
Abstract
The use of robotic platforms for neuro-rehabilitation may boost the neural plasticity process and improve motor recovery in patients with upper limb mobility impairment as a consequence of an acquired brain injury. A robotic platform for this aim must provide ergonomic and friendly design, human safety, intensive task-oriented therapy, and assistive forces. Its implementation is a complex process that involves new developments in the mechanical, electronics, and control fields. This article presents the end-effector rehabilitation robot, a 2-degree-of-freedom planar robotic platform for upper limb rehabilitation in patients with neuromotor disability after a stroke. We describe the ergonomic mechanical design, the system control architecture, and the rehabilitation therapies that can be performed. The impedance-based haptic controller implemented in end-effector rehabilitation robot uses the information provided by a JR3 force sensor to achieve an efficient and friendly patient–robot interaction. Two task-oriented therapy modes have been implemented based on the “assist as needed” paradigm. As a result, the amount of support provided by the robot adapts to the patient’s requirements, maintaining the therapy as intensive as possible without compromising the patient’s health and safety and promoting engagement.
Keywords
Introduction
Acquired brain injury (ABI) is an alteration of the brain structures after the birth that is not the result of a congenital disorder of development of progressive brain damage. 1 This condition can be temporary or permanent, and it is the origin of a disability in the functionality and the psycho-social adjustment that directly influences the quality of life of those affected. 2 It produces an interruption in the life development in psychological, physical, and social aspects, 3 and it is one of the most frequent causes of disability and death in the world. 4 The World Health Organization estimates that almost half of the world’s population could suffer an injury of ABI, and the National Center for Injury Prevention and Control estimates that around 2% of the US population suffers from a disability as a result of an ABI as a consequence of a trauma. It is estimated that in the United States 1.7 million people a year suffer a brain injury by trauma resulting in 275,000 hospitalizations and 52,000 deaths. 5 The most common causes of ABI are head trauma, brain stroke, brain tumors, brain anoxia, and other brain diseases.6–8
Robot-aided arm rehabilitation consists of selected therapies to be performed by the patient to provoke motor plasticity, and therefore improve motor recovery. 9 However, there is not a solid scientific understanding of how this goal can be successfully achieved. 10 Control strategies for rehabilitation robots have been designed on an “ad hoc” basis, usually based on some concepts from the rehabilitation, neuroscience, and motor learning literature.
Several published studies11–14 demonstrate the effectiveness of robotic-assisted therapy in patients with ABI. Almost every study shows that patients receiving assistive robotic training do not show better chances of improving their upper limb movement in most daily living activities. Nevertheless, they show a significant growth in motor function. A recent review 15 concludes that patients receiving electromechanical and robot-assisted arm training after stroke are more likely to improve their generic daily living activities. Paretic arm function may also improve, but not arm muscle strength. Assistive therapies appear to give modest additional benefit in addition to usual care. 16
The use of robots for rehabilitation purposes with passive movements is insufficient to alter motor recovery, 17 and the patients must be actively engaged and encouraged to move in order to induce neural plasticity and promote recovery.18,19 Rehabilitation robots have proved to be an excellent tool for administering physical therapy to patients suffering neurological injuries and diseases. The “assist as needed” paradigm promotes patient engagement by providing assistance only when it is useful, and by detecting the patient’s attempted movements. On the other side, the need for direct interaction with the patient poses some special requirements in its design. An important property in this respect is backdrivability, a property that increases patient safety, indicating that the patient is able to move the device, even when it is in a passive state.
There are many examples of robotic rehabilitation platforms.20–25 A review of robotic systems for upper limb rehabilitation of stroke patients from a historical perspective, and with a focus on modern methods to encourage patient engagement in therapy, is presented in Blank et al. 26 The article of Maciejasz et al. 27 provides another recent and comprehensive review of robotic devices for upper limb rehabilitation. End-effector devices can be classified into two broad categories. On one hand, those based on an industrial robot adapted for its use as a rehabilitation tool and, on the other, those specifically designed for this purpose. The main drawback of the first type28,29 is that, being essentially position-controlled devices, it is very difficult to obtain a low impedance behavior. Even using active force feedback, the degree of backdrivability required for proper behavior in response to patient actions is not achieved. The second category includes two classes of systems: 30
Class I devices,31,32 where system backdrivability is achieved by mechanical solutions aimed at minimizing the perceived inertia and usually implementing haptic techniques. They have good mechanical properties (low friction and inertia values) and, in general, a high cost.
