
Abstract
Introduction
The combination of virtual reality (VR) with an omnidirectional walking platform (ODWP) may have potential in rehabilitation settings. However, its use, acceptance, safety, and effectiveness are unclear. This preliminary study aims to understand the feasibility, safety, and user experience (including investigating the onset of cybersickness) while walking on the ODWP with fully immersive VR.
Methods
Participants engaged with eight immersive VR walking scenarios. The scenarios were created using 360-degree videos and were programmed to run with the ODWP. Safety modifications for the ODWP were made, with the addition of parallel bars. Quantitative feedback on the perceived safety and acceptance of using VR with an ODWP for rehabilitation was collected. Cybersickness was evaluated using the Simulation Symptoms Questionnaire (SSQ).
Results
Thirty-five participants (n = 8 physiotherapists, n = 27 healthy adults) were recruited for this study. The mean perceived safety score was 78.9/100 and acceptance was 64.5/100. Seventy-one percent of participants experienced mild to moderate symptoms of cybersickness as reported on the SSQ. The SSQ scores were not correlated to participant age or simulation exposure time.
Conclusion
VR while using ODWP has the potential for rehabilitation, however, more consideration is needed to address acceptance and cybersickness.
Keywords
Introduction
The advancement of virtual reality (VR) technology is becoming increasingly accessible, applicable, and utilized in rehabilitation.1,2 VR has shown therapeutic potential in the rehabilitation of patients with chronic conditions such as stroke, Parkinson’s disease,3–5 low back pain 6 and in patients with mild cognitive impairment. 7 Immersive VR technology typically involves the use of VR goggles and a movement controller such as a keyboard or directional pad. This allows users to maneuver in a VR world creating an immersive roaming experience.
Motion tracking technology can enhance the immersive VR experience. Users can walk freely around an enclosed space which is then captured and replicated within the VR environment. However, successfully navigating requires an obstacle-free space and, without visual input from the actual physical world, good body awareness of the user. This makes the translation of immersive VR into rehabilitation challenging. Treadmill-based VR walking has been proposed as a solution to overcome the need for obstacle-free space and has been investigated in patients with chronic stroke. 8 However, a major limitation of the treadmill is the inability of the user to easily regulate the walking speed and change in walking direction.
Omnidirectional walking platforms (ODWPs) provide a possible solution to facilitate the use of immersive VR in rehabilitation by allowing the user to walk “on the spot” and turn freely whilst exploring the VR environment. Current ODWPs are primarily designed for gamers to walk, run and crouch down in a simulated VR game environment. Users wear a waist support harness system that detects body movements whilst also providing safety and support. The majority of ODWPs are designed with a concave platform surface to allow users to “walk” by sliding their feet over the surface using special footwear to reduce friction. Therefore, users can explore the VR environment through “walking” without the constraint of physical space.
A recent study on the use of ODWP with VR on physical activities and enjoyment reported positive health benefits with physical training in healthy individuals. 9 However, limited studies exist investigating the use of the OWDP with VR for rehabilitation purposes. Physical walking within the VR environment for patients may pose a potential fall risk due to the removal of normal visual input by the VR headset. The use of ODWP with fully immersive VR creates a vection perception whereby the illusionary sense of moving through space is purely dependent on the visual stimulation provided by the system. Therefore, patients would not have the direct visualization of their surroundings required for balance and proprioception. To minimizes the risk of falls, there are inbuilt waist support harness features of ODWPs (for example, the Katwalk mini - https://www.kat-vr.com) to protect the users whilst exploring the VR environment. This safety feature can be utilized in the rehabilitation of patients with poor balance when exploring the VR environment. In addition to the general benefits of physical walking while immersed within the VR environment,8,10 the ODWP may create a more authentic experience and improve the physical functional training of the patients.
