
Abstract
Most gait training systems are designed for acute and subacute neurological inpatients. Many systems are used for relearning gait movements (nonfunctional training) or gait cycle training (functional gait training). Each system presents its own advantages and disadvantages in terms of functional outcomes. However, training gait cycle movements is not sufficient for the rehabilitation of ambulation. There is a need for new solutions to overcome the limitations of existing systems in order to ensure individually tailored training conditions for each of the potential users, no matter the complexity of his or her condition. There is also a need for a new, integrative approach in gait rehabilitation, one that encompasses and addresses all aspects of physical as well as psychological aspects of ambulation in real-life multitasking situations. In this respect, a multidisciplinary multinational team performed an overview of the current technology for gait rehabilitation and reviewed the principles of ambulation training.
Keywords
Introduction
Gait rehabilitation technology is growing exponentially as regaining a functional gait is seen as a must for an independent living in real-world scenarios. The drive for development comes as a result of the wide range of gait impairments in many neurological, medical and traumatic conditions that generate highly specific ambulation disabilities.
Gait-related disabilities in numbers
It is estimated that 15% of the global population – more than 1 billion people – live with some form of disability, of whom 4% have severe disability. 1 In 2015, 22% of US adults reported some form of disability, while disability in mobility was the most frequent type (59%). Prevalence of any type of disability was highest among people aged over 45 years old. 2 Half of the persons presenting difficulties in physical functioning have a gait disability. About 7.5% of adults in the United States are unable (or find it very difficult) to walk a quarter mile. 3
Disability generated by dysfunctional gait is a most common presentation of disability across Europe, too, with 5 million European citizens depending on a wheelchair. 4 The global population is ageing and, with age, chronic conditions generate more gait impairments and gait related disabilities which reduce individuals’ ability to perform activities of daily living (ADL) and his capacity to participate in social (professional as well as family) life. In 2013, 27% of European adults had moderate or severe long-standing limitations in ADL due to health problems. 5
Due to new developments in health sciences, access to healthcare, as well as to improvements in life style, life expectancy is increasing. A United Nations (UN) report demonstrated that the age demographic is changing significantly. At present, slightly more than 1% of the global population is over 80 years old and it will rise up to 4% in 2050. 6 Similarly, by 2050, the number of people over 60 will outnumber those between 10 and 24 years old. 7
Central neurological conditions represent the main source of gait related disabilities worldwide. Disability through neurological disorders of gait can be caused by acquired brain injury due to stroke or traumatic brain injury (TBI) as well as by neurodegenerative diseases such as Parkinson’s disease (PD) and multiple sclerosis (MS).
Secondarily, musculoskeletal conditions associated with falls and fall-induced injuries in elderly people are common worldwide and the ageing population trends will further raise the socio-economic burden and healthcare costs.
Stroke prevalence in White individuals is 500–600 per 100,000 individuals. 8 The incidence of stroke doubles with every 10 years passing after the age of 55, reaching the highest rate in the population over 85 years old. 9 At present, studies have revealed that brain disorders are much costlier than had been anticipated.
These costs represent a major health economic challenge all over the world. It is very difficult to have relevant statistics, even in Europe, due to the large variety of brain disorders and disabilities involved and due to lack of relevant data per year/country/disease. It is estimated that in 2010, European total annual cost was € 64 billion for stroke, € 33 billion for TBI, € 15 billion for MS and € 14 billion for PD. 10
An exemplary study made in 2011 in the United States on cost analysis of specialist inpatient neurorehabilitation services shows that the median total costs/bed-day were between £402–£530 (€ 459–€ 650) for adults. Children’s services cost almost twice that (£1017–£1177). 11
Taking stroke as an example, again, current statistics in United States indicate that 40% of stroke victims experience moderate to severe impairments requiring special care 12 and 60% of stroke survivors will regain independency in self-caring daily activities. About 75% will be able to walk, but 20% will need institutionalized and permanent healthcare.
In the United States, costs per stroke patient are between US$60,000 and US$230,000, representing 6% of the federal budget destined for healthcare and social services. 13 The indirect costs related to decreased productivity and thus taxes, as well as the non-economic costs of disability, generated by confinement and social stress are immeasurable for those directly and indirectly affected. 14
The perception of the general population on disability also has to change. About 38% of British people thought, in 2010, that the disabled are a burden, in a situation where 27% of young disabled British have a severe ambulation disability, while 72% of British wheelchair users are aged over 60. 15
Why advanced technology for gait rehabilitation?
Pathologic modes of walking provide slower speed and worse gait quality consume more energy and correlate with lack of stability and high risk of falling, leading to even more distorted gait patterns. Usually, the person with gait disability presents not only with sensorial deficits, lack of muscle strength and impaired muscle control and coordination, reduced effort capacity but also with different degrees of cognitive impairment; pain and movement avoiding strategies.
Rehabilitation of gait and ambulation disabilities involves multiprofessional and multidisciplinary teams. The therapeutical window for rehabilitation after stroke is fairly tight, with functional recovery being achieved at higher rates in the first 3–4 months, slowing exponentially in the following 3 months. At 6 months after stroke, functional recovery enters a plateau, requiring special intensity efforts. 16
Gait rehabilitation requires early mobilization, a long period spent in intense physical exercise and specific technology. Epidemiologic studies suggest that higher levels of physical activity prevent fractures and clinical trial data suggest that exercise programmes may reduce risk of falls. Nevertheless, there is a shortage of specialized staff in rehabilitation medicine; the document ‘Guidelines for Adult Stroke Rehabilitation and Recovery. A Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association’ (2016) states that stroke rehabilitation requires a sustained and coordinated effort from a large team, including the patient and his or her goals, family and friends, other caregivers (eg, personal care attendants), physicians, nurses, physical and occupational therapists, speech-language pathologists, recreation therapists, psychologists, nutritionists, social workers, and others.
