
Abstract
Qualitative evaluation of health interventions is recommended to document the reality of the intervention process in all its complexity. From this perspective, we have developed a study protocol for a family therapy intervention for adolescents with anorexia, grounded in the realist evaluation approach and the concept of robustness, which we called « infra-realist inquiry ». Family therapy is the internationally recommended first-line treatment for adolescent anorexia nervosa. Among the models developed, the Maudsley model is the most widespread and well-documented. While its effectiveness is now widely accepted, knowledge on its implementation process remains limited. Qualitative methods have scarcely been employed. We designed a longitudinal qualitative research study to explore the intervention process of the Maudsley model in a French hospital. In this ongoing study, we adopt an interpretative phenomenological analysis approach to understand change mechanisms in adolescents, and we use a focus group method with a reflexive thematic analysis approach to identify barriers to change and the resources needed for parents and healthcare providers. Over the course of one year, three individual interviews are planned with adolescent participants and three focus group discussions with parents and healthcare providers at regular intervals (months 1, 6, 12). Drawing on critical realism ontology, we constructed a study design aiming to understand the reality of adolescents with anorexia nervosa from their own perspective, using a visual narrative technique (photo-elicitation) and a future-oriented approach (possible selves).
Keywords
Background
Qualitative Evaluation of Health Interventions
Qualitative evaluation of health interventions is now recommended to document and analyze what actually occurs during an intervention (Pons-Vigués et al., 2019). Although the randomized controlled trial is the model of reference in the clinical field due to its high internal validity, it cannot be considered sufficient to study the complexity of health interventions (Skivington et al., 2021). Health interventions are implemented in natural settings that evolve and adapt in response to real-world conditions. These settings are characterized by a multiplicity of interacting components—including the people involved, as well as material, procedural, and financial aspects—whose outcomes depend on the context, the conditions of implementation, and the participants involved (Cambon et al., 2019). International recommendations emphasize the need to document not only the efficacy of the intervention, but also its process: what happens, how, when, and why (Campbell et al., 2007), thus requiring the use of a more flexible evaluation model.
Recently, several movements have emerged and have been grouped under the term “(re)turn to realism(s)”, which considers the need to account for the complexity of reality. The evaluation of complex health interventions is primarily situated within the framework of critical realism (Ridde & Haddad, 2013). Realist evaluation aims to understand the complexity of health interventions by seeking to determine what works, for whom, and in what contexts, within the paradigm of pragmatism. In realist evaluation, it is believed that it is not the intervention itself that produces changes/effects, but rather the interaction between the resources brought by the intervention and elements of the context that may (or may not) trigger one or more mechanisms that will produce the effect. In other words, it is the individuals who make change possible, thanks to the resources offered by the intervention program (Westhorp, 2014).
The qualitative evaluation of health interventions thus shifts the analytical focus from performance towards the robustness of the intervention framework, as conceptualized by Hamant (2024). Indeed, performance evaluation encounters challenges associated with standardization (if an intervention is effective for the majority, it must be effective for everyone), non-sustainability (the material, social, and psychological conditions of the evaluation may not persist thereafter), and optimization (deviations from the measurement are regarded as weaknesses or biases to be corrected). In this context, Hamant (2024) emphasizes that in the quantitative evaluation of progress (whatever its form), the measurement often becomes the target, thereby limiting its reliability. The concept of robustness, geared towards the study of fluctuation, learning, and the capacity for self-determination, appears better suited to investigating the reality of an intervention, given its multifaceted, dynamic, and unpredictable nature. The methodological challenge therefore becomes the ability to capture the unique experiences of the actors involved in the intervention, to facilitate their narration, and to generate knowledge that is useful for understanding the human and social phenomena associated with the intervention. Within this theoretical and conceptual framework, we developed a study protocol aimed at qualitatively evaluating an innovative and alternative intervention for the treatment of anorexia in adolescents.
The Maudsley Model in Anorexia Nervosa
The prevalence of eating disorders (EDs) among adolescents has increased steadily over the past decade. Anorexia is the most common ED and is characterized by intentional weight loss, induced and maintained by the patient (WHO, 2019). EDs are often associated with an intense fear of gaining weight and a distorted body image. Anorexia nervosa is notable for its potentially severe prognosis, ranging from the risk of chronicity and complications to the risk of death. Approximately 1% of the population is affected by anorexia, with the ratio rising to 4% among females (Keski-Rahkonen & Mustelin, 2016).
