
Abstract
This article is about an architectural hardware-software model creation—home-based smart health model—to boost healthcare to a higher position within society. As an emerging field, smart health modeling is still insufficient. Current smart health services are hospital centered, data are scattered and application dependent, and health service provision presents attention delays. Analyses of Internet of things, Internet of medical things, and smart health applications potentials are the bases for the proposed home-based smart health model. The model aims to facilitate the smart health development and strengthening. To evaluate whether the model does what it must do, first, check lists on how the model complies with current and future devices and applications, smart health impacts and smart health potentialities, and second, a case study analyses the model conformity through an Internet of things sophisticated cloud app.
Keywords
Introduction
The initial information and communication technology (ICT) adoption in the healthcare sector main contribution was cost reduction and efficiency. The mobile devices arrival with positioning capabilities set up m-health, which added leverages to e-health, such as global availability, immediacy, and monitoring. Another evolving concept is smart health (s-health), which is based on both smart city and Internet of things (IoT) use. “Smarter cities make their systems instrumented, interconnected and intelligent.” 1 IoT allows connecting identifiers, sensors, devices, and computers through wired and wireless networks.2,3
The emerging s-health are isolated intelligent customized health services, usually with sensor data gathering and cloud processing. Emerging s-health examples include person-to-person audio or video home patient’s guidance through smartphones 4 ; IoT early warning systems 5 ; Ambient Assisted Living (AAL) technology that provides real-time life parameters, for example, heart rate, and information on environmental conditions 6 ; cloud-based electronic health sensor parameters registration and classification techniques 7 ; automated sensor smart gloves technology for disabled and special needs people 8 ; IoT smart watches and eyeglasses 9 ; and intelligent medical implants such as cochlea 10 and cardiac 11 or brain 12 pacemakers. Emerging s-health IoT apps may be grouped into telemedicine, emergency, medication, pharmaceutical packs, and others. Figure 1 shows the emerging s-health model early architecture.
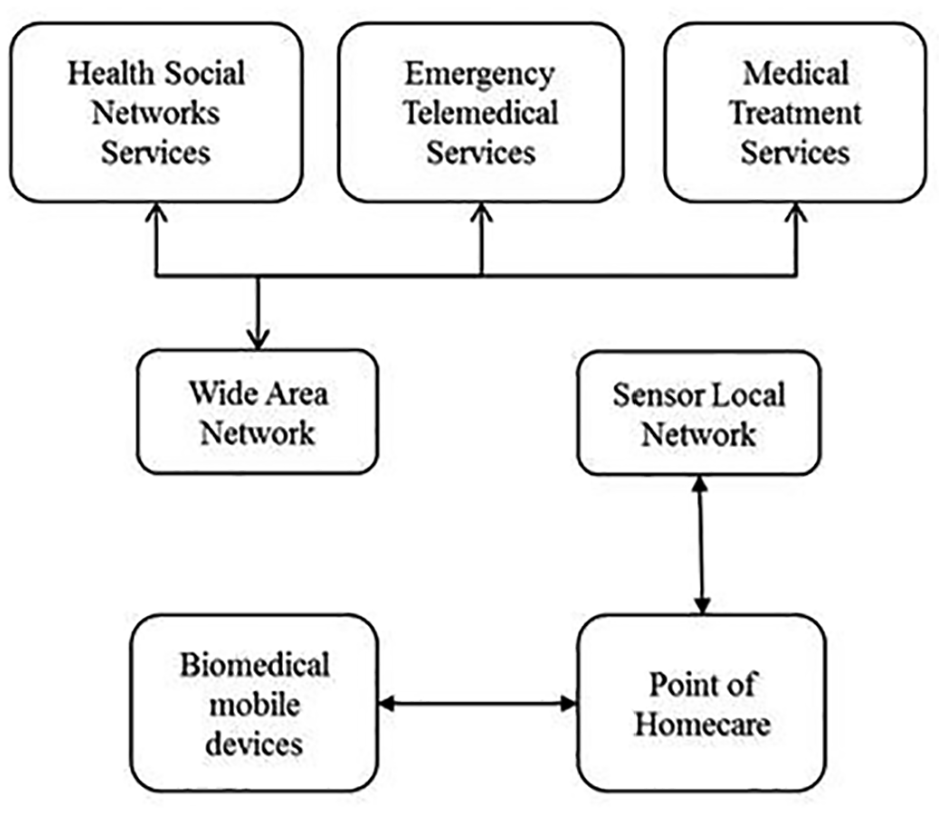
Emerging s-health.
The emerging s-health model in Figure 1 is a solution that offers a contextual perspective for medical care monitoring needs from both varied ages population and increasing online health services. The new model should support provision for home medical services that were previously available in hospitals. These services would be based on gathering and processing patient-related data from portable sensors. Raw data would not enough provide e-health services, because it may lead to risky misinterpretations. Monitored patient data will have better interpretation if evaluation includes data from daily life activities (DLA). Data need consistency validation and enrichment with metadata to enable a better understanding.