Although the ODWP may enhance the experience of the user, the stimulation of the vestibulo-occular system may potentially result in symptoms of cybersickness.11–13 The term cybersickness is a sub-type of motion sickness associated with exposure to an immersive VR environment. Although the underlying cause of these motion sickness may differ, their clinical symptoms of nausea, dizziness and cold sweating often are similar. 13 The unpleasant symptoms associated with the use of head-mounted VR devices has been reported to be influenced by the type of locomotion in the VR environment, the quality of the visual images, the preference of the user and the duration of exposure.14–16 It is unknown how cybersickness could affect users using the ODWP with VR as the vection perception may be different compared to the conventional controller-based locomotion VR or the treadmill-based VR system.
The purpose of this study was to understand the potential of ODWP with VR technology as a rehabilitation tool. The study investigated the feasibility, safety and user experience of physical walking on the ODWP with fully immersive VR, including investigating the onset of cybersickness. This would help VR technologists improve the safety of similar systems and to allow better consideration when designing it as a rehabilitation device in the future.
Methods
A cross-sectional study, using quantitative outcome measures, investigated the potential VR while using an ODWP as a rehabilitation tool. This study was approved by the Singapore Institute of Technology, Institutional Review Board (2019032).
A total of 35 healthy participants were recruited in the study through convenience sampling. The participants included 8 physiotherapists from a local hospital in Singapore, the rest of the 27 healthy adults (7 elderly and 20 younger adults) were recruited from the local community. All participants gave written informed consent before the study.
The Katwalk mini and the HTC Vive Pro headset were used to create an immersive VR experience for the participants. A software interface was written using the software development kit provided with the ODWP to generate the VR environment content using 360-degrees videos. The videos were pre-recorded using a GoPro Fusion 360 camera and integrated into the Katwalk mini and HTC Vive Pro headset. The 360-degree video playback speed was programmed to run in tandem with the walking speed of the participants. As the videos only portrayed a single path of movement, a directional arrow was overlaid onto the video to guide the participants in the VR environment to turn on the ODWP accordingly to the direction the camera is moving [Figure 1(a)]. Customized parallel supporting bars were added to the existing frame of the ODWP to enhance safety. Participants were able to hold onto the parallel bars as needed for support during the study [Figure 1(b)]. (a) Screenshot of actual walking scene with directional arrow in VR. (b) Kat-walk mini with added parallel bar.
At the start of the study, participants completed a set of questionnaires to find out their perception and experience with VR. They were given time to familiarize themselves with the operation of the ODWP before the start of the study. Participants were asked to complete 8 different walking scenes, and the total duration of usage was set to a maximum limit of 30 minutes. At the end of each scene, the participants were asked to report any signs of cybersickness. On average, the participants rested 2 minutes between scenes, a longer rest period was given as requested by the participants, and termination of the study was possible upon request or with the completion of all 8 scenes.
At the end of the study, participants completed questionnaires providing feedback on their perceived safety when using the system, their perceived acceptance of the system for use in rehabilitation, and measurement of cybersickness using the Simulation Sickness Questionnaire (SSQ). 17 The scoring of safety and acceptance was rated on a scale of 0 to 100 with 100 being the highest possible score for both safety and acceptance. In addition, the participants completed a written questionnaire to explore their experience with the ODWP. The SSQ scores were calculated based on different subscales of symptoms (N = nausea, O = oculomotor disturbance, and D = disorientation). A rating of 0 to 3 was given to reflect the severity of the symptoms for none, slight, moderate, and severe for each subscale respectively. The scores of the 3 subscales and total score were calculated using the formula proposed by Bimberg et al. 2020 (N = [total rating for nausea subscale] × 9.54, O = [total rating for oculomotor subscale] × 7.58, D = [total rating for disorientation subscale] × 13.92, total score = ([N] + [O] + [D]) × 3.74) with a higher score indicative of the higher degree of symptoms. 18
Statistical analysis
Descriptive statistics were used to report questionnaire findings for the acceptance and safety of ODWP with VR for rehabilitation purposes. Correlation analysis (Pearson’s R) was used to investigate potential factors associated with SSQ score (age and the total exposure time on the ODWP with VR system). A correlation coefficient of 0.9 to 0.7 was set as a strong correlation, 0.6 to 0.4 as a moderate correlation, and 0.3 to 0.1 as a weak correlation. 19
Results
Demographic information of participants recruited.

