
Abstract
The purpose of this study was to derive the local vibration that the sensorimotor area responds sensitively and to investigate changes in muscle activity of the lower limb when the vibratory stimulus was applied during the stair climbing. The electroencephalogram was measured when vibratory stimulus was applied to each tendon and changes in Mu rhythm activity were analyzed. A specific vibration frequency was selected through the results of the Mu rhythm analysis, and the specific vibratory conditions were set by combining the tendon site, vibration intensity, and frequencies. These vibratory conditions were applied simultaneously with the electromyogram measurement during the stair climbing. As a result, we confirm the specific vibration frequencies in each tendon. Also, we infer that there is a sensitive vibratory stimulus for each tendon. Moreover, the specific vibratory stimulus activates the sensorimotor area and elicits an increase in the muscle activity. This result means that specific vibration frequency and stimulation site should be considered in rehabilitation therapy that used the local vibratory stimulus. Also, local vibratory stimulus can be used to assist in stair climbing.
Introduction
Stair climbing is one of the basic behaviors in everyday life. Stair climbing is also a very difficult behavior in terms of musculoskeletal system because it requires more physical function in muscle coordination, movement, and loading conditions compared with walking.1–4 For these reasons, it can be a problem that can adversely affect the daily life of people with weak musculoskeletal system and physical functions. Therefore, there is a need for a method that can functionally assist movement of the weakened person.
There are several studies that have confirmed the effectiveness of vibratory stimulation applied to the human body. There are previous studies to improve the musculoskeletal capacity such as muscle activity, strength, and flexibility through vibration,5–7 and other studies have shown that vibration training positively affects mobility and postural and balance control.8,9 In addition, a clinical study has shown that the vibration applied to the sole of the foot of patient after stroke has a positive effect on balance improvement, 10 and another study has shown that patellar tendon vibration can reduce pathological extensor synergy after stroke. 11 However, it is difficult to compare the effects of vibration on the human body through the results of previous studies, because the vibration characteristics (such as the type, frequency, and intensity) used in each study are different. Therefore, a quantitative standard for the effect of vibration stimulus is needed, and it can be found through the change of Mu rhythm activity according to vibratory stimulus.
The Mu rhythm is an electroencephalogram (EEG) signal with a frequency band of 8–13 Hz and appears at maximally over in the sensorimotor area when in relaxed state. Mu rhythm has a characteristic that is attenuated by tactile stimulus, exercise execution or observation, and motor imagery, and this characteristic is used as an excitability index of sensorimotor area. 12 The vibratory stimulus causes excitation of Ia afferents, and this signal will reach the somatosensory and motor areas along the proprioceptive pathway 13 and will cause a change in Mu rhythm activity. Also, the vibratory stimulus causes excitement of afferents and recruits more receptors, which, in turn, activate a larger fraction of α-motoneurons whose muscle fibers contract. 14 In addition, it is confirmed that there is a linear inverse relationship between electromyogram and alpha band (Mu rhythm) during isometric contraction. 15 Therefore, we supposed that a vibration stimulus based on the Mu rhythm may help to understand the electromyogram (EMG) changes by the vibration and may be used as one of the methods to make the standard for the vibration application.
The aim of present study is (1) to investigate specific vibration frequency that can activate the sensorimotor area through the variation of Mu rhythm activity according to the frequency of the local vibratory stimuli applied to the tendon, and (2) to identify changes in muscle activity when vibratory stimulus of the specific frequency is applied to during stair climbing.
Method
Subject
In total, 12 healthy adults (age 24.8 ± 1.86 years, height 174.5 ± 3.61 cm, and weight 69.5 ± 6.04 kg) participated voluntarily. All subjects can perform stair climbing without the help of others and do not experience surgery, illness, or injury of the lower limb. One day before each experiment, to control factors that could affect EEG, EMG, and vibration perception threshold measurements, we asked the subject to take enough sleep and without excessive exercise, alcohol, and caffeine intake. The research was approved by the Institutional Review Board (IRB) of Chonbuk National University (IRB File No. JBNU 2017-03-011-001).