Currently, family therapy is the internationally recommended first-line treatment for adolescent anorexia nervosa (Hilbert et al., 2017). Among the developed models, the “Maudsley model” is the most widespread and well documented. Developed in the late 1980s within the Child and Adolescent Eating Disorder Service (CAEDS) at Maudsley Hospital in London, UK, it is a family-based treatment. The team combines pediatrics and psychiatry expertise through interdisciplinary collaboration between psychiatrists, pediatricians, nurses, psychologists (family and individual therapists), and dieticians, all working together at the same site. The model draws heavily on systemic family therapies, incorporating techniques from several approaches (strategic, structural, narrative), along with psychoeducational and cognitive-behavioral contributions. The intervention is divided into three phases (weight restoration, transitioning control of eating back to the adolescent, and addressing the adolescent’s identity), structured over approximately one year of care. The focus is on the factors that perpetuate anorexia, rather than its underlying causes (Doyle et al., 2010).
The number of studies demonstrating the effectiveness of the Maudsley model for adolescents with EDs is increasing (Fernández García & Quiles Marcos, 2024). These studies show that family therapy is effective in outpatient settings, yields excellent long-term outcomes, and is frequently recommended in treatment guidelines. The treatment framework based on the Maudsley model improves referral processes, promotes early intervention, enhances disorder detection, and increases treatment adherence (Wittek et al., 2023). Research also indicates that the vast majority of adolescents with anorexia can be treated entirely on an outpatient basis, with 70% to 90% achieving at least partial recovery by the end of 6 to 12 months of treatment, and relapse rates below 10% (Fernández García & Quiles Marcos, 2024). Lastly, hospitalization periods for adolescents often constitute disruptive moments in their development, family life, social life, and academic progress.
Need for Qualitative Evaluation of the Maudsley Model
While the effectiveness of the Maudsley model is now widely accepted, there is still limited knowledge regarding its implementation process, its adaptation to other contexts, the experiences of patients and families, and the mechanisms of change during therapy (Fernández García & Quiles Marcos, 2024). Although qualitative methods are best suited to produce such insights (Renjith et al., 2021), they have scarcely been employed to document the Maudsley model and family therapy in the context of eating disorders. In a scoping review, Baudinet et al. (2021) highlight that only 10 qualitative studies on this topic have been identified, with only 6 of them including patients in the data collection process. Qualitative data on treatment experiences suggest that it is perceived as helpful, encouraging, and lifesaving, but also highly distressing for both adolescent patients and parents. Adolescents report feeling they are not heard and experience a loss of identity during treatment, particularly during the initial phases when parents take the lead. Recently, Baudinet et al. (2024) conducted interviews with female patients that revealed that the changes that occur during treatment are closely linked to young patients’ level of trust in professionals and their parents. The authors also theorize several key moments in the care process: patients’ realization of their situation and condition, their perseverance and belief that recovery is the only way out, and the importance of maintaining a life outside of treatment and illness. Additionally, qualitative studies have highlighted the perceived benefits by parents of sharing experiences with other parents, and observing and learning from families in similar situations (Baudinet et al., 2021).
While these qualitative studies provide valuable insights into the experiences of adolescents during the intervention and acknowledge variations in the model’s effectiveness, there remains a scarcity of data on adolescents’ treatment experiences and their perceptions of how change occurs during therapy. Indeed, current research struggles to shed light on the mechanisms driving the effectiveness of family therapies (Jewell et al., 2016). Several hypotheses might explain this, beyond the general lack of qualitative research on the Maudsley model. Firstly, to our knowledge, only one study (Voriadaki et al., 2015) has employed Interpretative Phenomenological Analysis (IPA) to explore the experiences of adolescents (n = 5). IPA is the preferred approach for understanding and theorizing mechanisms of change, particularly in relation to identity processes and the therapeutic context (Smith et al., 2022). Secondly, no longitudinal studies have been conducted, leaving us with limited understanding of the dynamic and evolving nature of these change mechanisms. Thirdly, study protocols do not mention the involvement of affected individuals (adolescents or parents) in the design and implementation of research, even though this is now recognized as a quality criterion in health research. Engaging those affected in research can lead to the production of knowledge that closely reflects the real experiences of those involved (Davis et al., 2024).
