
Abstract
Background:
Deaf, deaf-blind, and hard of hearing (D/DB/HOH) individuals face communication challenges affecting their health, which can lead to medication errors. Pharmacists can mitigate medication-related errors for D/DB/HOH individuals, but there is a lack of evidence-based best practices. This study explored the experiences of D/DB/HOH people at a community pharmacy and offered practical solutions to improve pharmaceutical care for D/DB/HOH individuals.
Methods:
A qualitative study consisting of 5 focus group discussions occurred. Focus groups were formed based on participants’ ability to use sign language, their hearing ability, and their age.
Results:
Nineteen participants completed the study (8 HOH adults, 2 HOH seniors, 1 deaf-blind adult, 4 deaf adults, and 4 deaf seniors). Communication barriers depended on one’s hearing ability but included factors such as assuming one can hear, environmental noises around the pharmacy, pharmacists not knowing American Sign Language, and assuming individuals are proficient at reading English. Focus group participants shared the potential and actual impacts that communication barriers can have on health. Strategies to improve communication between hearing pharmacists and D/DB/HOH individuals are discussed.
Discussion:
This is the first study in Canada exploring D/DB/HOH individuals’ experiences at community pharmacies. Focus groups were effective at revealing the similarities and differences in pharmacy experience between D/DB/HOH folks, calling attention to access barriers and their impacts on health, and highlighting ways to better meet the needs of D/DB/HOH individuals.
Conclusion:
Communication barriers result in a lack of understanding of one’s medications. Pharmacists should ask about communication preferences and aim to reduce communication barriers for those who are D/DB/HOH.
Background
Deaf, deaf-blind, and hard of hearing (D/DB/HOH) individuals face several communication challenges affecting their health, including lower health literacy and language barriers. Reading skills are reported to be lower among deaf people than among people without a hearing disability, which can lead to difficulties in understanding medications. 1 The Canadian Association of the Deaf identifies a person to be deaf when the individual has little to no functional hearing and depends upon visual rather than auditory communication—such as sign language, lipreading, and writing. A HOH person has hearing loss that ranges from mild to profound and uses speech as their usual communication. 2
Knowledge into Practice
A patient’s communication preferences may vary, depending whether they are deaf, deaf-blind, or hard of hearing (D/DB/HOH).
Lack of access to health information was a common theme for D/DB/HOH individuals, as our systems are currently built for those without hearing loss.
This article provides practical tips on how to better care for D/DB/HOH patients.
Pharmacists not only should ask and accommodate their D/DB/HOH patients, but also should be aware of tools to support communication such as Canada’s Video Relay System.
A study from the United States found participants with hearing loss were 1.6 times more likely to report difficulty managing their medications. 3 This puts them at greater risk of medication errors and poorer health outcomes, such as more frequent emergency department visits. Another study reported that deaf American Sign Language (ASL) users had a 97% greater likelihood of visiting the emergency room over the past 3 years compared with the general population. 4
Deaf-blind individuals have reported similar experiences. The World Health Organization classifies visual impairment from mild or no impairment to blindness based on distance visual acuity. 5 In the United States, older people with vision impairment were 2.3 times more likely to report “poor” health compared to people without sensory problems and were approximately 3 times more likely to report difficulty taking medicines compared to those without sensory impairment—often depending on family members or care aides to help with medicines.6 -9
Current accommodations for D/DB/HOH individuals in Canada are limited. Signing D/DB/HOH individuals cannot request an ASL interpreter for most community pharmacies, as there is no funding or policy in place.
Anecdotal experiences in British Columbia have shown a handful of D/DB/HOH individuals visiting the emergency department due to incorrect use of their medications, leading to accidental overdose. These preventable emergency room visits likely could have been mitigated through appropriate communication during medication counselling to D/DB/HOH individuals.
Pharmacists are front-line health care professionals with medication expertise who can help mitigate medication-related errors for D/DB/HOH individuals. At the time of this project, there remained a lack of research and evidence-based best practices on how to meet the pharmaceutical needs of this group. Therefore, this study sought to explore the experiences of D/DB/HOH people at a community pharmacy in a Canadian context.
Mise En Pratique Des Connaissances
Les préférences en matière de communication d’un patient varient selon qu’il est sourd, sourd-aveugle ou malentendant.