Class II devices 33 have a simpler mechanical structure, with less efficient values of their mechanical parameters, but with a much lower cost. In this case, the control strategy used is an essential element for the proper performance of the device.
End-effector rehabilitation robot (E2Rebot) is a class II device, whose current version is the result of the evolution of a previous design based on the requirements of a clinical trial designed to evaluate certain aspects of stroke patients. 34 It is currently being tested in two clinical centers in Spain, in order to test its usefulness as a therapeutic tool in stroke patients. To our understanding, this is, currently, the only Class II device that implements the “assist as needed” paradigm and is undergoing clinical trials.
The main contribution of E2Rebot is a novel approach in implementing the “assist as needed” strategy and obtaining the appropriate values of the assistive force, by applying a control law that allows the apparent dynamics of the manipulator to be modified, rather than its true nonlinear behavior, which is a nonphysically realizable approach. For attaining this goal, the low-level haptic controller applies a dynamic relationship between the mechanical parameters of the robot, the kinematic variables, and the external and internal forces that are applied to the end-effector. As a consequence, an integrated control action is applied instead of separate corrections for each physical variable.
This approach provides great advantages from the point of view of implementing the control schemes developed: it simplifies the programming of control strategies, entails less stringent requirements on the hardware, and therefore allows the development of cost-effective platforms to be addressed. This aspect is of great importance since it allows the dissemination and use of E2Rebot to be enhanced.
From a structural point of view, CBM-Motus 27 is the most similar to our device. Both have a Cartesian kinematic structure with some similarities in the mechanical design, but the control approach is different. CBM-Motus implements a current-based impedance control in order to compensate for friction and enhance control performance in the interaction with the user, avoiding the use of force sensors mounted at the robot end-effector. In our case, the control of E2Rebot is based on the “assist as needed” paradigm and implements a low-level force-based impedance controller in order to support different rehabilitation therapies.
The E2Rebot device represents a remarkable evolution from two previous platforms. The first one was developed over an industrial commercial robot (Staubli RX90). 35 The second one, Softrobot 36 was our own design and has been working since 2013 at the Hospital Beata María Ana de Jesús in Madrid (Spain). The experience acquired during the design and the technical and clinical evaluation of Softrobot has been fundamental for redesigning the E2Rebot platform ergonomics, tuning the impedance-based controller parameters, and redefining the neuro-rehabilitation therapies.
In the remaining sections, we describe in detail the E2Rebot device requirements and its mechanical and electronic structure and components, the impedance-based controller, its integration, and the therapies module. Finally, some conclusions are given.
Description of the E2Rebot system
Requirements
E2Rebot is a cost-effective robotic platform for active assistance in the rehabilitation of patients suffering upper limb impairment as a consequence of ABI. Its architecture includes an impedance-based haptic controller developed according to the “assist as needed” paradigm that adapts the level of assistance of the robot to the patient’s condition during the course of the therapy.
Since the current design is the result of the evolution of two previous platforms, the experience acquired in their development and, above all, the results of previous tests performed with both healthy subjects and patients, allowed us to identify a set of requirements in order to obtain the desired characteristics and behavior.
The following requirements have been considered in the design of the E2Rebot device:
It must allow upper limb rehabilitation in patients who suffered ABI by performing tasks of flexo-extension of the elbow, and abduction–adduction of the glenohumeral joint.
It must be designed to provide a high level of usability and be cost-effective.
It must be intrinsically safe, with a transparent dynamics (backdrivability) and a simple mechanical design providing low inertias.
