
Abstract
Lower limb rehabilitation exoskeleton robots (LLRERs) play a positive role in lower limb rehabilitation and assistance for patients with lower limb disorders, and they are helpful to improve patients’ physical status. More and more experiments pay more attention to the kinematic and dynamic data characteristics of different patient groups. However, it is not clear whether these devices have broad adaptability and their clinical significance, so it is necessary to summarize and analyze these research results. This paper summarizes the LLRERs prototype and product in recent years, also compares the advantages and disadvantages of the theory and technology used in these research, and compares the functional characteristics of the devices, finally summarizes the aspects of the LLRERs to be improved. These devices apply advanced theories, techniques or structures, as well as human kinematics and dynamics data. However, due to the complexity of human body characteristics and movement rules, the theory or technology applied in the study design of LLRERs remains to be further studied, which can be improved in many aspects, such as improve the human-computer cooperation of equipment or carry out clinical trials. This paper can provide reference for researchers and designers in the future study, as well as understanding and selecting LLRERs for all kinds of therapist and patients.
Keywords
Introduction
One of the main reasons that people with lower limb dysfunction can’t autonomously complete basic activities of daily life is that their neural pathways are blocked. Medical knowledge has shown that repeated exercise reactivates the patient’s neural pathways. 1 LLRERs combines artificial intelligence and mechanical power device to help patients with lower limb movement and enhance muscle vitality, 2 which is a direct and effective means to compensate, replace or repair physical dysfunction, it is also one of the important ways to solve the problem of nursing shortage caused by population aging. 3 LLRERs are sturdy and durable, which can enhance the self-care ability of patients. LLRERs provides the possibility for the patients with lower limb disorders to return to society. 4 LLRERs also could reduce the burden on families and society.
In recent years, scholars have designed a variety of LLRERs, which can realize the movement and rehabilitation assistance for different joints, gait, as well as the daily life activities. The hip exoskeleton robot can improve the stability of the trunk, reduce the metabolic consumption, has a global impact on lower limb.5,6 Shi et al. 7 studied the torque field control for robot rehabilitation. The proposed control method can realize proper posture control of joints with three degrees of freedom or posture control of extremity end effectors. It is suitable for hip joint rehabilitation and can provide reference for controlling rehabilitation robots. The knee exoskeleton designed by Luo et al.8,9 can provide power for the knee joint of the patient, effectively generating assistance that are voluntary and intuitively controlled by the user’s muscle activity. The ankle exoskeleton designed by McCain et al. 10 could realize speed adaptive adjustment, improve the stress condition of the ankle joint, and protect the user from further injury during robot assisted movement or rehabilitation. Pan et al. 11 designed the LLRE system for gait rehabilitation and proposed the multi-loop modulation method (MMM; 3M), with better gait tracking response and stability, can assist the user to achieve normal gait. The rehabilitation robot designed by Singh et al. 12 can realize joint trajectory control. There are also some commercial devices that have been widely used in clinical practice. For example, LOKOMAT 13 is a new type of robot that can simulate physiological gait trajectory, drive the patient’s unilateral or bilateral lower limbs, and accurately control the speed of the treadmill to match the patient’s gait Consistent, organically integrate functional exercise therapy with the patient’s assessment and feedback system. Ekso Bionics 14 is a wearable exoskeleton that provides power to the legs. Designed to help patients stand and walk during rehabilitation, EksoNR works with clinicians to give the necessary support to the spine, trunk, and legs including hip, knee, and ankle joints promoting correct movement patterns in physical rehabilitation and challenging patients toward walking out of the EksoNR rehabilitation setting and back into their communities. EksoNR is also become the first exoskeleton cleared by the US Food and Drug Administration (FDA) for medical applications in treating patients with strokes, brain injuries, and SCI.
From these research results, it can be found that LLRERs plays a positive role in lower limb rehabilitation and assistance for patients with lower limb disorders, and is helpful to improve patients’ physical status. More and more experiments pay more attention to the kinematic and dynamic data characteristics of different patient groups. It is necessary to summarize and analyze these research results.
Materials and methods
The main purpose of this review is to summarize the state of the art of LLRERs and its control methods that are effective, advanced, and practically applicable through scholars’ research and experimental verification. According to the position of the LLRERs and the functions, it is divided into joints rehabilitation exoskeleton robots (JRERs), gait rehabilitation exoskeleton robots (GRERs), and daily life assistive exoskeleton robots (DLAERs). And summarizing the advantages and disadvantages of various robots and the applied technologies, providing a reference direction for subsequent LLRERs research, and can also help people with disabilities to understand and choose LLRERs.
