
Abstract
Global health and social research have advocated a requirement for community-engaged research methods to better address the needs of minoritised groups. However, conventional research practices, often influenced by positivist traditions, tend to prioritise convergence, overlooking critical tensions within and across data sets. Resultantly, changes within healthcare and policy have not been matched with parallel benefits for minoritised groups. These disparities underscore the need for research methods that can adequately give voice to multiple stakeholder groups and understand these discrepancies. In response to these issues, the present study introduces the novel development of the Qualitative Triangulation Framework (QTF). Extending previous triangulation methodologies, the QTF provides a framework for exploring both agreement and disagreement within and across qualitative data sets from multiple stakeholder groups. Developed in the context of research with trans and gender diverse (TGD) youth, the QTF was valuable for revealing both inter- and intra-group differences in what they deemed as health-enhancing. Thus, the QTF enhances the actionability of qualitative findings, allowing for the development of more effective policy recommendations that can better address these overlooked tensions. Beyond its application to TGD healthcare, the QTF provides a replicable model for amplifying minoritised voices in research with other underserved populations, advancing equity in healthcare research and practice. Extension of the QTF for systematically exploring competing perspectives beyond minoritised groups are also discussed. Overall, the QTF represents a significant advancement in qualitative methodologies, offering a powerful tool for researchers seeking to navigate complexity, reconcile conflicting viewpoints, and drive meaningful change.
Introduction
Qualitative research has long been a critical tool for amplifying the voices of individuals and communities whose experiences are often overlooked in mainstream discourse (Lim, 2024). These minoritised groups include, but are not limited to, ethnic minorities, LGBTQ + individuals, people with disabilities and socioeconomically marginalised populations (Cheraghi-Sohi et al., 2020). These minoritised groups have historically been underrepresented in research or included in ways that fail to adequately reflect their lived realities (Collins, 2000; Crenshaw, 1991; Hassler et al., 2024). While research has begun to increase the representation of minoritised experiences (e.g., Lovell et al., 2023; Zacharias & Aitken, 2025), positivist epistemologies that dominate research practices have limited the utility of these research findings for creating actionable and meaningful change (Campbell et al., 2020). This is because positivism strives for objectivity, reliability and generalisability which can oversimplify complex human experiences (Omodan, 2025).
Despite qualitative approaches advocating for an interpretivist stance (i.e., a focus on context, subjectivity, and multiple perspectives for understanding human behaviour), positivism creep (the subtle infiltration of positivist principles in research practices; Braun & Clarke, 2022) can narrow the scope of knowledge production. For example, positivism can encourage the quantification of qualitative research, whereby increased pressure to translate rich qualitative findings into measurable variables often reduces complexity and meaning (Braun & Clarke, 2022; Lee, 2025; Omodan, 2025). An emphasis on generalisability can also lead to a tendency to favour broad, widely applicable conclusions over context-specific insights (Braun & Clarke, 2022; Lee, 2025). Collectively, this can lead to a devaluation of critical and interpretative approaches, favouring dominant perspectives (i.e., ideas generally expressed by the group studied) while sidelining more situated and experiential knowledge (i.e., differential experiences within the group studied; Campbell et al., 2020; Ohmer et al., 2023).
This emphasis on dominant perspectives within qualitive enquiry has increased the marginalisation of minoritised voices, either through tokenistic inclusion, selective interpretation of data, or methodological approaches that do not fully account for power imbalances between researchers and participants (Lim, 2024). In response, scholars have increasingly advocated for community-engaged, participatory, and decolonial approaches that centre knowledge and agency of minoritised communities (Ohmer et al., 2023). These approaches seek to challenge traditional hierarchies of knowledge production and ensure that research is conducted with, rather than about, these communities.
Minoritised Voices in Healthcare Research
One area of research that particularly overlooks the needs of minoritised communities is healthcare. Within healthcare research, the need to prioritise minoritised voices is especially urgent given persistent health disparities and systemic barriers to care (Kerr et al., 2024; Macias-Konstantopoulos et al., 2023; Vela et al., 2022). However, healthcare research remains heavily influenced by positivist traditions, which privilege quantitative metrics and outcome-based evaluations over the lived experiences of patients (Park et al., 2020; Smith & Hasan, 2019). This positivist emphasis risks reducing minoritised experiences to statistical categories that may fail to capture interpersonal dimensions of healthcare inequities (Ohmer et al., 2023).