Vibratory intensity and stimulation site
Vibration perception threshold of each subject was measured for use as the vibratory intensity. The vibration was applied to the Achilles tendon (ACT), that is the tendon of triceps muscle of calf, and applied to the quadriceps tendon (QT), that is the tendon of quadriceps femoris muscle, and 14 frequencies ranging from 100 to 300 Hz to which the somatosensory receptors were respond sensitively 16 were selected. The vibration perception threshold of each frequency was measured three times. To prevent sensory adaptation, we gave 2 min between frequency conditions and 5 min between stimulation sites. Threshold is defined as the mean value of vibration perception threshold (100%) measured three times, and sub-threshold is defined as a value corresponding to 80% of the threshold. Linear actuators (DMJBRN0934AA; SAMSUNG ELECTRO-MECHANICS Co., Ltd, Korea) and function generators (AFG-21 25; Good Will Instrument Co., Ltd.) were used for vibration applications.
EEG measurement
The EEG was measured to derive the Mu rhythm. We used a disk electrode and placed electrodes at nine sites according to international 10–20 system (FC3, FCz, FC4, C3, Cz, C4, CP3, CPz, and CP4). The reference electrode was placed on both earlobes. EEG was measured during 60 s per frequency, and the vibration was applied simultaneously with the measurement. A Vision recorder (Brain Products GmbH, Germany) was used for EEG measurements. Experiments were conducted in a soundproof dark room to minimize noise due to external stimuli such as visual and auditory. We asked the subjects to maintain a comfortable position for relaxing the tension. We gave 5 min between each frequency and 10 min of rest between the stimulation sites to prevent sensory adaptation.
Mu rhythm analysis
To compare the degree of Mu rhythm change by vibration frequencies including none-stimulus, the EEG of C3, Cz, and C4 where Mu rhythm is maximally expressed and corresponding to the sensorimotor area was analyzed. 17 Also, Mu rhythm activities in the right hemisphere were analyzed. EEG signal was sampled at 1000 Hz and the low and high cut-off frequencies were applied at 0.5 and 50 Hz. 2 s is defined as 1 epoch, and raw data are divided into 30 epochs. The Mu rhythm activity is defined as the rate of the Mu rhythm to the total EEG signal, and power spectrum analysis was performed using BESA (BESA GmbH, Germany) for Mu rhythm analysis. Paired t-test of SPSS 20 (IBM SPSS Statistics, USA) was used for statistical analysis between the vibratory frequencies (p < 0.05).
Measurement of muscle activity according to the vibratory condition
EMG measured the muscle activity of the vibratory condition, including None applied during the stair climbing. The vibratory conditions were set based on the results of Mu rhythm analysis. The vibration was applied to subject with the intensity corresponding to threshold and sub-threshold of each subject. Linear actuators and function generators were used for vibration applications. Trigno Wireless EMG System (Delsys Inc., USA) was used to record EMG signals of lower limb. The EMG sensors were placed on the subject’s left lower limb—eight sites based on SENIAN suggestions 18 (tibialis anterior (TA), gastrocnemius lateralis (GL), gastrocnemius medialis (GM), soleus (SOL), vastus lateralis (VL), vastus medialis (VM), rectus femoris (RF), and hamstring (HAM)).
Protocol of stair climbing
A custom five-step staircase of 16 cm (riser) and 30 cm (tread) was used. The gait started at one step away from the stair, and subjects climbed in a step-over-step manner. The gait cycle was defined from the first foot-contact to the second foot-contact of the same foot. Before collecting data, the subjects repeatedly practiced so that they could adapt to the stairs and walk easily. Subjects walked each step at self-selected pace. Vibratory stimulation was applied at the same time as the start of the stair climbing. All subjects measured three trials per each vibratory condition including None.