Its workspace must allow natural movements of the human arm to be performed. The range of motion of a human arm in a planar area is approximately 800 mm × 500 mm. This workspace allows the patient to make a complete shoulder abduction, and a full elbow extension, whenever the medial plane is not exceeded during the abduction–flexion.
It must include a six-dimensional (6D) force/torque sensor located on the end-effector to measure the dynamics of the interaction between the patient and the robot.
It must implement a control strategy using both position and force measurements. Considering these measurements as independent is not a valid option, given the interactive nature of rehabilitation robots. Impedance-based control provides a convenient framework for designing the robot control algorithms.
It must include safety by hardware, because it interacts with human users.
Its software must include one or more multimedia interfaces for virtual environments and data analysis.
Its software must include a relational database of information about patient, therapy, kinematic (position and velocity), and dynamic (forces) variables for further analysis.
Overview
The E2Rebot mechanical structure is based on two Cartesian XY-axes. The workspace where the patient performs rehabilitation therapy is a rectangle of 975 mm × 600 mm. The robot is equipped with a 90M40 analog-output JR3 6 axis force/torque sensor that measures the force exerted by the patient on the robot end-effector during the rehabilitation therapy. The E2Rebot device is shown in Figure 1.

Two different views of the E2Rebot platform.
One of the main requirements of this design was the intrinsic security by means of the backdrivability of the actuator/gear couple. Two high-performance EC 90 flat DC Maxon brushless motors were selected to move the end-effector robot in the X- and Y-directions (Figure 2).
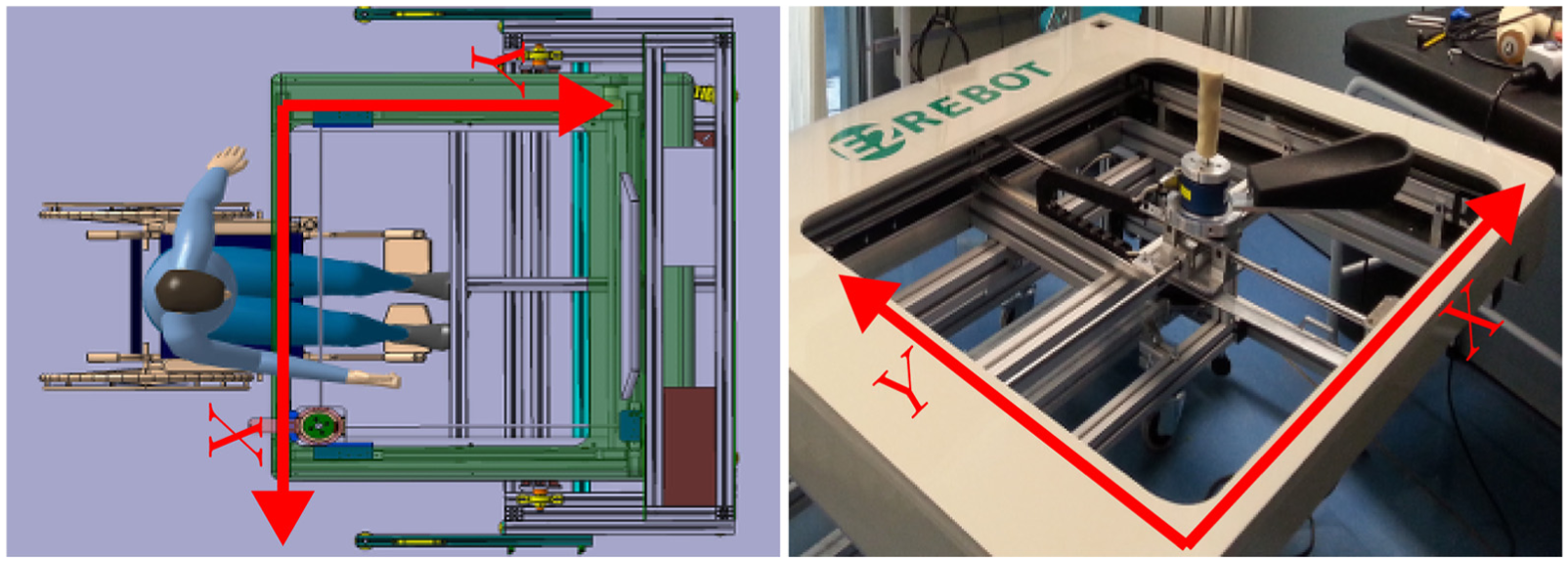
XY-axes of the E2Rebot workspace.