In an effort to address these disparities, global health research is increasingly drawing on community-engaged methods (i.e., methods that draw on the knowledge of the target population) to improve the development of healthcare pathways that better meet client needs (Hickey et al., 2022). Advocated by the National Institute for Health Research (NIHR), the requirement for community engagement within the research they fund reflects the commitment of funding bodies towards an evidence base in line with the call named “Leave No One Behind”, championed by Sustainable Development Goals (NIHR, 2019). The aim of this UK initiative is to improve the health and wellbeing of minoritised populations (NIHR, 2019), defined as individuals who are socially separated or seen as subordinate in comparison to other members of society (Wingrove-Haugland & McLeod, 2022).
Despite the widespread importance of community-engaged research methods, attested to by the development of multiple guidelines and standards (e.g., Bedson et al., 2020; World Health Organisation, 2017; also see Hickey et al., 2022), understanding what constitutes effective community-engaged research is lacking (Hickey et al., 2022; Kantamneni et al., 2019). Moreover, heedless of the intended meaning of community-engaged research methods for addressing health disparities between minoritised and non-minoritised populations (NIHR, 2019), we often see inclusion without voice (Pratt, 2019). In essence, minoritised individuals are present within research discussions, but their opinions and perspectives are not afforded equal weighting in comparison to non-minoritised individuals (Da’as & Slobodin, 2024; Onwumere et al., 2023). This can result in the development of healthcare services which, whilst anticipated to address the needs of minoritised communities, fall short of addressing health disparities between minoritised and non-minoritised groups (Han et al., 2021; Horton, 2024).
Evidencing this matter, research with ethnic-minority communities frequently notes misunderstandings and tensions between service users and professionals (Gaya-Sancho et al., 2021). Similarly with LGBTQ + communities, training programmes on LGBTQ + health are suggested to improve the knowledge, attitudes, and skills of health professionals (Damery et al., 2025), yet LGBTQ + individuals consistently report health inequities and type-cast treatment plans that do not consider intra-group differences (Hascher et al., 2024; Kelsall-Knight, 2021; Subirana-Malaret et al., 2023). These are just two examples. Nonetheless, it indicates how professionals may misunderstand the needs of minoritised groups, where healthcare policy changes are not matched by parallel benefits for health outcomes. These disparities underscore the need for research methods that can integrate, and adequately give voice to, multiple stakeholder groups. This would mark a step towards reducing the marginalisation of minoritised groups within healthcare research and practice.
Reducing Marginalisation Through Triangulation Research Designs
Triangulation offers a promising pathway to integrate multiple perspectives and navigate divergent understandings between stakeholders in research. Triangulation within research refers to the process through which multiple methods and perspectives are used to study a topic (Heale & Forbes, 2013). Typically, triangulation has been used for validating findings, whereby converging results from different data collection methods or samples enhance the rigour of a research study (e.g., using qualitative data to better substantiate the processes that underly observed quantitative outcomes; Heale & Forbes, 2013): a positivist approach. However, divergent perspectives between data sets can offer more insight into novel ways to understand a topic (Campbell et al., 2020; Heale & Forbes, 2013). Nonetheless, divergent perspectives are rarely reported within triangulation research (due to positivism creep), and, when they are, they are often presented without further interrogation of their underlying meaning (Howe, 2012; Morgan, 2018; Morse, 2015). This is problematic because disparate findings can be indicative of underlying tensions and differential expectations between two or more groups (Campbell et al., 2020; Farmer et al., 2006; Greene, 2007; Sands & Roer-Steir, 2006). For example, when findings do not converge, particularly where they have implications for policy, it can lead us to question which findings are credible and actionable (Campbell et al., 2020). In this way, triangulation is not just a method of data integrity, but it also presents an opportunity to evaluate what data collection methods and population samples offer the most usable data for implementing beneficial policy changes: an interpretivist approach.
Distinctly, within social sciences and health research, the variable nature of social phenomena means that there are actually more ways for data not to converge than to converge (Campbell et al., 2020; Flick, 1992; Mathison, 1988). Consequently, the positivist notion that triangulation is a method through which research findings can be verified or falsified limits the utility of triangulation for better understanding social phenomena. Instead, then, there is an increased call for research adopting triangulation methods to move beyond documentation of convergence, and instead begin to challenge the notion of clean-cut research findings (Campbell et al., 2020). By explicitly analysing both convergences and divergences through an interpretivist lens, triangulation allows researchers to understand why stakeholders interpret the same issues differently (e.g., why changes in LGBTQ + healthcare policy do not improve healthcare experiences for LGBTQ + individuals) and how these interpretations influence healthcare practices.