We therefore designed a study using Longitudinal Interpretative Phenomenological Analysis (LIPA) to document the intervention process of the Maudsley model and to generate knowledge about the change mechanisms that explain the model’s functioning conditions. We describe our approach as “infra-realist”, as it aligns with the realist evaluation framework, which seeks to document the operation of interventions in real-world contexts (Westhorp, 2014). However, our qualitative inquiry can be considered to be “infra” in that it focuses on understanding and transforming reality from within, exclusively through a phenomenological approach (and a qualitative method) centered on the possibilities and capacity of adolescents to reinvent themselves. The rationale for this approach is described in the Method section below.
Method
Type of Study
We are conducting longitudinal qualitative research (LQR), which aims to study how and why experiences change over time within a sociocultural context (Korstjens & Moser, 2022). The study started in February 2023 and ended in April 2025. LQR is used increasingly in the evaluation of health interventions for the in-depth analysis of the mechanisms of change engaged by the actors (Sheard & Marsh, 2019). It is therefore recommended to investigate the phenomenon under study with a small and homogeneous sample. We chose to adopt a LQR approach to align with an evaluation framework focused on “robustness”, emphasizing the study of individuals, contexts, and practices as interrelated elements engaged in a dynamic process of constant fluctuation and mutual adaptation.
The study is being conducted at Inter-Hospital Family Unit for Adolescent Eating Disorders at Jean Verdier Hospital in France (UFITAA, for the French acronym). It provides outpatient treatment that includes pediatric, dietary, psychiatric, and individual or group psychotherapeutic follow-up, with a strong focus on health promotion. This approach incorporates workshops aimed at supporting the autonomy and empowerment of adolescents and their families.
The average duration of treatment is approximately one year. For this reason, we have chosen to explore the experiences and evolution of adolescents, parents, and healthcare providers over the course of a year. Individual interviews are conducted with adolescents to gather information on their personal and intimate experiences of the intervention, as well as their individual progress. Meanwhile, focus groups are held with parents and healthcare providers to capture their perspectives and understand how they collectively form their opinions regarding the intervention.
The steering committee consists of two former patients from the unit, two parents of children with anorexia (previously treated in the study hospital), two professionals from the unit, and two researchers. The steering committee is involved in designing the study and in establishing the framework for analyzing the results, ensuring that all stages of the project are properly followed.
Paradigm & Theoretical Framework
Our study is situated within the field of complex health intervention evaluation, which is primarily dominated by the ontological framework of critical realism. In real-world contexts, the protean, contingent nature of outcomes and their dependence on context make it challenging to strictly evaluate causal attributions (Craig et al., 2008). For this reason, current evaluation models tend to focus more on studying contribution, aiming to understand how interventions play a role in achieving the observed outcomes (WHO, 2022). Consequently, the use of comprehensive evaluative approaches such as realist evaluation seeks to understand how interventions bring about change by shifting the focus from effectiveness to their functioning: how they work, why, for whom, and under what circumstances? This approach is pragmatic in that the results are used to revise, clarify, or redirect interventions, ultimately seeking to improve their quality (Bhaskar, 2008).
In the context of the Maudsley model for adolescents with anorexia, our primary focus is on the perceptions of the self. The risk factors associated with EDs are numerous, and there is no consensus on the causes of their onset (Miskovic-Wheatley et al., 2023). Current practice focuses on understanding the mechanisms that sustain the disorder rather than on discovering its etiology. Among the most frequently cited mechanisms in international literature is the influence of “self-perceptions” (self-concept, self-esteem, body image) on the intense fear of weight gain, distorted body image, and eating behaviors. It has been widely demonstrated that low self-esteem, the internalization of thinness standards within the self-concept, and consistently biased perceptions of one’s physical appearance can trigger and sustain anorexia (Karpowicz et al., 2009). Stein and Corte (2007) suggest that therapeutic interventions should focus more on identifying and cultivating positive self-perceptions, particularly concerning the possible future selves. Indeed, anorexia is closely related to patients’ concerns about their future body image and their desire for control over their development (Erikson et al., 2012).
Possible selves are defined as “the components of the self-concept that represent what individuals could become, hope to become, or fear becoming” (Markus & Nurius, 1986, p. 954). Research has documented a strong aversion to life changes and a need for fixed routines among patients suffering from anorexia, which relates to two dimensions of possible selves: probability and controllability (Strober, 2004). Additionally, Erikson et al. (2012) found that individuals with anorexia report a greater number of negative possible selves compared with the general population, and therefore evaluate the prospect of recovery from anorexia with a negative valence. Thus, the aim of our study is to document changes in adolescents undergoing treatment at UFITAA, focusing particularly on the evolution of their possible selves.
