
Abstract
Diabetic foot ulceration (DFU) is a complication of diabetes which contributes to global public health burden. In Afro-Caribbean populations, increasing diabetes incidence has resulted in increased likelihood of DFU and its dreaded sequelae of lower limb amputation. We describe the use of an interpretivist qualitative approach with aspects of discourse and cultural theories, to develop a video-based health education tool to increase understanding in Afro-Caribbean populations of the signs and symptoms of DFU. Focus groups, dyads and triads were conducted with persons living with DFU in a low-resourced health care setting. Modified verbatim transcripts were subject to inductive coding with application of discourse and culture theories to identify and explore themes around: illness; perceptions of illness; and preferred methods for knowledge transfer. The study unearthed the role that cultural and historical narratives of DFU play in influencing access and utilization of health care and informed the creation of a culturally sensitive tool that could improve uptake of healthcare information by marginalized populations.
Keywords
Introduction
Diabetic foot ulceration (DFU) is a complication of diabetes of public health significance, with 9%–34% of all persons living with diabetes estimated to develop foot ulcers sometime during their lifetime (Mcdermott et al., 2024). A DFU is any “break of the skin of the foot that includes minimally the epidermis and part of the dermis” (Van Netten et al., 2023). Risk factors for DFU may include foot deformities, peripheral arterial disease (PAD) and peripheral neuropathy (PN) (Wang et al., 1049). Black populations (including diaspora Afro-Caribbean populations) and those of lower socioeconomic groups in the United States, face disproportionately worse outcomes (higher lower extremity amputation) than white populations (Armstrong et al., 2024) with increased risk of amputations among black populations (Xu et al., 2024). In the United Kingdom, prevalence of DFU is lower in Black populations (2.7%) than European White populations (5.5%) (Abbott et al., 2005); despite a higher diabetes burden in Blacks, second only to South-Asian ethnicities (Bennett et al., 2015).
Within Caribbean populations, the incidence of diabetes is estimated at 9.6% according to 2014 estimates (Yisahak et al., 2014); and Afro-Caribbeans have been noted to have higher diabetes burden than African Blacks and White ethnicities, second only to South-Asian ethnicities (Bennett et al., 2015). DFU also disproportionately affects persons of Afro-Caribbean ethnicity (Gulliford & Mahabir, 2002), compared with persons of Indo-Caribbean ethnicity according to a single Trinidadian study. A study at a tertiary medical clinic in Jamaica, found that one in every eight persons had diabetic foot disease (Ferguson et al., 2013).
Various challenges exist within Caribbean communities in addressing diabetes and diabetic foot. Many health systems in the English- Speaking Caribbean use a Primary Health Care approach with free care at the point of access, in keeping with “health for all” as proposed by the World Health Assembly in 1979 (Carr, 1985), and echoed in the new WHO health investment case 2025-2028 in pursuit of Universal Health Coverage (World Health Organisation, 2024). However, socio-cultural and health systems-level barriers exist and interact, creating inequities across public and private healthcare sectors (Williams et al., 2017). Development of culturally appropriate effective primary care tools for prevention and management of DFU are lacking and given the burden of disease and knowledge gaps from literature related to risk factors, the development of such a tool is imperative (Lovell et al., 2024).
Cultural barriers to diabetes education largely point to the lack of cultural salience of health information and a conflict of traditional medical models of self-management and culturally normative management practices. This results in discordance of efforts of healthcare practitioners and persons living with diabetes (Moore et al., 2022). System and logistical challenges to care for persons with diabetic foot also lie in the mistrust of local health systems, and preferences for traditional medicines, instead of Western medicine. This challenges the acceptance of allopathic methods of health education by Afro-Caribbean populations (Lovell et al., 2025).
These barriers therefore present an opportunity for the creation of a culturally competent tool to meet the needs of diabetic foot education, using a qualitative methodology through theories of discourse and culture.
Theoretical Frameworks
We adopted interpretivism as the research paradigm (Denzim & Lincoln, 2013). Aspects of discourse theory (largely based on the sociocognitive approach) (van Dijk, 2008) and culture theory were used for interpreting the results after thematic analysis. Discourse theory explores how “multiple utterances fit together to specify meaning” and includes wide ranging phenomena of speech to add meaning and context to a linguistic piece (Bickmore & Giorgino, 2006). Critical discourse analysis (CDA) evaluates the social conditions of the discourse and is a qualitative analytical tool for exploring the construction and maintenance of legitimization of social inequalities through the discourse (Mullet, 2018; van Dijk, 2008;). Culture theory acknowledges that people do not exist in isolation, but rather the inner self interacts as expressed by motivators (e.g. values and beliefs), with the external, inclusive of one’s activities (e.g. actions and normative routines) and materiality (e.g. infrastructure and tools) within a community (Stephenson J., 2023). We therefore borrowed aspects of both discourse and culture theory to create a new framework for understanding how to address the issues and doubts surrounding accessing healthcare for DFU, including power-based structures and biases that may delay access and perpetuate health inequalities.