Our first option was to use non-gearbox motors to ensure the mechanical system reversibility, but due to the friction of the linear axes, it was necessary to place gearboxes to increase the effective motor torque. A 4.3:1 gearbox transmission was selected to obtain a good weight/torque ratio. The low ratio of the gearboxes is very useful, because it produces a large output torque, and also contributes to cancel mechanical nonlinearities such as cogging torque, due to the permanent magnets on the brushless motor, and surface friction discontinuities.
The control software of E2Rebot is modular and is organized in three levels: the high level runs on an external personal computer (PC), the intermediate level is implemented in a National Instruments “CompactRIO” cRIO-9076 controller, while the low level runs on two ESCON 50/5 motor control units (MCUs) driving the Cartesian XY-axes of the robot.
The safety functions are implemented by hardware: there are four limit switches that cut the motor driving currents when the robot is getting close to the mechanical hard stops on every rail. Additionally, the safety system prevents hardware degeneration over time by avoiding possible impacts.
The E2Rebot device has an electrical system that adjusts the height of the robot platform in the range of 750–1200 mm, according to the patient’s needs. Thus, the patient can receive rehabilitation therapy either standing or in a wheelchair. The configuration data are stored for each patient for future therapy sessions. Moreover, it has an additional rotation axis to ease transport and mobility. This axis allows the work area to be bent so that the robot fits through spaces that have a width of 800 mm during transport (see Figure 3).

Different adjustments of the E2Rebot device. From left to right, configuration for wheelchair therapy, configuration for standing therapy on patients of different height, and configuration for transportation.
Kinematics
The E2Rebot device, from the mechanical point of view, is a Cartesian gantry robot with two linear X- and Y-axes, which intrinsically has the following features:
A simple design that makes the robot’s direct and inverse kinematics straightforward to compute, therefore reducing computational costs.
A quasi-isotropic inertia tensor is achieved because of the similar mechanics on both axes.
Forces due to gravity are structurally compensated, so there is no need to include a gravity compensation model.
The kinematic structure of E2Rebot consists of two prismatic joints. The first joint moves the X-axis (range: 0–975 mm) and the second moves Y-axis (range: 0–600 mm).
These two joints are connected to the end-effector, where a JR3 force/torque sensor is located. This kinematic arrangement ensures that the end-effector has only translational degrees of freedom (DOFs) and maintains a fixed orientation in space during motion. This kinematics structure has been selected because it offers the patient a work area suitable to the mobility needs of the human arm, and allows therapies of flexo-extension of the elbow, and abduction–adduction of the glenohumeral joint to be performed.
The E2Rebot device also includes an anti-spasticity orthosis (see Figure 4). Spasticity is defined as an increase in muscle tone due to hyperexcitability of the stretch reflex and is characterized by a velocity-dependent increase in tonic stretch reflexes.37,38 It is associated to some very common neurological disorders such as multiple sclerosis, brain stroke, cerebral palsy, and other spinal cord and brain injuries.

Anti-spasticity orthosis of the E2Rebot platform.
The anti-spasticity orthosis allows the spastic limb to be maintained in a more normal position. The interface also has an anti-acoustic high-density foam which serves as a damper, as well as a mechanical noise filter.
Control system
The interactive nature of rehabilitation robots requires the use of control strategy which includes simultaneous position and force control. Impedance-based control, originally proposed by Hogan, 39 provides an appropriate framework for the design of control algorithms for applications involving human–robot interaction. Impedance-based control is now widely used for controlling robots where force or contact interaction is expected to be handled.