The emerging s-health model is understandably insufficient in terms of health care coverage and ICT architecture. It is hospital centered, and Koop et al. 13 predict that it will be home based by 2030. Data are application dependent and, therefore, not integrated. The health services, in many countries, also have other problems, such as delays in some services provision. 14
In addition, the model should aim for an IoT-assisted cloud-based health monitoring system, using different physiological and environmental signals to provide DLA contextual information. The proposed infrastructure at the same time could include health care providers to monitor older or lonely people health status and behavioral changes, as well as monitoring rehabilitation and recovery processes. No doubt that the wireless sensor network (WSN), an on-premises gateway for locally and quickly stored data in the healthcare record, and a cloud network architecture, for data processing and storage, will ensure an architecture and robust infrastructure to the proposed model. Thus, care support staff could have immediate access to data, and this would allow them to automatically validate observed anomalies. The proposed infrastructure implementation poses several challenges, in terms of remote environment monitoring, communication technology, intelligent processing systems, and service provision, among others. With the personal sensor network, it will be possible to capture sensor data based on the amount of data, its rate, mobility, latency, communication, and transmission.
The present day deficiencies converge into major challenges. Research questions needing answers include How is, and will be, IoT technologies use in the healthcare sector? What are IoT architectures within health services? How to build a solid home-based s-health model?
Technically, there is a need for an architectural model that speeds up, facilitates, and integrates emerging and newer s-health applications. The model also ought to be home based integrating patient with health care staff activities, home community, and hospitals. Small and large data need layer organization. Impacts may be on less intensive labor, lower operational costs, higher frequency use by chronic disease patients, and lower frequency use by acute illness patients.
To respond the questions and its derivatives, the article aims to build a model that contributes to the understanding of how s-health can be applied in a home environment and what fundamental infrastructures are needed to support s-health. Following this introduction, the article analyses the literature in terms of IoT and the healthcare sector, Industry 4.0, IoT technologies and s-health, and IoT architectures. Next, the article examines s-health potential through home intelligent service, smart treatment, and telemedicine. Then, the article develops the three layers home-based s-health model, which has the patient at home as its center. The second layer is the hospital, and the third is the ecosystem. The model proposes infrastructure and systems for the integration of and collaboration between the three layers. The article ends with two method validation sections: a comparison between before and after the model, and a case study.
Related work
This section focusses on what the literature says about the challenges to build a solid home-based s-health model; that is, Internet use in the healthcare sector, Industry 4.0 challenges, IoT technologies in s-health, and IoT architectures for s-health.
IoT and the healthcare sector
Healthcare sector uses of emerging IoT have the potential for reaching most people. The major impact is on health monitoring, especially in cases with silent symptoms. An early diagnosis may activate prevention procedures to avoid illnesses and even death. IoT and digital technologies advances were fundamental for developments in data storage, processing, and analyses. 15 Benefits cover wide spectrum of economic sectors, that is, business, communications, energy, education, health, people, sustainability, transport, water. 16 Currently, the main e-health apps concentrate on disease treatment monitoring and medical management. 17 In brief, larger IoT integration seems desirable, particularly because the global health system is clearly moving toward health care at home. 18 Figure 2 shows some IoT healthcare applications.

IoT apps in healthcare.
Figure 2 presents some health IoT applications. There is a scattered node set across several communicated areas. Each node may work in collaboration with other components such as telemedicine, researcher, nurse, physician, ambulance, among others. There may be a wide variety of applications for hospitals patient control through monitoring and control systems. Different networks, such as wireless local area network (WLAN), wireless personal area network (WPAN), wireless body area network (WBAN), radio-frequency identification (RFID), assist in automated identification, and electronic device data capturing.
Industry 4.0
Zhu et al. 19 and Nicolescu et al. 20 argue that Industry 4.0 will significantly impact s-health scenarios such as great growth in connected devices (up to 100 billion by 2030). Gubbia et al. 21 state that Industry 4.0 impacts will create value for businesses and consumers in multiple application areas: transport, urban planning, home automation, education, commerce, logistics, agriculture, industry and, notably, health. Dimitrov 22 reports that by 2020, 20% of the IoT market will be on Internet of medical things (IoMT) and that another 20% will be directly or indirectly related to health, well-being, and AAL. Thus, the health sector would have 40% of the market.
Industry 4.0 assumes IoT adopting and integrating products, processes, places, and people. 23 Industry 4.0 imposes challenges to the home-based s-health model. Imagine a modernly designed “Hospital at Hand,”24,25 which communicates all relevant data about objects and people. This would always allow people and situations identification, and have knowledge about teams and their work status, the medical actions, care, real-time updated medical history, the processes and their result, and so on. In short, to know all data and make decisions to achieve both citizens’ health and good management.
IoT technologies and s-health
Easiness to connect nodes is an IoT major attribute, which, in turn, is a challenge for new communication protocol developments and topology updating. WSNs comply with many needed requisites by Internet technology solutions.26,27 WSN is a set of scattered nodes interrelated through an ad hoc communication, which allows node collaboration. 28
Wireless technologies for biomedical sensor systems include, among many others, WPAN29,30; WBAN,31,32 also known as body area network (BAN) 33 ; medical body area network (MBAN) 16 ; WLAN34,35; WiFi 36 ; and Worldwide Interoperability for Microwave Access (WiMAX). 37 The IEEE 802.15.4 standard-based low-power digital radio signals for personal area networks (ZigBee)34,38; short distance wireless technology (Bluetooth) 36 ; wireless networking protocol (Adaptive Network Topology (ANT)) 39 ; ultrawideband (UWB) 40 ; e-textiles 41 ; endoscopic capsules; implantable and ingestible sensors; epidermal electronics; smart bands; smartphones apps 42 ; RFID used for object automatic identification and location 43 ; real-time location system (RTLS) 44 ; indoor positioning system (IPS) 45 ; and web conferences and webinars.
