
Abstract
Qualitative longitudinal research (QLR) elevates the dynamic dimensions of time, process, continuity and change and is particularly well placed for understanding how people’s lives unfold over their health journeys. This study illustrates how the application of a novel multimodal method for exploring patient life stories and complex health journeys enables enhanced sensemaking of their perspectives. The QLR was a two-year study spent collecting data over a one-year period with each participant, exploring experiences of people living with Chronic Kidney Disease (CKD) and multimorbidity and eliciting their preferences, needs, values and possible change over time. The method was based on Guided Self-Determination (GSD) theory using reflection and conversation sheets combined with photovoice for visual representation of lived experiences and semi-structured interviews. Unique layering of multimodal data and iterative analysis inspired by Thematic Trajectory Analysis, enabled creation of trajectory case profiles. Four case profiles are presented to provide illustration of new knowledge generated by the expression of lived experiences of patients, by patients and the researcher, through the QLR methods. Temporal change is evident in all cases in various forms through experiences expressed visually, in text and in conversation as either, (a) values challenged by reality, (b) adaptation, (c) navigation and uncertainty or (d) reflection and pr oblem-solving. In one case, study participation and use of the GSD tool had an unintended intervention effect. Researcher and participant reflexivity was promoted through the GSD and photovoice methods. The novel QLR methodology allowed complex trajectory case profiles to be framed in a new way to illuminate depth of person-specific insights about processes of change over time when navigating uncertainty in CKD and multimorbidity. This work further contributes new dimensions of sense-making in QLR through the layering of GSD and photovoice alongside interviews.
Keywords
Background
Qualitative research has established significance in health research for enabling depth of discovery of the human experience, and it continues to evolve in terms of methods and trends (Morse, 2020). Qualitative longitudinal research (QLR) in particular, is shown to be an evolving exploratory methodology that provides opportunities for exploration of new patient perspectives over time and achieves a perspective that captures understanding of changing, diverse human experiences in complex studies (Audulv et al., 2023; Neale, 2021a). Contemporary literature builds on the opportunities, challenges and creativity of longitudinal study methods, encouraging discourse on new ways to develop deep knowledge about people’s lived experience of health journeys through creative and flexible methods (Audulv et al., 2023; Goyes & Sandberg, 2024; Neale, 2021a). This paper intends to demonstrate the applicability of multimodal design in QLR in an exploratory study ‘DEEP’ (Decision making Experiences of Patients with Chronic Kidney Disease (CKD)), for enabling new knowledge of how and why things take place the way they do around the person and within, for people living with CKD and multimorbidity in the pre-dialysis stage.
Multimorbidity is defined as the co-existence of two or more chronic diseases (Johnston et al., 2019) and is a prevalent scenario for people living with moderate to severe kidney disease (Hawthorne et al., 2023; Walker et al., 2024). While current qualitative research about everyday life with CKD (Boonstra et al., 2022; de la Cuesta-Benjumea et al., 2023; Yapa et al., 2024) and navigation of multimorbidity exists (Peeler et al., 2024; Simpson et al., 2024) and ‘health trajectories’ are mentioned throughout the literature, there are limited studies that take a deliberate longitudinal approach focusing on living with multimorbidity (Cheng & Christensen, 2024). Even more scant is the literature describing QLR with a lens on both CKD and multimorbidity.
Qualitative longitudinal researchers are described as creative ‘bricoleurs’, that is, crafting the construction of something using an array of materials available, even adopting varied approaches to find new solutions (Neale, 2018, 2021). Therefore, the opportunity exists to progress QLR design development, with the suggestion of mixed longitudinal approaches and research tools and techniques refinement being an abundant area for potential creativity and imagination (Neale, 2018). Morse argues that amidst the array of methodological developments, attention must be given to the way we conduct our research to ensure the meaning intended by participants is deeply understood, brought into view, linked to existing concepts, then contextualized to enable implementation (Morse, 2020). The call to innovate is growing, to move away from reducing information to single word codes, which may potentially miss participants’ meaning and avoid prescribed, standardized approaches (Morse, 2020; Neale, 2018). Qualitative researchers are encouraged to reimagine data collection, not be restricted by interview dominance and embrace creative ways of gathering multimodal data (Braun et al., 2025; LaMarre & Chamberlain, 2022).
Qualitative longitudinal studies involving repeat enquiry with a backward-forward gaze in different contexts and timepoints are especially recognized as a valuable iterative method for richness of data quality (Neale, 2018), enabling an enhanced focus on the participants’ and researchers’ reflexivity and the ability to identify whether potential changes of position are sustained (Goyes & Sandberg, 2024). How ‘participant-researcher reflexive dialogue’ can be enhanced in a longitudinal context to support opportunities for sense-making through use of participatory approaches to generating data, such as visual and written art-based approaches (Harasym et al., 2024) can be further tested. Analytical approaches within QLR, such as Thematic Trajectory Analysis, are also deemed a ripe landscape for innovation, to deepen the interrogation of temporal and dynamic QLR data to explore ‘within-person’ changes for understanding “complex and dynamic phenomena” (Spencer et al., 2021).