We conducted an extensive search of articles related to LLERRs. The literature search was conducted from April to July 2020. The detail search results of each database are as follows:
IEEE Xplore (33 records) and Springer link (291 records) and Mendeley (35 records), by using the following groups of descriptors: “(Lower limb rehabilitation) AND (Exoskeleton) AND (Hip joint, Knee joint, and ankle joint).”
Science Direct databases (269 records), by using the following groups of descriptors: “(Rehabilitation assistive devices) AND (Rehabilitation) AND (Hip, Knee, ankle joint) AND (Exoskeleton) AND (Lower-limb Rehabilitation Robot).”
SAGE journals (97 records), by using the following groups of descriptors: “(Rehabilitation) AND (Hip, Knee, ankle joint) AND (Exoskeleton) AND (Lower-limb Rehabilitation Robot).”
PubMed (58 records), by using the following groups of descriptors: “(Exoskeleton) AND (rehabilitation) AND (lower limb joint) AND (lower-limb rehabilitation robot).”
Web of Science (136 records), by using the following groups of descriptors: “(Exoskeleton) AND (rehabilitation) AND (lower limb joint) AND (lower-limb rehabilitation robot) AND (lower limb).”
The inclusion criteria were: Original articles written in English, published until 2020, and articles related to the use of LLERRs to treat symptoms. Articles related to exoskeleton design such as lower limb joint rehabilitation and gait rehabilitation.
Data analysis: The references is divided into single-joint exoskeleton, gait rehabilitation exoskeleton, and daily life assisting robots according to the functional parts and names of the equipment designed by the author of these articles. In addition, the included articles all have structural design and experiments (design paper and test paper).
The exclusion criteria were: papers not related to the research topic, repetitive articles, articles related to walking aids for the blind and children’s rehabilitation aids, and papers other than English. On this basis, we first searched 919 papers. After reading the title and abstract and applying the inclusion and exclusion criteria, we excluded some papers related to children’s rehabilitation aids and walking aids for the blind, and finally 95 papers an overall assessment is required.
Result
Joint rehabilitation exoskeleton robots (JRERs)
Hip exoskeleton robots (HERs)
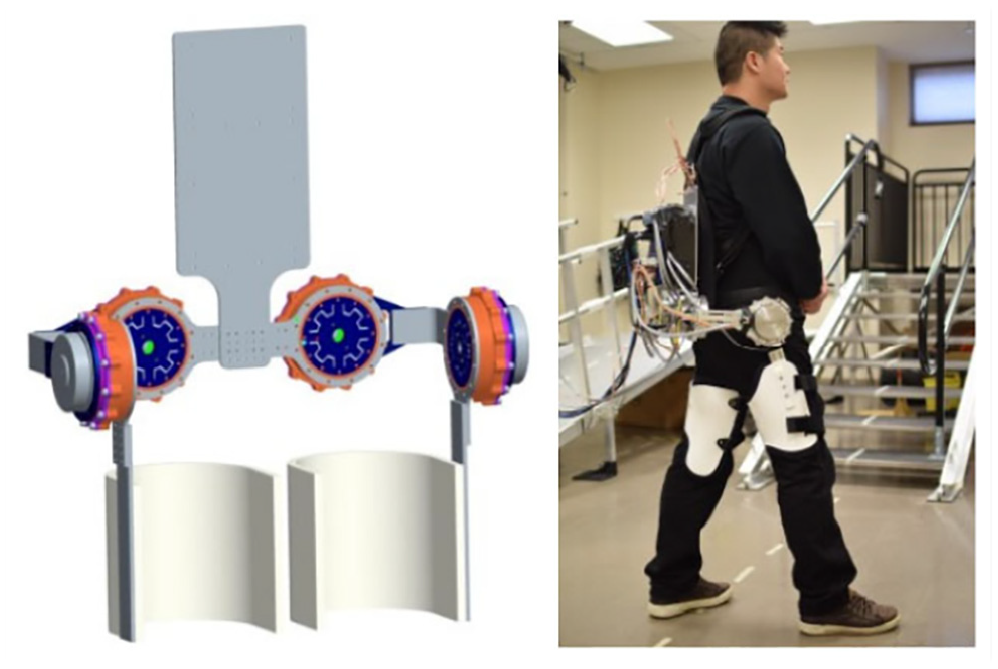
Ding et al. 15 designed an IMU-based iterative controller for hip extension assistance, which can evaluate the user’s state from the aspects of biomechanics and physiological responses, so as to determine the most suitable assistance mode for hip joint extension for patients during walking. Xue et al. 16 designed a new wearable hip joint exoskeleton, the flexible hip assistive exoskeleton with 4 DOF aligned with hip, which reduces the inherent mechanical impedance of the robot, realizes the compliant man-machine interaction, and realizes the walking intention estimation, provides comfortable and effective walking assistance for patients and reduce their metabolic consumption. Zhang et