EMG analysis
EMGworks Analysis software (Delsys Inc., USA) was used to process raw EMG signals. The EMG signal was sampled at 1000 Hz. The maximum voluntary isomeric contraction (MVIC) of each subject was measured to normalize the raw EMG signal. Before the MVIC measurement, the subjects were given two practices to achieve maximum muscle strength. The Biodex System 3 (Biodex Medical Systems Inc., USA) was used for MVIC measurements. EMG amplitude was normalized by the peak of MVIC amplitude and averaged three trials of the vibratory condition and then the ensemble average was calculated using the average curve across all subjects.
Result
Changes in Mu rhythm
Figures 1 and 2 show the Mu rhythm reduction rate of ACT and QT, respectively. The Mu rhythm reduction rate means how much Mu rhythm decreased in the vibratory stimulus condition compared with the None condition. The Mu rhythm was decreased at all frequencies than None (Figures 1 and 2). Also, the reduction rate was different for each frequency in electrode site. In addition, the same frequencies showed a different reduction rate according to the stimulation site. There was no significant difference of Mu rhythm between the electrode sites at the same frequency, but it was confirmed that the reduction rate was different.
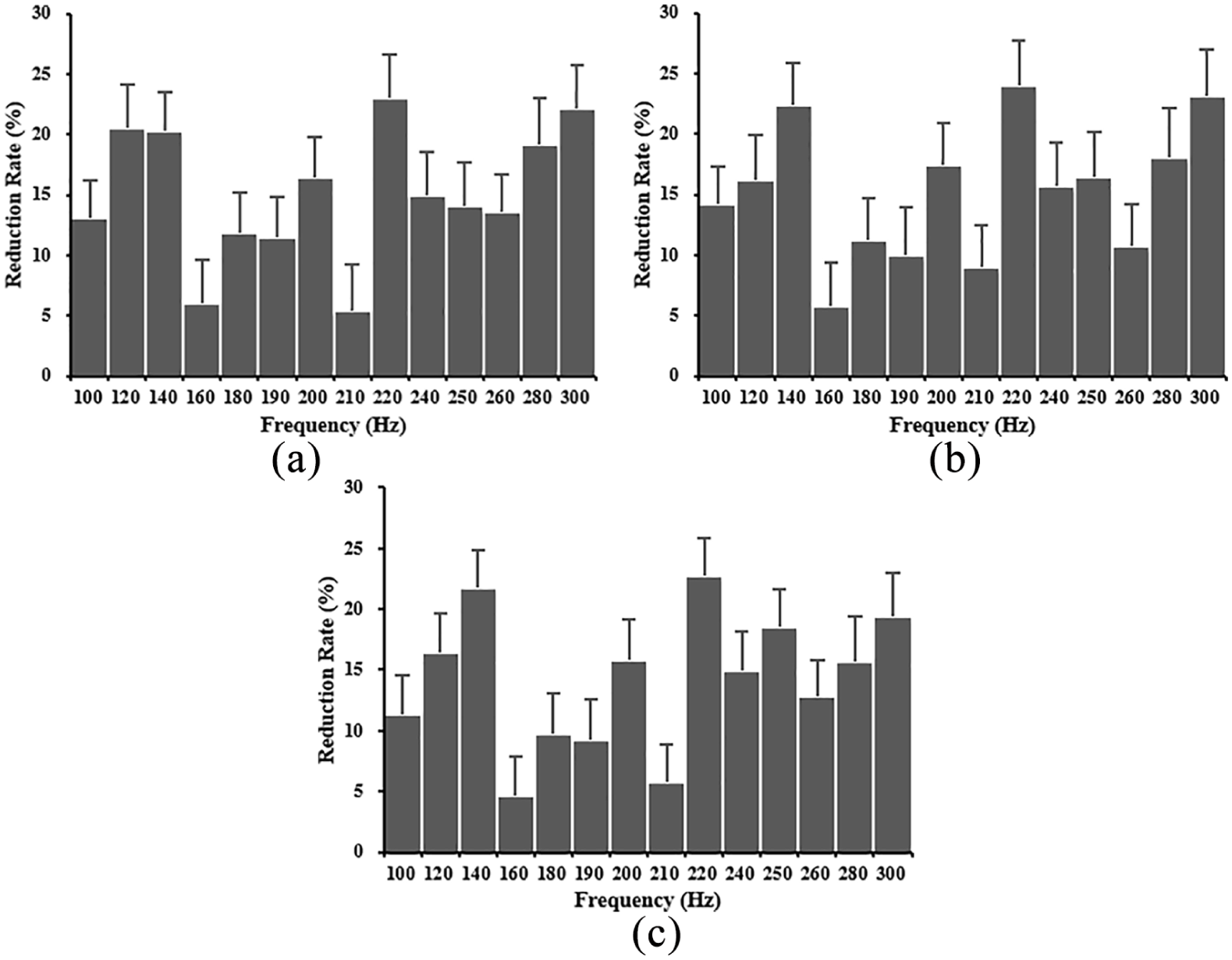
Mu rhythm reduction rate of ACT: (a) C3, (b) Cz, and (c) C4.