17
Technology for gait rehabilitation should empower the physical therapist to (1) promote new motor skill acquisition and training in order to stimulate restorative neural plasticity and avoid interference of pathological compensatory mechanisms (recovery vs compensation), (2) schedule therapies that can induce the acquisition of transferable motor skills, (3) focus on both repetition and intensity of training 18 and (4) increase the time of effective rehabilitation intervention.
Using advanced technology for gait rehabilitation is beneficial in terms of reducing the effort on the physical therapist. In terms of reducing the overall costs of disability and rehabilitation, by providing efficient, intensive, gradable and highly reproducible training.
Improved inter-professional staff education and training, greater patient and caregiver involvement in the rehabilitation programme and early mobilization protocols are crucial to prepare and support efficient rehabilitation approaches. 19
The worldwide clinical guidelines’ advice is for early, multimodal, intensive, individually tailored interventions in stroke rehabilitation and recommends the development and the rational therapeutic use of newer technologies such as virtual reality (VR), body-worn sensors and electromechanical systems for post-stroke gait rehabilitation. 20 The National Clinical Guideline for Stroke (Royal College of Physicians, London) recommends the same, adding that the patient should be taught to use the mobility aids, for safety and efficiency. 21
The article reviews some aspects regarding the current state of advanced technology for gait rehabilitation and to present the perspective of a multinational multidisciplinary team on future gait rehabilitation and ambulation rehabilitation.
Current state of technology for gait rehabilitation – robot-assisted gait training
Basic physical therapy for motor recovery in stroke and spinal cord injury (SCI) is low tech and includes overground walking therapy (OWT, walking with the aid of side parallel bars and physiotherapists), muscle strength training (i.e. eccentric or concentric repetitive exercises) and transferable skill training (sit-to-stand, tilted-table-standing and fitness exercises).
Body weight–supported treadmill (TM) training (BWSTT) has been proposed and gained a lot of attention for its advantage to allow patients to start training very early in the recovery process (as a result of harness support), to repeat stepping sequences with high intensity and for its advantage to help improving posture and gait pattern. 22 This therapy is exhausting for physical therapists who are needed to assist with lower limbs movements. 23
Robot-assisted gait training (RAGT) – Robotic systems were developed to allow BWS without the need for manual assistance to be provided by the therapist. RAGT allows natural and symmetric walking patterns while increasing the intensity and duration of the training sessions (since they do not rely only on the physical therapists) and can also record patient performance through embedded sensors. Robotic systems can partially or completely guide the lower limb movements through adaptive controllers, thus allowing subjects to try to initiate the movement (efferent motor commands) and eventually assisting them to finish it (afferent feedback drives).24,25
The Lokomat system (Hocoma, Zurich, CH, Switzerland) is an example of a RAGT system and consists of a TM equipped with a harness supporting the patients in an upright position and with robotic arms that can be attached to the patient’s legs to move them in a natural and symmetrical pattern. 26
Split-belt TMs have two independently controlled belts which permit different motor patterns on the two legs (e.g. one could step two times faster than the other) and the exploration of gait adaptation paradigms specific to the patients’ needs. A very recently developed system, the MIT-Skywalker (InMotion Technologies, Boston, MA, USA), exploits the principle of the split-belt TMs and goes beyond the standard therapies.27,28 MIT-Skywalker can be programmed to train rhythmic movements (speed and symmetry training), discrete movements (heel strike practice) or balance, potentially stimulating different neural circuits according to the task. 29 The system can accommodate patients with different pathologies by modulating speed and task and it allows the patients to engage with the task while ensuring self-directed movements.
Technologically empowered overground gait training is still under review regarding its efficiency, even if natural intuition says that, being the most life-like, it should be the best approach for ambulation training in the advanced phases of the rehabilitation process. 30 We conducted a bibliographical search and developed several classifications of these systems.
Drive modes and control strategies of gait rehabilitation technologies
The most used drive modes highlighted by X Zhang et al. 31 in a recent comprehensive review are hydraulic drive, motor drive, pneumatic drive and series elastic actuator, pneumatic muscle and electronic rod. The disadvantages of these drive modes are: limited power, increased mass and volume as well as noise.
The control strategies of current systems identified by the authors in Beijing are as follows: position control (trajectory tracking control); force signal control with three versions, (a) force signal produced by muscle contraction and interaction with the mechanical part of the system and measured by force and moment sensors, (b) a hybrid between force and position control, as well as (c) impedance control; and biological–medical signal control, using surface electromyographic bursts (EMG) indicating muscle-specific activation and electroencephalography (EEG) signals indicating the voluntary intention to move. 30
Classifications of technologies for gait rehabilitation
X Zhang et al. identified the following categories of RAGT:
TM-based exoskeleton robots (Lokomat, LokoHelp, Lopes and Active Leg EXoskeleton ALEX);
Leg orthoses and exoskeletons (The Active Ankle–Foot Orthosis – AAFO, 30 Knee–Ankle–Foot Orthosis – KAFO, Berkeley Lower Extremity Exoskeleton – BLEEX and Hybrid Assistive Limb – HAL);
Foot Plate–Based End-Effector Devices (Gait Trainer GTI, Haptic Walker and the G-EO Systems);
Platform-Based End-Effector Robots (The Rutgers Ankle, ARBOT and parallel ankle robots). 31
G Morone et al. make the distinction between exoskeletons moving joints and assisting gait movements and end-effectors addressing especially if not only the feet and imposing gait movements. They also identify static and dynamic systems, from the respect of restricted defined space over free space for user walking. 32
In the following classifications, we excluded devices for one joint (two segments) movement training purpose (Kinnect, Rutger Ankle) and only systems developed for whole body gait training will be considered.
In Table 1, we propose to classify the gait training systems according to the nature of the walking surface, as well as the modalities used for antigravitational assistance, to the training scope and to the user–system relationship (Patient Follows System – PFS versus System Follows Patient – SFP).
Classification of gait training systems according to walking surface.

BWS: body weight support.