al. 17 designed an asymmetric fully constrained parallel mechanism prototype that has three rotation degrees of freedom and three actuations, as shown in Figure 1. Novel parallel mechanism is synthesized and designed to provide assistance for the movement of hip joint. The asymmetric parallel mechanism (PM) with constrained is easy to design and the requests of machining and assembling are relatively low compared with symmetric PM. Developed a robotic hip exoskeleton called GEMS driven by motor. As shown in Figure 2, the thigh frame consists of two flexible plates that are constrained to slide on each other along the longitudinal direction. The exoskeleton can improve the gait function of users and reduce the metabolic cost of walking. The device is beneficial to the rehabilitation of patients after stroke and muscle strength of the elderly. Zhang et al. 18 developed the robot hip exoskeleton named NREL Exo, as shown in Figure 3, The exoskeleton is driven by series elastic actor (SEA), which can help users actively participate in walking, and provide balance assistance for individuals with muscle weakness. The rehabilitation robot designed by Zhang et al. 19 used an asymmetrical three-degree-of-freedom parallel mechanism to assist patients with hip joint stroke or trauma. As shown in Figure 4. The device using the reciprocal and closed-loop motion conditions, an improved force transmission index based on the previous method is proposed. A multi-objective optimization model is established. The device allows patients to use prone position for training, reducing physical burden. Mahdavian et al. 20 proposed a wearable HER based on ground reaction force and moment (GRF/M), as shown in Figure 5. It can help users to perform hip joint flexion and extension exercises and help users walk normally. Guzmán et al. 21 proposed a control strategy based on generalized proportional integral (GPI) controller. Although patients’ weight is different, the gain of GPI controller does not need to be changed. This make HERs have higher adaptability. However, there is a common problem in the adaptability of robots that there will be a time delay between self-learning and reaction, and the delay may increase with the increase of time and reduce the safety. Improving the efficiency of adaptive adjustment should also be the focus of future research.
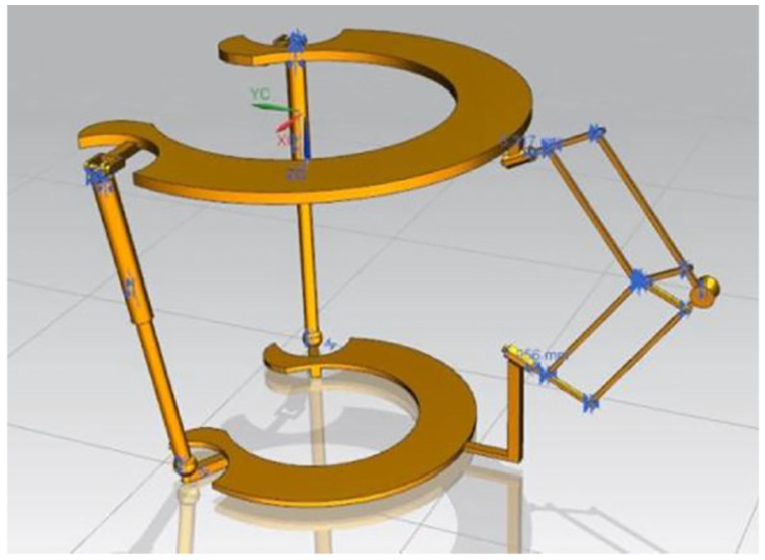
Hip joint assistant asymmetric parallel mechanism prototype. 17

The evaluation system with GEMSv2 fastened. 16
NREL-Exo prototype. 18

HipBot. 19

Optical marker placements for motion tracking while wearing the hip exoskeleton. 20
The structure of the hip exoskeleton is similar, mostly worn on the hip and the root of the thigh. These HERs can assist patients with hip joint flexion/extension/abduction and adduction rehabilitation exercises. However, the degree of freedom of the human hip joint in space is multi-dimensional. Although the current degree of freedom design can achieve a good auxiliary effect, it still needs to be improved to improve the human-machine cooperation.
