
Abstract
Background:
Patient–provider language discordances can negatively affect the availability, accessibility, acceptability, and quality (AAAQ) of pharmacy services as described by the AAAQ framework. With nearly 600,000 residents of Ontario identifying French as their mother tongue, the active offer (AO) of French language pharmacy services should be provided, yet little is known about pharmacists’ familiarity and use of AO.
Methods:
Ontario pharmacists completed an online survey measuring their knowledge, attitudes, and behaviours (KAB) regarding the AO for French language services (FLS). Demographics, including ability to converse in French, were collected. KAB AO scores were calculated and compared using descriptive and inferential statistics.
Results:
A total of 360 pharmacists completed the survey. The majority (65.1%) practiced in a primary care setting, 21.1% spoke French, and 71.8% lived in an area where less than 10% of the population were Francophone. Overall, AO scores were highest for attitude (3.8/5) and lowest for behaviours (2/5) and knowledge (1.8/5). Most pharmacists (62.8%) indicated an interest in AO training.
Discussion:
Gaps in KAB regarding AO for FLS by Ontario pharmacists resemble those observed throughout the health care system. Further training is suggested to address the lack of knowledge regarding AO, particularly its proactive nature, as well as strategies for its implementation.
Conclusion:
Although most participating pharmacists demonstrated gaps in AO knowledge and behaviour, many had favourable attitudes toward the importance of AO in the pharmacy setting and agreed that further training would be needed to improve their KAB. Further, the AO can address all 4 elements of the AAAQ framework.
Knowledge into Practice
Language-concordant health care delivery improves health outcomes.
A proactive offer by the health care provider of services in French (called “active offer”) is an important tool to serve Francophone patients.
Pharmacists are not familiar with active offer and the strategies that both English- and French-speaking pharmacists can use to provide an active offer.
Pharmacists are open to training about how best to provide an active offer to their patients.
Introduction
The Canada Health Act protects the right to health care for all Canadians. 1 However, in order for people to benefit from health care services, these services must be available. Taking a human rights approach, the World Health Organization has suggested that the right to health includes 4 essential elements: availability, accessibility, acceptability, and quality (the AAAQ framework). 2 Although pharmacists have been found to be highly available according to the AAAQ framework, language barriers can challenge their availability. 3 In Canada, the possible repercussions of language barriers are particularly relevant given the presence of 2 official languages, English and French, and the fact that French speakers outside of Quebec are a linguistic minority. Despite their minority status, Ontario is home to Canada’s largest Francophone population living outside of Quebec, with more than 1.5 million residents able to speak French (11.1% of the population) and nearly 600,000 identifying French as their mother tongue (4.2% of the population). 4
According to the AAAQ framework, availability refers to the quantity and location of French-language pharmacy services. 3 Although approximately 75% of Francophones residing outside of Quebec believe that access to French language services (FLS) is important and that pharmacists are among the most sought-after French-speaking providers, pharmacists are reported as the least likely health care professionals to provide French services. 5 Furthermore, a 2022 study found a maldistribution of French-speaking pharmacists in Ontario, with the majority located in communities where fewer Francophones reside, leaving densely populated Francophone communities underserved. 6
Although financial incentives are often used to help recruit health care providers in underserved areas,7,8 such incentives have shown limited success in retaining providers long-term or addressing provider maldistributions.7,9 Furthermore, although nearly 12% of Canadian health care providers outside of Quebec can converse in French, only 5% regularly speak French in their workplace. 10 Therefore, improving access to FLS in pharmacies may require several strategies beyond a redistribution of French-speaking pharmacists.
Mise En Pratique Des Connaissances
La prestation de soins de santé linguistiquement concordants se traduit par de meilleurs résultats sur la santé.
L’offre proactive (appelée « offre active ») de services en français par le fournisseur de soins est un outil important pour les patients francophones.
Les pharmaciens ne connaissent pas les offres actives et les stratégies exploitables par les pharmaciens qui parlent anglais et français.
Les pharmaciens sont ouverts aux formations destinées à améliorer l’offre active proposée à leurs patients.