Body weight support – In usual clinical activity, physiotherapists partially support the patient’s body weight during training, often using their own body strength. Conducted physical therapy exercises are thus possible for patients who have an ambulation index of 1 and 2 on the Functional Ambulation Scale. 48
Balance is one of the most studied aspects of motor control and motor learning. Balance during walking activities depends on the position of the axial body structures, the small support surface and the high and dynamic position of the centre of gravity, which has a latero-lateral sinusoidal trajectory in the vertical plane.
Posture represents the alignment of the body segments which allows balance keeping. Postural control involves the processing of a diverse range of sensory and cognitive inputs, involving continuous and intermittent feedback control 49 for ensuring body stability and precision while performing sustained and ballistic movements. Postural control may be disrupted by internal activities (changes in metabolism and in cardiac and respiratory activities) and by musculoskeletal and nerve pathologies. 50
Suspension in BWS is usually performed vertically, from above the head of the person in the harness, thus achieving posturing in orthostatism. 22 There are also devices that secure the patient in the system from behind, from the dorsal-lumbar area, for example, the Kineassist device. 51
Vertical suspension systems have a single point of attachment in the suspension mechanism. Therefore, there is no control over the direction of the harness in relation to the direction of walking or the lateral distribution of the weight. In case of systems such as the Lokomat and LOPES, the lack of control over the direction of the harness is compensated by the presence of a frame/handle for hands, the use of active orthoses for lower limbs and pelvis. 52
The Unweighing Support System and the VectorG device created at Biodex are equipped with pressure transducers that allow the control of the weight discharged based on the movement of the centre of mass. The VectorG device allows gait training with posture and reflexes training in the event of falling, the device having a delay relative to the time of the falling event (long enough to enable the triggering of the protective behaviour). 53
The RELIVE weight suspension subsystem has two anchor points (with a controlled position) to the mechanical support subsystem. Due to a mechanism generating vertical alternative oscillations, it allows training pelvic girdle movements, too. Pelvic girdle size and movement ranges vary greatly depending on gender, body size and walking speed, and the system can adapt to these. 54
Exskeleton parts – Pelvic orthoses are a new item in the arsenal of assistive devices used in rehabilitation. Movement of the pelvis during walking includes forward inclination (4°), downward movement of the contralateral side of the pelvis with regard to the lower limb standing in the balance (4°), transverse rotation (10°). 55
There are both nonpowered passive assistive and powered active assistive devices of this type designed to keep the posture in static and dynamic equilibrium and to correct the vertical and horizontal displacement of the centre of mass while walking. The active pelvic orthoses consist of technical solutions adapted to fixed or mobile training systems.
The WalkTrainer system allows a physiological walking exercise over ground by associating a body weight suspension subsystem with a fixed point of suspension within a mobile system with active orthoses for lower limbs and pelvis and with functional electrostimulation. 42
The Pelvic Assist Manipulator (PAM) system allows the recording of pelvic movements and the restoration of the trajectory through mechanical action of the pelvis in a fixed gait training system with TM. 56
The Lokomat Pro system ensures that weight passes from the right half of the body to the left and vice versa during the walking cycle as well as the rotation of the pelvis in the anterior–posterior plane. Lokomat systems also use orthotic parts for lower limb movement assistance.
Whole-body exoskeletons provide mechanical support by adjusting the degree of stiffening at the joint level and may provide real-time assistance of actively driven movements in overground free ambulation. 57
Advanced technology must be rationally used. It seems that acute nonambulating and subacute persons may benefit the most from training with electromechanical devices 58 and exoskeletons. 57 These results might be due to the fact that in acute and early subacute phases of rehabilitation after stroke, phenomena of spontaneous neuroplasticity occur with increased intensity.
Table 2 gives an indicative frame of appropriate technology related to the gait rehabilitation stage and to the level of assistance the person with disabilities requires.
Classification of gait training systems according to rehabilitation stage and to the need of assistance.

BWS: body weight support; HAL: Hybrid Assistive Limb.
Table 3 shows a classification of the gait training technology regarding the regimen of the training (guided by the system – PFS or by the user – SFP) and the training objectives.
Classification of gait rehabilitation technology according to the training scope and to the user – system relationship (Patient Follows System (PFS)/System Follows Patient (SFP)).
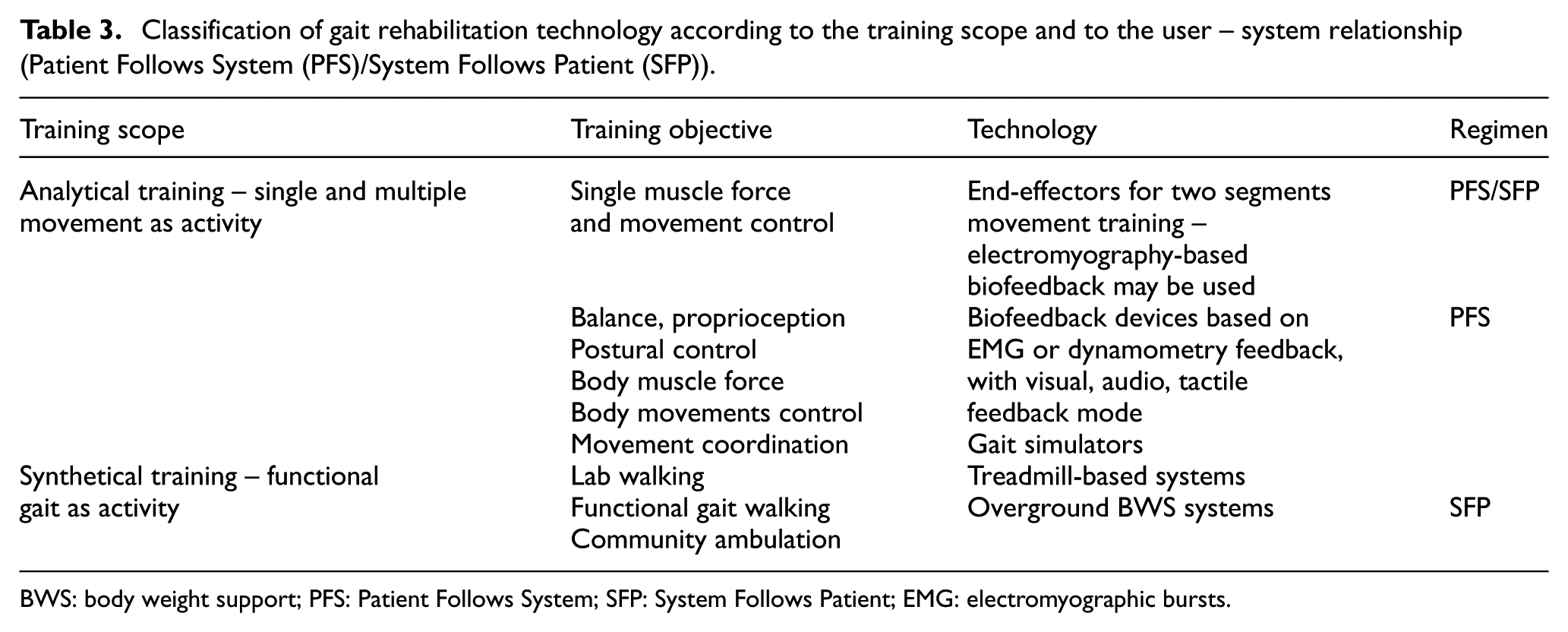
BWS: body weight support; PFS: Patient Follows System; SFP: System Follows Patient; EMG: electromyographic bursts.