The main goal of the impedance-based haptic controller is to implement a control law enabling the apparent dynamics of the manipulator to be modified, rather than its true nonlinear behavior, which is a non-physically realizable approach. The haptic controller uses a dynamic relationship that relates the manipulator variables, the kinematic variables, and the forces acting on the end-effector, instead of controlling these variables as if they were independent.
The impedance control methodology and control law equations we have implemented in the E2Rebot control system are described in detail in Rodríguez-Guerrero. 40
The control system of the E2Rebot device has a hierarchical modular structure organized in three levels (see Figure 5). The variables and parameters of the E2Rebot control system are as follows:
Input variables of the control system
Controlled variables
Parameters of the impedance-based haptic controller K (spring-capacitive): Describes the level of assistance given to the patient. In active-assistive mode, K is a variable that is computed online by a function that depends on time and on the distance between B (damping-resistive): Describes the resistance of the system to velocity and the energy dissipation. M (mass-inductive): Describes the resistance of the system to acceleration and characterizes the kinetic energy stored in the system.
Motor control parameters

The three levels of the E2Rebot control software.
These variables and control parameters are organized in the three levels of the hierarchical modular control system. The function and implementation of each level are explained as follows:
Level 1: high level—This level is implemented by software coded in C# language, and runs on a PC. It provides the following functions: Virtual rehabilitation therapies are to be performed by the patient. The Microsoft XNA framework of Visual Studio 2010 is used to implement the visual representation of these therapies. Mode selector block allows two modes of the neuromotor rehabilitation therapy: passive-guided and active-assistive modes to be selected. Human–machine interface to select the predefined therapies and change their settings. Data storage: During the course of the rehabilitation therapy, the following data are stored in an internal database: time instant of the therapy, position Online calculation of the K parameter provides the level of assistance to be given to the patient during therapy. This information is sent to the control level 2 using Transmission Control Protocol (TCP) sockets.
Level 2: intermediate level—This level is implemented in the Field-Programmable Gate Array (FPGA) of a “CompactRIO” controller. At this level, the software has been developed in LabVIEW. Communication between levels 1 and 2 is programmed using TCP sockets. The functions included in this level are as follows: Haptic impedance-based controller: This controller uses the input variables K, B, M, To send the force value Computing the torque reference signals for the axes motors and sending them to the control level 3. These are DC 0–5 V analog signals.
Level 3: low level—Both E2Rebot XY-axes use the same configuration: a MAXON MCU ESCON 50/5 encoder, and a direct current brushless motor as actuator. The torque reference signals received by the MCU are analog signals generated by the control system implemented in the FPGA of the CompactRIO system. Using the torque reference signals computed in the level 2, the MCU obtains the control signals for the XY-axes motors.
The control strategy
The control strategy of the E2Rebot is depicted in Figure 6. The mode selector block allows the two modes of neuromotor rehabilitation therapy: passive-guided and active-assistive modes, to be selected. Passive-guided

Block diagram of the E2Rebot control system.
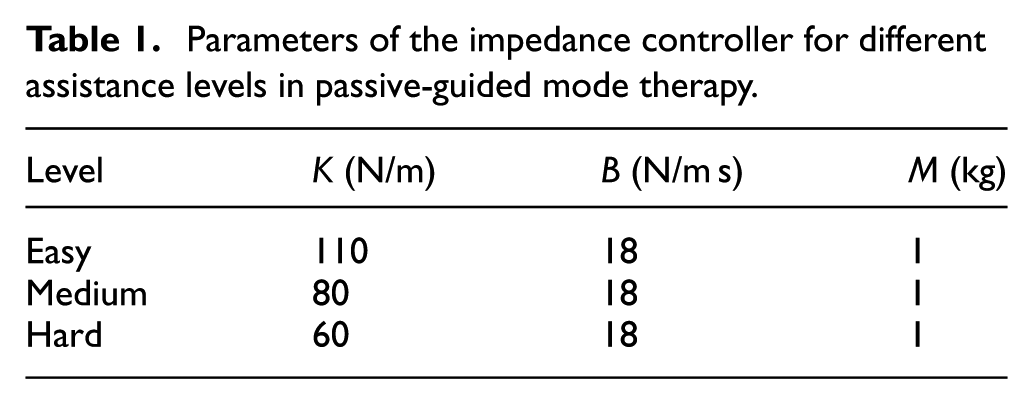
Parameters of the impedance controller for different assistance levels in passive-guided mode therapy.