Knee exoskeleton robots (KERs)
The knee joint is the main lower limb motor joint and the most vulnerable and susceptible joint. 22 The KERs can improve the leg movement ability, reduce the movement consumption, and provide power and assistance for the lower limb movement. Kamali et al. 23 proposed a kind of knee exoskeleton, as shown in Figure 6. The equipment uses a linkage mechanism. The inverse dynamic model is used to calculate the power and torque distribution of the knee joint, the initial joint angles as the input to predict the user’s intended sit-to-stand trajectory. Experimental results showed that the exoskeleton could provide strength support for the patient’s knee joint during sitting to standing. Gams et al. 24 proposed a prototype of robot knee exoskeleton, as shown in Figure 7, the equipment uses a linkage mechanism. It can provide power for users to squat. Experiments have proved the feasibility of the equipment.

FUM-knee exo. 23

Robotic knee exoskeleton. 24
Kim et al. 25 designed a modular knee exoskeleton system to support the knee joint of hemiplegic patients. The knee joint is designed to actively follow the polycentric path using a four-bar linkage structure, which could realize the multi-center motion of real human knee. The device weighs only 3.5 kg. The foot is equipped with a force sensitive resistor (FSR) sensor, the knee joint is equipped with a torque sensor. This exoskeleton could identify the movement intention of users, and provide walking assistance and sitting posture correction for users. Aguirre-Ollinger et al. 26 designed a single DOF knee exoskeleton, which could improve the swinging movement of the legs of the elderly. The increase of inertia compensation enables subjects to recover their normal motion frequency. Lee et al. 27 designed a knee exoskeleton with a multi-center (multi-axis) structure to minimize the misalignment between user and robot. Torque transfer can be carried out effectively and can provide a slightly lower speed than normal walking speed, which is suitable for passive walking rehabilitation training. This technology is expected to be developed to simulate the multi-dimensional motion of the human knee joint.
The exoskeleton designed by Sherwani et al. 28 applied an adaptive RISE (Robust Integral of Sign Error) controller, which has good robustness and the efficiency of tracking the reference trajectory. It can calculate the patient’s intention to control the walking trajectory or movement according to the electromyogram signal, and can assist users to achieve knee flexion/extension movement. Zhang et al. 29 proposed a wearable soft knee exoskeleton. The IMUs control system could measure the knee joint angle information. The average metabolic cost of walking can be reduced by 6.85% by helping the knee joint move during walking. The patient’s movement intention and the actual movement of the lower limbs are not uniform. The combination of these two technologies can make the knee exoskeleton more intelligent and make the patient more secure.
Ankle exoskeleton robot
The ankle joint supports the human body’s activities such as standing, walking, sitting, and standing transfer, the ankle joint provides most of the energy to support the individual’s activities.30,31 The lightweight passive ankle exercise device studied by Wang et al. 32 consists of four parts: the clever clutch, an extension spring, a shank brace, and a shoe, the spring can store and release energy, as shown in Figure 8. The device can assist the walking process, allow the ankle to move freely, which is suitable for nearly all users. Shao et al. 33 proposed an adaptive ankle exoskeleton for walking assistance. A new compact variable stiffness SEA (PVS-SEA) with nonlinear spring is developed. The physical stiffness of exoskeleton can be changed with the change of ankle joint, which can adapt to walking tasks at different speeds. Zhang et al. 34 proposed to use electromyography (EMG) signal to control the ankle exoskeleton. Four layer feed-forward neural network model and back propagation training algorithm are used. The experimental results shows that this method can accurately control the ankle dorsiflexion and plantar flexion. If PVS-SEA can be combined with EMG, the exoskeleton will become very flexible, and the stiffness of the device can be directly adjusted according to the patient’s body state instead of calculation and prediction, which will greatly improve the comfort of the patient.