In addition to their cloud computing use, RFID and ZigBee technologies, through connecting smart devices to the Internet, reduce working time and costs.46,47 Their wide variety applications make them attractive for developing healthcare settings, for example, patient monitoring and control systems, medical decision-making and administrative systems, and customer relationship management (CRM) systems. All these have qualitative impacts on improving health care services precision and quality as well as patient’s satisfaction. 17
IoT implementation architectures in s-health
IoT makes extensive use of wireless technologies. Figure 3 shows Berhanu’s BAN architecture that serves as a test bench for applications. 48 WSN is a low-power sensor network assembled into the patient body, for monitoring and controlling vital parameters and movements. In turn, sensor network is connected to a wide area network (WAN) to transmit data to a base station. These data then travel in real time to the hospital applications.

Body area network architecture.
Figure 3 presents a wireless IoT technology–based architecture as a test bench for body area networks (wireless sensor and actuator network (WSAN)). These networks use low-power devices (sensors) built into the body, which are connected to a wireless network to transmit data to a base station, and then to the hospital. The Internet Protocol (IP) addresses allow that most everyday objects be accessed and materialize IoT ubiquity. IP Version 6 (IPv6) over low-power personal area network (6LoWPAN) is a protocol that provides support for sensor networks. 49 Catapang et al. 50 present an architecture that integrates hardware and software, based on heterogeneous networks 6LoWPAN. It allows, for example, health monitoring applications through integrating a BAN and an environmental control network. Internet connectivity added the use of an edge router and allows access to a single node directly from anywhere on the Internet.
In addition, WSN-based intelligent systems consist mainly of two parts, as shown in Figure 3, where events are detected by the sensor nodes and converted into digital data. Data go through intermediate nodes using WBAN and Relay nodes. Finally, the nodes send received data to the Internet server, either in a single packet or in parts.
IoT has a four-layered architecture, as shown in Figure 4. From bottom to top, the first is the detection layer that fits the hardware different types linking the real world and data collecting. The wire and wireless networks are the second layer that provide data transfer. The service is the third layer that manages all kinds of user requirement satisfaction services. The interface is the top layer that provides user applications interactive methods, data processing and results displaying.
IoT architecture.
The technology and healthcare interaction have a long history. The rapid IoT growth and the miniature biosensors adoption have created new opportunities for personalized e-Health. The four layers in Figure 4 would work as follows: intelligent health services collect different data types at the detection layer through sensors in cyber physical or portable systems. Data are transported to the cloud or to storage servers over wireless networks at the network layer. The service layer provides the actual health care service, such as patient data processing on heartbeat, blood pressure, and glucose level, among others. The interface layer provides an easier interface that allows users to retrieve the results and understand the results; thus, physicians may diagnose or arrange an appointment. Therefore, patients quickly understand their health status, saving time, money, and medical checkups.
s-Health potential
There are abundant s-health potentials. The following examples describe some of them: intelligent emergency services (ES), medical assistance in smart homes, smart treatment services, smart mobile biomedical devices, health-centered social networking service, and telemedicine service. 51
Intelligent ES
ES also entered the evolution toward the patient-centered home medical service paradigm. The ES is very important since lives depend on both good and timely management. There are wireless IoT–based technology solutions that support pre-hospital service and ES good and timely management. Beltrame 52 reports a communication improvement between the dispatch control center, the ambulance, and the hospital emergency room. Ambulances equipped with remote technology may better handle emergency situations. This facility is extendable to home monitoring and patients’ emergency needs. Fan et al. 53 illustrate an intelligent medication monitoring system based on IoT and an ontology-based automation design methodology. The ontology helps symptoms and available medical resources understanding. It generates, quickly and automatically, a rehabilitation strategy and reconfigures medical resources according to the patient’s specific needs.