We situate our work within the epistemological framework of contextualism, acknowledging the contextual nature of the knowledge produced and the influence of researchers’ perspectives on this knowledge. In this sense, we draw upon sociocultural approaches to human development (Zittoun, 2022), which consider health interventions as processes of identity reconfiguration and acquisition of new skills. According to this framework, three modes of knowledge support individual development: the formal system, which pertains to institutionalized knowledge transmitted during formal interventions; socially and culturally shared knowledge, which pertains to master narratives; and spheres of experience, which pertain more to individual experience as an idiosyncratic unit of quasi-knowledge.
Our methodological approach is phenomenological. We aim to understand how the experiences lived by adolescents, parents, and healthcare providers shape their perception of the intervention, their vision of the future, and how they make sense of it. We therefore adopt a Longitudinal Interpretative Phenomenological Analysis methodological approach (Smith et al., 2022). We are particularly interested in exploring how the intervention influences the adolescents’ perception of their possible selves and not simply who they are. Our qualitative inquiry is thus “infra-realist” in that it is intended to understand and change reality from within, focusing on the lived experiences, sensations, and capacities for self-invention of adolescents. This approach is phenomenological, emphasizing an understanding of the person as inseparable from their experiences and the meaning they attribute to them. It accesses the empirical realm of the world exclusively—specifically the realm of sensory experience—according to the stratification of reality within critical realism, which also encompasses the real (everything that exists, whether natural or social) and the actual (events produced when the structures of reality are activated). Infra-realist inquiry is grounded in the epistemological and theoretical foundations of recent work toward a social psychology of and for world-making (Power et al., 2023). This work highlights the dynamic and fluctuating nature of psychological and social phenomena, the intention to produce knowledge that informs everyday understandings of these phenomena, the need to engage people’s imagination to capture their experience, and the future-oriented character of our attitudes and behaviors.
Sampling/Recruitment
In accordance with LIPA’s methodological principles, we apply purposive homogeneous sampling to select the adolescents, parents, and healthcare providers involved in the intervention, while obtaining a diversity of perspectives related to this process.
The adolescents participating in the study were selected from those admitted for anorexia at UFITAA at the start of the study. The inclusion criteria for participation included a diagnosis of anorexia and an age range of 13 to 18 years. Patients presenting a “high” risk level during the initial diagnostic assessment, who required full hospitalization, were excluded. Considering the longitudinal design of the study and its phenomenological and idiographic approach, a substantial amount of data can be gathered from a small sample (fewer than 10 participants) (Farr & Nizza, 2019).
The parents involved are the legal guardians of these adolescents. The participating healthcare providers consist of professionals from UFITAA. All staff members are included, with the exception of the unit director, in order to enable participants to express themselves freely during the focus group discussions.
The recruitment procedure was carried out by a child psychiatrist or a psychologist from UFITAA, who presented the study and the proposed treatment plan to the patients who met the inclusion criteria and their parents. An information sheet was also provided to them during the diagnostic evaluation week (at the beginning of treatment). Consent was obtained from the patients and at least one parent or legal guardian prior to participation in the study.
The adolescents took part in three interviews: at the start of treatment, halfway through (at 6 months), and at the end (at 13 months). The parents took part in three focus group discussions at the same intervals.
Finally, for the healthcare providers, the study was presented by the investigator to all team members during a weekly staff meeting. An information sheet was provided to them and their consent was obtained. The healthcare providers will also attend three focus group discussions at the same intervals as the other groups.
Data Handling and Analysis
Data Handling
The participating adolescents took part in three in-depth semi-structured interviews over a year (M1 – M6 – M12). The interviews are conducted via videoconference. Studies have shown that this method promotes study adherence by reducing the costs associated with participating in interviews (time, travel, etc.), increasing accessibility, and meeting the quality criteria for qualitative research interviews, particularly in contexts of repeated data collection (Gray et al., 2020; Rupert et al., 2017).
We used the Photo-elicitation technique, which combines photography with storytelling to enable individuals to document and reflect on their lived experiences (Bates et al., 2017). Incorporating visual stimuli into interviews has been shown to shift their tone, often eliciting emotional connections to memories, yielding more meaningful narratives, and offering new perspectives (Rose, 2014). Its feasibility and acceptability in research with adolescents with a chronic condition have been demonstrated (Sibeoni et al., 2017).