Safety and feasibility of using ODWP with VR in rehabilitation
Perceived safety and likelihood of using the system.
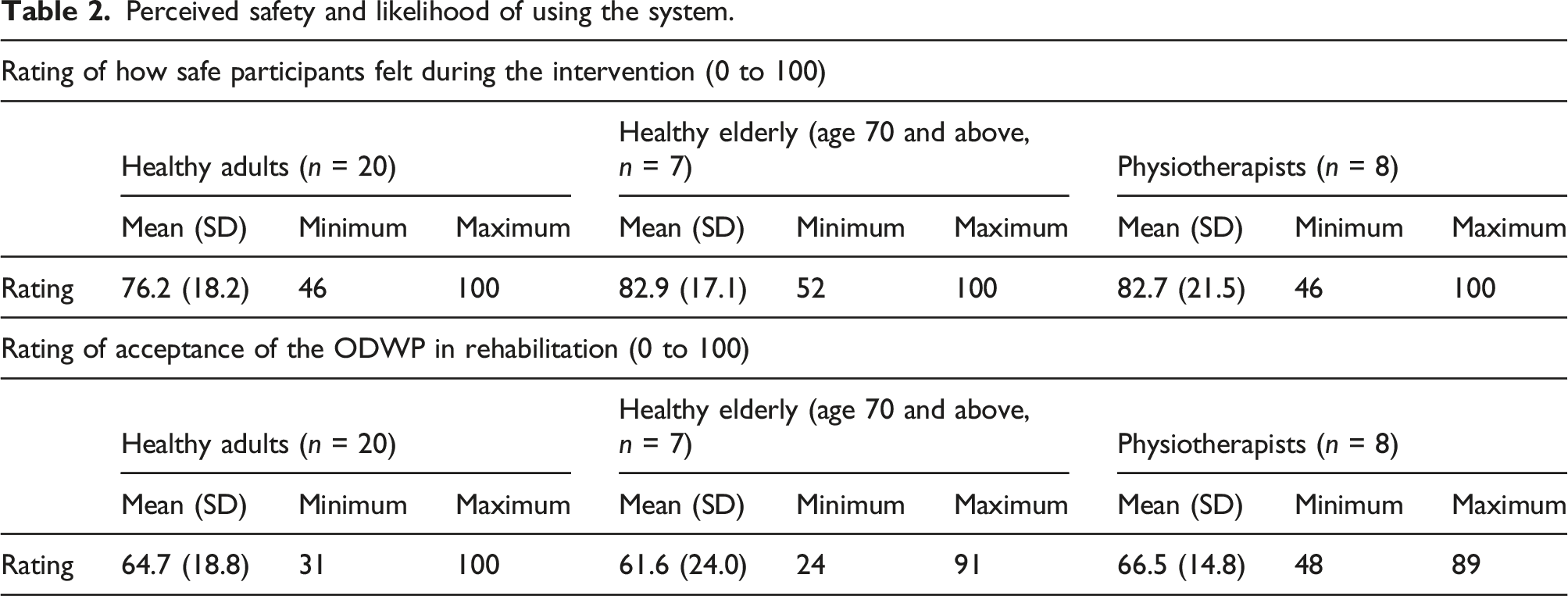
Qualitative feedback from participants revealed that the most common reason for feeling unsafe was the smooth characteristic of the concave-shaped platform. Ten out of 35 participants (28.5%) reported slipping or losing their balance while walking and changing direction on the ODWP. Other feedback was the onset of cybersickness due to the mismatch of VR imagery with normal walking speed. Two participants indicated that the addition of the parallel bar was an important feature in reducing the risk of slipping and improving their sense of safety on the ODWP.