Accessibility is divided into the physical, financial, administrative, social, and informational components of care. 3 In a 2020 study, a series of focus groups with Francophone patients found that those who were receiving language-discordant care perceived the services as being inaccessible in terms of their ability to engage with the service. 11 Although pharmacies are considered physically accessible, an absence of bilingual signage within the pharmacy can be a cause for confusion for Francophone patients. From an administrative point of view, having pharmacists who can practice in French and advertising their availability can add to the administrative burden to ensure adequate staffing of French-speaking pharmacists, and it can be a cause of frustration for patients if no French-speaking pharmacists are available. 3 Language barriers can also prevent the establishment of longer term, trusting relationships with patients and are thus a barrier to the social component of pharmacy care. Regarding the informational component, language discordances pose a challenge when providing information and are a barrier to health education, 12 which is associated with medical mismanagement, confusion regarding medication use, misunderstandings of care plans and instructions on medication labels, 13 reduced medication adherence, 14 and increased risk of adverse events.13,15
The AAAQ framework defines acceptability of pharmacy services in terms of cultural appropriateness and sensitivity to gender identity and life course. 3 Inclusive to cultural sensitivity is a respect for language needs and preferences. Francophone patients receiving language-discordant care describe their experience as uncomfortable and unsafe and are less satisfied when care is provided exclusively in English.11,16
Finally, the quality and effectiveness of health care are challenged in part by language discordances.16-18 Language barriers are associated with increased patient risks and delayed care. 19 Furthermore, medication misunderstandings, misuse, and mismanagement described above are associated with increased avoidable hospital admissions and prolonged hospitalizations. 20
The active offer (AO) of FLS has been suggested as a method to improve access to linguistically appropriate health care services to Francophone minority residents and has been found to improve the patient experience. 16 The AO is defined as a proactive offer of services in French that is available at all times, clearly communicated, visible, easy to access, and of equal quality to and with similar wait times as the services being offered in English.21,22 An AO is a verbal or written invitation to express oneself in the official language of their choice. To be considered active, this invitation must precede the request, thus removing the onus to request services in French from the patient and placing it on the provider. 23 The AO of FLS provides strategies that can be implemented irrespective of French-speaking abilities, ensuring that those who are fluent in French are using it in practice whereas those with limited linguistic competencies are provided with tools needed to better serve linguistic minority populations.
Pharmacists are front-line health care workers valued for their accessibility to patients. However, there is no published literature regarding strategies to optimize accessibility of pharmacy services to Francophone minority communities in Canada. To date, no study has investigated the presence of the AO of FLS in Canadian pharmacies. This study aims to understand pharmacists’ knowledge, attitudes, and behaviours (KAB) regarding the AO of FLS in Ontario. We also discuss how the AO can help address all 4 elements of the AAAQ framework.
Methods
Data collection tool
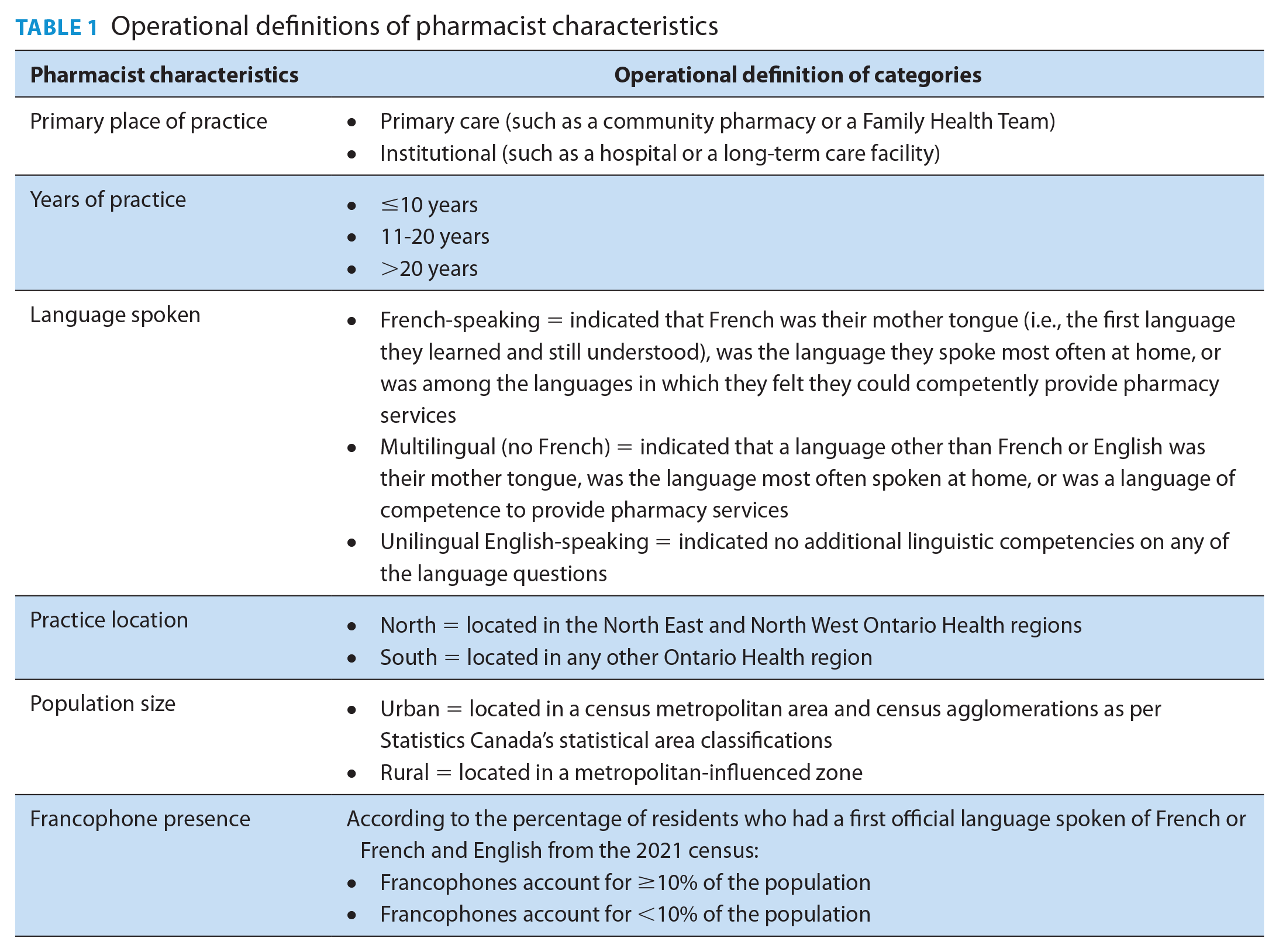
A survey was developed to measure the current state of AO of FLS by Ontario pharmacists. The questionnaire consisted of 2 main sections: “Demographics” and “KAB regarding AO of FLS in pharmacies”. The demographics section collected data on practice address, years of experience, type of practice, and languages spoken. Postal codes were cross-referenced with the 2021 Canadian Census and 2022 Postal Code Conversion File to determine pharmacists’ practice location (north vs south), the size of the community in which they practice (rural vs urban), and the Francophone population within the community in which they practice. Three questions were used to determine pharmacists’ ability to converse in French: their mother tongue, the language most spoken at home, and the languages of competence to provide pharmacy services.