Medically assisted smart homes
As the elderly has preference for home-based care, this is one of the fastest growing areas in the health sector. Figure 5 shows home-based care proposition. Its main objective is to better control the patient medical care, reduce hospital visits, and improve life quality. 54
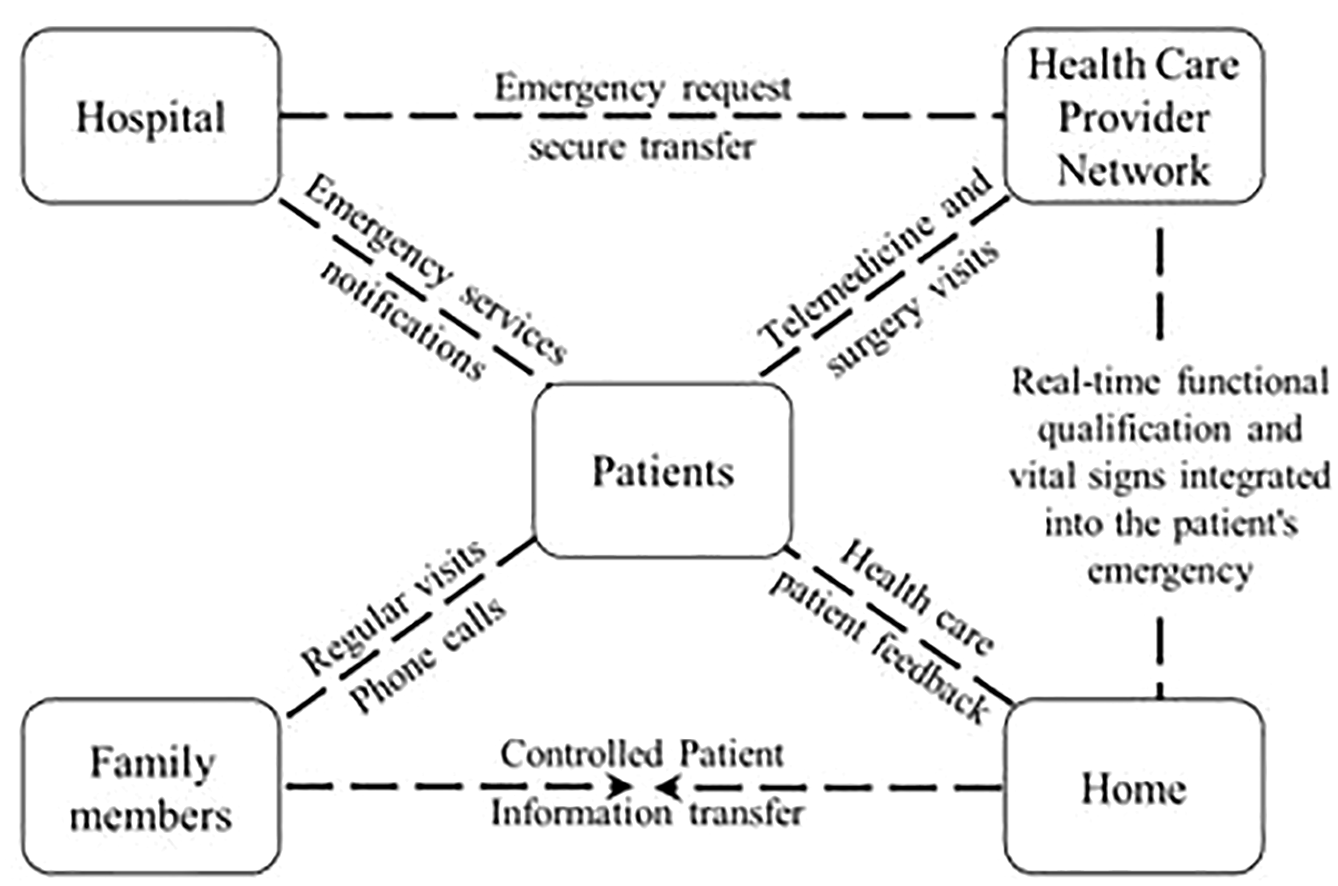
Home-based care.
Figure 5 shows several developed, implemented, and evaluated applications to assist patients care at home. They aim to have better control in the patient’s medical care as well as provide information to families.
Yu et al. 55 propose an information system based on IoT (EBPlatform) and designed for non-contagious disease patients’ home care in China. It uses an eBox sensor, which is implemented in the patient’s home, allows blood pressure and sugar regular control as well as electrocardiogram (ECG) signals. A web portal displays the measurements data, and physicians provide online treatment. EBPlatform testing was through 50 Beijing patients case study. Results showed that the platform allows physician–patient regular communication, increases physician’s efficiency, and achieves greater treatment monitoring and control.
Smart treatment services
Any disease treatment success depends on medication taking time complies with the prescription. Zhibo et al. 56 state that patient-associated factors may lead to miss medications taking. These factors may be psychological and associated to anxiety, motivation to recover from illness and, for the elderly case, forgetting the schedule.
During a routine consultation, it is difficult for the physician to find out if their patients are taking medication properly, unless patients mention it. This may seriously affect the patient recovery process. Therefore, there emerged systems to monitor patient’s medication at home. Zhibo et al. 56 developed iHomeHealth-IoT as a smart medication box and smart pharmaceutical package with RFID communication capabilities. The smart box advises the patient the medication time. The box also alerts the physician through a text message.
Smart mobile biomedical devices
Cerutti et al. 57 state that smart wearable device (SWD)-personalized health service research and development results motivate government’s investment and research. Agencies around the world, for example, Europe, USA, and Asia do similarly. A good example is the USA Oregon Center for Aging and Technology that focuses on sensor technology development into older adults home monitoring. Another example is the Hong Kong Innovation and Technology Fund that supports research aimed at developing SWD to monitor cardiovascular functions.
Lei et al. 58 propose a community medical network (CMN) architecture based on 3G, global system for mobile communications (GSM), Internet infrastructure, and wireless body area sensor network (WBASN). Lei’s proposed architecture has five main parts: WBASN, mobile devices, mobile communication networks, backbone, and local hospitals servers. WBASN is responsible for both patients’ health status the monitoring and medical information obtaining. CMN implementation is not costly and reduces diseases’ diagnosis and treatment costs.
Cavalleri and Reni 59 propose an active monitoring insole (AMI) device for lower extremities load control. Physicians and therapists use AMI for patients’ progress analyses and may take recovery corrective measures. Bianchi et al. 60 propose a Multi Sensor Assistant (MuSA), which is a mobile multisensory device that detects heart and breathing rates.
Health-centered social networking service
The World Wide Web enabled numerous society advances, for example, facilitating access to both knowledge and business doing. The Web 2.0 enabled the social networks trend, such as Facebook, Twitter, YouTube; these provide content apps, blogs, and wikis. Hwang et al. 61 describe a weight loss app through an Internet social network. The site provides anonymous and personalized support, and people share their motivations and experiences. The site improves its services via surveys.