To date there have been no DFU lived experience studies using both discourse and cultural theories within the qualitative context. This is important in the deconstruction of the narrative to address the gap in designing and implementing health education within Afro-Caribbean populations.
Setting and Historical Framing
Cultural Perspectives
The research is positioned within the primary care landscape of Barbados, a small island developing state within the Eastern Caribbean. Afro-Caribbean/Black is the predominant ethnicity (92.4%) with most of the population being descendants of enslaved Africans (Government of Barbados, 2025). Ethno-botanical practices are deeply engrained in many Afro-Caribbean societies where many of the healing traditional remedies are largely West African in origin (Vujicic & Cohall, 2021). The balance between “hot” and “cold” and use of “bush teas” which are still practiced today are rooted in African traditions such as the Yoruban community from Nigeria (Sutherland et al., 2014). Unfortunately, the meaning of traditional/ cultural medicines to the Caribbean peoples was virtually erased or suppressed with development of modern/ allopathic medicines (Sutherland et al., 2014). Therefore, most of these traditions are just passed down through oral history in communities (largely rural) and re-enactment, with increased gaps between users based on socioeconomic and educational backgrounds (Vujicic & Cohall, 2021). The fear of amputation and equivalence of DFU and limb loss is also a psychological barrier to care transcending different cultural groups. As noted previously the Barbadian population is largely descendant from enslaved Africans, oral history of lower limb amputation as punishment for escape from slave plantations also colors the mistrust of medical professionals for amputation and the desecration of this process on the human body (Kennedy, 2015). Therefore, the marriage of discourse and culture theories is most aptly positioned to understand the perspectives of communities that may be marginalized by healthcare systems.
Health Systems Setting
Although classified as a high-income country by the World Bank (World Bank), Barbados is still a small island developing state which faces economic vulnerabilities (based on high tourism dependency), environmental and social challenges (due to climate change effects and resultant increased non-communicable disease burden) (Campbell et al., 2024). Primary and tertiary healthcare are both free at point of access for Barbadian citizens and permanent residents, with the Beveridge model applied; funding through taxation provides financing for the public health system. As a result, purely economic barriers of access to care within this context are arguably minimal (Planning and Research Unit Ministry of Health of Barbados, 2015). However, rates of diabetes (18.7% incidence in 2021) (International Diabetes Federation) and DFU are still high (one year period prevalence was 14.7% (10.5, 20.1) at a local diabetes clinic) (Lovell et al., 2022). Estimates of lower limb amputation, a sequela of DFU have also been high with annual incidence of diabetes-related amputation of 936 per 10 5 population (Hennis et al., 2004). Therefore, traditional methods of health promotion and education involving diabetic foot may not be as effective in this population (Lovell et al., 2025).
Methodological Reflections
There is previous work reviewing lived experiences in the Barbadian population (Lovell et al., 2025), however methodological and conceptual gaps in knowledge exist. The analysis of DFU lived experience data through this lens of discourse and cultural theories to inform the design of a public health intervention has not been done and is the focus of this paper. The theoretical generalizations that may be identified from the stories of persons in the local context undergoing the health challenge, can be lost if analysis is limited to traditional qualitative stances that may not blend or merge philosophical paradigms or theories that inform.
Data Collection and Analysis
Participant Profiles

Site key
(1) Multidisciplinary center.
(2) Urban/Suburban facility.
(3) Rural facility.
(4) Rural facility.
(5) Urban facility.
Inclusion criteria included persons living with diabetic foot ulcer, medical capacity to provide consent and age over 18 years. Persons who did not have medical capacity to provide consent were excluded. Participants were recruited after identification of persons fitting the inclusion criteria by wound care nurses at the sites. Eligible persons were then consented by the researcher LL, prior to LL conducting interviews in clinical rooms within the polyclinic with researcher LL and participants.
A theory-informed interview guide was developed by the researcher LL, a female, trained postgraduate researcher who currently practices clinical medicine in the field of diabetic foot. Theories of planned behavior (Bosnjak et al., 2020) were used to develop the interview tool of 12 questions, which explored three major areas surrounding diabetic foot: exploration of diabetic footcare knowledge; exploration of the diabetic foot in the Barbados context and amputation and limb loss.