Le manque d’accès à l’information sur la santé était un thème courant chez les personnes sourdes, sourdes-aveugles et malentendantes, car nos systèmes sont actuellement conçus pour les personnes qui ne présentent pas de perte auditive.
Cet article fournit des conseils pratiques sur la façon de mieux prendre soin des patients sourds, sourds-aveugles et malentendants.
Les pharmaciens devraient non seulement s’informer auprès de leurs patients sourds, sourds-aveugles et malentendants, et subvenir à leurs besoins, mais aussi être au courant des outils d’aide à la communication, comme le système de relais vidéo du Canada.
Methods
This was a qualitative study consisting of 5 focus group discussions. Participants were grouped into the following:
Deaf signing seniors (≥65 years old)
HOH non-signing seniors (≥65 years old)
Deaf signing adults (19-64 years old)
HOH non-signing adults (19-64 years old)
Deaf-blind individuals (≥19 years old)
Focus groups were formed based on participants’ ability to use sign language, their type of hearing ability, and their age in order to account for cultural differences. The deaf-blind participants were not grouped by age due to limited sample size. For each focus group, there were 2 facilitators, a social worker from Vancouver Coastal Health’s Deaf, Deaf-Blind, and Hard of Hearing Well-Being Program (aka, the Well-Being Program) and a pharmacist from the University of British Columbia (UBC). Two ASL translators were available for signing focus groups. The facilitators asked questions using a semistructured interview format and open-ended questions. Questions are provided in Appendix 1, available online in the Supplementary Materials. Study protocol, including the interview guide, was approved by UBC’s Behavioural Research Ethics Board.
Sample/participants