Inspiration for a temporal lens on change in the DEEP study was drawn from intervention studies in chronic illness that had employed Guided Self-Determination (GSD) method within a nurse-led theory as a way to build evidence of an individual’s potential for change in their awareness, willingness and capacity for shared-decision making (Zoffmann et al., 2008, 2023). GSD is a value-clarifying mechanism, that positively impacts the life skills of patients with chronic diseases, with improved self-understanding and insights, meaningful self-management actions and more meaningful relationships with health professionals (Finderup et al., 2016; Linnet Olesen & Jørgensen, 2023; Zoffmann et al., 2023; Zoffmann & Kirkevold, 2012). The GSD intervention methods, translated into clinical practice as an intervention across multiple chronic conditions, including end stage renal failure (Linnet Olesen & Jørgensen, 2023; Simonsen et al., 2020; Zoffmann et al., 2023). The method comprises a series of four to eight conversations with reflection sheets based on an explicit invitation to a person to communicate, either verbally, by written text or by visual methods such as drawing, about difficulties in their life and health (Zoffmann et al., 2008, 2023). Evidence of health professionals getting to know people in a new way, gaining new knowledge for relational problem solving with GSD conversation and reflection sheets (Zoffmann et al., 2023) was the driver for deciding to apply two different GSD tools uniquely in DEEP’s longitudinal research. QLR using GSD sought to enable a new and deeper understanding of the complexity and burden of living with CKD and multimorbidity through elicitation of patients’ values, needs and preferences over time in an expedient exploratory manner.
Photovoice, a participatory method, considered to be a form of autoethnography that has a role in social change and empowerment (Pang, 2019; Wang & Burris, 1997) was also included in the DEEP study to enable individuals’ choice to identify aspects of their experiences they wanted to capture and include as data if they chose to do so. To enhance their storytelling and articulation of their experiences and needs differently, provided by visualization, is a participant engagement opportunity within the research process. Photovoice has previously been employed in studies related to end-stage-kidney-failure (Cluley et al., 2023, 2024). Cluley et al. (Cluley et al., 2023, 2024) showed photovoice as a flexible method to facilitate a participant-led approach and effectively capture the impact of dialysis outside of the treatment setting, helping in further understanding complexity of chronic kidney disease. The inspiration for layering photovoice together with GSD, and then inserting it into interview dialogue, was driven by the participatory nature of both the GSD interventional research that showed benefit for a person using drawings (Zoffmann et al., 2023) and narrative researchers who similarly applied photovoice in a layered approach to allow participants to construct verbal and visual accounts to convey their message of (Mortensen & Questiaux, 2025; Spradley et al., 2022).
The objective of this paper is to illustrate how the DEEP study progresses sense-making in QLR through utilization of novel methodology to craft the construction of trajectory case profiles. Embracing GSD and photovoice as tools interwoven with interviews in QLR, offered the possibility of creative elicitation of rich, combined longitudinal data. A selection of four individual case trajectory profiles from the DEEP study are presented in this paper to illustrate the strength of this method. The profiles show how inviting patients to contribute multimodal data and articulate the depth and complexity of their multidimensional perspectives in a new way, supports the creation of distinct sense-making both at the individual level and across the dataset between individuals.
Methods
Design
DEEP Study Setting, Recruitment and Participants
Patients living with advanced CKD (pre-Stage (5) with multimorbidity (Jun et al., 2024; Kidney Health Australia) from the Chronic Complex Care Clinic (outpatient clinic) at a tertiary hospital in the western area of Melbourne, Australia, were invited to participate. Participants were identified by the Clinical Nurse Consultant and eligible if they (a) had a confirmed diagnosis of CKD and were at pre-dialysis stage (stage 3 or 4) and had no diagnosis of cognitive impairment (b) was over 18 years of age and (c) able to speak and understand English sufficiently to participate. The researcher (JB) contacted the potential participants and obtained verbal and written consent to participate. A total of nine patients were recruited and included in DEEP. The characteristics of the four participants’ case profiles chosen for this paper can be seen in results and case selection is described. Pseudonyms have been used to present their stories.
Patients were provided with incentives in the form of shopping vouchers following each interview as an acknowledgement of time and effort for their participation over the twelve months.
Longitudinal Case Profile Selection
The key elements of enquiry in QLR are time, process, continuity and change (Neale, 2018). The four case profiles reflect temporality, change or continuity in participants’ life stories stimulated by the GSD tools and photos, which enabled insights about how and why their values, needs and preferences were realities in their lives. Processes of health care interactions, navigation, adaptation and behavioral change, alongside consistency of values, are highlighted across the selected cases.