The remainder of the questionnaire focused on KAB surrounding the AO of FLS in the pharmacy setting. Knowledge was measured using 5 close-ended questions and 1 open-ended question. First, pharmacists were asked about their familiarity with the AO of FLS, followed by 4 self-rated questions evaluating their level of knowledge (on a 5-point scale ranging from limited to expert) regarding the implications of language barriers in health care, and the availability of French language resources and communication strategies when serving French-speaking patients. These questions were created by the research team based on Le Réseau du Mieux-être Francophone du Nord de l’Ontario’s AO training modules. 24 Finally, pharmacists were asked to define AO in their own words.
Attitudes and behaviours were measured using select questions from the Active Offer of French Language Services in Minority Context Measure, which measures the frequency of various AO behaviours. 23 The development of this instrument consisted of a literature review identifying all practices and behaviours associated with an AO of French language health services, the results of which were validated with a pan-Canadian Delphi survey of expert consultants and pilot tested in a sample of 60 health care providers. 23 The results from this pilot test provided evidence of an acceptable level of internal consistency (Cronbach α ranging from 0.7 to 0.9) and showed signs of temporal stability. 23 In this survey, 13 questions measured attitudes toward AO by having pharmacists rate the importance of various AO strategies from the Active Offer of French Language Services in Minority Context Measure (using a 5-point scale ranging from strongly disagree to strongly agree). An additional 13 questions from the AO measure were selected to assess AO behaviours (using a 5-point scale ranging from never to always). The list of the KAB items is available in Appendix A (available online in Supplementary Materials). The wording of the attitude and behaviour questions was slightly adapted to better reflect the pharmacy setting by a panel of experts from the School of Pharmaceutical Sciences at the University of Ottawa and from the Ontario Pharmacy Evidence Network (OPEN). The final questionnaire was pilot tested with 5 pharmacists and translated in both French and English before being entered into the Qualtrics online survey platform.
Study participants and survey distribution
Ontario pharmacists with an active Part A license who had consented to be contacted for research purposes were sent an email with an individualized link to the study survey. Their contact information was accessed through OPEN’s data-sharing agreement with the Ontario College of Pharmacists (OCP). The survey was open for completion for 8 weeks (July 28 through September 15, 2022). Reminders were sent to non-responders at 1, 3, and 7 weeks after the initial distribution.
Analysis
Three independent scores were calculated by averaging responses on the 4 knowledge questions, the 13 attitude questions, and the 13 behaviour questions. Missing data were accounted for by imputing a prorated scaled score that filled in missing values with the individuals’ average scores from all completed questions and was appropriate when data had lower percentages of missing values with a 20% cut-off point often being applied.24,25 Thus, KAB scores were suppressed if 20% or more of the respective questions were unanswered.
Descriptive statistics were used to present participating pharmacist demographics and overall KAB scores and to identify the most and least commonly reported AO attitudes and behaviours. A series of t-tests and analyses of variance (ANOVAs) were used to compare differences in KAB scores based on the pharmacist characteristics defined in Table 1. Differences in individual KAB items were also explored using a series of chi-square tests. All statistical analyses were conducted using IBM SPSS Statistics Version 24. Ethics approval for the present study was provided by the Montfort REB#21-22-03-042 and the University of Waterloo ORE#44275.