The impedance-based haptic controller reduces the nonlinear effects in the axes due to stiction and viscous friction. Also, a feedforward compensation was implemented to improve the tracking performance by increasing the gain
A major challenge regarding the design and implementation of the impedance-based controller was choosing an appropriate range for the values of the stiffness K and damping B coefficients. High stiffness values produce low damping ratios and resonant dynamics. Thus, the higher the stiffness, the larger the control force,
The value of the error gain
E2Rebot integration and implementation issues
The synchronization of the information and control strategies of the E2Rebot system was another challenge because of the great complexity of the real-time operation. The control architecture is designed to minimize the effect of uncertainties and noises, such as those caused by network delays in the data flow. Not considering these aspects is usually a source of modeling error that leads to poor performance of the controller. The sampling rate was selected taking into account the nature of the problem and the time response to achieve a smooth and stable behavior. When interacting with humans, the time response of the robot must be slow. Thus, the sampling time was selected to get a smooth trajectory.
The control system of the robot acts as follows. The target point
Virtual rehabilitation therapies
The virtual therapies module provides the target position every 500 µs. The computation of the parameters of the impedance-based controller
The E2Rebot device has been designed to have a high degree of flexibility in performing rehabilitation tasks. This flexibility is obtained by a module of rehabilitation therapies that was designed and programmed taking into account the following requirements:
Intuitive and easy to understand interfaces for patients with auditory and tactile disabilities.
Rehabilitation therapies must be simple, clear, and intuitive, so the therapist does not have to be permanently monitoring the patient while doing the therapy.
Visual and auditory messages that guide, help, and encourage the patient to successfully perform the therapies.
In the motor recovery of patients, it is desirable that the robot only provides assistance when the patient needs it. Most of the virtual scenarios used in rehabilitation with robots include game-based therapies, where the subject has to reach or follow an object moving in a virtual scenario. The patient is constantly moving the arm which is attached to the robot end-effector. Patients suffering from ABI cannot reach or follow the object only by their own effort and need robot assistance. Thus, it is crucial to determine when the robot should begin to assist the patient and how much assistance should be provided. This is the basis of the “assist as needed” paradigm.
The impedance-based haptic controller computes, in real-time, the amount of assistance that should be given to the patient to ensure that the therapy is successfully performed. The developed therapies promote patient engagement by providing only the assistance that is needed by detecting the force exerted to drive the robot end-effector. Consequently, patient’s effort is higher and this results in boosting the neural plasticity process.
Two modes of neuromotor rehabilitation have been developed, that is, passive-guided and active-assistive modes. Both modes are based on a graphical environment in which different games are played as therapeutic tools. The patient interacts with the game using the robot end-effector as if it were a joystick.
Passive-guided mode
Passive-guided mode consists of a series of repetitive rehabilitation therapies, in which the patient is asked to follow a series of trajectories by moving the robot end-effector by hand. The patient is guided by the action of a virtual interface and the impedance-based haptic controller aids task completion. This mode is mainly used at the chronic stage of the therapy, in which patients are highly impaired, and their motor function capabilities are almost null. Passive-guided mode acts mostly like classical therapy, in which the patient is guided by the therapist’s hands to complete a certain task. This mode exploits the fact that task-oriented movements can improve muscle strength and movement coordination in patients with neurological impairments. 42
In the passive-guided mode, the therapist moves the robot end-effector to define the desired trajectory for the patient’s therapy. This trajectory is registered by the CompactRIO controller at a rate of one point every 500 µs and constitutes the desired trajectory for the patient. Then, the therapist is prompted to enter an assistance level. During the therapy, the patient grabs the robot end-effector and tries to track the desired trajectory during a certain time interval for the preselected robot assistance level.