Ethical Considerations
Ethical approval was granted by a health service Low Risk Human Ethics Committee and their University agreement. All participants provided written informed consent prior to participating in the study and were provided with written and verbal study information. All data has been de-identified prior to analysis to ensure confidentiality and anonymity and informed consent was provided for publication. To ensure a low risk of any person becoming uncomfortable talking about difficult issues related to their life and health, the researcher always paid close attention through careful listening to their needs. The researcher has experience in qualitative interviewing and is a nurse with experience in talking with people in distress.
Data Collection
Interview conversations with participants, over a minimum of three meetings at timepoints determined by each individuals’ patient journey, were audio-recorded and took place in settings that best suited the participants on each occasion. Field notes were taken during and after interviews.
The semi-structured interview guide was used in a flexible way, with the GSD responses and photos the driver for the direction of the lived experience discussion. Incorporating patient reflections into the interview ensures they have an opportunity to expand on further description of their lived experiences, provide examples and perhaps even deeper reflection during the interview process. Open ended questions in the interview guide that were integrated with the GSD response discussions and photos, focused on patients’ decision-making experiences, experiences interacting with their health professionals and overall lived experience (Supplementary file 1).
Data collection timepoints of all three methods for the four profile cases are depicted in Figure 1 which shows four different timelines, determined by the patient journey, labelled for each participant, all spanning 12-13 months. Each timeline tracks data collection points including interviews, GSD (‘Unfinished Sentences’ and ‘Space in Life’ components) and includes camera icons to indicate when photos were discussed during interviews. The timelines use a consistent colour coding system across the interview iterations. Examples of photographs and GSD sheets throughout the paper illustrate some of the data collected. Timeline of Participant Data Collection
Guided Self-Determination Reflection Sheets Adjunctive to Repeat Interviews
Participants were invited to complete the two GSD reflection sheets at two timepoints, prior to the first (at study commencement) and the final (at twelve months) interviews. Two ‘Unfinished Sentences’ from a sheet of twenty-three possible sentences and the ‘Space in Life’ reflection sheets were chosen to elicit ‘person-specific knowledge’ (Zoffmann et al., 2023). The two GSD tools chosen align with intervention studies that have used ‘low dose’ GSD (Zoffmann et al., 2023). Zoffmann et al. (Zoffmann et al., 2023) found that it is feasible to adapt GSD according to needs in different clinical contexts, including dose adjustment of the number of reflection tools used. One reflection sheet used in DEEP consists of two unfinished sentences, (i) ‘The worst thing about kidney disease is….’ and (ii) ‘Before I go to visit my health professional, I……’ (see Case 2). The other reflection sheet combined with unfinished sentences to promote problem solving, the Space in Life circles, is a visualization tool that asks participants to complete two circles, either by illustrating or writing how much space kidney disease takes up in their life now, and in a second circle, how much they would like it to take up in the future, with a reflection about what the difference is between the two (see Case 3). Each GSD reflection sheet response became a central point for conversation during the interviews, enabling the researcher to explore, with the patients, details of their challenges and problem-solving when living with CKD with multimorbidity, that they may not have otherwise considered or talked about with others (Zoffmann et al., 2023).
Data Collection Using Photovoice Adjunctive to Repeat Interviews
Participants were provided the choice to opt-in to contribute their information using photovoice and, if they chose to, were asked to take photos of their day-to-day experiences for discussion and analysis. There was no set minimum or maximum number of photos to be taken, this was entirely open to participants’ preference, and they were able to contribute photos at any point during the study period, allowing for the possibility of photos being taken at significant touchpoints for individuals as they occurred. For some, photos were submitted on a single occasion, for others it was two or three times over the year. Flexibility for participants to engage in Photovoice was paramount. For patients who consented and wanted to use Photovoice but did not have a smartphone or camera, a disposable camera was provided by the researcher. The time period between when images were taken, to the interview discussion, was anything from one week to five months with photos always discussed at the next possible interview after submission. Disposable cameras were returned by post or at an interview and required at least a week for processing and printing the film. Digital images were often sent to the researcher by participants between three to seven days prior to interview, suggesting that the planned interview was a reminder of thinking about their story of daily living. One exception was Belinda (Case 2), who started capturing photos of her health prior to commencement of the study and submitted two of those images for inclusion at the first interview. Factors impacting variable uptake of Photovoice include: lack of familiarity and comfort in using a phone for taking and sharing images (overcome by supply of a disposable camera for those who wanted to use one); strong feelings about generally being photographed (even though they were not going to be shown in the images), a feeling of uncertainty regarding what in their lives would be valuable or of interest to photograph (explanation provided by researcher that anything they wanted to show or include was suitable), and the additional effort required for thinking about taking photos and possibly returning the camera in the post. These queries or concerns reinforce the existing burden of multimorbidity workload and requirement for a flexible approach using Photovoice. In fact, participant Cathy (Case 3) contacted the researcher prior to the final interview, explaining she had not been able to take any photos in the period prior; however chose to submit a written narrative about her experiences instead, and this was included in the data set for this case.