Body parts’ movements can be retrained one by one (analytical training) or as a whole, in functional gait movements (synthetical training).
Effects of using technology for gait rehabilitation
A Cochrane review on 36 trials with 1472 participants with electromechanical gait training devices found that using technology for gait rehabilitation clearly increased users’ odds of becoming independent (odds ratio: 1.94), but the technological approach to gait rehabilitation combined with physiotherapy increased walking speed (mean difference of 0.04 m/s) and the ability to perform 6-min walking test (mean difference of 5.84 m). 58 Another recent review, reporting exoskeleton training, found an increase of 0.4 m/s in mean speed for users presenting with some voluntary control. 33 However, one of the most important effects that we aim to achieve in all rehabilitation interventions in neurological condition is that of inducing neural plasticity, and advanced technology used for gait rehabilitation has proven to provide this.22,24
The RAGT approach to gait rehabilitation could significantly improve time and quality of motor recovery. Following RAGT training, SCI patients showed changes in spinal reflexes circuitries as well as the re-emergence of physiologically modulated H-reflexes in the soleus muscles. 59 RAGT-induced additional improvements in comparison with conventional training in stroke patients 60 and is also undertaken as a type of aerobic exercise which potentially benefits metabolic and cardiopulmonary capacities. 24
A very recent study investigated the functional connectivity correlates of RAGT through EEG recordings and demonstrated that step kinematic errors correlated with the strength of a frontal–central–parietal network observed during and post-training. This was therefore proposed as a potential neural marker of motor learning and adaptation for patients undergoing RAGT. 61 Active RAGT (i.e. with low guidance/support by the robotic arms) was shown to activate sensorimotor regions more than passive RAGT. 62 Accordingly, high level of support during RAGT (i.e. 100%, passive movement) was demonstrated to minimize the involvement of the sensorimotor cortex: as this brain region is known to be essential in visuo-motor integration, and learning during walking, lower levels of guidance should be preferred in order to stimulate active participation and cortical activations. 63 Indeed, passive movement of the impaired limb does not promote patients’ engagement: robotic systems for RAGT define a specific trajectory and sequence of movements and impose them to the patient, preventing variability and timing of step.
Split-belt TMs allow subjects to behave naturally and to explore different motor control strategies. 64 Walking speed was increased with stroke patients in order to augment step length asymmetry and this induced after-effects of reduced step length asymmetry in overground walking, even maintained in the long term with repeated practice. The MIT-Skywalker was tested with stroke and cerebral palsy patients and was shown to be able to accommodate each patient and successfully induce locomotor and balance improvements. 28
There are studies suggesting that TM systems and overground training give different results regarding different gait parameters. Ultimately, what we aim for is that our patients walk over the ground, this being their natural condition. 65
A device that allows the suspension of body weight above the head has the advantage that it discharges symmetrically or asymmetrically the person’s weight (the subsystem can allow a controlled weight discharge) and allows the maintaining of the alignment of the trunk and limbs. Therefore, early gait training after stroke is possible without high energy consumption from the patient. Partial weight support not only makes it possible to have a longer-lasting training with controlled posture and safety but also has some effects on walking parameters:
The length of the double phase support is reduced and the duration of the unipodal support phase is increased;
The need for antigravitational postural control is reduced, as the weight discharge level increases, the magnitude of EMG for the erector spinae, gluteus medius, vastus lateralis and gastrocnemius muscles decreases;
The magnitude of the EMG signals is reduced in the sural triceps muscle and increases in the anterior tibial muscle during the balance phase, which can ease the detachment of the foot from the floor;
The maximum knee and hip balancing angles are reduced, perhaps due to the limited excursion of the centre of mass;
The amplitude of the lateral and anterior–posterior movements of the torso is decreased. They are associated with the heel’s attack and the initiation of the balance phase. 66
Regarding the use of these devices for gait rehabilitation through training on the TM, studies show different effects:
For gait rehabilitation after stroke, body weight support (BWS) training on TM proved to be as effective as ground training for walking speed and endurance improvement (for patients who can ambulate). For patients in the acute stage, effects on walking ability and walking speed are superior when using BWS devices. 67
Neurodevelopmental approaches are inferior in improving walking speed and walking category compared to BWSTT during post-stroke inpatient rehabilitation. 68
Electromechanical gait trainer with Functional Electrical Stimulation (FES) simultaneously improves scores on the Barthel Index, Berg Balance Scale, Functional Ambulation Categories Scale and Motricity Index. 69
For gait rehabilitation after spinal cord injuries, there is an increased efficiency in the recovery of the gait capacity and of the walking speed. The persons with the greatest deficit had the greatest benefits. 70
Gait rehabilitation in PD – the walking speed and the length of the step are increased. 71
Gait rehabilitation in MS – the walking speed and the maximum walked distance are improved.72,73
There is less information on the effects of using partial weight suspension for overground training. A study on the influence of a suspension device on ground walking parameters in people with post-stroke chronic hemiparesis (more than 1 year after onset) resulted in decrease in the step length, reduced amplitude of movements in the bilateral coxofemoral joint, reduced amplitude of the thigh and calf movement under weight discharge conditions, improved postural alignment and stability and decreased travel speed. The partial suspension device can be used with or without weight discharge in incomplete SCI patients, with beneficial effects on the energy costs of walking and posture. 59
The use of different technologies is a challenge by itself due to the limitations of current systems: delay in functional responses, unloading, the harness’ constraints, noise, the stress of being at the mercy of a nonhuman entity.