FGs with semi-structured interview questions provided rich descriptive texts where meaning was also generated by interpersonal dynamics of the group. All interviews were conducted in the English language. Focus groups included between two to four participants based on the available population fitting the inclusion criteria at each location with a total of 15 participants throughout four groups with no attrition. Study locations were purposive to provide a range of the demography of the Barbadian health system- rural, suburban/urban and mixed (multidisciplinary centre).
Table 1 shows the participant population across the sites.
All data collection (audio recordings with field notes), transcription and analysis activities were completed by one researcher with another completing assisting with manual double coding of the first 2 transcripts, generating inductive codes and participating in data condensation discussion using Atlas. ti 25 (GmbH, 2023) leading to the formation of themes as shown in Figure 1 below. Qualitative Data Analysis Process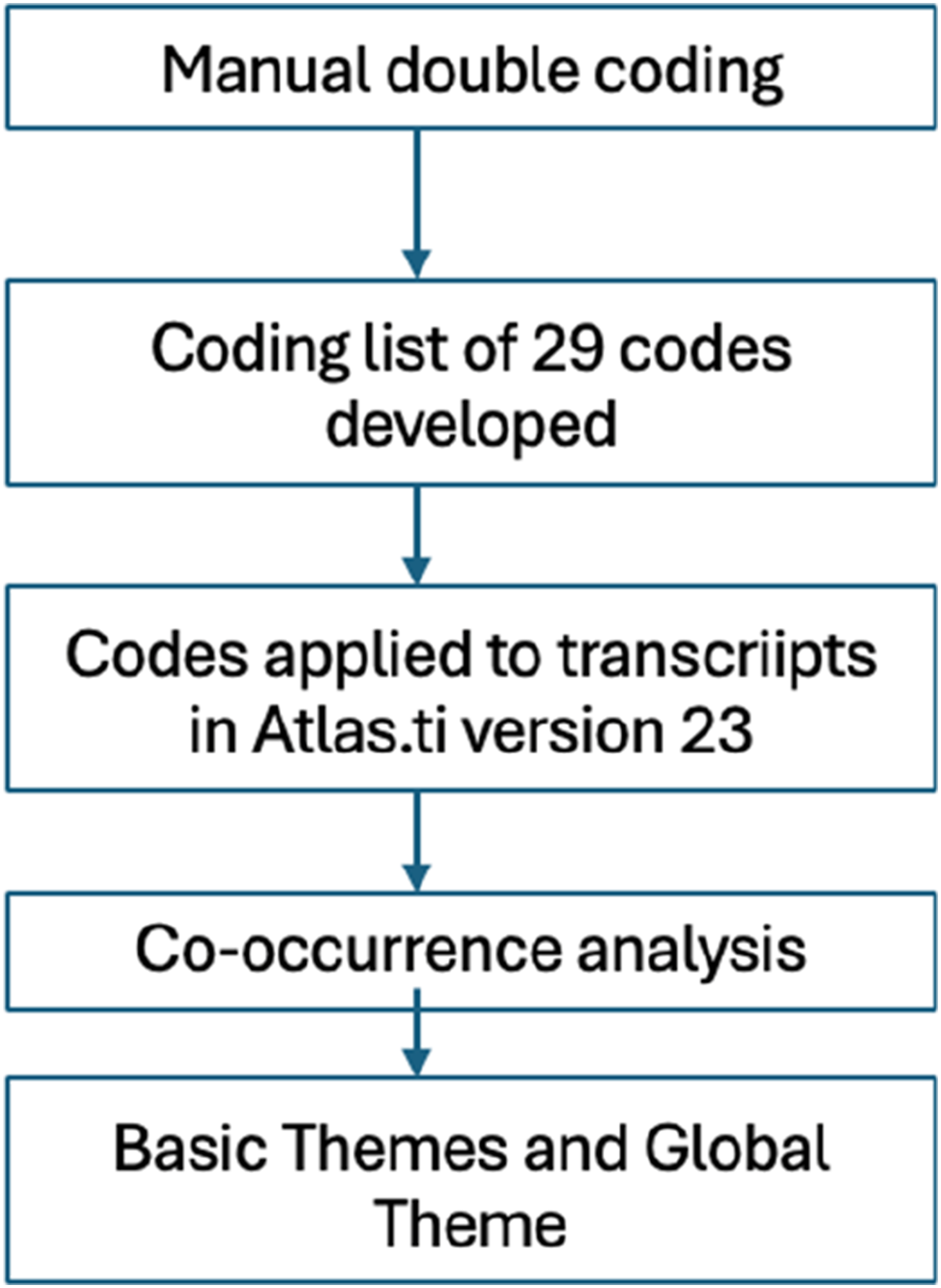
Following data collection, the basic themes relevant to discourse and culture theory were developed. These are presented briefly with a direct segue into their application into the design of the health education tool design. Themes were derived from using inductive coding via a 29-item coding framework (Green & Thorogood, 2018). Data saturation was achieved when no new emerging themes were established.