All four participants in the case profiles reported here contributed photos, taking a range of three to ten photos each (snapshot examples of images included in this paper). Participants choose a title or label for those images, to describe what the images show, what that means to them, why is it like that and how might things be different, as well as the narrative about the setting and timepoint of the photo. This is aligned with the SHOWeD framework of questions (Wang & Burris, 1997) and evolving approaches for photovoice data elicitation and analysis (Wang & Hannes, 2020). Photos were also used iteratively in some cases from one interview to the next to sense check about a participants’ perception of change. Participants therefore could choose to change image labels between conversations if that clarified meaning in the image based on their experiences.
Data Analysis
To engage with the DEEP textual, visual and narrative data in a way that reflected contemporary approaches to understanding temporal and dynamic data, Thematic Trajectory Analysis (TTA) provided inspiration. TTA has been used within studies for diary data and interview data but is still considered a relatively novel approach providing room for creativity in its application (McNeilage et al., 2022; Spencer et al., 2021; Zhu et al., 2023). Using parts of this trajectory approach, the DEEP data was analysed iteratively in two ways, as a whole, with interview transcripts across the set of participants thematically analysed, where GSD and photos were tools for the dialogue (to be reported elsewhere), and as individual cases with three data channels, to develop within-participants’ case profiles of different trajectories, patterns and responses of identified values, needs and preferences themes over time (Spencer et al., 2021), enabling the GSD and photovoice data to be prominent elements that demonstrate the individual journeys.
The data for each case were provided by participants as layered data over timepoints (GSD, interviews and photos). The iterative nature of the analysis informed subsequent conversations with participants as the year unfolded, enabling continuous sense-checking of the significant experiences and themes generated throughout. Inductive analysis generated the following categories: values, preferences, needs, and any change over time between the two GSD data timepoints, looking back (‘the Worst thing is’ sentence….) and looking forward (the Space in Life future circle). The researcher’s field notes and case data contributed to the creation of the exploratory case profiles. Combined, the analysis of all data provides a rich and thick description of the exploration of patients’ lived experiences of multimorbidity over time. Lumivero (2023) NVivo (Version 14) Lumivero https://www.lumivero.com/ software was used to store and manage thematic coding of de-identified data.
Reflexivity
Reflexivity is the capability to examine your own feelings, values, assumptions and motives for action and how these influence and shape thoughts and actions in a situation (Neale, 2021a). The interviewer (author JB), as a health professional/researcher, was active in reflexive practice by logging field observations after each conversation and interview regarding the participant’s shared descriptions of life with CKD, a process that ensured continuous awareness of one’s assumptions as sense-making occurred. Conversations that seemed surprising or unexpected in terms of day-to-day living or what was previously known about patient engagement with health care services and professionals were noted and these became part of the overall data. A resonance with participants’ lived experience developed quickly, impacting on the decision to commence the iterative analysis process after the first GSD conversation within interview 1. Each GSD and photovoice element was considered participant-led data which provided a nuanced set of data for each person that focused the researchers’ iterative interview preparation in the longitudinal study and allowed for flexibility and reflexivity, for participants to express themselves in different modes, as well as for the researcher creating the case profiles over time. Immersion in the data longitudinally enhanced the ability to bring participant voices to the fore.