Patrick et al. 62 study weight loss control in 18- to 29-year-old young adults. The purpose was eating habits guidance and weight control analyses. Results showed Facebook’s use strengths and limitations in health research. Sato and Costa-i-Font 63 present a statistical study on social networks used for trust and privacy medical research. The study uses European behavior and perceptions data on privacy and social media. The results showed evidence of an age digital gap, while in the health area, there is no evidence that income does not affect access to social networks. Auffermann et al. 64 claim that social networking services have changed the way society communicate and offer opportunities to improve radiology practices.
Lober and Flowers 65 reviewed consumer’s education and technology use activities. They found that social trends are visible in health area as ICT integration; in the search for Internet information; in innovative interactions with family, suppliers, and partners; and in e-patient apps. Vera et al. 66 report a social network that shares worldwide MS patients’ experiences and information as well as on medical research into its relationship with chronic cerebrospinal venous insufficiency (CCSVI). This article reviews Internet available for MS patients seeking information about CCSVI. It also explains the physicians’ responsibilities when participating in these online discussions. Hidy et al. 67 assess mental health social network development and uses. The site addresses ethical, legal dilemmas, and practice guidelines for mental health professionals interested in social network development.
Telemedicine service
Telemedicine is the medical practice through computers, communication networks, medical technology, and health staff providing patients with remote service. 68 Stowe and Harding 69 list services that include consultation, diagnosis, prescribing, health education, and general medical information. Thayananthan 17 argues that 3G-, 4G-, and 5G-based ICT, including IoT and communication protocols, are the main enablers to treat patients, covering the elderly, through e-health applications.
Lu and Liu 70 concluded that IoT based on RFID technologies had the sick room most suitable performance. Sudhamony et al. 71 report that cancer is one of the main public health problems in India, and that wireless technological oncological telemedicine allows offering remote expert medical guide, helping prevention, early detection, palliative care, and rehabilitation in hard-to-reach places. Chaudhari and Karule 72 show architecture types for telemedicine using proven, widely used, and low-cost technologies.
A telemedicine application highly used is the ECG. Sufi et al. 73 present a mobile cardiology system that sends, in real time, the electrocardiography signal through a smart telephone. Busra and Rahman 74 report a study in Bangladesh, where most people live in rural areas lacking specialized care. Telemedicine systems would allow physicians and hospitals to collectively provide health services to the rural population. The article details a multiple hospital telemedicine distributed information system that connects medical experts with rural area patients.
The home-based s-health model
The analyses included (a) how healthcare sector IoT technologies is, and will be, used, (b) Industry 4.0 implications for the health sector, and (c) health services IoT architectures. These cause constraints so that a home-based s-health model solid building must include information systems integration, artificial intelligence, big data analysis, real time, data processing, device communications, digitization, cloud computing, and the ecosystem. In brief, integrating emerging and potential s-health applications is the base for building up an architectural model to enable its embodiment.
Caragliu et al. 75 provide a smart cities definition as “cities solidly based on information and communication technologies, that invest in human and social capital, to improve citizens’ life quality, promoting economic growth, participatory governance, intelligent resource management, sustainability and efficient mobility, while guaranteeing citizens privacy and security.” Mobile devices use helps more efficient task performance. s-Health allows remote patient monitoring, communication between professionals with family members and patients and redefines health services in three main aspects: it provides access to unprecedented services and knowledge that are user oriented, and customizable.
The health sector, seen as layers, contains a variety of components, some of which project themselves over the smart city layer. As an illuminative way, Figure 6 shows five health application representative cases, covering a widest scope as follows:
Case 1: Classic health. A typical health activity is a physician visiting a patient at home using traditional tools (not necessarily involving ICT).
Case 2: e-Health. This involves using electronic health records databases to store patient medical information. This is classical health that uses ICT.
Case 3: m-health. It involves patients checking prescriptions from mobile phones to ensure medication adherence. This is e-health using mobile devices to access medical data.
Case 4: m-health enhanced with s-health. A cyclist, wearing a vital sign monitoring sensor wristband, has an accident. The body sensor network detects the fall and sends an alert to the city’s infrastructure. 76 The system responds analyzing traffic conditions and sends an ambulance through the best route. In addition, city traffic lights are dynamically adjusted to reduce the ambulance time to get to the cyclist.
Case 5: s-health. Patient gathering health-related information from an interactive information system about, for example, the pollen and dust contamination levels. Patient decision may include avoiding dangerous areas or getting antihistamine pills.
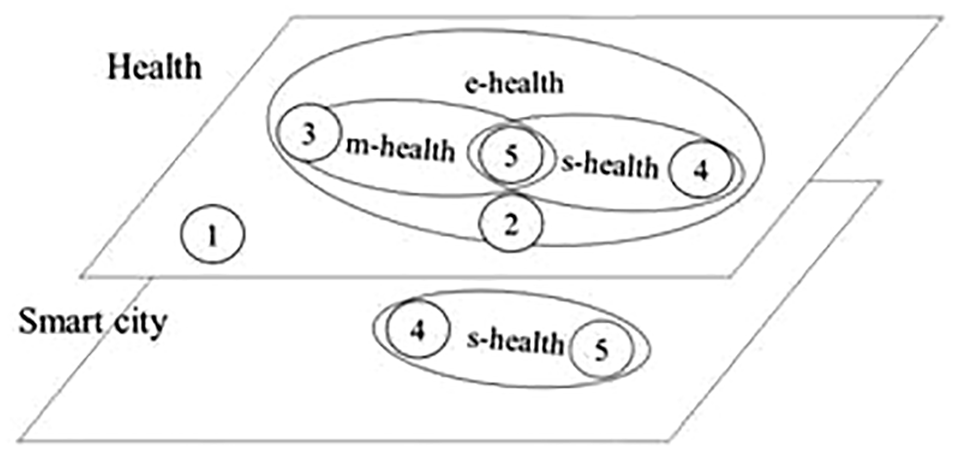
s-Health layers and components.