For each interview, the adolescents are asked to take a photo that represents “how they feel at that moment in time: their emotions, their thoughts, their expectations”. At the beginning of each interview, the photo is projected onto a computer screen and the adolescents describe and explain what the photo represents. An interview guide (see Appendix) is then used to conduct the interview in order to cover different domains of the intervention experience (adherence, self-management, self-concept, etc.). The adolescents are then asked open-ended questions about their “possible selves” (how they envision themselves in the future and what actions they are taking to achieve that vision). This technique is derived from the international literature on possible selves in anorexia (Erikson et al., 2012). Lastly, the interview ends by asking the adolescents if they wish to add anything, if they feel that all the topics they wished to discuss have been covered, and if they are satisfied with how the interview went. Each step of the study (the three interviews) and other data collection efforts involving the parents and healthcare professionals reiterate the same process. The emphasis placed on the notions of becoming and novelty requires the use of methods that enable patients to “engage in the possible” and that aim for them to “both become aware of it and actively explore it” (Glăveanu, 2018, p. 519). While imagination is the underlying ability that enables any reflection on the future, the use of elicitation techniques (such as photo-elicitation) is essential to imaginatively create what is to become (Gergen, 2015). The adolescents are thus placed in the role of investigator of the evolution of their possible selves, through their successive narration over time and through the process of description and interpretation of their articulation with lived experience.
The parent focus group discussions aim to explore the factors that promote adaptive strategies and the development of parents’ sense of competence in supporting their child within UFITAA (see Section 7.2). Healthcare providers also participate in three focus groups, with each group comprising 6 to 12 participants. The focus of these discussions is to identify the facilitators and barriers to implementing the care system (see Section 7.3). As with the parent groups, these focus groups last approximately 1.5 hours each and are conducted via videoconference.
Both focus groups are co-facilitated by researchers trained in qualitative research (MM and LP).
Analysis
The data collected from the participating adolescents are analyzed according to the principles of longitudinal interpretative phenomenological analysis. LIPA seeks to explore how individuals navigate and interpret their experiences, emphasizing the fluidity of the phenomenon under study and each person’s capacity for change beyond fixed roles (McCoy, 2017; Snelgrove et al., 2013). LIPA thus documents experiences in their temporal dynamics based on the following postulates: the experience of change must be understood in its subjectivity, and each lived experience is interpreted by the individual based on memories of past experiences and anticipation of the future (Ashworth, 2016; Finlay, 2009). LIPA is therefore recommended for exploring a range of temporal experiences, such as life transitions and health interventions (McCoy, 2017).
LIPA adopts an idiographic approach to analysis, focusing on the complexity of each case’s developmental processes. Each adolescent’s trajectory is examined and interpreted on an individual basis. Subsequently, these intra-case analyses are compared to uncover inter-case patterns, highlighting shared mechanisms of change or stability. The analysis involves identifying descriptive, linguistic, and conceptual insights. We utilize the approach of themes tied to time points to structure the emerging themes. In this approach, participants’ progression in the temporal process is obtained by reading the entire collection of themes. Through this method, we seek to illustrate how the different experiences that appear at each time point contribute dynamically to the overall process of identity transition to adulthood (Farr & Nizza, 2019).
Transcriptions are analyzed using the seven-step process outlined by Smith et al. (2022), which consists of examining each case individually to identify personal experiential themes, and then developing group experiential themes across cases.
The focus group discussions are analyzed using reflexive thematic analysis (Braun & Clarke, 2021), which aims to develop a coherent and meaningful categorization of the discussions and information shared. This analytical framework focuses on the participants’ experiences, highlighting how they construct their perceptions and cognitions related to the intervention. We adopt this methodological framework as it better suited to this type of data collection and to the objective of gathering opinions and viewpoints, which are less directly tied to phenomenology in the strict sense.
Ethics
The study has been approved by the ethics committees of Sorbonne Paris Norh University.
We ensured to elaborate a research design that is non-stigmatizing and will not reduce adolescents to a sick status. Indeed, research on identity in health acts as a vehicle for social information on the being and becoming of the participating adolescents. The ethical issue thus consists of exploring identity from the perspective of the experience of illness in order to avoid confining the adolescent to a reductive categorization, a restricted and fixed entity that would contribute to a self-narrative that would prevent the exploration of alternatives and other possibilities. Fox and Ward (2008) recommend that studies on health identity explore “what else a body can do, what it can become”, referring to the work of Deleuze and Guattari on the concept of deterritorialization, which considers, alongside the individual, the new forms of experience, social interaction or environment that allow patients to express themselves, entirely liberated from the constraints of any health condition or social discourse. The exploration of possible future selves should promote adolescents’ expression of self-determined identity.