Results
Value of Layering GSD, Photovoice and Interviews in QLR
Profile Characteristics of Anne

Case 1 ‘Anne’: Values Challenged by Reality - Changing Acceptance, Trust and Coping
Significance derived from layered data: Anne’s trajectory reveals change over time when a patient’s values are in conflict with the experience of reality (Figure 2). Anne expressed acceptance of her CKD and Crohn’s Disease realities early in her time-1 GSD which was consistent throughout and highlighted later in a new way in Image 2 (discussed at final Interview 3). Image 2 represented her embedded coping and self-management over a long time through depiction and conversations about the boxes and supplies for her ileostomy on shelves captured in the image. This acceptance was all despite the time-1 worst thing GSD being ‘not having control’. Interview 2 came following the death of her husband and an awareness of needing to make some decisions to improve her life (expressed throughout Interview 2 and Image 1), however by the end of the study period things had not been positive, her relationship with her health professionals had deteriorated due to an adverse medication event and poor communication, leaving her ‘not coping’ (time-2 GSD, changed label for Image 1 at final interview, and reinforced through Image 3 at interview 3), but ‘hoping’ (time-2 GSD worst thing and circles) for improvement. Trajectory Profile and Life Story for Anne
The context and meaning of Image 3 (Figure 3) was explained: “I was in tears when I was taking that photo…and anger. Tears of frustration and anger and freezing cold”. Anne had gone to the pathology clinic on her mobile scooter from the GP clinic for a requested investigation and was told on arrival the referral form was wrong, and she needed to go to another clinic to get the test done. She took this photo from the path outside, sitting in the cold on her scooter very upset after great effort to follow the GPs instructions. This photo was a visual emphasis of her growing lack of positive interactions with her health professionals and change in trust and coping, correlating with what was described in the interviews and GSD. Tears and Anger’ (Int 3 Conversation)
Case 2 ‘Belinda’: Adapting to ‘Swimming with the Tide’ - Necessary for the Turbulence of Stress and Stability in Multimorbidity
Profile Characteristics of Belinda


Trajectory Profile and Life Story Outline for Belinda
Belinda took the photo in Figure 5 after she left hospital following a gastric bleed crisis and then an allergic reaction to something unknown. She says she was “the mystery woman with the rash on her legs. They still don’t know, honestly they still don’t know… they used to have big meetings about my rash” (Int 1). Her rash was on both legs and she chose this photo because “That’s what it’s been like, that what most of this year has been like for me. It’s not knowing, you think you’re going along, but NO, you’re body’s not functioning…” (Int 1). She had already taken this photo for herself during this crisis hospitalisation and explained that it helped to describe what changes had been happening to her body, “I think it helped cos if I’m telling you or I’m telling the doctor something, ‘this is how it started or…’” (Int 1). ‘The Great Unknown’ (Int 1 Conversation)
Belinda took the photo in Figure 7 in her backyard of two birds on the clothesline. Belinda and her family live on a large area of land and her garden is a valuable place for her to spend time. She chose to include this image “…because usually dramatic things you take pictures of… that [image 3] would be a representation of calm.” (Int 2). Belinda explained that staying ‘stable’ and out of hospital meant things were ‘calm’ for her, “…they [ health team] want me to make a decision [about transplantation], but my aim is just to keep as stable as I can…just staying out of hospital and being able to just be normal I suppose for a bit.” (Int 2). Example of GSD Unfinished Sentence Response – Belinda Time 2 ‘Where we are at – Calm’ (Int 3 Conversation)

Case 3 ‘Cathy’: “Just a Waiting Game…” - Navigating Complexity and Uncertainty in CKD
Profile Characteristics of Cathy


Trajectory Profile and Life Story Outline for Cathy

Example of GSD Space in Life Circles – Cathy Time 1 (Left) and 2 (Right)