In general, the s-health aim is to promote health to a higher position within society. It revisits the m-health and smart cities principles in a distributed, private, safe, efficient, and sustainable way. 77
Figure 6 shows health plans and smart city diagrams. The relationship/projection/intersection between the two planes is represented as the s-health area, and the numbers refer to the examples given above. There are two planes: health and smart city. Although the planes seem independent, when the health is projected over the smart city there appears the intersection that represents the health services provision with the smart city infrastructure. Figure 6 makes it clear that s-health is a subset of electronic health, as health is based on the smart city ICT infrastructure.
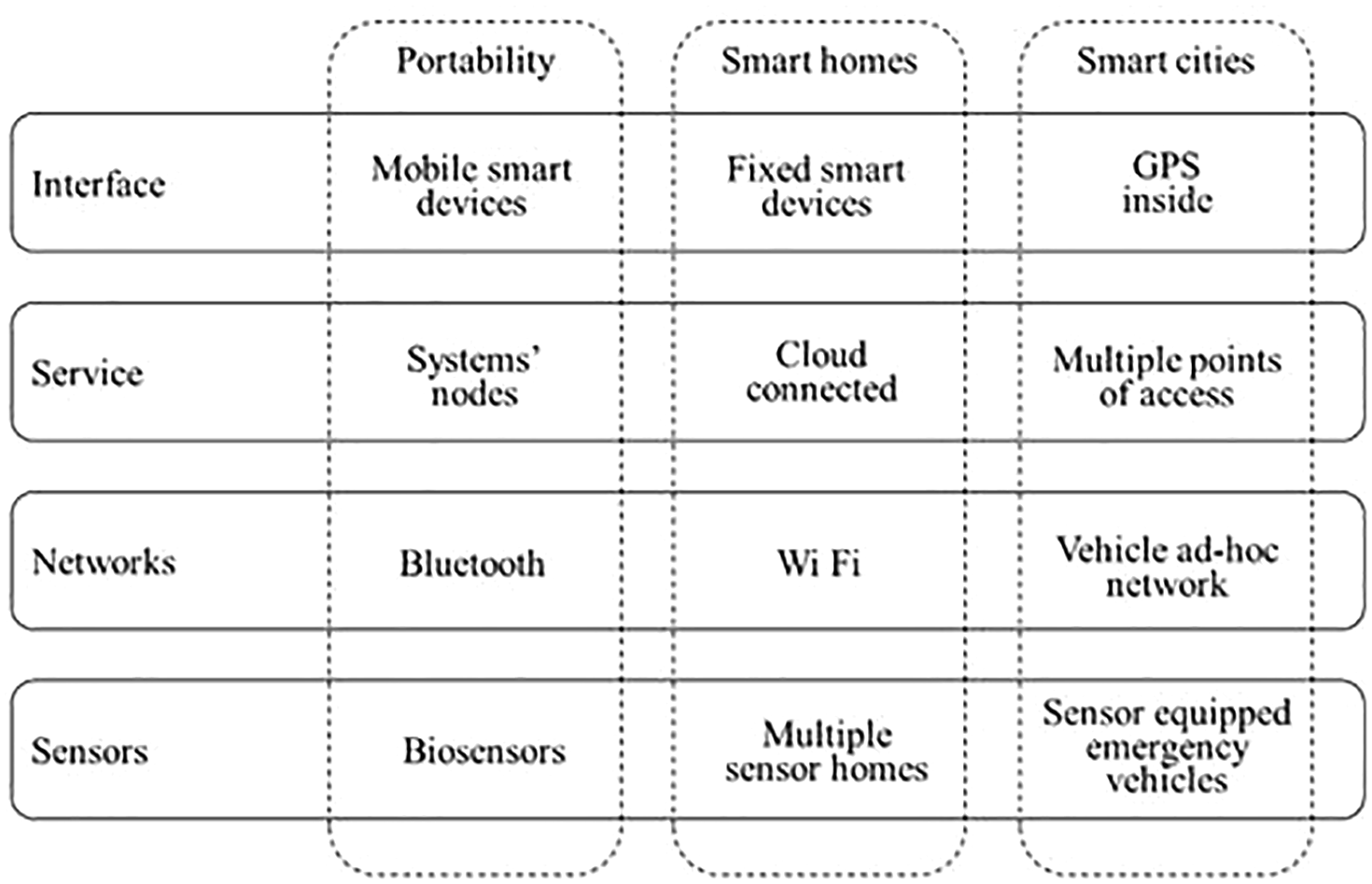
Figure 7 shows that the proposed s-health model has hardware, platform, and interfaces as components. Hardware includes devices, mainly sensors as magnetic raw information receivers; platform incorporates raw information storage, usually as databases for consultation and analysis, containing applications’ logic and providing device software management; front-end includes user interfaces, Internet integration and connectivity, and tools for integrating with other information systems.