The majority of participants were convinced that this technology looked interesting (“it’s the future, really cool”) and may improve motivation and adherence to therapy (“it’s more entertaining and adds an extra touch to the conventional therapy”). Participants also stated that this technology could simulate realistic environments that were not possible within hospitals and may enhance rehabilitation outcomes (“provides an alternative environment for the patient to interact with… can be adjusted to simulate ideal conditions for different patients”). However, 9 participants (all healthy adults) expressed they would not choose this technology as a rehabilitation approach if given a choice. The reasons were due to the onset of side effects (“discomfort – felt nauseous after session”) and the unnatural walking pattern (“I’m not walking normally, and I can’t see my feet to correct it”) on the ODWP. All elderly participants in this study indicated that they would choose the technology if it was provided in rehabilitation.
Physiotherapists’ perception of ODWP and VR
Of the eight physiotherapists, one felt that the ODWP with VR could pose some challenges for implementation in a rehabilitation setting due to the possible implication of cybersickness-related side effects. The remaining seven physiotherapists expressed that the ODWP with VR could be incorporated into rehabilitation to enhance current rehabilitation outcomes due to the features of it being interactive and being able to simulate environments (“an interactive environment in addition to set therapy goals could simulate the minds of the elderly and provide additional benefits beyond physical therapy benefits”). Physiotherapists suggested that patients with frailty, dementia, vestibular conditions, and neurological conditions such as stroke could benefit from using the ODWP with VR. Physiotherapists also expressed that the ODWP with VR could potentially be used in balance, endurance and strength training for the patients. Additionally, it was raised that ODWP with VR could potentially aid in the community integration of patients (“a person who has rehabilitated to his/her full potential, can function independently and is attempting to reintegrate into community after long periods of hospital stay”).
However, when given the option to offer ODWP with VR as part of the rehabilitation therapy, two physiotherapists expressed that they would not choose to offer the ODWP with VR over conventional therapy. Reasons given were due to time constraints during rehabilitation and the possible onset of cybersickness. Other points raised included potential poor acceptance from older patients (“elderly may not like the technology as it looks difficult to operate”), and the cost of machine installation and maintenance over time. Physiotherapists were also concerned about the unnatural walking pattern on the ODWP which might not translate to gait improvement (“walking is unnatural, lack of normal gait/functional movements for gait training”).
Cybersickness
Seventy-one per cent (n = 25/35) of participants in the study experienced some form of cybersickness throughout the study. Two participants (1 healthy adult and 1 physiotherapist) requested for the intervention to stop due to the development of unpleasant cybersickness. The results of Pearson’s correlation coefficient analysis showed no significant association between age and exposure time to SSQ scores in our study. The results of the SSQ subscale from the 25 participants with cybersickness were, Nausea = 24.42 (20.1), Oculomotor = 19.4 (15.5) and Disorientation = 37.86 (40.5), total score = 305.51 (261.42).
Discussion
This study investigated the feasibility, safety and user experience of physical walking on an ODWP with VR. The majority of participants in our study provided positive feedback about the use of ODWPs with VR in rehabilitation despite most experiencing cybersickness to varying levels. Although we had a small sample size, both physiotherapists and healthy adults tended to agree that ODWPs with VR was interesting and has the potential to enhance rehabilitation outcomes.
There was no correlation of cybersickness with age or exposure time for participants in our study. This contrasts with other studies that have found longer exposure time and age of participants does influence the extent of cybersickness. 15 This is possibly because we limited the cumulated exposure time using the ODWP with VR to a maximum of 30 minutes and broke this time up into smaller sessions rather than a single continuous session of exposure. The segmented exposure allowed our participants time to recover and reduced the cumulated effects of continuous exposure.