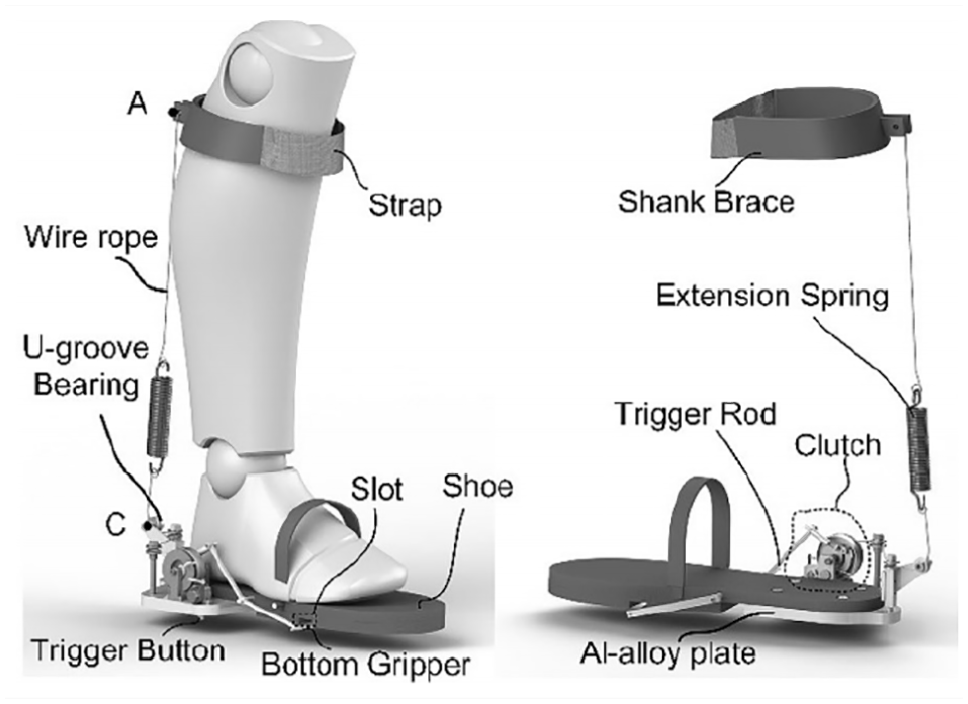
Lightweight passive ankle exercise device. 32
The ankle foot orthosis (AFO) proposed by Li et al. 35 allows users to change the stiffness of AFO to complete different lower limb activities. A quick release concept for AFO was presented and validated, the equipment has good strength. Kim et al. 36 designed a foot ankle orthosis, including a basic single degree of freedom exoskeleton and an artificial pneumatic actuator. The feed-forward control can reduce the muscle stiffness of soleus muscle, and the plantar flexion torque of the ankle joint can be reduced, which can provide ankle plantar flexion motion for the elderly.
Gait rehabilitation exoskeleton (GREs)
Gait rehabilitation exoskeleton robots (GRERs)
GRERs can assist patients to complete walking in a normal gait and provide power for them, which is suitable for patients with abnormal gait trajectory or joint trajectory. Shi et al. 37 designed a novel force field control for the three-dimensional gait adaptation. Trajectories of ankle center position in the 3D space measured by motion capture system were fitted to establish the Frenet frame. The force field controller was designed to guide the ankle center to move on a target trajectory in the 3D space. Simulation results showed that the designed system can effectively realize motion control in different modes. The actuator can improve the adaptive control ability of exoskeleton robots, so that robots can provide patients with an acceptable working state, which is more conducive to gait rehabilitation or standing posture improvement of users.38–41
The use of EEG signals for user intention recognition and robot state control can further increase the human-computer interaction function of GRERs. Wall et al. 42 designed HAL (Hybrid Assistive Limb) as shown in Figure 9, a Hybrid gait machine, and its control system can capture the intention of the user. The Autoencoder-based Transfer Learning (ATL) framework designed by Tan et al. 1 can use EEG signals to classify tasks, which can help the rehabilitation robot to understand the intention of the patient and help the patient to carry out rehabilitation exercise effectively. Sanguantrakul et al.43,44 have shown that if the use of EEG signals to assist patients to exercise with imagination can give play to the initiative of patients’ movement intention, then the working mode provided by rehabilitation robot may be the most suitable for users.