Recruitment methods included advertising with a flyer in written English and ASL in different formats accessible to D/DB/HOH populations on the Well-Being Program’s website and its Facebook and Instagram accounts. Recruitment materials were also sent to team members at the Well-Being Program to support snowball sampling. The study did not aim for data saturation but purposively recruited participants from varied backgrounds to capture different perspectives and experiences. Consent was provided/obtained on Zoom with interpreters available upon request. Inclusion and exclusion criteria are shown in Table 1.
Inclusion and exclusion criteria
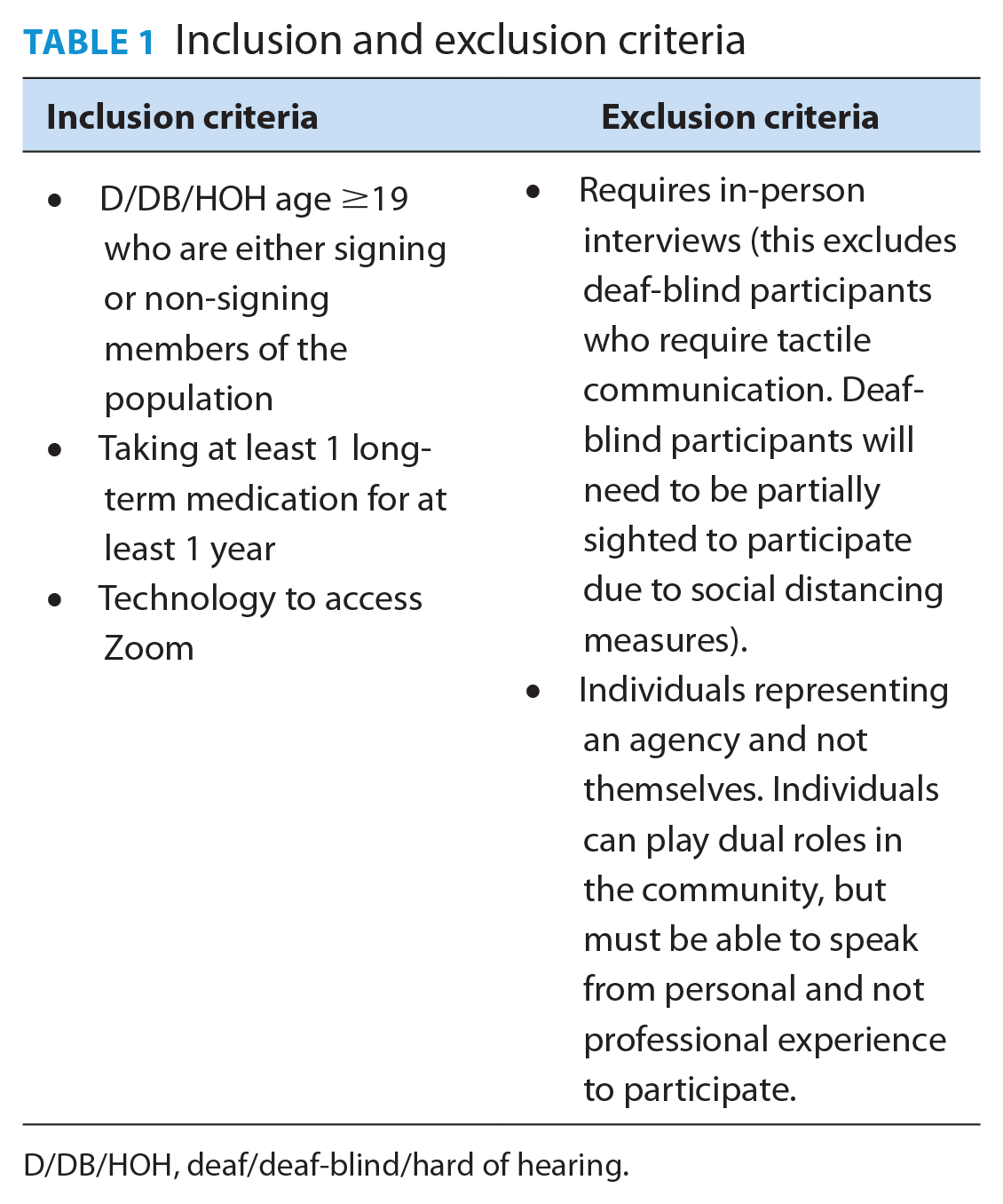
D/DB/HOH, deaf/deaf-blind/hard of hearing.
Data collection
Demographic data were collected using the Qualtrics survey tool. The font size on the demographics survey was increased to enhance accessibility. Focus groups hosted via Zoom were digitally recorded, transcribed, and anonymized.
Data analysis
Focus group transcripts were thematically analyzed to explore participants’ lived experiences, perspectives, and behaviours. The study applied an interpretive description approach to the qualitative data. 10 Independent coding and assessment of common themes were done inductively by 2 reviewers (M.T. and T.L.), and their findings were assessed for intercode agreement. Themes were finalized following discussions among the research team. Participant validation was achieved by sharing findings with participants to verify that research findings corresponded with community members’ lived experiences. 11
Results
Nineteen participants completed the study (8 HOH adults, 2 HOH seniors, 1 deaf-blind adult, 4 deaf adults, and 4 deaf seniors). Demographic information is presented in Table 2. The presentation of demographic data was adapted to accommodate cell size suppression rules (n < 5). One HOH participant did not complete the demographic survey. Due to larger enrollment in the HOH adult group, 2 focus groups were completed instead of 1 to accommodate for participants’ schedules. Each focus group was 90 to 120 minutes long and occurred from September 2022 to March 2023.