Case 4 ‘Darren’: “It’s Given Me the Umbrella” - Reflexivity and Change for Problem Solving
Profile Characteristics of Darren

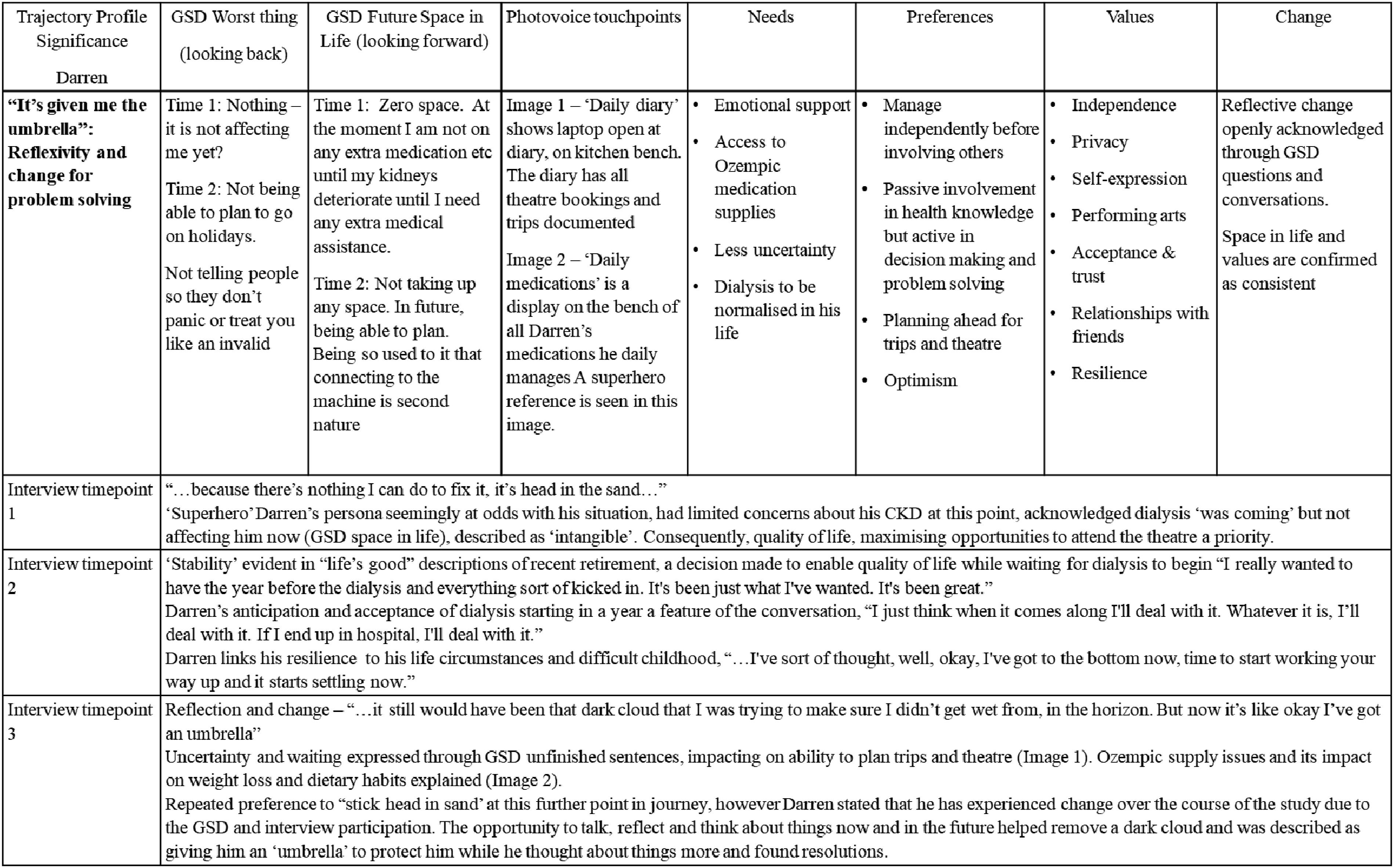
Trajectory Profile and Life Story for Darren
Discussion
This study intends to demonstrate four DEEP study participants’ case study profiles, to showcase creativity in methodological approach in QLR that elicits and illuminates patients’ preferences, values and needs in life experiences of CKD pre-dialysis with multimorbidity. The DEEP results show how combining iterative GSD reflection sheets, photovoice and interviews is a novel way to deeply and powerfully engage with participants to elucidate the fluid relationship of time (present, past and future), shifting transitions and what works for whom, when and how in peoples’ life journey with chronic illness and multimorbidity. Sensemaking was a multifaceted generative process, built on the visual, written and verbal pieces of information brought forward with each technique.
Demonstrating the Potential of a Novel Multimodal Approach in QLR
Temporality and Change
The bespoke design for engaging temporality in the DEEP study was built around participatory data collection techniques, which shaped a forward and backward gazing interview exploration, or recursive strategy by the researcher (Henry & MacIntyre, 2024; Neale, 2017). Participants were facilitated in “…revisiting [unfinished sentences], re-visioning [Space in life circle reflection] and updating a life journey [via photovoice capturing life in the moment]…and reimagine the future through the lens of the ever shifting present.” p18 (Neale, 2017) (italics added by author), at three - four timepoints throughout the year of engagement.
Significantly in DEEP, a unique examination occurred of the characteristics of change and process of change for participants, described by Henry and MacIntyre (Henry & MacIntyre, 2024) as two aspects of methodological innovation in qualitative research that have lacked focus. In DEEP this exploration took place through a lens of time being the period pre-dialysis, in itself a stage of CKD with no defined boundaries of length of time. Hence time became a phenomenon examined as well as a QLR process. All change processes illuminated in these case profiles are unique narrative data anthologies. Change was ubiquitous, but variable in style across the four longitudinal case profiles and nuances of change were brought to light through this new methodological approach for QLR that deepened the exploration of difficult aspects of life with layered insights within the same individuals over time. The journeys were unpredictable and non-linear for example: navigating worsening uncertainty with CKD pre-dialysis (Anne and Cathy); adaptation to the complexity and uncertainty through a sense of ‘stability’ due to ‘swimming with the tide’ in the second half of the twelve months (Belinda) and; reflective actions and change of acceptance of living with CKD and multimorbidity (Darren). These longitudinal and layered journey profiles offer a deeper way of understanding the complex work of continuous problem solving faced by patients with CKD (Cluley et al., 2023).
Nuance is described by Goyes and Sandberg (Goyes & Sandberg, 2024) as not only more information but contrasting and even contradictory information possible with repeat interviewing. It is evident from the DEEP study that repeated reflective backward and forward conversations based on the knowledge of what they described as the worst thing about CKD and the space CKD took up in their life, brought the nuance and complexity of navigating multimorbidity and the health system to the fore. There was layering of information, sometimes described in different ways with the addition of photos as a participatory method by which participants visually revealed nuanced circumstances (Nykiforuk, 2021), culminating in the final interview with repeat GSD reflection sheets to confirm or contrast experiences and reflections about their health and life journey. This iterative and dynamic approach also made the intensity and timing of change over time obvious, for example worsening quality of life with uncertainty (Cathy), sense-making about stability of health as a preferred changed state (Belinda) and loss of trust in health professionals (Anne).