HAL. 42
EMG signal recognition is also effective. Xie et al. 45 established an surface Electromyography (sEMG) signal and interactive force (IF) fusion model based on the results of plantar pressure and flexion and extension recognition, which can identify the flexion and extension state of the lower limbs according to the EMG signal, and the trajectory of the robot can be planned online based on the sEMG-IF model to improve human-robot interaction and adaptability of lower limb rehabilitation robot. Chen et al. 46 Proposed the “Assist When Needed (AWN)” control strategy of gait rehabilitation robot, which provides flexible adaptive robot assistance function only when the user needs it. If this control strategy is combined with EEG or EMG signal recognition technology, it may be more flexible to provide patients with the required movement mode. The nonlinear control strategy can also achieve good gait tracking function.
Zhou et al. 47 proposed a triple-step nonlinear control strategy based on dynamic model. The results show that each joint of the human-robot system can follow the reference gait trajectory well under different interaction torque levels. Wu et al. 48 designed a LLERR with 3 DOF, as shown in Figure 10, which has an adjustable yet simple structure with hip, knee and ankle joints for different heights of patients. This research result is conducive to the realization of the personalized development of LLRERs.

LLERR with 3 DOF. 48
Shao et al. 49 introduced the conceptual design and size synthesis of the cam linkage mechanism for gait rehabilitation. The original movement mechanism is a two-degree-of-freedom seven-bar crank slider mechanism. A constant speed motor is sufficient to control the mechanism. The experimental results show that the generated trajectory is in good agreement with the expected trajectory.
Lowell et al. 50 designed a prototype of gait rehabilitation exoskeleton, as shown in Figure 11. It can be used to customize and verify the gait mode and modify the gait in the process of rehabilitation. It can be used to specify personalized gait mode in the future.

Gait rehabilitation exoskeleton. 50
Some promising structures/devices
Pneumatic artificial muscle is a promising development direction because soft robots offer advantages over rigid robots in adaptability, robustness to uncertainty, and human safety. 51 Gu et al. 52 proposed a soft wearable orthopedic device for gait assistance, with Pneumatic artificial muscle (PAM) the actuator, which reduces the weight of the equipment. The orthopedic device weighs only 680 g. Hashimoto et al. 53 developed a gait assist device composed of PAM and a common bracket, which is small in size, light in weight, and low in cost. The user has little discomfort in the process of using the device. This device has important commercial value.
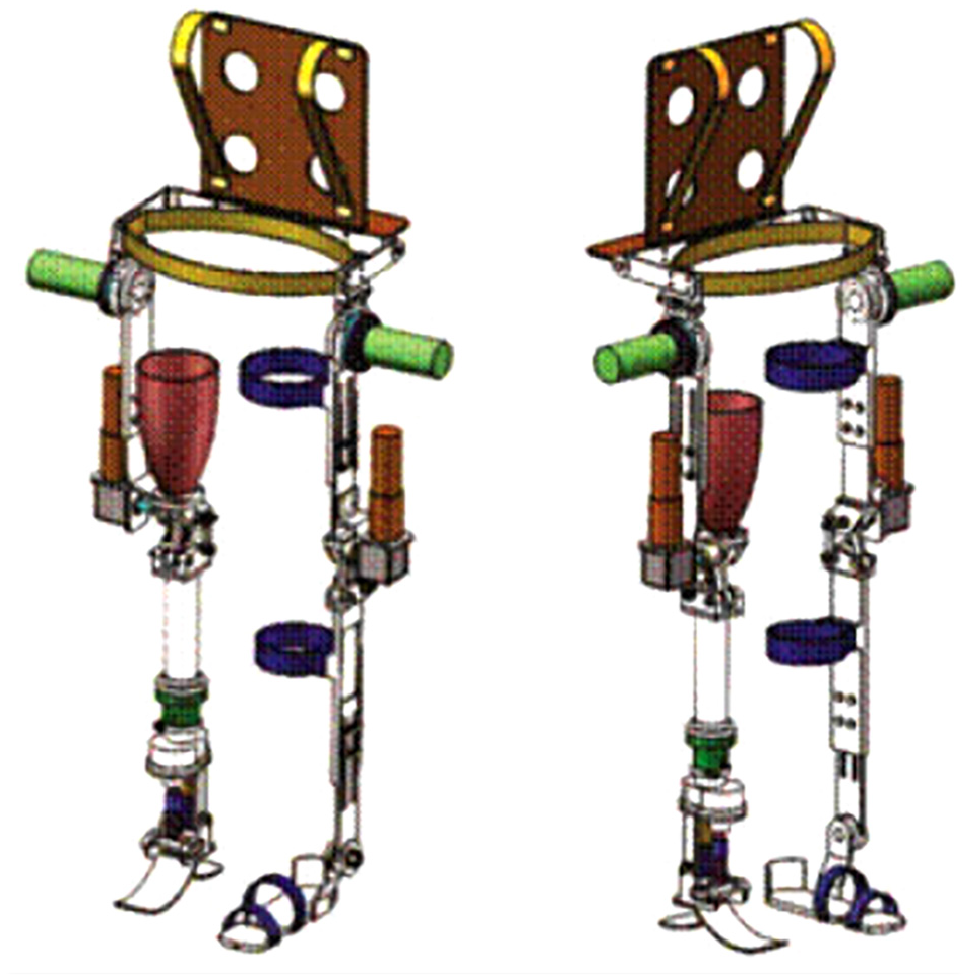
The lower limb training with sitting and lying posture can reduce the weight burden of the user’s buttocks and legs, and increase the range of motion of the lower limb joints. 54 Cheng et al. 55 have designed a sitting and lying exoskeleton robot for lower limb rehabilitation, as shown in Figure 12, which can be used to improve the stability of patient rehabilitation training. The sitting and lying rehabilitation robot designed by Chen et al., 56 as shown in Figure 13, can realize adaptive and compliant control of reference trajectory. The robot can better protect patients and provide effective rehabilitation training for patients.