Baseline demographics
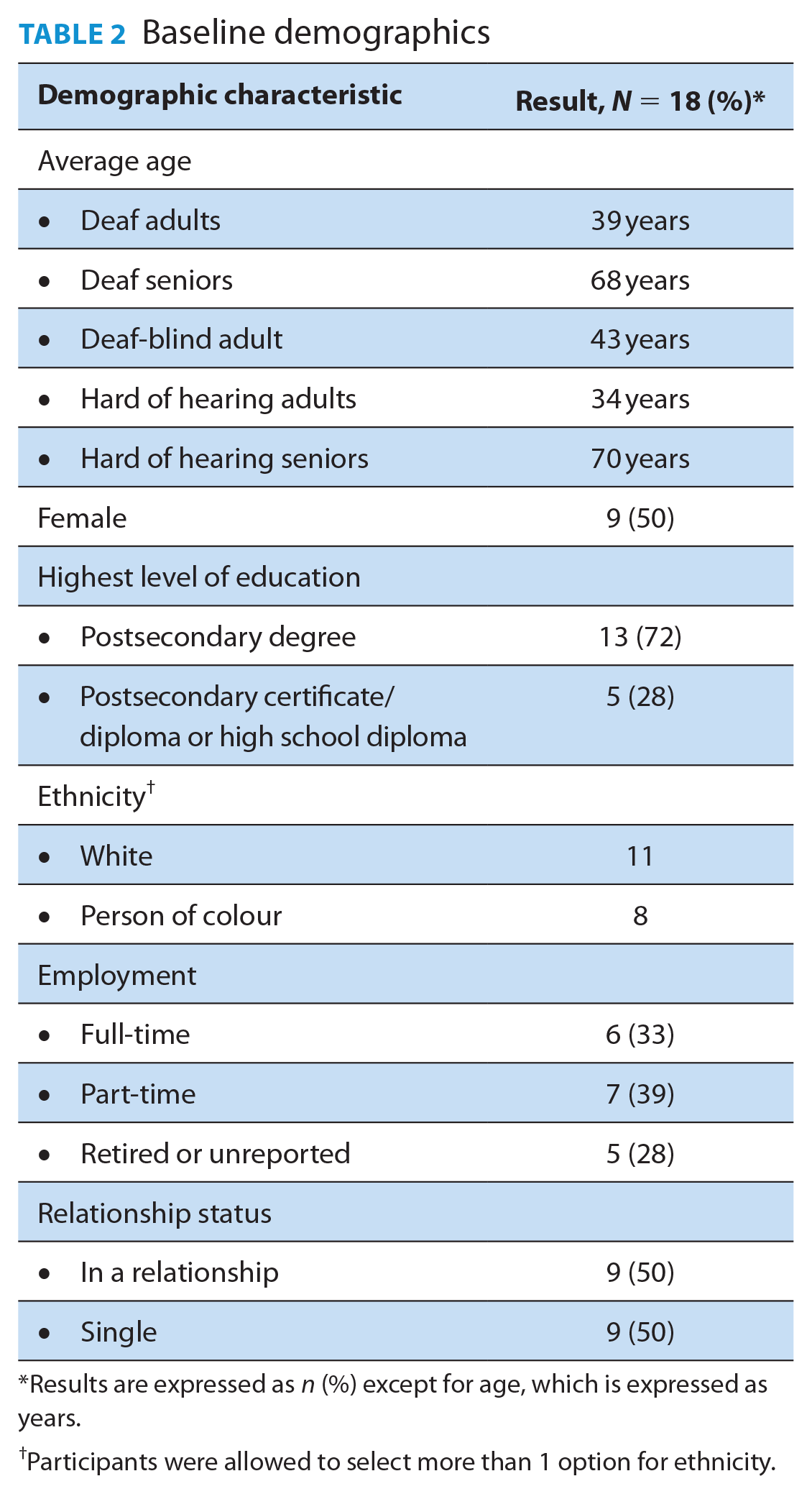
Results are expressed as n (%) except for age, which is expressed as years.
Participants were allowed to select more than 1 option for ethnicity.
Major themes identified in the focus group are shown in Figure 1 and are categorized into the following: (1) barriers to communication, (2) experience interacting with pharmacists and (3) impacts on health. Figure 1 also depicts the relationality between the 3 themes—that is, how communication barriers can influence one’s experience with the pharmacist, which can ultimately have health impacts.