Limitations of Existing Triangulation Methods
Although existing triangulation methods have permitted researchers to integrate multiple methods and perspectives, as mentioned, these are largely focused on convergence rather than divergence (Campbell et al., 2020). This can be limiting as it does not allow researchers to appreciate the complexity of experiences within the group they are studying (Campbell et al., 2020). Further, while some triangulation methods have begun to explore the role of divergence, these too have their shortcomings.
For example, Campbell and colleagues (2020) developed a triangulation system that built on the work of prior triangulation theorists (e.g., Denzin, 1978; Farmer et al., 2006; Sands & Roer-Steir, 2006). Their aim was to coalesce multiple strategies from previous research for interrogating divergent data points across multiple methodologies and stakeholder groups. However, given the copious amounts of data in Campbell and colleagues’ (2020) study, themes from qualitative data were used as key arguments/data points to be triangulated with other forms of data (e.g., quantitative and archival records). Although practical, it meant that their triangulation system was applied after data analysis. This overlooks divergent data points that may have been present within qualitative data, for instance, intragroup differences that may have been filtered out through the convergent nature of qualitative theme generation (Braun & Clarke, 2022; Mathison, 1988).
In a similar vein, Reicher and Sani (1998) introduced Structural Analysis of Group Arguments (SAGA). SAGA aims to identify the different arguments that ingroup members construct to justify the in-group stereotype (i.e., what ingroup members should be doing, thinking, and feeling: Haslam et al., 2018). In short, it considers whether ingroup members have divergent perspectives on what thoughts and behaviours constitute their social identity. However, although SAGA identifies key divergent arguments between group members, it does not propose strategies for interrogating potential reasons why we might observe this divergence. This is a significant drawback, particularly in comparison to Campbell and colleagues’ (2020) triangulation methods, because it limits researchers’ ability to understand why group members disagree, and therefore how this dispute can be resolved (Campbell et al., 2020; Farmer et al., 2006; Greene, 2007; Sands & Roer-Steir, 2006). Furthermore, dissimilar to prior triangulation theorists (e.g., Campbell et al., 2020; Denzin, 1978; Farmer et al., 2006; Sands & Roer-Steir, 2006), SAGA does not consider the salience of an argument (i.e., is it common within one group, across both groups, or neither?), just that an argument exists. This is limiting because they may analyse/present arguments that do not represent the group at large. Instead, they may only demonstrate individual meanings. Resultantly, SAGA is unable to determine whether arguments are common across groups or within groups and, therefore, how divergent understandings can be best resolved (e.g., is there disagreement among minoritised group members, or between minoritised groups and professionals working with them?).
Overall, these challenges reflect the requirement for a qualitative data triangulation method that explores divergence and convergence on a level closer to the original data (i.e., during the data analysis stage of qualitative research rather than post analysis), whilst simultaneously considering the salience of key arguments within and across stakeholder groups. Such a method would enable researchers to focus on meaningful divergences both within and across stakeholder groups to understand how they can impact healthcare outcomes. This paper presents the Qualitative Triangulation Framework (QTF) to address these aforementioned limitations.
Development and Application of the Qualitative Triangulation Framework (QTF): Healthcare Experiences of Trans and Gender Diverse Youth
To illustrate how the QTF was developed, as well as its potential for uplifting minoritised voices within healthcare research and practice, the context in which the QTF originated is presented.
Context
The QTF was developed to assist and enrich the authors’ analysis of data generated from a research study. The study aimed to explore the healthcare and social engagement experiences of trans and gender diverse (TGD) youth, meaning young people whose gender identity differs from the sex assigned to them at birth (Crowley et al., 2021), with a specific focus on how social interventions, such as Social Prescribing, could improve their health outcomes. Such interventions could complement existing Gender Identity Clinic (GIC) services by addressing non-medical aspects of care. This may be particularly valuable for individuals who do not wish to medically transition or are navigating extended GIC waitlists (Cipolletta et al., 2017; Hughto et al., 2017; Radix, 2016). These interventions also provide vital support for individuals whose health precludes them from accessing medical care (i.e., because they are deemed ‘unfit’ for medical intervention; Staras et al., in preparation). The development and utilisation of the QTF was felt to be important given the marginalisation of TGD young people across multiple aspects of their life, including their healthcare experiences, which are often misunderstood by professionals (Horton, 2022, 2024). Explanation of this marginalisation is provided in further detail below to provide key contextual information for understanding the utility and application of the QTF.