Prototype of the robot. 55

Mechanical structure of rehabilitation exoskeleton. 56 (1-Man-machine interactive display device; 2-Telescopic mechanical leg structure; 3-Patients; 4-Seat structure with adjustable backrest; 5-Mobile platform structure.).
Cable driven is a new direction. Veneman et al. 57 designed LOPES, a newly developed gait rehabilitation device, which can realize two-way man-machine interaction. There are two modes, “patient in charge” and “robot in charge,” which control the robot to follow or guide the user respectively. Wang et al. 58 designed a modular cable driven lower limb rehabilitation robot prototype, as shown in Figure 14, which can complete the rehabilitation training task of human lower limbs with high stability, but subjects have not been recruited for real gait experiment.

Rehabilitation robot prototype. 58
Daily life assistive robot (DLAR)
Daily life assistive exoskeleton robots (DLAERs)
DLAERs can provide users with protection, support and assistance, reduce the burden of lower limbs, and assist patients to complete activities. It is suitable for stroke patients, patients with brain trauma, patients with movement disorders caused by spinal cord injury (SCI), and elderly people with muscle weakness and insufficient joint strength. DLAERs can provide power to lower limb 59 and can assist patients to climb stairs, squat, sit-to-stand, and walk.60,61 Wu et al. 62 designed a lower-limb-driven exoskeleton robot using linkage mechanism to help patients with SCI complete sit-to-stand, walk, and stand-to-sit by driving the hip and knee joints, as shown in Figure 15. Two participants with a complete SCI were recruited for this clinical study. The results indicated that with a lower level of exertion and walked faster and farther without any injury or fall incidence when using the powered exoskeleton than when using a knee–ankle–foot orthosis. Chen et al. 63 designed the exoskeleton CUHK-EXO, as shown in Figure 16, to provide users with assistive force/torque, the user is able to transfer his/her center of gravity (COG) left and right more easily during walking. The left hip joint has two DOFs including the hip flexion/extension and hip external rotation. The antiflexion bar is designed to be adjustable with three DOFs to better fit for different wearers.

Wearable exoskeleton Suit. 62

CUHK-EXO: (a) a patient with CUHK-EXO supported by a pair of smart crutches, (b) diagram of the overall mechanical structure, (c) waist structure, (d) thigh structure, (e) shank structure, and (f) foot structure.
The passive assisted walking device for the lower limbs proposed by Martin and Li 64 helps the user by negative work on the knee joint at the end of the swing, the device is capable of reducing metabolic energy expenditure equal to the amount of additional energy required to carry the weight of the device. Zheng et al. 65 designed a simple wearable walking assisted LLER which adopts unbundled lifting method, the mechanical structure is more flexible. The device can adjust the working state through the sensor to adapt to the user’s physical state. Zhou et al. 66 designed a gravity-assisted walking LLER with a compact layout, which improves the acceptance and safety for users when using the assistive device; this LLER could reduce the user’s hip and knee torque when walking at the same time helps to maintain balance at a lower walking speed.
