
Abstract
Background
Chronic kidney disease (CKD) is common amongst people experiencing a myocardial infarction (MI) (a ‘heart attack’), and confers an elevated risk of mortality and morbidity as well as increased healthcare costs (Fox et al., 2010; Santopinto et al., 2003; Sederholm Lawesson et al., 2015). Moderate to severe CKD affects up to 40% of those with MI (Santopinto et al., 2003; Sederholm Lawesson et al., 2015). Risk of death is positively associated with severity of kidney impairment: in-hospital mortality for those with severe (stage 4–5) CKD is 4–5 fold that of people without CKD (Bagai et al., 2018). CKD significantly increases the risk of major bleeding, (James et al., 2010) acute kidney injury (Bagai et al., 2018) and stroke (Jakobsson et al., 2014) after MI. In the longer-term, morbidity associated with cardiovascular disease may act as a barrier to successful dialysis and kidney transplantation in those that progress to kidney failure.
The primary clinical aim in the management of people experiencing MI is to restore blood flow to the heart muscle to resolve ischaemic chest pain and minimise long-term cardiac injury. Concomitant initiation of cardioprotective medications reduces the risk of further MI, hospitalisation for heart failure and cardiovascular death.
Need for mechanical coronary revascularisation (percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG)) is dependent on assessment of the extent and location of the disease coronary vessel(s), most commonly achieved through invasive coronary angiography. The decision to undertake coronary angiography is determined by the nature of the clinical presentation, with ongoing chest pain associated with ST-elevation or dynamic electrocardiographic (ECG) changes, haemodynamic instability or severe arrhythmia necessitating urgent/immediate assessment (Collet et al., 2021). Patient factors, such as comorbid conditions and expected survival, are also taken into account. Current cardiology guidelines recommend PCI for ST elevation MI (STEMI) be conducted within 90 minutes from the onset of chest pain (Ibanez et al., 2017). In contrast, guidelines recommend angiography to be undertaken within 24 hours of presentation in high-risk patients with non-ST elevation MI (NSTEMI) (Collet et al., 2021).
Quantitative international observational studies have shown that people with CKD are less likely to receive coronary angiography or revascularisation following MI. They are less likely to receive cardioprotective medications after an MI (Sederholm Lawesson et al., 2015), and are less frequently counselled about lifestyle modifications (Vasaiwala et al., 2012). The reasons for the disparities in MI care for people with and without kidney disease are not known.
Clinicians and patients are required to make a number of different treatment decisions at varying time points during and following an MI. These include whether and when to seek advice from healthcare professionals, whether a patient requires referral to a cardiologist or admission to a specialist cardiology ward, the extent of investigation required, whether to attempt mechanical restoration of blood flow to the heart muscle, and which cardioprotective medications to start after an MI.
Our understanding of the optimal management of MI in people with CKD lags behind that in the general population because people with CKD have been excluded from the majority of large-scale randomised controlled trials that have advanced MI care over the past 50 years (Konstantinidis et al., 2016). Recommendations in international guidelines regarding the treatment of MI in the CKD population are based on the results of small sub-group analyses, observational research and expert opinion only (Collet et al., 2021; Lawton et al., 2022). Treatment decisions for the 30%–40% of MI sufferers who have CKD are therefore being made in the absence of high-quality evidence, often on the basis of consensus (Lawton et al., 2022).
Study Justification
People with kidney disease not only have a significantly increased risk of MI compared with the general population but suffer greater morbidity and mortality as a result of these events. There is a lack of both qualitative and quantitative research relating to the management of MI in this population, especially in the UK. This study aims to address these gaps in our knowledge base. This study will contribute understanding that will lead to the improvement of care pathways for this high-risk population presenting with MI.
There is insufficient research specific to people with CKD to understand how treatment decisions are made in the absence of evidence, what factors influence decision-making, to what extent decision-making is shared, and what factors explain the reduced access to intervention for people with CKD. A review of the literature undertaken during the development of this study identified a single qualitative study from Canada relating to either MI treatment decision-making, or experience of MI care, specific to people with CKD. This single-centre study investigated barriers and facilitators to shared decision making for coronary procedures in people with kidney disease. Interviews were undertaken with 20 patients, one carer and 10 cardiologists (Finlay et al., 2020). The research team identified the patient’s age, comorbidities, kidney function, perceived potential to benefit from revascularisation and individual treatment preferences as factors taken into account by cardiologists with respect to treatment decisions. Cardiologists were most likely to seek patients’ opinions in situations where the benefit of one treatment over another was not clear. Patients reported the complexity of information and lack of time during acute care as a barrier to involvement in treatment decisions.