Marginalisation of TGD Youth
While TGD youth face pervasive marginalisation across many aspects of their lives (Jones et al., 2020, 2021), healthcare settings exacerbate this marginalisation, where barriers such as infantilisation, doubts about their mental capacity to consent, and mandatory parental approvals impede their access to gender-affirming care (Carlile, 2020; Horton, 2024; Hughto et al., 2017, 2021). This lack of access not only hinders timely care but also restricts social engagement and authentic gender expression, leading to broader exclusion from societal participation (Huit et al., 2024; Robards et al., 2020; Staras et al., in preparation.
These challenges are mirrored in healthcare research and practices, where systemic changes often fail to adequately incorporate TGD perspectives (Horton, 2024). For example, recent shifts in the UK such as decentralizing care from youth Gender Identity Clinics (GICs) to regional multidisciplinary teams (NHS, 2023b; 2023a) have inadvertently created disjointed care pathways (Staras et al., in preparation). Poor coordination between services has resulted in disruptions to continuity of care, heightened uncertainty, and elevated anxiety for TGD youth (Staras et al., in preparation; Horton, 2024). Resultantly, young TGD people’s healthcare needs are largely unmet (Horton, 2024), indicated by healthcare policy ‘improvements’ not being reflected in TGD youth’s health outcomes (Jackson et al., 2023; Scheim et al., 2024). This highlights how the perspectives and needs of TGD youth are often overlooked during the planning and implementation of such policies (Horton, 2024; Jackson et al., 2023; Scheim et al., 2024).
Crucially, this disconnect extends beyond practical healthcare delivery to fundamental differences in how young TGD individuals and healthcare professionals understand and articulate key issues in the UK. Professionals often frame challenges in terms of logistical barriers such as waitlists and resource shortages, while TGD youth emphasize the psychological toll of navigating these systems (Staras et al., in preparation). This misalignment can result in well-meaning but ineffective interventions, as healthcare policies frequently address surface-level symptoms rather than the deeper systemic and emotional challenges faced by TGD youth (Horton, 2024). Addressing this gap is critical for ensuring healthcare reforms genuinely enhance outcomes for this vulnerable population.
Logic Behind the QTF
Given these differences in perspectives between young TGD people and the professionals working with them, we anticipated that the QTF would provide a framework for understanding where these two stakeholders agree (converge) and disagree (diverge). For example, in the context of TGD healthcare issues, divergent data might reveal why professionals perceive waitlist reductions as a solution, while TGD youth highlight ongoing struggles with bureaucratic processes that extend far beyond initial healthcare access. These insights can help identify critical gaps and tensions, such as unmet psychological needs or unacknowledged systemic biases that hinder the effectiveness of current policies.
For TGD youth, this approach is essential to ensure their voices are neither ignored nor over-simplified in research aimed at improving their wellbeing. Indeed, an over-emphasis on producing efficient and actionable research (due to positivism creep) can mean that even the most well-intentioned researchers who aim to capture complex lived experiences may over-simplify their findings (Keenan, 2022). Resultantly, the QTF granted value in both convergence and divergence that allowed the research to challenge the notion of clean-cut research findings (Campbell et al., 2020). Instead, the nuanced understanding that the QTF proffered was critical for comprehending how to develop truly inclusive and effective healthcare practices. The following research questions were of interest: (1) Can the QTF shed light on how and why the perspectives of TGD young people and professionals working with them converge and diverge? (2) How can the QTF improve the co-creation of knowledge between TGD young people and professionals to produce better health outcomes?
Methods
Participants, Design, and Data Collection
Data were gathered from two stakeholder groups residing and working in England: (1) Twenty TGD youth (aged 18-26) and (2) Eight healthcare, social, and voluntary sector professionals who work with TGD populations. Semi-structured interviews and open-ended survey responses were employed respectively to collect qualitative data from both groups, allowing for a rich exploration of their perspectives. Interviews and open-ended surveys covered the same topics to ensure consistency (see osf.io/xqp9h for the interview schedule and survey questions). These topics included social engagement patterns of TGD young people, the benefits of social support (including how it could facilitate better navigation of healthcare challenges), and barriers to accessing this support.
The inclusion of these two groups ensured a balanced understanding of healthcare and social engagement experiences, incorporating insights from both service users and providers. A qualitative approach was chosen to obtain richer data than that which could be achieved with quantitative data. This richness was needed not only to give adequate voice to both samples, but to allow for a detailed exploration of sources of tension between the two samples; to understand the why of the convergence and divergence observed.