The depth and breadth of data collected in these DEEP case profiles, suggest the application of these tools may overcome some of the practical design challenges described in longitudinal research literature related to timeframes and tempo of study (Wanat et al., 2024). ’Intensive tempo’ oriented QLR involving shorter timeframes or waves of data collection, is deemed particularly effective for depth of engagement and gathering nuanced information or rapidly capturing changing contexts (Wanat et al., 2024). However, application of GSD early in the study design, combined with photovoice no matter when it took place, appeared to achieve depth and nuance without any intensive frequency of engagement burden on participants living with chronic illness and multimorbidity. Using GSD reflection sheets was key in arriving at the critical dimensions of the patient journey earlier in the period of engagement before and during the first interview than if interviews alone were relied upon, and created the ability to “…zoom in on the intricacies of participants’ lives…” pg 4 (Wanat et al., 2024) in the same way intense tempo methods are hailed by Wanat et al. (Wanat et al., 2024), but over the continuous timeframe of a twelve month longitudinal design which is considered more challenging (Wanat et al., 2024). The photos contributed by participants were also helpful for capturing and explaining what might be considered as hidden or more discreet daily events and emotions such as Anne’s moment outside the pathology clinic and Belinda’s feeling of calm in the moment seeing the birds in her backyard. These moments of emotion are not likely to be explained or may be forgotten at a future interview conversation in a longer study timeframe and yet add nuance to the understanding of the individual’s entire experience trajectory.
Enablement of Voices, Trust and Engagement
Primacy of relationships, sustainability, trust and rapport are important in QLR (Goyes & Sandberg, 2024; Henry & MacIntyre, 2024; Wanat et al., 2024). The DEEP profiles were created from a rich participant-researcher relationship resulting from facilitation of the reflective methods that built novel and rapid engagement and trust. Therefore, a shared understanding of meaning between participant and researcher was achieved. One example of giving participant’s voice to shape and reshape the data for meaning generation, is seen in Anne’s profile, when Image 1 was initially labelled ‘Making Decisions’ at Interview 2, and then based on her challenging experiences described during Interview 3 asked again to reflect on that photograph in light of those experiences, Anne chose to re-label Image 1 as ‘Hopeless’.
The inclusion of GSD unfinished sentence ‘The worst thing about CKD is….’ seemed to trigger a sense of care about their plight. Trust was important in the context of asking for reflection using the GSD tools as it promoted stretching participants beyond their usual comfort zone, as much as they wanted to do so. This sense of care and trust did not diminish over the twelve-month period. At final interviews, when asked to describe a positive health professional interaction over the study period, a common response was ‘talking to you’. Goyes and Sandberg (Goyes & Sandberg, 2024) found similar reflexive expression by participants in their repeat interviews with prisoners, who also described the benefits of talking and having conversation about issues during exposure to the study. Information provided about the complexity of living with multimorbidity was given central visibility throughout the research process, obviously valued by participants that what they were conveying was being considered important. The resulting depth of trust in exchanges throughout DEEP, which elicited information about what mattered to these people and why, is evidence of the relational understanding that Neale (Neale, 2021b) indicates is necessary if QLR is to achieve its potential of knowing ‘how things work’.
Reflexivity with GSD and Photovoice in QLR
Researcher curiosity and flexibility is a hallmark required in QLR as “Working with time is never straightforward…” p 120 (Neale, 2018) due to it being an entity that continually shifts for both researcher and participants in terms of fluidity of forward, backwards processes. Engaging with the fluid and interacting elements of the GSD, photos and interview data across timepoints, pre-interview, during and after interviews, promoted researcher and participant reflexivity over a period of time as processes in individual’s lives were followed. The development of life stories over the year became more powerful as the case profiles were created and were profoundly impactful for the researcher. Throughout the longitudinal study period an ‘openness to creative refinement’ (Neale, 2018) was required as change and process of each individual’s life situations altered, such as with mobility, declining health, appointment schedules, IT access, family circumstances. While key to the rigor of the QLR process (Neale, 2018), the openness to exercising flexibility in data collection locations, modes and timeframes, was only possible with a significant degree of continual reflexivity about the complexity of living with multimorbidity as it was having tangible impacts in real-time on the ways of collaborating between participants and the researcher in context of this study.
To explicitly ask participants, using the GSD Space in Life circle sheet at the beginning and end of the study, to imagine how it might be in the future, enabled a dynamic engagement with the research method. Neale (Neale, 2021a) suggests “…the conjuring of an imaginary future may become a trigger point for change.” (pg 30), so the promotion of participant reflexivity during the DEEP study is a positive element of the study approach.
In case 4 though, Darren’s trajectory profile is a profound example of increased reflexivity and positive change in behaviour and attitude being triggered towards solving problems related to his life and kidney disease. While an unplanned influence of the DEEP methods, this is significant change over the year for him and illustrates GSD changing from being a method to an intervention effect. Darren’s description at the final interview of how things were different for him when the uncertainty of waiting for dialysis remained was, “It still would have been that dark cloud that I was trying to make sure I didn’t get wet from in the horizon…but now it’s like Ok, it’s given me the umbrella…” (Int 3). Darren explained that completing the unfinished sentences and circle drawings “made him stop and think about things” and realise his life with kidney disease was not that bad and had solved some problems that were in his mind that he had been “sticking his head in the sand” about. He also expressed that this insight came after the conversations, where the next day he was thinking differently after this ‘different type’ of conversation than he was having with his health professionals.