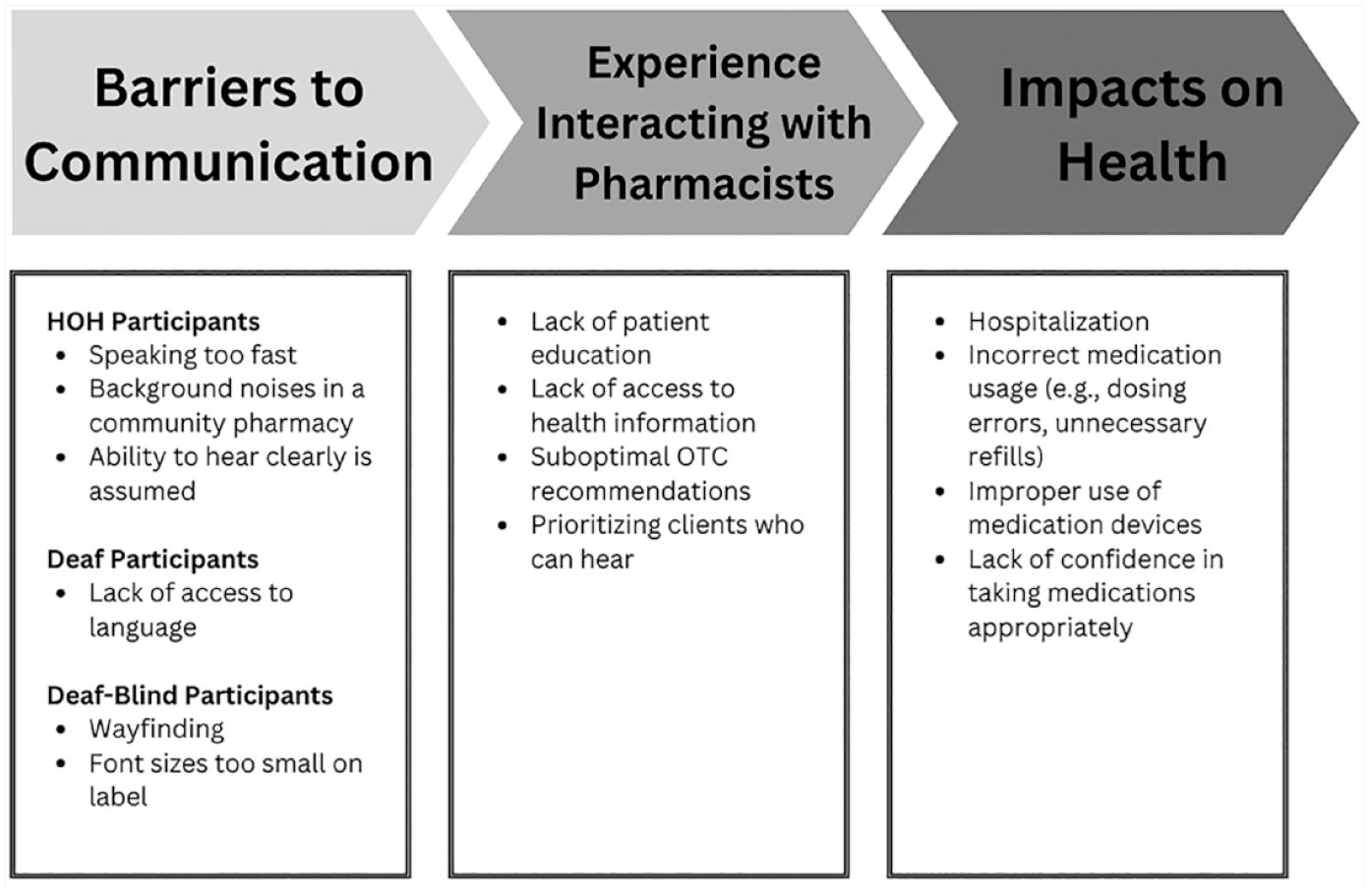
Key themes identified by focus groups
Barriers to communication
Communication barriers varied by hearing ability. For HOH participants, the major theme that arose was the assumption one can hear clearly: “When I got my COVID vaccine, I got the pharmacist to write down the side effects, what I should watch out for because I couldn’t hear what she was saying. I couldn’t understand.”—HOH senior
External factors, including the pharmacist not speaking loud enough or the physical space of the pharmacy, contributed to the difficulty in hearing clearly: “You can’t hear when a person talks low or muffles.”—HOH adult “It’s just completely noisy because it’s a grocery store and there’s lots of background noise.”—HOH senior
The theme of lacking language access arose among the deaf focus groups. Barriers to accessible language included the following:
1. The assumption that people can read English fluently
“I’ve had to read something 2 or 3 times to be able to comprehend what it’s telling me . . . but that doesn’t mean everybody has the same access to the language I do, so there can be a problem.”—deaf adult “They give such brief explanations, but I want a full explanation, and reading the written English is not accessible.”—deaf senior
2. Pharmacists or pharmacy teams not being able to sign
“Most pharmacies will not have ASL-speaking pharmacists.”—deaf adult
3. Limited resources in ASL
“Some medication information is in ASL, which I’m glad for . . . it would be nice to have all medications translated into ASL.”—deaf adult
One deaf-blind participant was recruited for the study and had some vision. They were able to see if they read up close or used an app to magnify text. They found their visual ability more of a barrier than their hearing ability: “Oftentimes the prints are really small, so that’s not always accessible.”—deaf-blind adult
A similarity shared between all groups was that physical barriers such as masks and plexiglass negatively affected communication during the COVID-19 pandemic. Masks impeded participants’ ability to lip read if needed or to hear information clearly: “The 2 places that I go [to] are still behind plexiglass and being hard of hearing is just challenging.”—HOH senior “I mean, with a mask on, it’s obviously totally impossible [to lip read].”—HOH adult
Experience interacting with pharmacists
None of the participants were aware that pharmacists can provide medication review services at the community pharmacy, but the participants expected pharmacists to dispense medications safely, administer vaccines, provide patient education, and be friendly during patient interactions.