However, the study provided limited evidence regarding the actual process of treatment decision-making. In addition, only cardiologists were interviewed, despite many other clinical staff being involved in making decisions regarding MI care, especially in those with kidney disease. Decision-making may also differ between centres and/or healthcare systems.
The experiences of patients with kidney disease also remain under-described. The majority of patients interviewed by Finlay et al. [ref] were male (75%). Whilst some had experienced MI, others had received coronary intervention for other reasons, such as stable coronary artery disease. We therefore lack sufficient information relating to how people with kidney disease are informed about and understand their treatment options following MI, what their treatment preferences and priorities are, and how involved they are, or wish to be, in treatment decision-making. This study is designed to address these gaps in our knowledge and thus inform the improvement of UK care pathways for people with CKD who develop MI.
Explanation and Justification of Method
Qualitative methodology will enable us to understand how MI management decisions are made for, and by, patients with CKD, and how people with kidney disease experience MI care. These insights will assist with the interpretation of quantitative research demonstrating disparities in MI care between people with and without kidney disease. Recognising the limited knowledge in this area, we will use semi-structured in-depth interviews to guide conversations with patients and clinical staff whilst being open to new avenues of interest. As the primary researcher is a doctor working in kidney care, we appreciate that her background and perspectives will influence all stages of the research process. We will use reflexive thematic analysis (Braun, & Clarke, 2006; Clarke, 2019) to recognise and communicate these positions within the study.
A previous systematic review and thematic synthesis of qualitative studies investigating the views of patients and carers found that decision-making for treatment for chronic kidney disease is influenced by the experiences of other patients and their social context (Morton et al., 2010). We have therefore adopted an interpretivist and social constructionist epistemology to acknowledge the importance of prior experiences and the social context of individuals on decision-making. In this approach, the reality of what is being studied is considered socially constructed and subjective, and knowledge of this is developed through attempts to understand people’s views and experiences of that reality (Burr, 1995). With regards to thematic analysis, adopting a constructionist approach signifies that language is not only viewed as a simple reflection of meaning or experience, but implicit within the social production and reproduction of these concepts (Schwandt, 1998). Codes and themes will be drawn out from the data according to how meaningful the researcher believes the information to be, where meaningfulness is determined by relevance to the research question and the degree of conviction in the participant’s expression when addressing different issues (Braun, Clarke, 2012), rather than a simple count of recurrence within the data.
Data will be analysed according to the six steps outlined in thematic analysis (Braun, & Clarke, 2006). This simple and systematic methodology will enable us to identify patterns within the data and interpret both semantic and latent meanings. Initial theories and hypotheses will be derived by examining the data inductively, and an iterative process will be used to progressively refine our understanding by repeatedly revisiting the data to confirm or refute patterns and themes as they are generated (Hopwood, 2009)
Research Aims
Our overarching aim is to understand the process of MI care decision-making for, and by, people with CKD, and the experiences and opinions of people receiving and providing this care.
In interviews with clinical staff, we will investigate: • What influences decision-making? • Who is involved in decision-making? • How the risks and benefits of treatments are deliberated? • Perceived barriers to and facilitators of the delivery of optimal care.
In interviews with patients, we will investigate: • Experiences of heart attack care in the NHS. • Understanding of the risk of cardiovascular disease associated with CKD. • The extent, and way(s) in which patients are involved in treatment decision-making and their treatment preferences. • Patients’ priorities in the management of concurrent heart and kidney disease.