Mu rhythm reduction rate of QT: (a) C3, (b) Cz, and (c) C4.
Figure 3 shows the change of Mu rhythm reduction rate in the right hemisphere. The grayscale behind the line shows the standard deviation. The three markers in each line mean the specific frequencies (p < 0.05). These specific frequencies in the ACT were 140 Hz with the highest reduction rate (HRR) and 160 Hz with the lowest reduction rate (LRR). Also, the specific frequency with average activity between 140 and 160 Hz was 240 Hz. In the QT, the HRR was at 190 Hz and the LRR was at 260 Hz. 220 Hz showed an average activity between 190 and 260 Hz.

Mean of the Mu rhythm reduction rate in the right hemisphere: is specific frequencies with statistical significance in ACT (p < 0.05) and  is specific frequencies with statistical significance in QT (p < 0.05).
is specific frequencies with statistical significance in QT (p < 0.05).
Based on these results, the vibratory conditions were set. The intensity of vibration is set to threshold and sub-threshold. The HRR condition was set at 140 Hz for ACT and 190 Hz for QT. The LRR condition was set at 160 Hz for ACT and 260 Hz for QT. The middle reduction rate (MRR) condition was set at 240 Hz for ACT and 220 Hz for QT. For example, when the HRR is applied to the stair climbing, vibration of 140 Hz is applied to the ACT and vibration of 190 Hz is applied to the QT at the same time.
Muscle activity according to the vibratory condition
For threshold condition
Figure 4 shows the degree of muscle activation changed by the vibratory condition during the stair climbing. TA showed the highest peak of HRR compared to None. However, LRR and MRR showed the lowest peak. GL, GM, and SOL showed higher activity than None in HRR. MRR and LRR showed lower activity. Also, the highest peak of GL and GM appears later than None. VL and VM showed the highest peak in MRR. In VL, HRR showed a lower peak than None, while VM showed a higher peak in all vibratory conditions than None. RF showed a higher peak in LRR, and in HAM, there was no noticeable change between all vibratory conditions including None.

Changes in muscle activation patterns of stair climbing according to threshold conditions: (a) tibialis anterior (TA), (b) gastrocnemius lateralis (GL), (c) gastrocnemius medialis (GM), (d) soleus (SOL), (e) vastus lateralis (VL), (f) vastus medialis (VM), (g) rectus femoris (RF), and (h) hamstring (HAM).