The energy expenditure must be a concern when training people in old age or with acute and subacute neurological conditions. A 2016 systematic review on 14 studies on stroke and spinal cord–injured participants states that RAGT with BWS is less energy consuming and less demanding for heart and lung than overground training using no technological assistance. 74
Moderate discomfort due to tight straps, heavy weight of the device, moderate pain at cuffs (all solved by readjusting), as well as four cases of orthostatic hypotension (due to the patients’ condition) have been reported related to using HAL.47,75
One study on exoskeleton training in post-stroke rehabilitation included in a 2017 review reported minor temporary adverse effects – skin irritation and pain from cuffs and electrodes for bioelectric detection. 33 There is a report on a ReWalk user getting a hairline bone fracture of the talus after using the device. 76 Bone mineral density should be assessed before proceeding to training with robotic devices to avoid such accidents. 77
While adverse effects are transitory and mainly due to lack of individual adjustments, the beneficial effects of technologically assisted gait training can be seen even after one single session. For example, one session of training on TM with FES on dorsi and plantar flexors increases the peak of anterior ground reaction force and of integral ground reaction force in post-stroke users. 78
There is general agreement that there is not enough evidence to show that there is a rehabilitation technique superior to others in terms of efficiency. It is, though, clearly stated that more constraining systems (as Lokomat) seem to be more efficient in the early phases of gait rehabilitation and for severely impaired patients, while using a BWS on a TM is more efficient in more advanced phases of the rehabilitation process, and for less severely impaired patients. 79
The perspective of a multinational multidisciplinary team on gait rehabilitation – ambulation rehabilitation
To design technology destined to be used in gait rehabilitation is a great challenge. Pathologies generating gait related disabilities are extremely diverse, and the specific impairments individuals present with are rarely simple.
During bipedal locomotion, the motor control system supports body weight, gives forward and lateral stability and promotes forward progression. These processes can be damaged or even stopped in the event of a neurological injury or disease. Lesions of any levels of the hierarchical control system impairs initiation, maintenance and modulation of posture and gait. In the advent of a stroke, cortical and descending neural pathways are damaged or disrupted, but spinal and musculoskeletal systems remain intact, as well as usually brainstem and cerebellum. 22 Gait abnormalities after stroke can be due to the pathology itself (i.e. disruption of descending pathways) or to developed compensatory strategies (i.e. abnormal adaptive processes).
Stroke survivors usually exhibit reduced walking speed and asymmetrical walking behaviours, and the unaffected side is usually most involved in carrying the body weight and propelling the body forward. This abnormal behaviour causes spatio-temporal asymmetries (e.g. shorter stance and longer swing times of the affected limb, shorter step length of the unaffected limb) and is strongly correlated with risk of falls and balance impairments. 80
Another potential consequence of a brain infarct is muscular impaired control, whereby muscles often show spasticity (due to the hyper-excitability of spinal reflexes), atrophy (due to limb initial immobilization) and/or abnormal co-activation patterns (i.e. synergies, modules). The latter may be an adaptive strategy adopted to generate joint stiffness and compensate for gait instability. A reduced number of activated muscular modules was registered in stroke patients in comparison with healthy subjects during gait, possibly resulting from merging healthy synergetic patterns together. 81 The number of observed modules correlated with gait velocity and asymmetries and thought to result from adaptive responses of the central motor system for the automatic and simplified control of the affected limb. 82 Asymmetries characterize arm swing and trunk movements as well in gait post-stroke with an increase in trunk rotation compensating reduced pelvis rotation 83 and increased trunk acceleration especially in the medio-lateral direction. 84 Abnormal trunk movement magnitude has been recently shown to be a reliable marker of movement stability and abnormality in healthy adults, in post stroke and even in PD patients. 85
Stroke severity determines the functional capacity of the patient. Age, cognition and the functional level after stroke are consistently associated with post-stroke rehabilitation outcomes. 86
Patients with cerebellar damage due to stroke are able to react to movement changes during gait as well as to learn predictive locomotor adaptive strategies, whereas patients with non-stroke cerebellar impairments are not (e.g. split-belt TM protocols). 87
A completely different scenario concerns SCI patients, affected by a partial or complete lesion of the neural pathways embedded in the spinal cord which causes reduced or lost control of those body parts whose peripheral nerve starts below the injury location. Locomotor abilities are severely affected in SCI patients and only those with partial lesions have the potential to restore gait control via specific rehabilitation therapies. 24 This is supported by the fact that lower limb cortical representations are intact in SCI patients, which would be extremely useful for the design of assistive BCI systems. 88
The international classification of functioning framework
In the terms of the International Classification of Functioning, Disability and Health (ICF), 89 gait performing is a basic ability that ensures the person’s activity and participation capabilities level as required in order to be independent and efficient in the ADL as well as socially and professionally fit and useful. Personal factors related to medical conditions, age and related impairments in sensing and execution, cognitive functioning disturbances, as well as contextual factors related to the natural, anthropic and social environment, influence this ability. The instrument of ICF itself evolves while our understanding regarding the components of the biopsychosocial framework improves. 90
Gait is a complex activity by itself, requiring the integrity and good integrated functionality of the musculoskeletal system, of the sensory organs and of the peripheral and central nervous system (involving all somatosensory, motor and higher level cognitive as well as all executive functions). Gait is impaired and even impossible in some medical conditions, and the personal and environmental factors may support or may decrease the walking ability of the person. Gait has great specificity due to gender, body mass index, age, anatomic individualities and achieved habits, fatigue level, attention and motivation. 91 Gait is recognized as a biomarker of healthy ageing and disease; but, all the same, gait may enable identification of individuals, the same way they are identified by their unique fingerprint. 92
In the Physical Activity and Exercise Recommendations for Stroke Survivors, it is stated that The magnitude of activity limitation is generally related to but not completely dependent on the level of body impairment. Other factors that influence level of activity limitation include intrinsic motivation and mood, adaptability and coping skill, cognition and learning ability, severity and type of pre-existing and acquired medical comorbidity, medical stability, physical endurance levels, effects of acute treatments, and the amount and type of rehabilitation training.