Operational definitions of pharmacist characteristics
Results
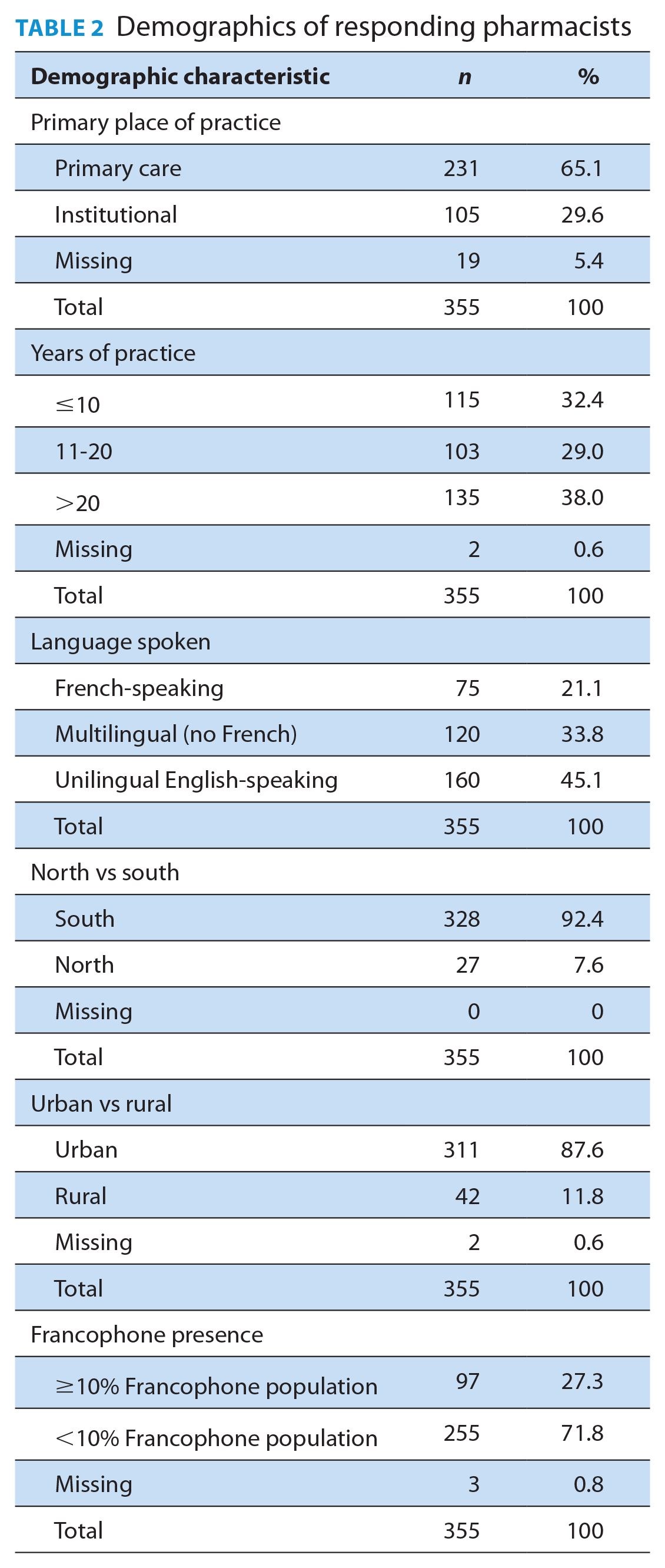
Of the 6557 pharmacists contacted, 360 (5.5% response rate) completed the AO survey. Five surveys were excluded because 2 were incomplete and 3 were completed by pharmacists outside of Ontario. The majority of responding pharmacists (65.1%) were practicing in a primary care setting and had been in practice for more than 20 years (38.0%) (Table 2). More than 20% of respondents were considered French-speaking; an additional 33.8% were multilingual but could not speak French, and 45.1% were unilingual English speakers. Geographically, 92.4% were practicing in Southern Ontario and 87.6% were practicing in an urban community. Regarding the presence of Francophone communities, most respondents (71.8%) were practicing in areas where Francophones constituted less than 10% of the population.
Demographics of responding pharmacists
Knowledge
When questioned whether they were familiar with the AO of FLS, only 20% of respondents indicated a familiarity with the concept. Overall, pharmacists reported an average knowledge score of 1.8 out of 5, representing limited understanding (Appendix A).