QTF Development
An adapted version of Campbell and colleagues’ (2020) triangulation process was developed. Their approach combines interview, observation, and archival data from multiple stakeholder groups to understand divergence and convergence within the data, and includes guidance on how to determine data credibility, and its usability for the development of policy. We felt that adopting a similar process, whilst addressing the aforementioned limitations of existing triangulation frameworks, would be appropriate for the present study.
Campbell and colleagues’ (2020) triangulation process was deemed to be more suitable for adaptation in the current context than other triangulation methods (E.g., SAGA; Reicher and Sani 1998) given: (1) its focus on triangulating data for improving policy development, which is similar to our intention to improve healthcare pathways, and (2) its ability to interrogate underlying reasons behind divergent data. Nonetheless, we identified a limitation with Campbell et al.’s (2020) method, which, as previously mentioned, involved them triangulating the data after analysis. To address this, we introduced triangulation earlier within the data analysis process. This meant comparing key arguments between data sets (i.e., stakeholder groups) prior to developing themes. Themes were thus developed after triangulation so that they reflected both divergence and convergence, enabling us to capture the richness of our data. Building on the limitations of SAGA, we also considered the salience of each argument (i.e., is it common within one group, across both groups, or neither?), and what can be inferred from this (see Sands & Roer-Steir, 2006 for a similar approach).
QTF Process
An Example Excerpt of the Triangulation Table Adapted From Campbell and colleagues (2020) Used to Triangulate the Two Data Sets

Notes. Main Codes and Sub-Codes can be found in columns one and two respectively. The coding categories for triangulation were as follows:
A) Consistent within and present across groups (i.e., most young people and most professionals discuss this Main Code/Sub-Code).
B) Consistent within and not present across groups (i.e., most young people discuss this Main Code/Sub-Code, but it is not discussed by professionals, or vice versa).
C) Inconsistent within and present across groups (i.e., some young people and some professionals discuss this Main Code/Sub-Code, but this is not discussed consistently within either group).
D) Rarely mentioned in either group (i.e., only one/a few individuals from either group discuss this Main Code/Sub-Code).
The triangulation process involved the authors classifying each Main Code and Sub-Code into one of four categories: A) consistent within and present across groups (i.e., most young people and most professionals discuss this Main Code/Sub-Code); B) consistent within and not present across groups (i.e., most young people discuss this Main Code/Sub-Code, but it is not discussed by professionals, or vice versa); C) inconsistent within and present across groups (i.e., some young people and some professionals discuss this Main Code/Sub-Code, but this is not discussed consistently within either group); and D) rarely mentioned in either group (i.e., only one/a few individuals from one of the groups discuss this Main Code/Sub-Code).