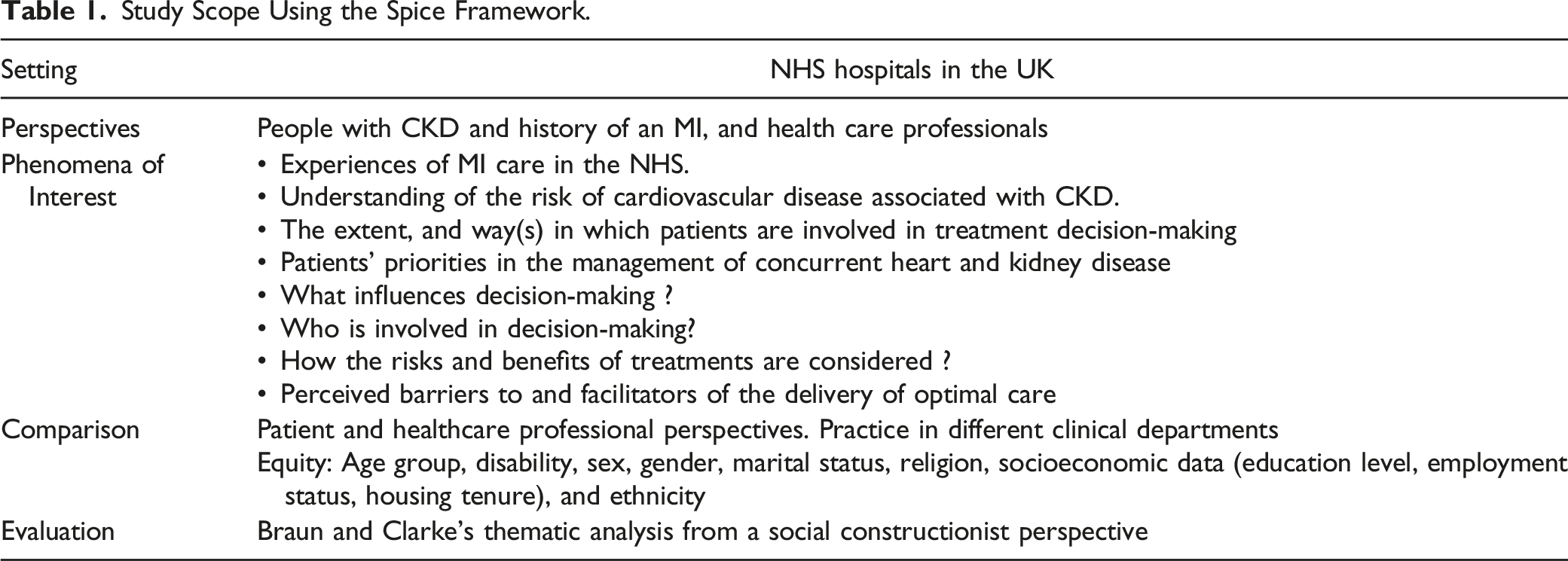
The Setting, Perspective, Comparison, Evaluation (SPICE) Framework was used to define the scope of the study and formulate the research question (Table 1) (Booth, 2006).
Sample and Recruitment
Setting: This study will take place in between three and five NHS hospital trusts in the UK. Hospital sites will be selected to ensure diversity with respect to the ethnicities and rural-urban spread of the populations served and the availability of cardiac and/or kidney specialties. Three sites will be initially purposively selected, with the option to theoretically sample up to two further sites if required to further explore patterns identified in initial analyses (Marshall, 1996).
Eligibility
Inclusion Criteria
People with kidney disease and a history of MI: • UK-resident adults aged ≥18 years with moderate to severe kidney disease (CKD stages 3–5, +/− kidney replacement therapy) who have received treatment for a heart attack in a UK hospital within the past 24 months will be eligible to participate.
Clinical staff: • Doctors and nurses currently practising medicine in the UK, who have self-reported experience of managing heart attacks in people with kidney disease (CKD stage 3–5, on kidney replacement therapy) will be eligible to participate.
Exclusion criteria
Patients with kidney disease who: • Are deemed by their clinical team to be lacking the mental capacity to consent to involvement in the study. • Underwent coronary valve or aortic root repair or replacement during the MI hospitalisation.
Sampling
The exact sample size will depend on when the sample has delivered sufficient information power (Malterud et al., 2016). Similar studies conducted previously (Finlay et al., 2020; Jansen et al., 2019; Richter et al., 2020) suggest the total sample size (people with kidney disease and clinical staff) is unlikely to exceed 40 participants.
Patients and clinical staff who meet the relevant eligibility criteria will be purposively sampled from participating sites. Iterative purposive sampling will be undertaken initially to achieve diversity with respect to age, gender, and ethnicity. Sampling of patients will also aim to achieve diversity with respect to CKD stage, type of MI treatment received and socioeconomic status. Sampling of clinical staff will aim to achieve diversity with respect to specialism (e.g., nephrology/cardiology) and profession (e.g., doctor/nurse). Initial sampling will aim to achieve a diverse sample, but subsequent sampling will be theoretical, selecting participants with the aim of expanding or explicating patterns identified in the initial analyses and to test and develop hypotheses (Marshall, 1996).