The experiences of D/DB/HOH participants were similar in that each group expressed a lack of access to health information, such as patient education on prescription medications and over-the-counter (OTC) counselling. Participants attributed this to prioritization of hearing patients in the pharmacy, lack of patience, and/or the time it takes to communicate with them: “Being an immigrant, having less privilege than others, feels as if they prioritize other people ahead of seeking my needs . . . you know, not a good experience.”—deaf adult “Hearing people can quickly grab somebody and say, ‘Hey, I need to ask you a question,’ [but] deaf people take a lot longer to communicate . . . we are kind of the last people to know what’s going on because it’s more time.”—deaf senior
Participants reported positive experiences when pharmacists accommodated them (e.g., writing down instructions, typing, or texting) and demonstrated patience during the encounters. Most participants across the focus groups expressed either general satisfaction or indifference with their experiences at a pharmacy and with a pharmacist. However, there were also sentiments of frustration: “I would say satisfied [with my pharmacy experience] but challenged.”—HOH senior “Having gone into the pharmacy, you can communicate via writing. Sometimes they don’t respond to the sentence that I have written, and then they’re talking to somebody else while I’m trying to get the service, and I’m trying to write back and forth with them, but I feel brushed aside . . . then somebody else takes on the writing, back and forth, and so it’s pretty frustrating.”—HOH senior
Communication barriers also lead to mistrust. For instance, a patient expressed her frustrations when separate communications with her physician and pharmacist led to more confusion regarding whether she should or should not take acetylsalicylic acid: “[It] feels really frustrating when you’re getting different information from 2 different professionals, like, I feel like there’s a piece missing in the puzzle . . . I don’t trust that they’ll know what I’m talking about.”—deaf senior
Impacts on health
Focus group participants shared both potential and actual impacts communication barriers have had on health. Impacts included hospitalization, incorrect medication usage (e.g., dosing errors or unnecessary refills), improper use of medication devices, and overall lack of confidence in taking medications appropriately.
One participant shared how their lack of confidence in taking medications influenced their behaviour around medications. Specifically, since they have a hard time communicating with the pharmacist, they avoid asking for OTC recommendations and will endure their ailment to avoid any risk of medication-related adverse events: “I don’t buy anything over-the-counter because I don’t want to do something wrong. I’d rather be safe.”—deaf senior
Another patient shared an experience where they had an adverse event from taking a medication that contained sulfate, but sulfate was not put on their pharmacy profile as an intolerance: “I do remember having dizziness and fainted, actually fainted, because of the wrong medication.”—deaf senior
These impacts on health are the result of communication barriers and experiences between the pharmacists/pharmacy and study participants.
Moving forward and recommendations
A major takeaway from each focus group was the need for mutual access to a shared language for clearer interactions with the pharmacist. One participant emphasized the value of a common language by expressing their willingness to go out of their way to have a pharmacist who can sign: “I do want to emphasize that I would be so happy to drive out of my way to a pharmacist that could sign . . . to be able to have that conversation in my own language . . . it just . . . it really makes a difference.”—deaf adult
This quote underscores the magnitude of desire D/DB/HOH folks have for health care that is accessible to them.
