sagon Biotech). The first strand of complementary DNA (cDNA) was synthesized by reverse transcription using random primers and a reverse transcriptase kit (superscript II). Then, TLR4 and MyD88 messenger RNA (mRNA) expression levels were detected by reverse transcriptase–polymerase chain reaction (RT-PCR) using GAPDH gene as an internal standard. The relative expression of the targeted gene = 2−ΔΔCΤ.
Detection of TLR4 and MyD88 protein expression levels in peripheral blood monocytes by western blot
The collected monocytes were added to 200-µL cell lysates (50 mM Tris–HCl pH 8.0; 150 mM phenylmethylsulfonyl fluoride (PMSF); 0.1% NP-40, protease inhibitor). The mixture was centrifuged at 12,000 r/min for 15 min at 4°C, the supernatant was collected, and protein concentration was detected by Bradford method. A total of 50 µg of the pre-prepared protein sample was added onto a 15% sodium dodecyl sulfate polyacrylamide gel electrophoresis (SDS-PAGE) gel. After electrophoresis, the protein was transferred onto a nitro cellulose (NC) film and was enclosed with 5% skimmed milk powder. Then, the first antibody (SIGMA) was added and incubated for 2 h at 37°C. After rinsing with 0.1% Tris-buffered saline and Tween 20 (TBST), the second antibody (1:2000) was added and incubated at room temperature for 2 h. After the film was rinsed with TBST, enhanced chemiluminescence (ECL) was added, fixation was performed with X optical film, and image analysis was performed with IPP6.0 software.
Statistical analysis
Statistical analysis was performed by SPSS 19.0 software. The data collected were presented as mean ± standard deviation (SD), count data were tested by χ2, and data were measured by t-test. P < 0.05 was considered statistically significant.
Results
Baseline clinical and laboratory findings of TBM patients
The clinical and laboratory findings of the two groups before treatment were shown in Table 1 and not statistically significantly different (P > 0.05).
Baseline clinical and laboratory findings of 60 TBM patients.
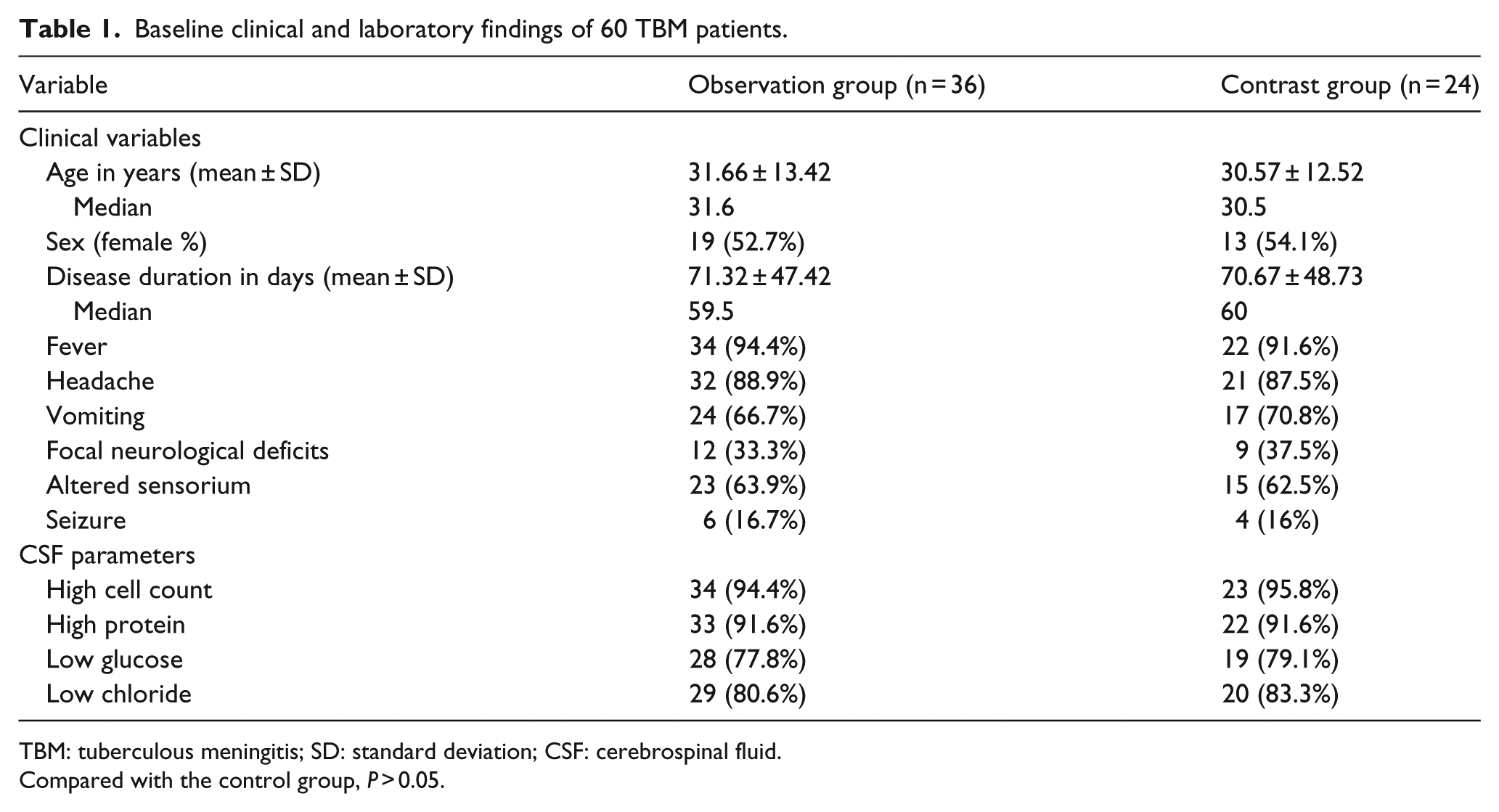
TBM: tuberculous meningitis; SD: standard deviation; CSF: cerebrospinal fluid.
Compared with the control group, P > 0.05.
Analysis of clinical curative efficacy between the two groups of patients
Therapeutic effects between two groups of patients were compared. Results revealed that 23 cases were excellent effective, 10 cases were effective, and total efficacy was 91.67% in the observation group, which was significantly better than the control group (χ2 = 5.17, P < 0.05; Table 2).
Analysis of clinical curative efficacy between the two groups of patients.