s-Health and s-city infrastructure.
s-Health expands indoor monitoring environment’s capabilities. It enhances several research lines, such as patient continuous status assessment, early emergency detection, health condition change detection, abnormal situation detection, and fragile situations early detection. s-Health is the natural e-health expansion in the context of smart cities. The s-health adoption as part of smart cities presents two trends: developments in mobile health promote ICT advances and national and regional governments’ encouragement for smart city deployments. Smart cities infrastructure and technologies may combine with the s-health and telemedicine concepts to create the s-health as a more universal concept.
The detailed s-health model, its structure, components, and cutting-edge technology inclusion are in Figure 8.

s-Health model and cut-edge technology.
Figure 8 shows the patient monitoring process, with detection and communication capacity, where all objects (people, equipment, medications, and others) can be traced and monitored by different devices. Thus, it is possible to process health-related information, such as logistics, diagnostics, therapy, recovery, medication, management, finance, through relational database management systems, data mining with servers permanently connected. The processed data may be displayed by browser or mobile applications, with state-of-the-art interconnecting technology infrastructure.
Recapping, IoT enables smart devices receiving and sending data about home patients’ health. Hence, the model has the patient home at the central level. Hospital also has patients’ data that may be processed, managed, and integrated to patients’ home data. Thus, the hospital is the model next level. As the hospital relates to suppliers and other agents, the hospital ecosystem is the external level.
The home level includes an Information Home Health Station (IHHS), which integrates home devices data. It also has users, devices, apps, and interfaces. Users incorporate patients, nurses, physicians, paramedical, and clerks. Devices comprise, among others, smart wrist and ankle laces, wearable sensors, medical devices, medicine RFID. User interfaces may include touch screen, local sensors, and others. Device interfaces contain near-field communication (NFC), Universal Serial Bus (USB), Bluetooth, ZigBee, 6LoWPAN, effective isotropic sensitivity (EIS) interface, 5G, and others.
The hospital level has infrastructure, finances, human resources management, technology, procurement, inbound logistics, operations, outbound logistics, and marketing and sales. 78 Together to typical organization departments and systems, hospital infrastructure includes pharmacy, ES, laboratories, blood bank. Finances matters for budget planning and management; capital, risk, and tax management. Human resources have the usual staff selection, training, and promoting as well as rewarding and incentive. Technology includes equipment for back-end front-end services, running enterprise resoure planning (ERP), expert systems, EHR database, and home and hospital networks. It also must include intelligent information systems, and the management of both a collaborative health cloud networks (CHCNs) and an electronic healthcare record (EHCR) through a secured, standardized, distributed, integrated, and interoperable database. Procurement includes suppliers, stock management, among others. Inbound logistics focus on ambulatory and hospitalized admissions. Operations consist of clinical evaluation, diagnosis, laboratory and image tests, surgery, and treatment and follow up, pharmacy packs, recovery. Outbound logistics comprise discharge, transfer to other health facility. Marketing and sales have billing, casher, patient’s satisfaction surveys, and others.
The external level is the hospital ecosystem comprised by political, economic, social, technological, and ecological factors 79 as well as suppliers, buyers, entrants, and substitutes. 78 For the model purposes, major relevance comes from government and their healthcare and environmental delegated authorities. Other hospitals, direct and related suppliers are also relevant as well as the hospitals served population and specialized services such as telecommunications and medical.
The model value added rests on the technology enhancement through the inclusion of both the EHCR and the CHCN. These two proposals enable the relationships among all the model components. Figure 9 illustrates a model view. Table 1 illustrates how the underlying technologies work under the model.

s-Health model structure and components.
Technologies interacting through the model.

ECG: electrocardiogram; GPS: Global Positioning System; RFID: radio-frequency identification; IP: Internet Protocol.
One of the proposed model outstanding features is patient health management through integrating home s-health, intelligent ES, and hospital management into a distributed system. The proposed cloud infrastructure layer components constantly interact with each other as underlying support technologies, in fields of action, as in Table 1. Objects and technology platforms are usually connected to the Internet through local, extended, personal area networks, allowing the communication with each of the patient to manage patient health and provide prompt and efficient medical care. Another model feature is easier systems and smart homes apps access to key stakeholders, such as doctors, care takers, patients’ family and friends, and service providers.
Discussion
Sensors and computing in general are cheaper, faster, and lower power consuming than a few years ago. Therefore, collecting disperse data is also cheaper and big data processing takes shorter time. The home-based s-health model, as shown in Figure 9, handles the data complexity in terms of variety, volume, and speed. For example, simultaneously, electrocardiogram (ECG) data communicate in XML format and an IoT-based camera handling image formats detects skin diseases. Another example is cloud data flow and cloud computing management. Similarly, devices may have remote location, which facilitate simple and autonomous s-health systems set up. Well-designed patient-friendly interfaces may require minimal expert participation. Joyia et al. 95 identified 18 IoT applications and 11 IoT future challenges in the medical domain. All these are well supported by the home-based s-health model. Table 2 evaluates whether the model supports current and future applications and their devices.
Applications support before and after model.

The model covers city and homes through data collecting sensors, communicating antennas, big data intelligent algorithms, data processing application programming interface (API) to analyze user requests and interfaces to report to the user. Patients that use IoT medical services save time since they do not wait for appointments or test results.
The home-based s-health model depicts a three-level integrated health applications lifecycle, from requirement specification to deployment, with security and privacy. The CHCN provides security, while the EHCR guarantees privacy. Table 3 evaluates whether the model supports current and future s-health impacts.