Finally, the psychologists at UFITAA are available to discuss any questions that may arise during the study and any concerns that participants may have. Participants are informed of the availability of psychologists for this purpose.
Rigor
We rely on the quality criteria established by Smith et al. (2022) for IPA and those by Braun and Clarke (2021) for Reflexive Thematic Analysis (RTA) to adopt a rigorous approach to qualitative research. Our research project began with a reflexive process on our theoretical assumptions, leading us to define an ontological framework (critical realism), an epistemological framework (contextualism), and an axiological framework (the possible), all presented in the Method section. We have ensured adherence to all stages of a qualitative study according to these approaches: state of the art, formulation of a research question, sampling strategy, data collection techniques suitable for the population and research objectives (photo-elicitation), analytical framework, and interpretation of results.
Furthermore, the participatory approach of our study, through the involvement of stakeholders in the steering committee, enhances the focus on the needs and experiences of the concerned populations, as well as on producing knowledge aimed at operationalizing intervention strategies.
Finally, our study is framed within a triangulation approach. Firstly, we employ source triangulation by collecting data from all stakeholders involved in the intervention: adolescents, parents, and healthcare providers. Secondly, we utilize method triangulation by combining individual interviews with adolescents using a phenomenological approach and focus groups with parents and healthcare providers using reflexive thematic analysis.
Full Copies of Interview Schedules and Focus Group Schedules/Fieldwork Plans
Interview Guide with Adolescents

Interview Guide with Parents

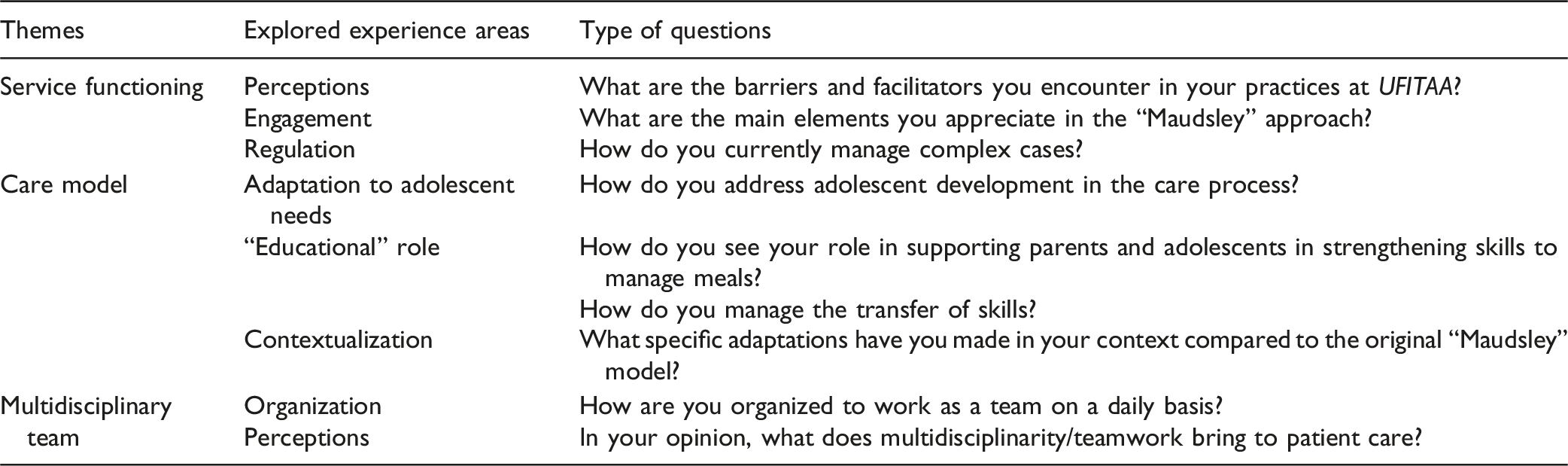
Interview Guide with Healthcare Providers
Schedule

Footnotes
Ethical Considerations
The study has been approved by the ethics committees of Sorbonne Paris Norh University (File No. 2023-023).
Consent to Participate
The informed consent form was signed by the participants before taking part in the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Université Sorbonne Paris Nord.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and analyzed during the current study are not publicly available due to participant confidentiality and anonymity considerations.