Analysis of TLR4 and MyD88 mRNA expression in peripheral blood monocytes in patients in the two groups
TLR4 and MyD88 mRNA expression levels in peripheral blood monocytes in the two groups of patient were analyzed by RT-PCR. Results demonstrated that TLR4 and MyD88 mRNA expression levels in peripheral blood mononuclear cells were significantly lower in the observation group than in the control group (P < 0.05; Table 3).
Analysis of TLR4 mRNA and MyD88 mRNA expression in peripheral blood monocytes between the two groups of patients (mean ± SD).

SD: standard deviation; mRNA: messenger RNA.
Compared with the control group *P < 0.05.
Analysis of TLR4 and MyD88 expression in peripheral blood monocytes in patients in the two groups
TLR4 and MyD88 expression levels in peripheral blood monocytes in the two groups were analyzed by western blot. Results revealed that TLR4 and MyD88 expression levels in peripheral blood monocytes were significantly lower in patients in the observation group than in the control group (P < 0.05; Table 4, Figure 1).
Analysis of TLR4 and MyD88 expression in peripheral blood monocytes between the two groups of patients (mean ± SD).

SD: standard deviation.
Compared with the control group *P < 0.05.

Expression of TLR4 and MyD88 in the two groups of patients.
Discussion
TBM is a global public health problem, especially in backward countries and regions. Epidemiological studies have revealed that 1/3 TBM patients would die, 1 while TBM patients combined with HIV infection have higher mortality.5,11 Some patients would suffer from severe central nervous system sequelae such as cerebral infarction, hydrocephalus, and cranial nerve damage. 12 Early diagnosis and timely treatment are of critical significance for the prognosis of TBM patients. 5 At present, the treatment of TBM includes symptomatic support, anti-tuberculosis drug treatment, the prevention of complications, and so on. Early administration, as well as the adequate, combined, and full use of drugs, is the principle of the administration of anti-tuberculosis drugs. Early administration of corticosteroids could reduce intracranial pressure, reduce brain edema, inhibit fibrosis to prevent adhesion, and ease poisoning symptoms. Some studies have demonstrated that intrathecal administration plus CSF replacement therapy on the basis of conventional anti-tuberculosis treatment could significantly increase clinical cure rate and effective rate, and the recovery time of CSF pressure and biochemical indices has significantly advanced.13,14 On the basis of conventional anti-tuberculosis treatment, the added treatment of dexamethasone can significantly improve clinical efficacy and shorten treatment time with no increase in reverse reaction.15–17 Dexamethasone is a potent anti-inflammatory substance. As a main immune regulator that has been applied so far, it can influence multiple pathways of the inflammatory cascade and has a two-way regulation on immune response. Due to the risk that it could diffuse in tuberculosis, the application of dexamethasone is forbidden for serious tuberculosis infected patients.
When Mycobacterium tuberculosis enters host-alveolar macrophages through the respiratory tract, the bacteria begins to replicate and spread into the local lymph circulation system. Before the start of the acquired immunity response, the bacteria can spread through the blood to other organs of the body, causing the occurrence of TBM and other extra-pulmonary tuberculosis. This process is influenced by the nature and extent of innate immune responses. TLRs are its transmembrane signal transduction receptors, which works through the identification of the highly conserved structure of pathogen-associated molecular patterns (PAMPs) on the surface of pathogenic microorganisms. 18 Through the activation of a series of signaling cascades, it induces the production of cytokines and inflammatory factors, therefore playing an important role in Mycobacterium tuberculosis infection. TLR4 markedly contribute in the typical immune response in tuberculosis. 19 A recent study has shown that genetic variation in TLR2, 4, 8, and 9, indicating TLR-related pathways influencing the innate immunity response, regulate latent tuberculosis infection and pulmonary tuberculosis susceptibility in Chinese. 20 MyD88 is important to the downstream TLR activation. MyD88 signaling in dendritic cells and macrophages is indispensable to control the Mycobacterium tuberculosis burden. 21 In vitro studies have demonstrated that dexamethasone can inhibit lipopolysaccharide (LPS)-stimulated TLR4 expression, 22 while the decrease in the activation of TLR4 reduces MyD88 expression and inhibit inflammatory response. 23 Therefore, we explored the mechanism of dexamethasone for the treatment of TBM based on the TLR4-MyD88 signaling pathway. These results have revealed that routine anti-tuberculosis treatment combined with dexamethasone can significantly improve curative efficiency and inhibit TLR4 and MyD88 expression in monocytes in peripheral blood of patients, compared with the control group, suggesting that the TLR4/MyD88 signaling pathway may play an important role in the occurrence and development of TBM, as well as in the action of dexamethasone.
Footnotes
Author contribution
Jie Zhou and Jing Wang are responsible for the design and the conception of this article as well as data interpretation and analysis. Mei-Ying Gu and Shu-Qiong Zhang were responsible for the acquisition of data. Sheng-Li Chen performed statistical analysis and data synthesis. Xian-Wei Zhang and Li-Na Zhang were responsible for study coordination and revising and critically reviewing this article. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by our hospital, and all participants signed a document of informed consent.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.