93
The rehabilitation and assistive devices themselves provide challenges to the dynamics of the body. 94 To develop and to appropriately use a device able to adjust to every individual specific needs is a major challenge.
Outcome measures – The clinical measures of improvement (outcome measures) in gait and ambulation after a rehabilitation intervention differ based on the underlying pathology. They generally include time measurements 10MWT (10-min walking test), WISCI II (Walking Index for Spinal Cord Injury II), the measure of endurance 6MWT (6-min walking test), measured changes of speed95,96 and clinical gait observation. Gait analysis methods may involve also different technology providing instrumented motion analysis (using cameras, markers on the limb segments and calibration systems and mathematical algorithms or electrogoniometers), 97 external forces analysis (torque and reaction forces, moments and power developed), 98 muscle activity (dynamic electromyography) 99 and mechanical and metabolic efficiency. 100
There is no shared consensus on the specific clinical outcome measures that should be used to assess the effect of the electromechanical and RAGT. The selection of the most appropriate outcome measures for the future studies should start from those most commonly used in the literature, according to ICF domains (function, activity, participation). The physical therapist still remains the most sensitive assistance and compensation ‘system’ and the best real-time and emotional driving feedback generator.
A basic gait rehabilitation programme must provide improvement and retraining of posture, static and dynamic balance, muscle strength and movement control and coordination, stepping and walking forward, backwards and to the sides. Compliance, task specificity and intensity of training, in terms of hours of therapy, are the main determinants of functional improvement after stroke. 101
When striving to achieve functional gait, one must consider that gait, being by itself an activity, is generally used to help us performing a large range of other complex multiple tasks, thus determining the person’s participative capacity.
Indoor ambulation in-house or at a job requires the abilities of walking on different floor textures, turning around, avoiding obstacles of different shapes and size placed on the floor or moving around, ascending and descending stairs, adopting and maintaining different postures and positions, while reaching for and using different objects/tools/appliances. Non-instrumented and instrumented ADL may look simple from the perspective of a skilled independent nondisabled individual, but they are not.
Outdoor ambulation requires extra abilities: the ability to gain and keep balance and walk with different speeds on rough, slippery, deceptive plane or inclined surfaces; the ability to calculate speed and trajectory of different objects/persons in order to avoid/allow contact; the ability to change your speed, direction, cadence, ground reaction force, whenever needed, in due time; the ability to identify and keep the optimal trajectory to the destination point; and the ability to handle all these in different lighting, visibility and sound conditions.
Community ambulation requires also the ability to manage personal spaces and the ability to perform a lot of other tasks while walking. 102
Ambulation rehabilitation principles
In classical rehabilitation medicine, there are two different approaches: the restorative approach (interventions aimed to restore functionality) and the compensative approach (interventions aimed to assist or even cover for a lost function). The compensative intervention creates a better frame for a restorative intervention and a restorative intervention tailors the compensative intervention. Important is the commitment of the patient to the therapy. 92 The powered exoskeleton systems are an ideal solution in terms of assistance, correcting and maintaining posture, providing balance in stance, as well as in movement. End-effector systems are ideal as analytic (single movement) and synthetic (global) gait movements training. Best ambulation training requires real-life input for body and mind, therefore, nowadays, even with the developments in immersive and non-immersive VR-based systems, overground real-life gait training remains the best option in terms of proprioceptive, visual, tactile and multiple cognitive input and feedback.
When designing new technology for ambulation rehabilitation, one must acknowledge and promote new principles of training for ambulation rehabilitation:
‘SFP’, mentioned by PL Seiciu, in 2014, 103 in order to express the necessity of the active involvement and choice/intention of the patient concerning the trajectory and gait parameters he or she must follow in order to solve a specific imposed or freely chosen task;
‘Ambulatory Environment – AE’ underlines the importance of training the whole body and mind together at the same time. When we say whole body we have to realize that the unaffected lower or upper limb in a stroke patient will also not function correctly because of the affected side.
Regarding gait related disabilities, several studies have shown that rehabilitation is faster and more efficient when goal oriented close to maximal range of motion exercises are used and if VR or augmented reality is added to overground training sessions.104,105
Active walking assumes that the patient has the ability to voluntarily perform the walking movements, even with considerable assistance: the patient is supported and guided by at least two therapists (‘classical’ therapy) and he walks with all his body weight which is not always beneficial. The active mode of training has three submodes: active assisted mode, active free mode and active resist mode, 106 which can be achieved under one’s own body weight load or with different degrees of weight unloading.
Limitations of gait rehabilitation technology
A great challenge in order to provide active modes of training in safe conditions with no constraints and delay has been developing the technology allowing the system to detect the person’s intention to move for gait performing. Peripheral gait detection technologies use plantar pressure sensing technology as well as lower limb movement (EMG based) and position, forces and angles sensing technology. There is also the possibility to detect intention to move from the central nervous system, using sensing technology based on brain–computer interfaces. Exoskeletons use many technologies for movement intention detection, but there are still limitations in this approach because of vulnerability to interference, delay in processing and derived constraints, lack of 1-to-1 mapping overlap between torque and EMG signals detected and poor adaptability. 29
The majority of the existing rehabilitation devices use the repetitive methods of passive walking, in the terms of gait parameters and decisions imposed by the system or the therapist, via GUI, making the user the slave of the robotic system. Each of the actual systems for overground gait and ambulation rehabilitation, even those built to meet the principle of the ‘SFP’ has its own relative advantages and disadvantages, is presented in Table 4.