In the focus group, participants were asked their communication preferences at a pharmacy. These are presented in Table 3. Deaf participants preferred American Sign Language as their first choice and written language as a second. They will resort to lip reading as a last option. A unique point brought up was the fact that people assume all deaf people can lip read: “Oftentimes lip reading can be quite confusing. Different letters, like ‘B,’ ‘P,’ even ‘M’ . . . when you’re trying to lip read, they all look the same . . . a lot of people assume that deaf people are great at lip reading.”—deaf adult “You can only access up to 30% of what is being said from lip reading, the other 70% of information is guesswork.”—deaf adult
Communication preferences between hard of hearing, deaf, and deaf-blind groups
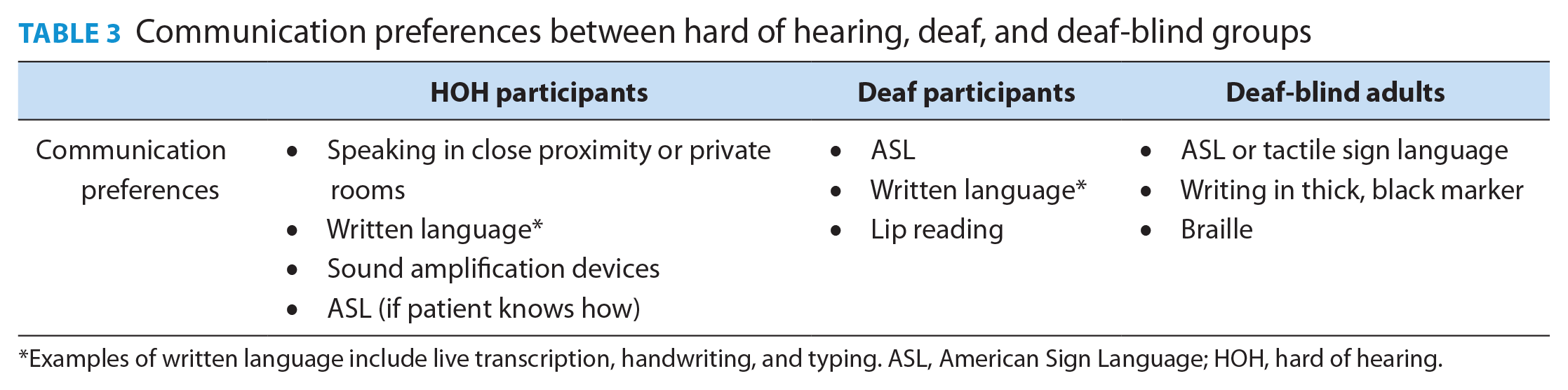
Examples of written language include live transcription, handwriting, and typing. ASL, American Sign Language; HOH, hard of hearing.
The deaf-blind participant shared the desire for access to tactile methods of wayfinding around OTCs and differentiating medications. HOH participants preferred communicating through speaking nearby and written language: “If they could just turn [the monitor] around when somebody is struggling to hear them . . . if they can just type it . . . because reading is just so much easier.”—HOH senior
Several focus groups emphasized using technology such as the Canada Video Relay System (VRS) to interact with people who are fluent in ASL: “I think that the law needs to . . . make sure there’s accessibility for deaf, hard of hearing, and deaf-blind people [for] anything to do with health care needs . . . when you’re communicating with them, a remote video interpreter should be required.”—deaf senior “I think it’s important [to] be aware that video relay services exist so that when they do get a phone call, they can recognize it for what it is.”—deaf adult “If they can write English by pen and paper or texting . . . and when you phone in for prescriptions you can also use video relay services.”—HOH senior
Another form of technology brought up in the HOH focus group included sound amplification devices. Avoiding medical jargon, having resources like medication pamphlets communicated in ASL, and using larger font sizes for those with visual impairments were also expressed.