This limited familiarity was further demonstrated when respondents were asked to provide their own definition of the AO. More than a quarter of respondents (26%) either left the question unanswered or indicated that they were too unfamiliar with the concept to provide a definition. An additional 4% incorrectly identified AO as a translation service. Only 27 individuals (7.5%) correctly identified the proactive nature of the AO, specifically that the offer to be served in French should occur at the first point of contact and should precede any request, which is a key hallmark of the concept. An additional 23% of respondents provided various AO strategies as a definition, such as advertising the availability of FLS, inquiring about patients’ language preferences, greeting patients in both official languages, hiring bilingual staff, providing information and medication labels in French, learning to speak basic French, and using common expressions when communicating. Nine percent of respondents defined the AO as the general availability of FLS without identifying their role or the role of other health care providers in the provision of such services. More than 21% of respondents believed they themselves had to be fluently able to practice in French to provide an AO, suggesting they perceived the concept as irrelevant to them. Although being fluent in French is an advantage, it is not a prerequisite, and such a belief undervalues the important role that non-French speakers play in providing linguistically appropriate health care services to Francophone minority patients. Last, 7.5% of respondents defined the AO using terms that contradicted the concept of an AO. Some believed it meant offering services in French upon request only, whereas others indicated that the AO meant waiting for patients to speak with an accent, to have a French-sounding name, or to be noticeably struggling in English before offering services in French. Each of these strategies contradicts the proactive essence of the AO. Furthermore, a few respondents indicated that FLS were not needed because their Francophone patients were bilingual, demonstrating a lack of recognition for the importance of serving patients in the language of their choice.
Attitudes
Pharmacists had relatively positive attitudes toward the AO, with an average score of 3.8 out of 5, reflecting their agreement with the importance of various AO strategies in a pharmacy setting (Appendix A). Strategies considered most important included providing patient-friendly resources and information in French, providing French pharmacy labels, encouraging patients to express themselves in the language they feel most comfortable, and offering French counselling services. Respondents generally indicated that they agree to strongly agree with the importance of each of these strategies. Alternatively, strategies such as informing patients of the availability of French services without being asked, recruiting staff capable of offering services in French, and addressing patients in both official languages of Canada were deemed less important.
Behaviours
Despite favourable attitudes toward the AO, participating pharmacists reported an average AO score of 2 out of 5, suggesting infrequent practice of the most common AO strategies (Appendix A). The most frequently reported behaviours included asking bilingual pharmacy staff members for translation assistance, using the teach-back method, asking patients their preferred language, and obtaining and using French educational or information material (leaflets, pamphlets) that had been adapted to a patient-friendly language. These strategies were reported as occurring between rarely and sometimes. In contrast, the least common strategies (reported as occurring rarely to never) included requesting services from French-speaking interpreters, using French questionnaires when interviewing Francophone patients, greeting patients in French and English when answering the phone, and wearing identification indicating the ability to offer FLS.
Comparative analyses
The KAB scores were compared with respect to the various pharmacist characteristics defined in Table 1; the only characteristics that achieved statistical significance were differences in the presence of the Francophone population in the community of practice and the pharmacist’s language(s) spoken. Pharmacists who work in a community where Francophones represent 10% or more of the population had significantly higher scores compared with those in communities where fewer Francophones reside (Table 3). Similarly, French-speaking pharmacists reported significantly higher scores than multilingual non-French-speaking and unilingual English-speaking pharmacists. No differences were detected between the latter 2 groups in knowledge or attitudes. However, multilingual non-French-speaking pharmacists reported more frequent AO behaviours than their unilingual English-speaking counterparts. Although significant differences were observed, French-speaking pharmacists and those practicing in communities with a higher density of Francophones reported limited knowledge about the AO and demonstrated infrequent AO behaviours. No differences were observed based on the type of practice setting (primary care vs institutional), years of experience, or practice location (north vs south or rural vs urban).