Patients with kidney failure need to use multiple coping skills for decision making and navigating their complex life situation (Subramanian et al., 2017). Zoffmann et al. (Zoffmann et al., 2023) and others have demonstrated in chronic illness intervention studies that a person’s specific knowledge about their life and health challenges can be increased through the use of GSD reflection sheets. The GSD tools act as conversation starters and prompts for reflection about things in life they may not have been previously aware of or communicated with others (Linnet Olesen & Jørgensen, 2023; Simonsen et al., 2020; Zoffmann et al., 2023). Evidence that the DEEP methodology had given Darren an ‘umbrella’ throughout this period of uncertainty was a significant realization as a researcher and reassuring that the study participation had not been a burden, in fact quite the opposite. Despite these conversations not having an intervention purpose, the use of the GSD questions, circles and photos, with discussions about all these, have helped him in a new way (researcher fieldnote, Int 3). It was apparent that Darren had achieved a new level of what Zoffmann et al. (Zoffmann et al., 2023) describe as ‘relational capacity’ resulting from his reflections, whereby an increased openness to share his new self-insights led to a decreased loneliness in his CKD self-management journey.
Darren’s use of the ‘umbrella’ metaphor gives rise to new knowledge and an ability to piece together the processual change evident in his trajectory. The need to be shielded or protected, or having something to hold onto, or perhaps even the space for reflecting, problem solving and contemplating the positives in a situation (being under the umbrella) are new ways of seeing the nuance of how things are for someone living with CKD in the pre-dialysis phase.
Strengths, Limitations and Future Perspectives
The intervention-effect unplanned finding for Darren, Case 4, strengthens the argument for the contribution that GSD can provide for self-awareness and empowerment in the context of living with CKD and multimorbidity and points to greater opportunity to action research in this space. This finding also provides a reminder that QLR is a continuum, where research methodology and interventional approaches may be intertwined; therefore iterative reflexivity and responsiveness along the trajectory of engagement are all the more essential.
The DEEP study methodology presented via four case-based trajectory profiles represents the variety of values, experiences of change as described in this paper and does not attempt to be representative of all perspectives of the DEEP participant cohort, nor of all patients living with pre-dialysis CKD and multimorbidity. These case studies are chosen to illustrate influence of the novel methodological approach on eliciting values, preferences and needs in the context of the DEEP study. Making sense of marking time pre-dialysis was found to be advanced through the DEEP QLR study. People were empowered to articulate and reflect on what happens when and how in life over the pre-dialysis temporal, uncertain journey through the multimodal approach applied in DEEP.
Conclusion
The DEEP study offers a novel contribution for utilization of a combination of guided self-determination tools, photovoice and interviews, as a methodological approach in QLR as well as potentially contributing to the further development of GSD in healthcare research. DEEP’s methodology articulates how creative and dynamic combinations of methods in QLR can accomplish a depth of longitudinal person-centred and person-specific insights about changes that are caused by and located in time. In DEEP, a new sense-making of the complex trajectory of patients’ pre-dialysis CKD and multimorbidity health journey has been illuminated.
Supplemental Material
Supplemental Material - Application of Guided Self-Determination Method and Photovoice in Qualitative Longitudinal Research for Enhanced Sensemaking in Chronic Kidney Disease with Multimorbidity
Supplemental Material for Application of Guided Self-Determination Method and Photovoice in Qualitative Longitudinal Research for Enhanced Sensemaking in Chronic Kidney Disease with Multimorbidity by Jennifer Barr, Kevin Mc Namara, Elizabeth Manias, Anne Frolich, Lars Kayser, Bodil Rasmussen in International Journal of Qualitative Methods
Footnotes
Acknowledgements
The authors would like to thank the participants of the DEEP study as well as Bili Velevski, Clinical Nurse Consultant, who assisted in the identification of all potential participants. We are also grateful to Vibeke Zoffmann, valued consultant on the application and sense-making with GSD in the DEEP study.
Ethical Considerations
The DEEP study was approved by the Western Health Low Risk Human Ethics Committee and meets the requirements of the National Statement on Ethical Conduct in Human Research (2007 and updates): WH/91762 and WH – Deakin Research Collaboration Agreement. All persons in this study gave informed consent to participate and for their data to be used in publication.
Author contributions
JB contributed to this study by collecting all data, the GSD reflection sheets, photo elicitation and interviews, also writing all drafts of the article.
LK, BR, KMcN, EM and AF contributed by discussion and approval of data analysis, editing of all drafts and approved submitted manuscript. All authors have been involved in the conception and design of the article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The case profiles are available from the first author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.