Education was a clear motive in moving toward better care. A lack of education on the needs of D/DB/HOH people appeared to be a root cause of the dissatisfaction with pharmacy services. The deaf-blind participant shared that he thought that a presentation to pharmacists on deaf-blind culture by a deaf-blind person would be impactful. Other sentiments included the following: “I don’t think that’s a focus of their education—to learn about different disabilities.”—HOH adult “English is my fourth language and I still struggle with it. Educating pharmacists about who their customers are and the layers of who we are . . . we live in a diverse community . . . and then you add in someone who’s deaf, whose first language is not English or ASL . . . so [there’s] another layer of communication barriers.”—deaf adult
Discussion
This is the first study in Canada exploring the experiences of D/DB/HOH individuals at community pharmacies. Focus groups were effective at discerning the similarities and differences in pharmacy experience between D/DB/HOH folks, calling attention to access barriers and their impacts on health, and pointing out ways to better meet the needs of D/DB/HOH individuals.
Existing literature looking at the experiences of D/DB/HOH patients with pharmacists and pharmacies is very limited. All existing literature available was conducted outside Canada. In 2015, Ferguson and Liu conducted a similar study with focus groups and searched for qualitative themes. 1 The results shared similar findings to this study, including the reliance on written communication, the assumption that all deaf or HOH (D/HOH) people can lip read, the awareness that pharmacists can administer vaccines, and the recognition that VRS can be an effective way to communicate with deaf people. The similarity in results from that study and our study suggests the universal experiences of D/DB/HOH individuals with pharmacists.
Another study, which explored the pharmaceutical care needs of older people with sensory impairments (i.e., visual, auditory, or dual impairment) on 4 or more medications in Scotland, yielded similar experiences for deaf-blind seniors. 12 Difficulty navigating through the pharmacy and strong reliance on a care provider to support the individual were also observed.
Previous studies have articulated the low health literacy of D/HOH individuals.4,9,13,14 A study by Paracha et al. 13 found that 12% of study participants took a prescription medication without understanding how or why. In our study, most participants were able to read, although discussions in the focus groups suggested differing levels of comprehension. For instance, a participant expressed sometimes not being able to understand the medication pamphlet dispensed along with medications at the pharmacy, while others mentioned that reading the medication pamphlet was helpful or that they referred to online resources to learn about the medication. Irrespective of reading comprehension, participants expressed minimal access to patient education due to difficulties communicating with the pharmacist in all focus groups.
In our study, there was a mention of apps to support patients in the pharmacy in the deaf-adult group. Our literature search revealed 2 studies where deaf patients provided feedback on an app designed to facilitate communication between pharmacists and the deaf community. 15 Apps that support communication between D/HOH folks are a unique solution to the identified gaps in care.
Limitations of the study include a small sample size. A possible reason for the small sample size and not being able to recruit 5 participants in each group can be attributed to the online format of the study. Not all interested individuals in the recruitment phase were able to use Zoom, and the deaf-blind group requested in-person meetings for tactile signing. Another limitation of this study includes not collecting data on the number of medications each participant took in order to potentially explore the impacts of polypharmacy in these populations.
Conclusion
This study highlights the saliency for pharmacists and pharmacy teams to better understand how to provide care for D/DB/HOH individuals and develop strategies to communicate with these populations. Improvements are needed to allow these people to access pharmacy services and receive safe and effective pharmaceutical care. Communication barriers result in a lack of understanding of one’s medication and are a risk for potential or actual adverse drug events. Pharmacists should ask about communication preferences and aim to reduce communication barriers for those who are D/DB/HOH. ■
Footnotes
Author Contributions:
Timothy Lim applied for grant funding, mentored PharmD students, supported with ethics submission, implemented the study protocol and analysis, and participated in manuscript write-up. Mel Tsai reviewed the grant proposal, helped with ethics submissions, conducted study analysis, and participated in manuscript write-up. Alecz Reyes helped write the grant proposal, reviewed and edited transcripts, reviewed analysis, and participated in the manuscript write-up. Anita Kapenen reviewed the grant proposal, supported with ethics submission, supported with analysis, and reviewed the final manuscript. Felicia D’Amato applied for grant funding, implemented the study protocol, reviewed analysis, and reviewed the final manuscript.
Declaration of Conflicts of Interest:
No conflicts of interest to declare.
Ethical Statement:
Study protocol, including the interview guide, was approved by UBC’s Behavioural Research Ethics Board.
Funding:
This project was funded by the Vancouver Coastal Health Research Institute Research Challenge.
Supplemental Material:
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.