Advanced overground gait training systems with body support applying the principle ‘System Follows Patient’.

3D: three-dimensional.
Robotic systems developed very recently, such as the walker Andago – Hocoma, Switzerland 40 and the fixed unidirectional ZeroG – Aretech, Virginia, USA, 38 allow overground training within safety conditions. The need to administer the space of the walker and the movements of the user inside the system’s restricted space, respectively, the unidirectional and the relative instability of the BWS, put limits to the use of these systems. These issues are partially solved by solutions like HAL exoskeleton – Cyberdyne. Wearing the armour of the sensitive and actively assistive exoskeleton can help you walk and assists you in stepping over obstacles, proving to be an efficient tool for an assistive – compensatory approach, indeed useful as well for gait rehabilitation. However, it is not the most appropriate in order to provide safety in ambulation and self-space management training for persons within the Functional Ambulation Categories of 0–3.
The bottleneck seems to be solvable in the future, when taking into account future possible developments of technology developed recently for VR gaming, providing BWS as well as relative postural stability while the user is immersed in VR.
Main disadvantages of these systems include the unnatural contact with low-friction or high-friction special concave surfaces and the quality of the VR, even when visual and sound are combined with haptic feedback. In addition, there is no perfect harness for rehabilitation training interventions, all of them inducing focal pressure and restricting functional normal movements involved in gait and ambulation.116–121
The ambulation rehabilitation intervention
Ambulation is a complex activity involving whole body movements during gait cycle. It requires also abilities to process the data received from the physical and social environment, in order to avoid, in due time, static and dynamic obstacles, climbing and descending stairs and slopes, walking on different texture surfaces, turning around and self- and shared-space management. Normal ambulation ability involves walking with a predefined goal while multitasking in the complex interaction with the physical and social environment.
A Cochrane review from 2015 states that some attempts in this direction have been already made (virtual practice and mental imagery, community or outdoor ambulation practice), but there is still insufficient evidence to establish the effect of community ambulation interventions or to support a change in clinical practice. 122
Due to its importance, persons with ambulation disabilities strive themselves to regain walking ability. Even individuals with very low mobility capacity use in walking activities up to 30% of the time scheduled for physical therapy. 123
All these abilities may be achieved only with one’s self and environmental awareness, focused and distributive attention and with active participation and the sustained intention of the patient. For an optimal gait rehabilitation intervention, the patient must be approached in an integrative manner. An enhanced stimulating environment, biofeedback, mental imagery and multiple tasks training improve neuroplasticity and functionality and lead to better outcomes of the rehabilitation programme.124,125
Awareness, attention, memory, orientation in space and time, as well as executive functions and language training must go along the physical gait and ambulation rehabilitation programme. The International Society for Posture and Gait Research only organized the 1st Joint World Congress on Gait and Mental Function, in Norway, 24–28 June 2012.126–128
The therapeutic environment is very important as well. A facility providing an everyday environment enriched in stimuli and activities will ensure more extensive rehabilitation interventions, in time span and variety, improving in a higher rate the functional independence and the participative capacity of the persons undergoing rehabilitation, reducing overall costs of the rehabilitation inpatient stay.129–131
The therapeutic environment, in order to be of real use, must meet some requirements regarding size, shape, lighting, sound as well as interior design, aspects important when aiming to train visual and auditive perception, self-balance and proprioception, along with all the other physical and cognitive functions. 132
Multisensory stimulation through different methods can augment the training session to resemble more real-life-like conditions, allowing a natural cognitive integration and a higher level functional recovery. 133 Augmented reality and VR 134 are as good for this approach as action observation 135 and mental imagery training, 136 but the last mentioned approaches require a previous contact of the user with the technology involved and a bit of confidence in one’s imagination.
VR seems to improve outcomes of robotic gait training in MS, through positive attitude and improved problem-solving attitudes. 137 EEG studies reveal that VR induce improvements in chronic post-stroke rehabilitation outcomes by entraining several brain areas, probably through the mirror neuron system. 138
Emotion, will and social abilities must also be trained and empowered along with physical functioning and cognition. Even if nowadays we acknowledge the influence of the environmental conditions on the level of performance of training tasks, training is mainly focused on single movement’s control and coordination, as well as on lab conditions gait training. Very little time is used for community ambulation activities during inpatient (1%–5%). 61
Real-time gait biofeedback is an important tool in rehabilitation, providing objective here, and now, data aimed to improve awareness regarding one’s own degree of impairment and empowering the user to correct movement trajectory and aberrant gait patterns.139,140
Technology for ambulation rehabilitation – levels of complexity
In general terms, for assisting a disabled person to regain significant ambulatory functional capacity needed for an independent and fruitful life, an optimal rehabilitation programme should consist of and individually tailored combination of the following:68,141 (1) appropriate medication; (2) a comprehensive programme of physical therapy including a variety of exercises such as walking on a TM, TM with BWS, open field walking (climbing/descending slopes and stairs); (3) whole body exercise such as aerobics, strength and balance training, yoga or dancing; (4) assistive technology (e.g. robotic and haptic devices); (5) occupational therapy and (6) preventive measures. Crucially, the order of these components will differ according to severity of condition, specific nature of gait-related symptoms, the type of condition (e.g. acquired vs neurodegenerative) and expectations of patients and therapists. Secondary problems may arise from age-related comorbidities such as degenerative musculoskeletal diseases (e.g. osteoarthritis, osteoporosis), cardio-vascular dysfunction (coronary heart disease, hypertension) and respiratory conditions that limit exercise capacity (chronic obstructive pulmonary disease) and not least cognitive and social skills. The condition of sensory functioning is very important.