For sub-threshold condition
The changes in muscle activation of vibratory conditions are shown in Figure 5. TA showed higher activity in HRR than None, but no significant difference. LRR and MRR showed the same or slightly lower activity than None. HRR and MRR in GL showed higher activity than None, but showed a slightly lower peak compared to the threshold. Also, GM showed the same pattern for the threshold, but it was found that the peak value was lower than None in all vibratory conditions. In the case of SOL, LRR showed the same activity for None, and the vibratory conditions showing lower activity than None are HRR and MRR. MRR, unlike the threshold, showed the lowest activity. VL and VM showed higher activity in MRR than None. LRR and HRR showed phase shift but the peak values indicated no significant difference. RF showed the same activity in all vibratory condition including None, but the highest peak in LRR appears later than the peak of None. Like the threshold condition, HAM could not identify the difference between the vibration conditions including None.

Changes in muscle activation patterns of stair climbing according to sub-threshold conditions: (a) tibialis anterior (TA), (b) gastrocnemius lateralis (GL), (c) gastrocnemius medialis (GM), (d) soleus (SOL), (e) vastus lateralis (VL), (f) vastus medialis (VM), (g) rectus femoris (RF), and (h) hamstring (HAM).
Discussion
The purpose of the study was to investigate the vibration frequency that the sensorimotor area is sensitively responding and to confirm the changes in muscle activity when applied vibratory stimulus during stair climbing.
Responses of the sensorimotor area to the vibration frequency
To find the vibration frequency that the sensorimotor area responds sensitively, the vibratory stimulus was applied to ACT and QT and the Mu rhythm activity was analyzed. As a result, it was confirmed that Mu rhythm activity decreased at all frequencies than None. This means that vibratory stimulus signals begin from the muscle spindles travels along the proprioceptive pathway, reaches the thalamic ventral posterolateral nucleus, and finally, reaches the somatosensory in turn, the motor cortical area in linked to somatosensory. 13 In other words, the sensorimotor area was activated by the vibratory stimulus, and this appeared as a change in the Mu rhythm. We can confirm that the same frequency has a different reduction rate depending on each stimulation site and there is a difference in the reduction rate between each vibration frequency in each stimulation site. The difference of the Mu rhythm reduction rate in stimulation site is due to the distribution and density of the sensory receptors. 19 This means that there is a difference in the acceptability of each body parts to accept vibration. It can be assumed that there is a difference in information transmitted by sensory receptors to the central nervous system depending on the vibration frequency. 20 In other words, the activity of the primary spindle endings, which is a sensory receptor, is dependent on the vibration frequency and the intensity of the vibration, 21 and our result is consistent with previous studies that muscle–tendon vibration has a frequency-dependent effect on excitability of the cerebral cortex. 22 Therefore, the vibration frequency that showed the highest Mu rhythm reduction rate (140 Hz for ACT, 190 Hz for QT) may be the most sensitive frequency at each stimulation site.
Based on these results, we set the frequency of the vibratory stimulus conditions for application during the stair climbing. HRR condition was set as 140 Hz for ACT and 190 Hz for QT, MRR condition was set as 240 Hz for ACT and 220 Hz for QT, and LRR condition was set as 160 Hz for ACT and 260 Hz for QT.
Influence of vibratory conditions based on Mu rhythm to stair climbing
To confirm changes in the muscle activity according to vibratory condition, the EMG was measured during the stair climbing, and the vibratory stimulus was applied to the ACT and QT at the same time.