Differences in KAB scores based on pharmacist demographic characteristics
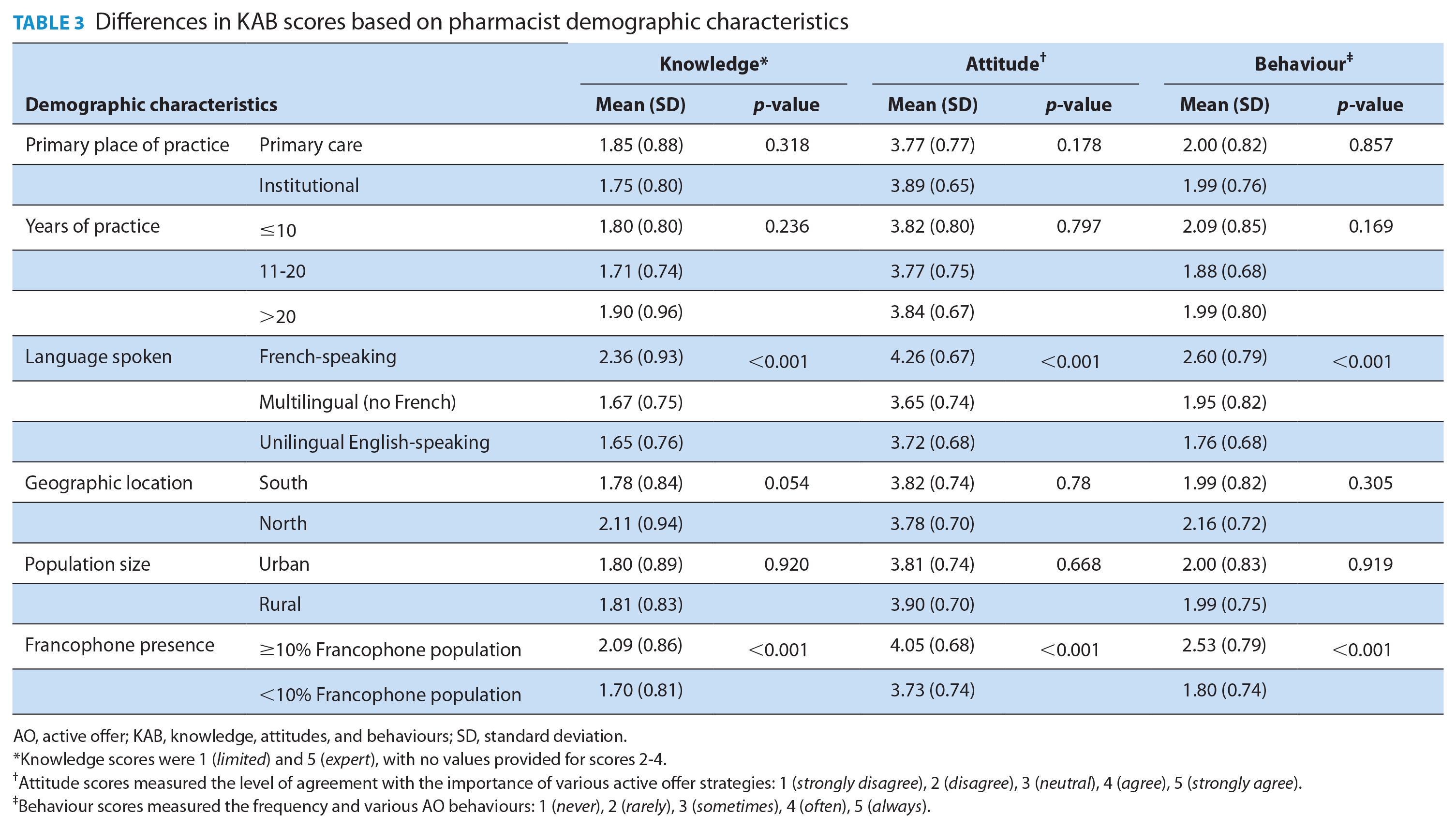
AO, active offer; KAB, knowledge, attitudes, and behaviours; SD, standard deviation.
Knowledge scores were 1 (limited) and 5 (expert), with no values provided for scores 2-4.
Attitude scores measured the level of agreement with the importance of various active offer strategies: 1 (strongly disagree), 2 (disagree), 3 (neutral), 4 (agree), 5 (strongly agree).
Behaviour scores measured the frequency and various AO behaviours: 1 (never), 2 (rarely), 3 (sometimes), 4 (often), 5 (always).
Active offer training
The majority (62.8%) of survey respondents agreed that further training would help them to better understand and implement the AO of FLS.
Discussion
Overall, participating pharmacists demonstrated limited knowledge of the concept of an AO of FLS, yet most had a positive attitude toward it, agreeing that many AO strategies were important in a pharmacy setting. However, AO behaviours were reported as rarely being practiced in Ontario pharmacies. Notably, there was a consistent tendency for French-speaking pharmacists and those working in communities with a higher density of Francophones to demonstrate greater AO attitudes and behaviours.
French-speaking pharmacists and pharmacists working in Francophone communities reported being more knowledgeable on every measure of knowledge. Although knowledge scores were higher among certain pharmacists, they were relatively low overall, suggesting limited knowledge within the profession. French-speaking pharmacists and pharmacists located in a Francophone community were also consistently more inclined to recognize the importance of strategies such as addressing patients in both official languages of Canada, conversing in French with French-speaking patients, asking which language would be preferred for medication counselling, and recruiting staff capable of offering French services. Finally, a review of the behaviours section of the survey suggests that pharmacists working in Francophone communities were more likely to provide patients with the option of hearing messages in English or French on their workplace phones, to seek help with translation, and to greet patients in both official languages. French-speaking pharmacists were more likely to ask patients their language preference, to greet patients in both official languages, and to assist patients in understanding educational or informational resources. Conversely, multilingual non-French-speaking and unilingual English-speaking pharmacists were more likely to request services from French-speaking interpreters or to ask bilingual pharmacy staff to help translate.
A pattern emerges from the data whereby pharmacists appear to undervalue the proactive nature of the AO. Very few pharmacists identified the proactive underpinnings of AO when defining the concept, with some even indicating that they wait for FLS to be requested before offering. Additionally, addressing patients in both official languages or offering services in French without being prompted was considered of little importance when measuring attitude, and greeting patients in both French and English was among the least frequent behaviours reported. This underscores the relative unfamiliarity that pharmacists have with regard to AO. Most pharmacists seem to underappreciate the very aspect that makes the offer of FLS active—namely, being proactive in their approach. According to the former FLS Commissioner of Ontario, it is vital for the AO to occur at the first point of contact with a service provider. 22 The first interaction sets the tone for the patient’s expectation for receiving future services in French. Starting in French builds confidence for the continued provision of FLS, whereas an English start may lead to an expectation of future English services, potentially leading patients to decline later French offers. 22 Although some pharmacists did report practicing certain AO behaviours, the entire profession could benefit from learning to implement AO more proactively, as indicated by most survey respondents who agreed that additional training would help them better understand and implement the AO.