A good ambulation requires appropriate visual, auditory, tactile and vibrational, as well as proprioceptive appropriate input. Related disabilities lead to a markedly decreased quality of life (QoL) and lack of independence, increasing the personal and social costs for especially, but not only, elderly persons. There is an urgent need to improve acquired loss of function and ameliorate the progressive loss of function due to several types of neurological conditions.
There are several neurological conditions that may benefit from use of a modular integrative gait rehabilitation system. We have focused on four major conditions that have significant worldwide incidence and associated socio-economic costs to serve as examples, stroke, TBI, PD and MS, all of which can involve symptoms of gait disturbance.
An ideal system for ambulation rehabilitation should be compact, modular, flexible, versatile, easy to use, easy on and off, friendly to both categories of users (physical therapist and persons with ambulation-related disabilities) through the adequate interfaces. It should be a well-sensorized high usability tool, able to provide in the same time whole person training, assistance (adapted to the user’s limitations and to the objective of the training programme), challenge, constraint, drive and support, a precise and real-time real act diagnosis, evaluation and assessment tool and a valuable real-time persuasive, comprehensible and comprehensive biofeedback. 142 The system must be ‘self-contained’ and not require special arrangements of the facility in which it is installed and has to provide complex therapy programmes, based on patient’s voluntary control at free choice as well as predefined tasks.
In Table 5, the design complexity of ambulation rehabilitation technology is scaled to symptom severity, and Table 6 shows design complexity required in some specific conditions generating gait and ambulation disabilities.
Scaling design complexity with symptom severity for different gait disturbances.

IMUs: inertial motion sensing units; FES: Functional Electrical Stimulation; EEG: electroencephalography; EMG: electromyographic bursts.
Scaling design complexity with exemplary deficits in central neurological conditions.

IMUs: inertial motion sensing units; FES: Functional Electrical Stimulation; EEG: electroencephalography; EMG: electromyographic bursts; PD: Parkinson’s disease; MS: multiple sclerosis; TBI: traumatic brain injury.
The highlighted gait performance characteristics (cells) may benefit most from the ideal system in an ambulation environment. Symptom Scale is ‘Functional Ambulation Category’ (FAC; zero is no ambulation at all and five is healthy normal; it is widely used clinically and is quite simple).
The basic mode of the system may be upgraded by adding inertial motion sensing units (IMU) and coordinated FES with or without lower limb and trunk orthoses.
Electromyography has been demonstrated to yield deep insights into muscle synergies, co-contraction and motor adaptation. 143 Likewise, wearable IMU networks have been demonstrated to provide real-time information about the orientation and position of body segments 144 as well as joint angles 145 and gait phases. 146
On the one hand, this enables ambulatory gait analysis and objective assessment of the rehabilitation outcome. On the other hand, the real-time motion information has been used successfully for feedback control of leg orthoses 147 or neuromuscular stimulation (NMS). 148
Significant improvements in rehabilitation outcome have been obtained by combining BWS with NMS 149 and it has been demonstrated that learning control can be used to adjust the stimulation to the situation-dependent needs of an individual patient. 150
Therefore, an ideal system should incorporate these key technologies and exploit the aforementioned benefits for the sake of an improved gait rehabilitation.
In Table 6, the design complexity is scaled to examples of clinical conditions/severity. An ideal system for gait and ambulation rehabilitation should also provide real-time feedback to the user regarding his performance (qualitative and quantitative biofeedback opportunities 139 ), as well as gait analysis opportunities (to assess the efficiency of using a certain technology for gait rehabilitation in a specific condition). 151
Table 7 presents the most important differences between the classical approach regarding gait rehabilitation interventions and the new approach, that of integrative whole person training for gait and ambulation rehabilitation using an ideal technology for gait rehabilitation.
Classical versus new methodological approach in gait rehabilitation.

ADL: activities of daily living.
Conclusion
The ideal outcome of a rehabilitation programme is for the patient to achieve the highest level of functional independence in given situation. This goal requires intensive and extensive (in terms of variability and time span) training in one’s most familiar life – like environmental conditions and challenges. Inpatient rehabilitation programmes must be followed by rehabilitation and reintegration in one’s community. This requires sensory motor training and cognitive training, combined, in multisensory stimulation environments. Training in real-life tasks is needed to relearn to perform real-life activities. Boosting motivation, self-esteem and self-confidence is essential for compliance to ambulation rehabilitation, empowering the whole rehabilitation multiprofessional and multidisciplinary team, in which the patient must be the active central element.
Advanced technology is a must for this new approach in rehabilitation medicine, allowing and sustaining the process of regaining functional independence and activity – participation skills. Advanced technology for gait and ambulation rehabilitation may empower us to better understand and make use of the substrate and the subtle mechanisms underlying relational functions of human being and the means to improve them when needed.
Our aim is not to achieve the perfect movement, but the perfect harmony of the person with disability and his own life, in his own terms of QoL and in the best possible functional relationship he can get with his own universe.
Future objectives for advanced rehabilitation technology for gait and ambulation rehabilitation should be as follows:
To increase the clinical access, as well as use, utility and the usability of rehabilitation devices and systems.
To develop of three-in-one systems, destined for training, complex biofeedback and research, in order to empower the patient and the team for improving the efficiency of the therapeutic intervention, as well as for rehabilitation research, in the attempt to develop evidence based rehabilitation medical knowledge.
New sensitive and friendly user – system interfaces and development of systems to be used in one’s community.
To increase the capacity of personalizing and real-time tailoring the training and safety parameters.
To increase the addressability of gait and ambulation rehabilitation systems, in order to cover complex impairments and gait-gait related disabilities generated by diverse pathology.
Designing and developing advanced rehabilitation technology requires sustained and intensive interdisciplinary team work, involving physical medicine and rehabilitation physicians, physical therapists, occupational therapists and mechatronic engineers, specialists in electronics and automation, as well as psychologists, biologists, architects and, last but not least, the active involvement of the persons experiencing disabilities.
Footnotes
Handling Editor: Liyuan Sheng
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.