EMG analysis showed muscle activation patterns of the lower limb. GL, GM, and SOL are activated after the first foot-contact. This is presumably due to push up the body and to maintain through the single-limb support during the swing phase of the opposite leg.4,23 TA is activated after toe-off. It was presumed that the ankle is flexed to ensure stability and the foot clearance when the leg is moved to the second foot-contact. The activity of VL, VM, and RF appeared when reaching the leg for second foot-contact. The reason is presumably to control the proper extension of the leg for the second foot-contact. The activity of HAM showed a low but sustained activity change across the first to the second foot-contact. This may be to maintain knee flexion during the swing phase and to prevent excessive knee extension when the leg is stretched for the second foot-contact. These HAM activations were confirmed through a result of the previous study investigating muscle activation patterns during stair climbing and level walking. 3
We could be confirmed that muscle activity increased than None when the vibratory condition was applied in the threshold. But, sub-threshold did not confirm the effect of increasing muscle activity like threshold. However, it was found that the active timing and the peak change were observed. It is assumed that muscle activity did not show a significant increase, but affected the lower limb muscles. At the threshold condition, the MRR was most noticeable among the vibratory conditions. GL, GM, VL, and VM were especially affected. The result is harmonious with previous studies that confirmed the improvement in muscle strength of the triceps muscle of calf during vibration application to the ACT. 24 Also, the increase in the muscular activation of the thigh is consistent with the results of previous studies showing that EMG amplitude of the quadriceps femoris muscles increased by applying local vibration to the quadriceps femoris tendon. 25 The vibratory condition in the GL and GM showed clearly a higher peak than None during push-up after first foot-contact. The reason for this increased peak value is presumably that vibration applied to the tendon can activate the proprioceptive sensory system, which is based on the excitation of Ia afferent signal from the neuromuscular spindle. 26 Also, vibration, in turn, activates large α-motoneurons and leads to recruitment of motor unit. 27 Finally, this motor unit recruitment leads to an increase in the force output. Therefore, these increases in the force output were confirmed by EMG. The SOL was activated at the same time with the GL and GM, and the SOL showed higher activity than None at the vibratory condition. But muscle activity was lower than GL or GM. TA did not show an increase in the muscle activity due to vibratory conditions. This seems to be because the vibratory stimulation is not applied directly. However, the HRR showed that the peak is faster than None. It can be explained with the HRR of GL and GM. The activity of GL and GM decreased after the peak, but the activity of HRR decreased faster than None. This suggests that because the GL and GM activity for the push-up terminated prematurely, the activity of the TA rapidly exhibited the toe-off progressed. The activity of VL and VM increased when reaching the leg for second foot-contact. The highest peak was observed when applied the MRR. This presumed because the flexion of the leg is reduced by vibration 28 and the distance of foot placement can be increased to ensure a wider base of support. As a result, it is thought to contribute to posture stability. RF did not change after toe-off, presumably because it was not involved in hip flexion for lifting the leg. However, the activity of RF appeared in the second foot-contact with VL and VM. The activity of MRR in RF inferred for the same reasons as VL and VM. In addition, it is also assumed that RF plays the role of VL and VM. It is considered that the HAM showed no significant increase in the muscle activity between the vibratory conditions because the vibration is not applied directly like TA. This result is related to the previous study which confirmed that there was no change of hamstring muscle strength when local vibration was applied to the hamstring. 29
We confirmed the order of muscle activity and activation patterns through EMG, assuming that the vibratory stimuli will assist the muscular function of the lower limbs when stair climbing. We could confirm that vibration based on the Mu rhythm can help functional assistance of stair climbing motion. But, we need additional information such as kinetic and kinematic factors to better understand the effects of vibratory stimulus applied to motion. For that reason, the further study is needed to analyze the kinetic and kinematic factors using the three-dimensional motion analysis system to comprehend the interactions and changes of the lower limb segments during the stair climbing applying the vibratory stimulus.
Conclusion
In this study, it was confirmed that there is a specific vibration frequency that the sensorimotor area responds sensitively according to the stimulation site. Based on this result, we could observe the change of the muscle activity of the lower limb when applying the local vibratory stimulus during the stair climbing. Our results show that the excitability of the sensorimotor area is dependent on the site and frequency. It is shown that when applying local vibratory stimulus, appropriate frequency should be used according to the stimulation sites. In addition, the application of local vibratory stimulus during stair climbing resulted in an increased muscle activity. Therefore, it is expected that the results of this study can be utilized for the functional motion assistance for persons’ difficulty in everyday activities, and it will be useful for patients with weak musculoskeletal system in the clinical and rehabilitation fields.
Footnotes
Handling Editor: Wen-Hsiang Hsieh
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science, ICT & Future Planning (NRF-2017R1A2B2009389).