Impacts support before and after model.

The CHCN is a holistic layering approach which connects front-end data capturing devices and transmits data through gateways and cloud nodes to back-end storage and processing equipment. The EHCR is the model storage kernel that manages a secured, standardized, integrated, interoperable, distributed database, which facilitates algorithmically, warehousing, and big data processing as well as data aggregation to reporting transfer to cloud connected devices. Table 4 evaluates whether the model supports future s-health potentialities.
Potential support before and after model.

Case study
The case study addresses how the home-based s-health model would work for telemedicine, in a non-intrusive manner, for a specific case: cloud-assisted smart glove. A smart glove may be useful to meet telemedicine requirements in Parkinson’s disease. 96 The smart glove has a sown flexible sensor on the pointing and thumb fingers to detect motor symptoms, such as tremors, stiffness, or slow movement, as the one shown in Figure 10.

Smart glove.
The smart glove uses Arduino 101, which houses any brand of existing processors on the market, in this case, it is used an Intel Curie chip to communicate the computer equipment and low energy Bluetooth with the local network. The Curie Chip reads voltages from the flexible sensors, allowing to perform the unified Parkinson’s test through finger tapping. 97 The task of finger tapping is chosen because of its clinical value and the easiness for the patients to perform it at home. The data collection and signal processing tasks require patients to touch 10 times their fingers. Here, there is a peak detection algorithm to measure the tapping intensity. Data are stored on the EHCR, described in the model as secured, standardized, distributed, integrated interoperable database. Further data processing may be performed, for example, detecting if the signal amplitude is greater than a predefined value; depending on signal values, sending messages or warnings to patient’s relatives, nurses, or physicians through the CHCN, described in the model as the mix of WiFi, WSN, WPAN, WBAN, MBAN, WLAN, wide network port (WNP), signal battery (SB), remote file inclusion (RFI), next generation (XG).
The model will also support more sophisticated smart gloves applications, such as their integration to IoT and the cloud. Figure 11 shows a cloud-linked computing environment for low-power integrated processors.98,99 It includes an Intel Edison and Raspberry Pi, which acts as a built-in cloud computer to run an i386 Debian/Jessie distribution running Octave 3.8.2-4 for data processing.

Cloud-linked computing environment for low-power processors.
The smart glove collects data and stores them in a text file and sends it to the EHCR through the CHCN. The integrated cloud network using Edison or Raspberry Pi acts as a gateway to the cloud, that is, it is the collaborative cloud network layer that processes the data with its respective interfaces for the different used devices, which contain NFC, USB, Bluetooth, ZigBee, 6LoWPAN, EIS interface, 5G, and others. Hence, the model has the patient at home at its central level and, if necessary, the hospital also has the patients’ data for further processes, managed and integrated with glove user patients’ home data.
This case study uses the cloud health collaborative network layer to work with a central processing system that would consist of 500-MHz dual-core, threaded Intel Atom CPU, and a 32-bit Intel Quark microcontroller at 100 MHz, along with Bluetooth 4.0 and IEEE 802.11a/b/g/n dual-band connectivity interfaces via an integrated chip antenna. The process would then be benchmarked for time, CPU load, and memory load measurements. The results would be generated in the electronic health log by combining the information collected from the Octave function profile and the top of the Linux program. The profile function running within Octave would collect algorithm timing details, while the top program is able to collect CPU timing and memory loads for the entire process.
The model easily supports the above configuration and processes. The proposed infrastructure would work by placing the cloud node (in this case, it would be Edison and Raspberry Pi) between the smart glove and the cloud. The model allows that entrance and service processes be distributed. The cloud node may be placed in locations with only a small number of devices, such as an elderly home. Each cloud node is used to collect data from smart gloves, processes the received data, and then publishes the processed data to a cloud server, all within the model’s three layers (infrastructure’s environment). The model incorporates a wide range of typical users: patients and their family, nurses, physicians, paramedics, employees, providers, stakeholders, among many others.
Conclusion
ICT widespread adoption led smart cities emergence. ICT, IoT, and mobile technologies use in healthcare accelerates patients’ medication and general medical care monitoring. Networks, ultra-wide band, ingestible sensors and epidermal electronics, smart bands, and smartphone applications are predominant in current and future s-health implementations.
IoMT together to technology advances, such as the proposed EHCR, and architecture IoT-based networks, and the proposed CHCN, provide favorable scenarios for large, fast, widespread maximum IoT technology use to advance integrated home-based healthcare solution developments. The article aimed to build a smart city’s ICT infrastructure for home-based s-health. The purpose was a contribution toward the understanding of what and how are needed to support the integration the scattered emerging and forthcoming s-health applications.
The model value added rests on the technology enhancement through the inclusion of both the EHCR and the CHCN. These two facilitate integrate and accelerate, the emerging and forthcoming s-health applications. If adopted, the model will, for example, allow smart ambulances carrying out on diagnoses the way; thus, hospital personnel be prepared for the patient arrival. Other examples are multi-institutional data access, tele surgery, and so on.
Finally, it is thrilling to realize what the model may achieve, if adopted. It makes a significant contribution to facilitate integrate and accelerate, the emerging and forthcoming s-health applications.
Footnotes
Handling Editor: James Baldwin
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for our research came partially from Vicerrectoría de Investigación, Desarrollo e Innovacion of the Universidad de Santiago de Chile.