The therapist can select between three assistance levels: easy, medium, and hard. For each level, the
In Rodríguez Guerrero et al.,
36
we presented the results of a study with eight patients suffering traumatic brain injury at the Hospital Beata Maria Ana de Jesús in Madrid (Spain). The analysis of the results obtained in this study allowed us to determine the most appropriate values of the parameters
These values remain constant until the therapy is completed. The parameter values for each assistance level are given in Table 1. The greater the value of K, the robot provides more assistance to the patient during the therapy and therefore, smaller is the error allowed between the actual position
For a desired trajectory with initial point

Mechanical analogy of the impedance-based controller (left) and reactive force field force generated (right).
Next, we present an example of a therapy in passive-guided mode performed by a male patient suffering post-stroke hemiplegia at a chronic stage with upper limb impairments. His stroke occurred more than 6 months before the tests with E2Rebot. Figure 8 shows the desired trajectory (in red color) recorded by the therapist, who selected the “medium” assistance level (see Table 1), and the patient repeated the desired trajectory during a session of 30 min. The measured trajectories performed by the patient are depicted in the same figure in blue color. The

Representation of the desired trajectory (red) and the set of measured trajectories (blue) performed during therapy in passive-guided mode for a patient with right hemiplegia.
Active-assistive mode
This mode offers a task-oriented therapy type, augmented with an “assist as needed” that modulates online the amount of assistive force that the robot provides based on the patient performance. Physical therapists manually implement this technique in clinical rehabilitation on a regular basis for both upper limb training.
In this mode, the patient can freely move a virtual hand in the interface screen and he is expected to catch a virtual mouse that moves away when the virtual hand approaches. The mouse behavior is highly customizable. Three levels of difficulty were implemented, that is, easy, medium, and hard. As the level of difficulty increases, the mouse movements are faster and it is harder to catch it. The therapist should select the appropriate level of difficulty for each patient’s condition.
The therapy is performed as a “catch the mouse” game. Each time that the patient catches the mouse, the game score increases in a certain amount, depending on the patient’s ability and the level of difficulty, and the mouse moves to a new random position to play a new game.
The amount of assistance that the robot provides to the patients is adaptive online, using the information about their movements. A software module located at the PC (control level 1) updates the stiffness and damping coefficients
The algorithm to update the parameters of the impedance-based controller is given in Figure 9. The value of the virtual mass parameter M is constant and is normalized to

Algorithm for computing the parameters of the impedance-based haptic controller in active-assistive mode.
Active-assistive mode regulates online, using the “assist as needed” paradigm, the amount of assistive force,
The patient’s improvement can be analyzed using the force error index while performing the therapy. This index is given as a percentage, that is,
Figure 10 shows the evolution of the force error index for an active-assistive therapy performed by the male patient suffering post-stroke hemiplegia at a chronic stage with upper limb impairment, during 51 sessions (30 min per session). The index evolution for the percentage of the exerted force on the robot is depicted for axes X and Y in blue and red color, respectively. Each index value in the graphic has been obtained by averaging the forces
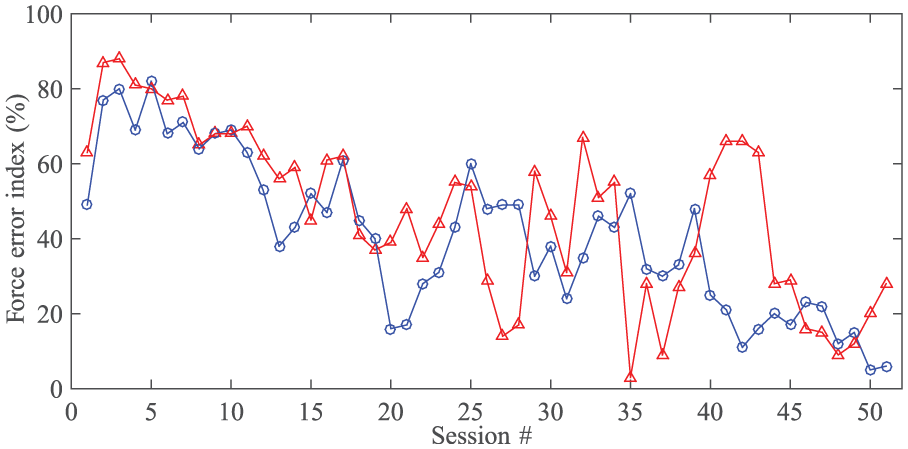
Force error index during active-assistive therapy performed and 51 sessions for a patient with right hemiplegia. Blue color: X-axis, red color: Y-axis.