Trustworthiness of the data was also supported through adoption of transferability, credibility, confirmability and dependability (Bingham, 2023). Triangulation with the data, researcher and reflection of the current literature and social cognitive theory aided in providing rigor through transferability, credibility and confirmability with researcher journalling throughout the qualitative process to add dependability.
Researchers’ Positionality
The researchers’ approach this work as two physicians within the primary care and public health landscape of Barbados. One researcher works within the primary care landscape almost exclusively so reflective journaling was used to reduce any biases. Their research from this perspective is aimed at improving patient outcomes through finding culturally sensitive methods that work through greater understanding of the voices served by the work. Another researcher is an applied public health qualitive researcher with interests in life threatening illness and empowering people through communication.
Findings
Three basic themes emerged from the data: “The Doctor is My Teacher”, “Respect for Traditional Medicine” and “Fear and Trust, the Subliminal Factor”.
Basic Theme 1: “The Doctor is My Teacher”
Participants trusted information given by medical professionals especially, considering diabetes status. Fact checking traditional remedies and valuing advice from medical professionals (doctors and nurses) was seen. “Because I am diabetic, I don’t know if that (a traditional/natural treatment) will agree (will work) so when I come here, and they put something on it I know that she (doctor or nurse) will tell me what it is and how to do it.”
P1-1, FG4 (71-Year-old Retired Salesclerk) “I would put some trust in the nurses too… letting you know what you should do or not.”
P1, FG5 (54- Year-Old General Worker) “Well, I think I could go to the doctor, and they could share that information (diabetic foot education)”
P1, FG3 (58-year-old male)
Participants also recounted that information sharing in one-to-one interactions was preferred. This may have also been due to literacy barriers some elements of the population may face. “Yes anything (video or pamphlets) so…everybody aint (isn’t) going to come out and tell you that they got problems reading and they aint (will not) going to want you to know that. Sometimes that’s how some of the problems does come up too.”
P2-1, FG4 ( 67-Year-old Female)
Participants also expressed information gathering through conversation as a preferred media, either conversationally in a doctor-patient interaction or through promotion campaigns on mainstream media. “Usually when you listen to the radio and stuff if there are any programmes or sessions about diabetes and stuff, I would listen…”
P2, FG5 ( 58-Year-old Female) “It (information sources) would have to be the radio, your computer, look online, and you’ll learn things.”
P1, FG 2 (58-year-old male)
Basic Theme 2: “Respect for Traditional Medicine”
Despite the narrative pointing to medical professionals giving the best information, participants alluded to trust in neighbors or members of their communities who were able to provide opinions on traditional remedies. “You see when my mum was good, we used to drink bush tea all the time and she used to eat all sorts of things, and her blood sugar used to be good”.
P3, FG 1, (50-Year-old Male) “I went into a health shop and I tell the girl I got a wound and its taking long to heal….and she ask if anyone tell me about zinc. And she said if no one told me about zinc then it would heal from inside so that’s what I am doing now…”
P1, FG3 (58-year-old male)
Basic Theme 3: “Fear and Distrust- the Subliminal Factor”
The risk of amputation as a sequalae of DFU also posed a barrier sometimes to accessing the healthcare system. The perception that admission to hospital equated to limb loss “LL: What have you heard that makes you scared? Participant 1: Everything! Them is Cut Cut, Cut, Cut!”
Exchange between researcher LL and P1, FG5, 54-year-old female “Meaning that at the clinic you don’t get the proper attention…and eventually you get your foot amputated” (Referring to public healthcare system).
P2, FG3 79-Year-old Female
Use of Theories and Development of the Tool
The researchers acknowledge that culture is a distinctive pattern of activities, motivators and materiality shared by a group of persons within dynamic ensembles (Stephenson J., 2023). Discourse theory also reveals that ensemble is shaped by the same culture and cannot be divorced from how information and stories are shared in communities. The basic themes therefore tell a story of arguably suppressed cultural norms within a modern medical society with use on neighborly informal discourse to understand health phenomena and guide health care seeking behaviors.
When discourse and culture theories were applied to the interpretation basic theme features of an acceptable health education tool emerged captured under a global theme: “Video Media- Wha Diabetic Foot Education Look Like fuh Me”. Video-based multimedia was derived to be the best format for a culturally competent health education tool..