Furthermore, all pharmacists and pharmacy technicians have a role to play in the AO, regardless of one’s ability to speak French. For instance, identifying the patient’s preferred language should be a best practice standard. Although following up on this question with FLS may be easier for French-speaking pharmacists, the AO provides many strategies for unilingual English-speaking and multilingual non-French-speaking pharmacists to adapt their communication style to meet the needs of minority-language populations. Examples include providing reading material and documentation in both official languages, using an interpretation service, using technology such as a translation app (e.g., Google Translate), hiring bilingual staff, knowing the linguistic abilities of their colleagues as a source of additional support, and learning a few basic words in French in order to proactively greet Francophone patients in their preferred language.26,27
That being said, the limited presence of AO behaviours by participating pharmacists is not surprising considering that only 4.7% of Ontario pharmacists report using French at work, with only 1.4% of those located outside of Ontario’s 2 largest urban centres, Toronto and Ottawa, reporting the use of French. 10 Furthermore, the state of AO in the pharmacy setting reflects the general lack of AO observed throughout Ontario’s health care system.28,29 For instance, undergraduate nursing students from the University of Ottawa had limited knowledge of the AO upon graduation and reported having received little training on the implementation of the AO. 30 Additionally, physicians practicing in Northern Ontario demonstrated similar gaps in their AO knowledge and behaviours as those observed in pharmacists. 31
AO through the lens of the AAAQ framework
As we discussed in the introduction, language-discordant pharmacy services are a barrier to accessible care. However, the AO can help address all 4 elements of the AAAQ framework. First, in terms of availability, although it will not improve the geographic maldistribution of French-speaking pharmacists, 6 the AO would provide all pharmacists (even those who are limited or non-French speakers) with the tools needed to better communicate with linguistic minority populations, thus improving the availability of language-concordant pharmacy services.
Second, many AO strategies directly address the accessibility of language-concordant care. 32 For instance, posting bilingual signage and hearing French-speaking staff converse in French will create a physical environment in which Francophone patients feel comfortable and confident engaging with staff in French; greeting patients in both official languages, asking patients their preferred language, and learning a few basic words and expressions in French will demonstrate a respect for the individual’s linguistic identity and communication needs and help build a social rapport; and providing handouts in both official languages, using the teach-back methods (where the pharmacist asks the patient to explain what was just said to them in their own words to ensure comprehension), and using a translator when needed will help ensure the information that is shared is well-understood.
Third, in terms of acceptability, the AO is a patient-centred approach to care delivery, with the goal of offering services adapted to the linguistic minorities’ culture to ensure that Francophones feel comfortable when receiving services.23,33 Accordingly, a positive and relatively strong correlation between AO and patient satisfaction has been observed, whereby Francophone patients are more satisfied when they perceive more AO behaviours by their health care provider. 16
Fourth, the relationship between language concordance and improved quality of care is well-established in the literature.34,35 The AO can affect quality in 2 ways. First, patients are more likely to seek, comprehend, and follow through on information in their preferred language.36,37 Second, Francophone patients are more satisfied with the care received when they perceive more AO behaviours from their provider, and satisfied patients are more likely to contribute to their own quality of care by returning to see the health care provider, disclosing crucial medical information, complying with medical recommendations, and actively participating in their own treatment.38,39
Policy implications
Somewhat surprisingly, given that many institutions are subject to Ontario’s French Language Services Act (FLSA), no differences in AO KAB were observed between community pharmacists and those working in institutions. In addition to ensuring that all services provided by the provincial government are available in both official languages (much like the Official Languages Act does at the federal level), a recent modernization of the FLSA has added a new subsection regarding the AO of FLS. 40
According to the new subsection, service providers are required to inform individuals who have a right to receive front-line services in French under the Act of the availability of such services from the initial point of contact. As a result, the modernized FLSA legislates the AO of FLS. With the passing of Bill 74, The People’s Health Care Act (2019), this responsibility has been extended to Ontario’s new integrated care delivery system, known as Ontario Health, and its respective Ontario Health Teams. 41 Bill 74 recognizes that the public health care system should respect the FLSA’s requirements, with section 6 of Part II emphasizing that 1 of the objectives of Ontario Health is to “respect the diversity of communities and the requirements of the FLSA in carrying out its objects.” 41 Thus, pharmacists working in a French-designated institution as well as those working within an Ontario Health Team are expected to practice the AO of FLS. The Ontario Pharmacy Act further states that pharmacists “must possess sufficient language proficiency, in either English or French, to be able to communicate and comprehend effectively, both orally and in writing”. Thus, adopting the AO of FLS would also ensure that pharmacists are compliant with these requirements.