Recruitment
Patients With Kidney Disease
Patients who are eligible to participate in the patient interview study will be identified by local principal investigators at each of the participating NHS hospital sites. The principal investigators will undertake purposive and later theoretical sampling according to the sampling criteria and specific requests from the chief investigator. Individuals will be invited by post or by a nurse or clinician at their next Nephrology outpatient visit. Patient information will be transcribed into other languages commonly spoken in the region of the selected Trusts if there are significant populations of individuals for whom English is not a first language. Contact will be made with non-responders by phone, post or in-person (by a clinician at their next Nephrology outpatient visit) after a two-week interval to ensure they have received the invitation and to respond to questions.
Clinical Staff
Local principal investigators at each of the hospital sites will invite eligible clinical staff to participate either in person or via email. Potential participants will receive an information sheet specific to clinical staff. The principal investigators and/or chief investigator will undertake purposive sampling of staff with respect to age, gender, ethnicity, and specialism. A snowballing approach may also be used. Later, theoretical sampling may be undertaken.
All participants will be offered £25 to thank them for participation and travel and caring costs (e.g., childcare) will be reimbursed where applicable.
Consent
Before consent is requested, all participants will be given an information leaflet with full details about the study. Written consent will be collected with additional verbal consent at the time of interview where written consent has not yet been received or received more than 24 hours in advance. Specific consent will be requested for audio-recording of the interview and sharing anonymised transcripts with other researchers and during teaching. Information on demographic characteristics will be requested at the time of interview. One copy of patient consent will be filed in the individual’s medical records.
Data Collection
Semi-structured interviews will be conducted by the Chief Investigator (first author) and digitally audio-recorded either in person at a site of the participant’s choosing (hospital building, university building, home or other private location) or virtually via videoconferencing or telephone. Professional interpreters will be used for interviews with people who are not fluent in spoken English or communicate by sign-language. The interview will be guided by the use of flexible topic guides. The topic guides will evolve over time as the interviewing progresses, based on initial findings, patterns in the data and hypotheses. Initial topic guides are provided as Supplementary Material (Supplementary Tables 1 and 2). Interviews are expected to take 60–90 minutes.
The following demographic data will be requested: age group, gender, and ethnicity. In addition, patient participants will be asked to provide data on marital status, religion and socioeconomic factors (education level, employment status). Clinical staff will be asked where they undertook their medical training, and how long they have been working in their current role and at the study site. This will allow us to direct future sampling to achieve diversity. It will also allow us to investigate relationships between personal and professional characteristics, experiences of healthcare, and views on optimal management of MI in advanced CKD and a possible future trial to improve patient experiences and outcomes.
Participant Withdrawal
Participants can stop the interview at any time. Participants will be able to withdraw from the study and have their interview data deleted at any point up to two weeks after their interviews. After two weeks the interview will have been analysed and so participants will not be able to withdraw their data at this stage. They will be informed of this in the participant information sheet. Contact details for the chief investigator will be provided in the information leaflet so that participants can withdraw.
Analysis
Interviews will be audio-recorded, transcribed, and analysed using the six steps outlined in Braun and Clarke’s Reflexive Thematic Analysis (V. Braun, & Clarke, V., 2006) from a social constructionist position. Interviews will be transcribed verbatim and personal identifiers removed at transcription. Transcripts will be uploaded onto NVivo qualitative software to facilitate analysis. Each transcript will be read, and the audio-recording listened to repeatedly by the Chief Investigator (JS), for familiarisation. Coding of the data will be undertaken by JS by assigning descriptive labels to sections of text to highlight semantic or latent meaningfulness. Coding will be predominantly inductive. Codes will be collated, reviewed and organised into clusters with shared meaning relating to a central single concept (“themes”) (Braun & Clarke, 2013). Initial themes will be reviewed and combined, refined or discarded in order that the data within each fit together meaningfully, and there is distinction between themes. Themes will be defined and named before the report is produced. Five further researchers (PB, LS, FJC, YBS and TJ) and members of a patient and public involvement group will be involved in refinement of themes, exploration of different possible interpretations of the data and sense-checking ideas. Data collection and analysis steps will take place iteratively to follow-up on themes, patterns and hypotheses identified in prior interviews using theoretical sampling.