The therapy always starts at easy level of difficulty. The plot shows that, during the first 22 sessions, the force error index decreases in both axes. This means that the patient is improving and the force exerted on the robot is increasing. At session 22, the therapist changed the level to medium and kept it until session 51. The force error index increases after this change of level. After the patients adapt to the new level of intensity, the force error has more variability, but with a decreasing trend.
Conclusion
In this article, we presented the E2Rebot platform, a new end-effector robot for upper limbs rehabilitation. Our previous robot rehabilitation platform, Softrobot 36 has been working for 2 years at Hospital Beata Maria Ana de Jusús in Madrid. The experience acquired over these 2 years of full-time operation has allowed us to analyze its performance, detect deficiencies, and propose improvements for a new improved design. As a result, we have developed the E2Rebot device that is reported in this article.
The main contribution of E2Rebot is a novel approach in implementing the “assist as needed” strategy to obtain the appropriate values of the assistive force, by applying a control law that modifies the apparent dynamics of the manipulator rather than its nonlinear behavior, which would not be physically realizable. Additional features and improvements are as follows:
A new and improved ergonomic structural design providing a comfortable and easy patient adaptability when performing therapy, either in a standing position or in a wheelchair.
An intrinsically safe design providing transparent dynamics, backdrivability, human safety, and portability.
An improved impedance-based feedback controller with a feedforward loop that deals with highly nonlinear friction without compromising performance and using cost-effective control hardware. The impedance-based haptic control implemented provides a successful and friendly patient–robot interaction by performing smooth trajectories and compensating the patients’ shaking due their spasticity.
A module of active-assistive therapies developed under the “assist as needed.” This means that it provides the patient the required amount of force at every instant of the therapy, by detecting physical activity to drive to the robot.
Key in the development of E2Rebot is the modular architecture of its control system, organized in a hierarchy of three levels. Other key development aspects are as follows: the ergonomy of its mechanical structure, and the sensors and actuators selected and optimized for patient-cooperative control strategies. Although some preliminary successful results have been obtained in patient’s rehabilitation, an extensive program of testing and validation with patients has been defined and is under development.
Finally, we are planning new improvements that include a rotational 1-DOF mechatronic device at the end-effector in order to perform therapies for stimulating motor recovery of paretic hands and the definition of more flexible, attractive, and realistic scenarios for the rehabilitation therapies using three-dimensional (3D) graphics and virtual reality techniques.
Footnotes
Acknowledgements
The authors would like to thank the Consortium of Companies that supported this project: APLIFISA S.L., IDES, IDECAL, Centro Tecnoógico CARTIF, and Centro Hospitalario Benito Menni. Juan C. Fraile, Javier Perez-Turiel, and Enrique Baeyens designed the control system and developed and programmed the control algorithms. Pablo Viñas, Rubén Alonso, and Alejandro Cuadrado developed and implemented the control electronics. Manuel Franco-Martín and Esther Parra developed the protocols for the experimental testing and supervised the tests with patients. Laureano Ayuso and Francisco García-Bravo developed and programmed the database and collected data during the experimental testing with patients. They also developed the off-line data visualization system. Félix Nieto and Laurentiu Lipsa performed the mechanical design and build the prototype.
Academic Editor: Alicia Casals
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work has been partially funded by the Spanish Centro para el Desarrollo Tecnológico Industrial (CDTI) through the project with code IDI-20130740.