From Theory to Video
The Presenter Image and Speech
From the data, the perceived lack of communication from healthcare professionals on diabetic foot and the possible power imbalances (skewed towards health professionals) that are at play in a Barbadian health system resulted in participants resorting to neighborly conversations for health education. Participants also highlighted multimedia as a tool to receive information (e.g.television, radio); as traditional models of health promotion ( e.g. paper based leaflets) did not resonate with this population. Speech used to construct meaning within a social context is a tenet of discourse theory (te Molder, 2009) and this was reflected in the data which found that participants required information from a medical professional, despite power differences, as well as persons they could trust or relate to in the community (the neighbor concept). However, the speech (utterances and linguistic style which is predominantly in standard English with medical jargon) of medical professionals in the current environment did not adequately resonate with the audience, thus providing a disconnect, although still preferred.
Resonance with Cultural Norms
Culture theory is inextricably linked to discourse theory in this context. The motivators within the framework of culture theory encapsulate the “beliefs, values, norms aspirations and forms of knowledge and understanding” within this framework (Stephenson, 2023). Thus, understanding the meaning of the text must be taken in context of the motivators of the actors in Barbadian context. The Barbadian context of diabetic foot is against the background that most persons equate diabetic foot to the dreaded amputation (Lovell, Laura, Campbell, & Greaves, 2025). Therefore, any experiences shared would be colored against that background and therefore materials developed for health promotion need to address this potential fear.
Shareability
Easily shareable and accessible media options were also important as participants had a wide range of information sources. Written words through booklets or posters were not seen as best health education methods by participants as some noted that lack of literacy or comprehension of paper-based materials were barriers to education. Therefore, a video entitled “Red Light Green Light 1-2-3” using a traditional Caribbean game with the same name, was designed to relay the message of diabetic foot education. “Red Light Green Light 1-2-3” is a rhythmic, easy to remember and transgenerational game engrained within the Caribbean cultural landscape and is also tied to a traffic light system which offers cue to action for DFU prevention and care.
Video Development
Video development used traditional Barbadian linguistic style to simulate a neighborly interaction between two Barbadian female adults and a known diabetes specialist doctor. The doctor in the video explains symptoms and signs and how to access care for diabetic foot. The setting of the video was a local freedom park, known by almost all locals to represent separation from colonial systems and recreation to reflect positive and empowering positions. The opening video scene took the form of two lay people/ neighbors (non-medical professionals) discussing diabetic foot. This was scripted to allow for Barbadian linguistic style (Bajan dialect). In these scenes the subject-verb agreement was changed from classic British English to present continuous tense and melodic intonations in keeping with a familiar Bajan conversational tone.
Gender roles were also considered, and it was decided that the health professional sharing the information should be female given the local health system where half of doctors are women and over 80% of nurses (Knaul et al., 2022). The figure below details two scenes from the video and the Red-Light Green Light 1-2-3 model (Figure 2). Scenes From Red- Light Green Light 1-2-3. (Left Top: Neighbor Conversation About DFU; Left Bottom: Doctor Conversation (Female); Right: Red Light Green Light Explained)
The doctor in her explaining, introduces listeners to DFU and outlines signs of accelerating disease, using a traffic light system with clear points for action should a viewer identify a possible sign in themselves.
In total the video is three and a half minutes and end with an empowering narrative which is designed to move the listener from a contemplation to action phase in the context of the transtheoretical model of behavioral change. “Take control of your feet and take control of your diabetes!”.
Limitations
The limitations of this study are largely contextual. It was conducted in small island setting where one of the researchers is deeply embedded in the field of diabetic foot clinical management. Although all efforts to avoid participants who had prior doctor-patient relationships with the interviewer were made, participants may have known of the researcher and therefore this may have colored their responses to some degree. Additionally, treatment at various healthcare centres is varied within the healthcare system and this may have differences on how participants experience care living with diabetic foot.
Conclusion
The use of cultural theory and discourse theory provides the base of a viable framework for establishment of health education tools within Afro-Caribbean settings. The development of the “Red Light, Green Light 1-2-3” tool from qualitative exploration of these settings can be a transferable method for establishing health education in marginalized groups.
Footnotes
Ethical Consideration
This study was approved by The University of the West Indies/ Ministry of Health and Wellness of Barbados Ethics Committee (Ref: CREC-CH.00124/11/2022) in accordance with the Declaration of Helsinki (World Health Organization, 2024).
Consent to Participate
A copy of the informed consent form is available in the supplementary material for this manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Additional data may be available upon reasonable request by contacting the corresponding author.