The Chief Investigator is a trainee nephrologist working in a UK hospital with tertiary kidney and secondary cardiology services, who is undertaking this work as part of her Doctoral Fellowship. She has experience of making MI treatment decisions for, and with, people with and without CKD and has a broad understanding of the quantitative observational evidence base demonstrating variation in MI care between these populations. Her primary research interest is equity of utilisation of healthcare services and understanding treatment variation. Theoretical sensitivity and reflexivity will be supported by the Chief Investigator’s previous professional experience working clinically with people with CKD, input from a patient advisory group, extensive review of the relevant literature, and an open attitude to the analytic process (Glaser B, 1967). Reflexivity during the research process will also be promoted by maintaining a research diary and regular meetings with team members (PB and LS) for reflexive discussion.
Ethics
Before study initiation the study plan and documents were reviewed by an NHS Research Ethics Committee (REC) and the Health Research Authority (HRA). Ethical approval was granted by NHS Research Ethics Committee Southwest (Reference 21/SW/0162)).
Participation in this study presents no physical risk to participants but there may be an emotional impact. The experiences of patients and their families may have been difficult, and participants may discuss these difficulties. Prior to participation individuals will have been provided with information about the study in the participant information leaflet. Participants can stop the interview at any time. A Distress Protocol will be followed if patients become upset. If individuals do raise unresolved medical, surgical or psychological issues, with consent, these will be fed back to the clinical team. In situations whereby serious concerns for a participant’s wellbeing are raised, local safeguarding procedures will be followed. Risks to the primary researcher (JS) will be minimised by conducting in-person interviews in accordance with the Sponsor’s Lone Working policy, and regular debriefing with the supervisory team.
Rigour
Several strategies will be adopted to ensure qualitative rigour. High-quality Reflexive Thematic Analysis requires strong reflexivity and openness to scrutinizing who the researcher is, why the researcher has chosen the specific topic, methodology and methods, what assumptions have been made, and how these fit with the research objectives (Clarke, 2019). The research team will write a reflective piece on our positionalities at the start of the project, and will revisit these during data collection, and analysis, for example in generating the themes.
Within reflexive thematic analysis, Braun and Clarke propose twenty questions to guide reviewers in assessing the quality of research (Clarke, 2021). These focus on the rationale for, and explanation of, the methods and methodology used, and the existence of a well-developed and justified analysis. Braun and Clarke highlight the importance of explaining why thematic analysis has been chosen, the type of thematic analysis and how this fits with the theoretical and conceptual stance of the researcher(s) and the research methods chosen. They specify the need for each theme to reflect a distinct central organising concept with which codes with shared meaning interact, rather than existing as a summary of a domain of data, and for the authors to understand the differences between the assessment of generalisability between qualitative and quantitative research. The use of NVivo facilitates transparency during analysis as summaries or interpretations can easily be linked back to the raw data.
Study Scope Using the Spice Framework.
Patient and Public Involvement
People with kidney and heart disease have been consulted on the acceptability and importance of the research topic and research design. Members of the UK Renal Registry patient committee and Royal Free Kidney patients’ association offered comments following presentation of the research idea at group meetings. An advisory group comprising patients with CKD and heart disease have commented on patient-facing materials and the topic guide for the patient interviews. They will be asked to assist with the interpretation of findings from the interviews via online group meetings and dissemination of findings to wider patient and public groups. Members will be appropriately reimbursed for time, travel and any other costs incurred whilst assisting with this research in keeping with NIHR guidance (NIHR, 2022).
Supplemental Material
Supplemental Material - Treatment Decision-Making in Myocardial Infarction for People With Advanced Kidney Disease: Protocol for a Qualitative Study
Supplemental Material for Treatment Decision-Making in Myocardial Infarction for People With Advanced Kidney Disease: Protocol for a Qualitative Study by Jemima Scott, Lucy Ellen Selman, Fergus J. Caskey, Thomas Johnson, Yoav Ben-Shlomo, and Pippa Bailey in International Journal of Qualitative Methods
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is funded by the National Institute for Health and care Research (NIHR) [Reference NIHR300906]. The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.