Limitations and representation
Certain limitations of this study warrant further consideration. The consideration of generalizability arises, as only approximately 2.3% of Ontario’s pharmacist population responded to the survey. Nevertheless, characteristics of the sample that responded to the survey closely resemble those of the general pharmacist population in terms of years of experience and geographic distribution. For instance, a 2022 study of all practicing pharmacists found that 31.3% were in practice for 10 years or less (vs 32.4% in our sample), 25.2% were in practice for 11 to 20 years (vs 29% in our sample), and 43.5% were in practice for more than 20 years (vs 38% in our sample). Similarly, 94.7% of pharmacists worked in Southern Ontario (vs 92.4% in our sample) and 93% worked in an urban area (vs 87.6% in our sample). 6
Nevertheless, certain differences in our sample may limit the generalizability of our findings. Our sample had a higher proportion of pharmacists working in institutions (29.6% of the sample vs 19.1% of the general pharmacist population). 6 Considering that certain institutions are subject to the FLSA, it is possible that our sample was more aware of the AO of FLS than the typical pharmacist. Furthermore, our sample had a higher representation of French-speaking pharmacists (21.1% vs 7.2% of general pharmacists) and pharmacists working in a community where Francophones represent 10% or more of the total population (27.3% vs 11% of general pharmacists). 6 This tendency may be attributed to the inclination for French-speaking pharmacists and those who see more Francophone patients to participate in a study that they find particularly relevant to their professional context. Given the present finding that these pharmacists were more knowledgeable about the AO, it is quite likely that the average pharmacist is even less aware of the AO than our results suggest.
We must also acknowledge that we recruited solely from the OPEN-accessed OCP dataset. Although we do not know to what extent pharmacists in the dataset are representative of the general pharmacist population, it is reasonable to expect certain differences. For instance, those who agree to participate in research may be more attuned to recent findings in health research and more knowledgeable of concepts such as patient-centred communication and the AO of FLS. A larger, more diverse, and more representative sample would be needed to support our findings.
Finally, although the Active Offer of French Language Services in Minority Context Measure is a validated tool to measure AO behaviours, we are not aware of a validated instrument for assessing knowledge or attitudes. Consequently, the questionnaire used in this study, although designed by experts and subjected to pilot testing, carries inherent limitations.
Conclusion
This study is the first of its kind to document the state of KAB regarding AO of FLS in Ontario pharmacies. Although some participating pharmacists demonstrated a familiarity with AO, most had limited knowledge of the concept, particularly the proactive nature of AO. Pharmacists had relatively positive attitudes toward AO, being supportive of various strategies that could be implemented. However, a behavioural assessment shows that most common AO strategies are infrequently practiced in pharmacies. Most pharmacists surveyed agreed that further training would help them to better understand and implement AO of FLS. Furthermore, the AO can improve access to language-concordant pharmacy services by addressing all 4 elements of the AAAQ framework. A training module designed specifically for pharmacy practice is in development by the Réseau du mieux-être Francophone du Nord de l’Ontario as a means of addressing the current gaps in KAB of AO of FLS in Ontario pharmacies. ■
Supplemental Material
sj-pdf-1-cph-10.1177_17151635241308874 – Supplemental material for Reporting on knowledge, attitudes, and behaviours of pharmacists regarding the active offer of French language health services in Ontario: A quantitative survey study
Supplemental material, sj-pdf-1-cph-10.1177_17151635241308874 for Reporting on knowledge, attitudes, and behaviours of pharmacists regarding the active offer of French language health services in Ontario: A quantitative survey study by Patrick Timony, Arielle Leone, Carolanne Caron, Pierre Giguère, Pierre Thabet, Alain Gauthier, Nancy M. Waite and Christine Landry in Canadian Pharmacists Journal / Revue des Pharmaciens du Canada
Footnotes
Author Contributions:
Timony: conceptualization, methodology, formal analysis, writing—original draft preparation, writing—review and editing; Leone: conceptualization, methodology, writing—original draft preparation; Caron: conceptualization, writing—review and editing formal analysis, writing—original draft preparation, writing—review and editing; Giguère: conceptualization, methodology, analysis, writing—original draft preparation, writing—review and editing. Thabet: conceptualization, methodology, analysis, writing—original draft preparation, writing—review and editing. Waite: conceptualization, methodology, analysis, review and editing. Landry: conceptualization, methodology, analysis, review and editing, supervising. All authors have read and agreed to the published version of the manuscript.
Declaration of Conflicts of Interest:
Waite reports grants from Sanofi during the conduct of the study and personal fees from Sanofi, Novavax, and GSK outside the submitted work. All other authors declare no relevant conflicts of interest or financial relationships.
Funding:
No funding was received for this research. The authors of the study had full control of study design, data collection and analysis, decision to publish, and preparation of the manuscript.
Ethical Approval:
Ethics approval for the present study was provided by the Montfort REB#21-22-03-042 and the University of Waterloo ORE#44275.
Data Availability:
Data are available to review for this study upon request.
Supplemental Material:
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.