A total of 25 participants (71%) experienced some level of cybersickness in this study based on their SSQ scores. This is similar to previous studies investigating the use of VR where more than half of participants reported symptoms of cybersickness with fully immersive VR.20,21 In a fully immersive VR environment, the vection perception is generally enhanced. Although it was not fully understood why some individuals and not others experienced cybersickness, the sensory conflict between vestibular, visual, and somatosensory input could be a likely cause based on the sensory conflict theory.12,22 This mismatch between the visual and vestibular senses and what was expected from previous experience provided the basis to explain the sensory conflict theory. Under the sensory conflict theory, users may perceive they are moving or turning at a speed which does not match the actual motion of their physical body while moving on the ODWP with VR. Another possible explanation of cybersickness could be due to the exposure of long-lasting postural instability from frequent changes in environmental dynamic similar to travelling on a ship. 23 Notably, our participants in the study were all healthy individuals without balance or sensory deficit. It is currently unknown if patients with conditions that affect vestibular function would make them more susceptible to VR related cybersickness. The issue of cybersickness with the use of VR remains a long-standing problem despite the development of VR technology. 24
Cybersickness is influenced by multiple factors such as age, gender, stress, anxiety and types of VR content used.25–30 Factors such as the quality of the images, display resolution (rendering mode) of the VR headsets and display lag from the VR headsets to the actual head movement have shown to affect cybersickness.31,32 On the ODWP, the users feel themselves walking in the VR environment without visualization of their body (feet and hands). Coupled with the factors influencing cybersickness and balance related concerns while on the ODWP, the action of walking may add another layer of complexity to the vection effect and cybersickness. This may be more so when there is a mismatch between the expected walking speed and the movement within the VR environment. 33 Further research is needed to understand the cause and effects of VR induced cybersickness before we can fully mitigate the problem.
It is possible the physiotherapists who were unwilling to use the ODWP with VR were concerned about the possibility of cybersickness for the patient population compared to traditional therapy. Further studies are needed to investigate this effect in patient populations to determine whether it is safe to implement VR related technology compared to traditional interventions. In doing so, a pre-exposure assessment of symptoms similar to cybersickness should be considered as medication and underlying conditions may influence the outcome of cybersickness evaluation. 34 Future research could compare benefits and onset of cybersickness between treadmill and ODWP walking with VR.
Current ODWPs available in the market are mainly designed for able bodied gamers. To provide an additional sense of security and safety for patients to use the ODWP with VR, we included upper body support with handrails. The additional parallel bars likely increased participants’ confidence in walking when VR replaced the visual input from the physical environment. While the risk of falling was reduced with the in-built waist support, the additional parallel bars provided a safer transit off and onto the ODWP. This important safety consideration has not been factored into the design of most ODWP as it is primarily designed for able bodied gamers. A greater need for safety and balance support features are needed in the design of ODWP for use in rehabilitation as patients may have underlying conditions which would challenge their balance and mobility on uneven surfaces.
In this current study, walking using the ODWP was fundamentally different from walking on the actual ground or a normal treadmill When walking on an ODWP, the users must actively extend their hip to slide their feet backwards to “walk” and maintain their position on the same spot. This is different from a normal gait whereby a step is taken forward in concordance to the shift in the body center of gravity. Therefore, greater hip extensor muscle activation and control are required while “walking” on the ODWP. The difference in ODWP gait may not directly translate to improvement in actual gait control and balance based on the differences in movement kinematics. The use of ODWPs, with or without the use of VR for gait retraining might be challenging for patients with neurological conditions involving the lower limb. More research is needed to determine if there may be small translation benefits of walking on the ODWP with improvements in actual gait. However, the increased muscle effort of walking on the ODWP may be beneficial as a form of lower limb exercises for some patients. Compared to a treadmill, ODWP walking allows users to move at their own pace. The self-paced movement may offer new rehabilitation opportunities for rehabilitation of patients with Parkinson’s disease or mild stroke to have better control over their speed of walking and movement initiation which would be an advantage over the conventional treadmill systems.
This study provides preliminary data on the potential of ODWP with VR for rehabilitation. We recognize that the small sample size and inclusion of elderly participants and physiotherapist participants may not represent the views and perceptions of all potential rehabilitation providers and users. Although we identified potential issues with using ODWPs with VR for rehabilitation, we believe that there is still potential for its use in rehabilitation. However, further development and research is required. Given the increasing interest in the development of innovative rehabilitation technology, ODWPs with immersive VR can likely be improved and customized for rehabilitation in the future.
Footnotes
Acknowledgements
Special thanks to all the physiotherapists from Ng Teng Fong General Hospital for their participation and contribution to the study. This study was made possible by the ignition grant from Singapore Institute of technology.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Singapore Institute of Technology (Ignition Grant / R-MOE-E103-E005).