Dong et al. 67 proposed an electric lower limb exoskeleton: “Human Universal Mobility Assistance (HUMA).” This device can be adapted to patients of different weights and can help patients walk at various speeds. Poliero et al. 68 designed a soft modular, energy-saving lower limb exoskeleton that integrates quasi-passive actuation into the soft exoskeleton to assist low to moderate intensity activities in daily life. For patients whose lower limb movement chain is damaged due to limb loss, prosthesis is needed to make up the missing lower limb parts and functions, promote physical activities, and make lower limb activities tend to be normal.69–71 Li et al. 72 designed an asymmetric exoskeleton, as shown in Figure 17, the left leg is an exoskeleton mechanical leg worn on the healthy leg of the amputees. The right leg is an assisted lower limb prosthesis composed of intelligent lower limb prosthesis and exoskeleton mechanical leg, which is connected to the stump of the disabled thigh through the prosthetic receiving cavity. The assistive lower limb prosthesis can be used as an intelligent prosthesis alone. The length of the thigh and shank of the device can be adjusted to adapt to different people.
Asymmetric exoskeleton. 72
Technology to improve the safety of DLARs
For organisms and robots, the ability to perceive and respond to disturbances and changes in the environment is essential. 73 The DLARs should have the ability to recognize obstacles to improve safety. Some scholars have proved the practicality of some obstacle detectors.74,75 Obstacle detectors can detect terrain and make adjustments to working conditions to replace the user in making some action decisions. Researchers should improve the accuracy of detection technology, so as not to let the wrong decision cause harm to users.
Some advanced learning algorithms and control algorithms are also could improve the human-machine coordination ability. For example, Gaussian process learning algorithm can improve the accuracy of joint torque prediction, 76 active disturbance rejection control (ADRC) can improve the anti-interference and tracking performance. 77 Nonlinear model predictive controller (NMPC) can improve the robustness and stability of the system. 78 Kalinowska et al. 79 proposed an algorithm, it can identify contact events without touching the sensor, which is particularly useful when providing real-time assistance during walking. The sensor 80 can collect the lower limb state signal, improve the robot’s prediction and recognition ability, so as to predict gait events.
Other medical methods for lower limb rehabilitation
The researchers have conducted studies and shown that the combination of multiple rehabilitation medical methods can play a better effect, such as the functional electrical stimulation (FES) or acupuncture therapy.
Functional electrical stimulation (FES) could stimulate muscles to produce joint movement, or to stimulate the lower limbs in motion to cooperate with exoskeleton.81,82 The overall physical condition of patients with FES assisted training has been significantly improved: Hwan et al. 83 combined robot assisted exercise with FES, the system can be operated in three different modes allowing both passive and active exercises, it can better protect the user from secondary injury. Ama et al. 84 designed a dynamic hybrid exoskeleton called Kinesis that can effectively balance muscular and robotic actuation during walking. Li and Yin 85 realized the time control of electrical stimulation, which can adjust the working mode according to the muscle fatigue state. Hmed et al. 86 designed a real-time FES system used model-free control (MFC) strategy to calculate the pulse width in the stimulation mode.
FES has some shortcomings. Users need high-intensity stimulation, sometimes even beyond the necessary stimulation intensity, to try to stand up. 87 FES supported standing requires the user to have sufficient muscle strength, which is achieved through muscle training.88,89
The acupuncture and moxibustion therapy is beneficial to correct the posture, muscle shape and gait of the lower limbs,90,91 restore the lower limb movement function of patients. 92
In the future, a acupuncture module could be set on the corresponding acupoint according to the position of the human body. The aforementioned joint rehabilitation robot, gait/lower limb function rehabilitation robot, daily life assistive robot could all be combined with acupuncture and FES, this will achieve better training results.
Discussion and conclusion
The details of the rehabilitation robot mentioned in this paper are shown in Table 1.
Details of each rehabilitation robot.

After statistics and analysis, it can be seen from the full text that the existing research still has problems that need improvement in the following aspects:
Therefore, future research can be improved in the following aspects:
Footnotes
Handling Editor: James Baldwin
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Key Project of Tianjin Natural Science Foundation (19JCZDJC33200), Tianjin Natural Science Foundation (18JCQNJC75300).