This classification system facilitated a systematic exploration of convergence (through category A codes) and divergence (through category B and C codes). Divergence was examined using interpretative strategies to explore reasons for the disagreement and to identify actionable insights (see Campbell et al., 2020; Farmer et al., 2006; Sands & Roer-Steir, 2006). For example, are there different perspectives across stakeholder groups?; Does each sample have different knowledge about the same topic?; Is one group unwilling to talk about something, but the other group is (e.g., is something alluded to, but participants express apprehension around the topic)? This allowed us to develop themes that captured nuanced understandings (See Figure 1). Triangulation Process Flow Diagram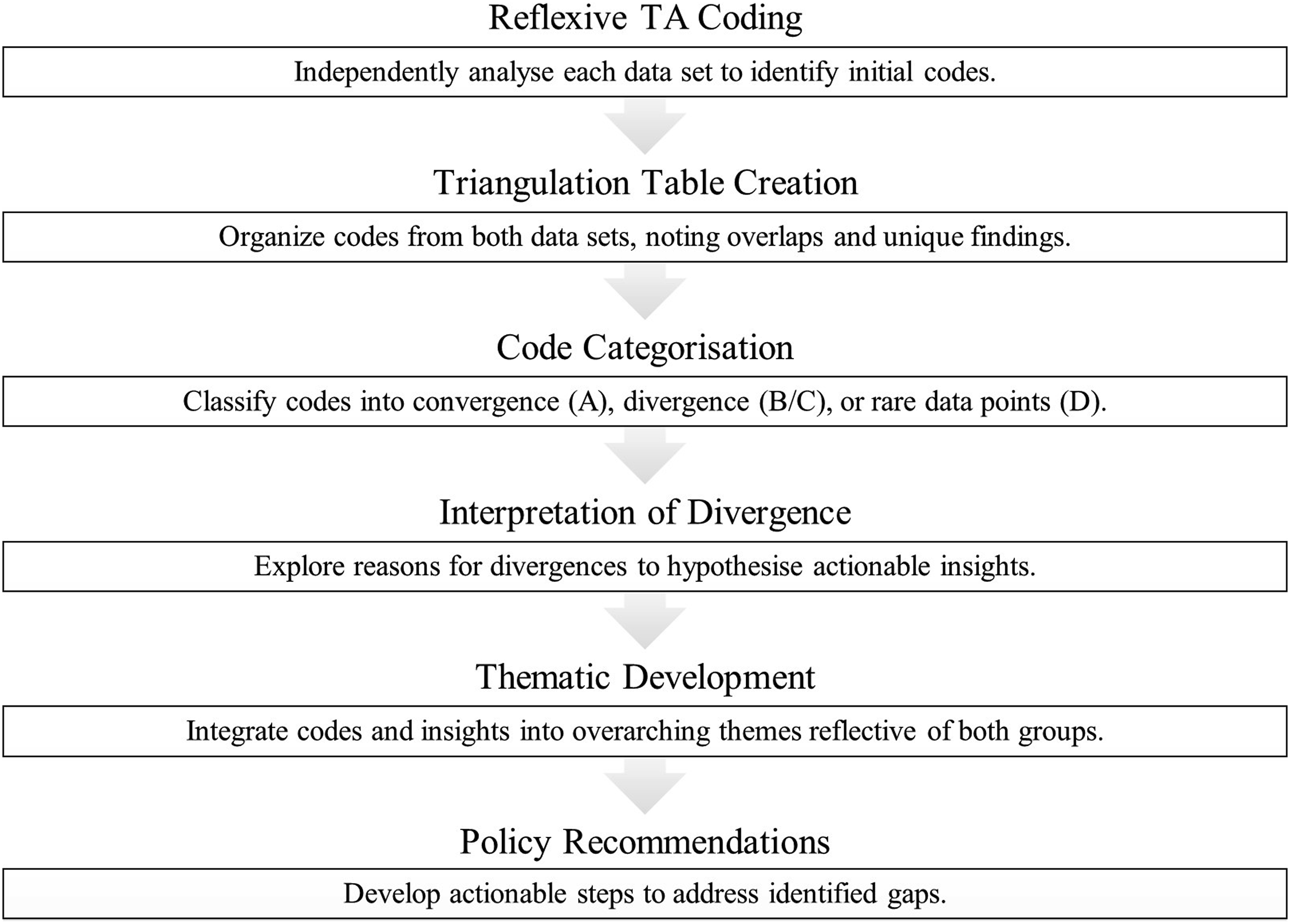
It is important to clarify that while this grouping method might seem quantitative (or “small q”; see Braun & Clarke, 2022), its purpose is not to count code occurrences to identify themes, as in content analysis. Instead, it serves as a tool to explore similarities and differences both between groups (e.g., young TGD people and professionals) and within groups (e.g., among young TGD people themselves). The goal is to develop deeper, latent themes rather than surface-level, descriptive ones, thereby aligning with the principles of Reflexive Thematic Analysis (RTA; Braun & Clarke, 2022). Thus, the QTF is suited to qualitative methods that aim to generate nuanced themes (e.g., RTA, IPA) rather than simply patterns and trends within the data (e.g., content analysis).
Results
To illustrate the utility of the QTF, a series of case studies examining each of the triangulation categories will be presented to demonstrate how the questioning of divergent/convergent data points extended understandings of young TGD people’s health and social engagement experiences.
Incomplete Understandings: A Case Study of Triangulation Categories A & B
In fields where research has practice and policy implications, the consequences of implementation errors (e.g., policy-makers neglecting an aspect of healthcare that is perceived as crucial by service-users, and/or vice versa) are heightened. This is because it can lead to changes within service delivery that do not lead to improvements in outcome measures of interest (e.g., Jackson et al., 2023; Scheim et al., 2024; White et al., 2023). However, the reasons for disagreement or misunderstanding between young TGD people and the professionals involved in implementing healthcare changes have not been identified. Whilst intergroup tensions have been noted (e.g., Bartholomaeus et al., 2020; Vance et al., 2015), the specific point at which understandings diverge is unclear. For example, is it that TGD youth and professionals have different understandings of the health and social needs of TGD young people, or is it that they have similar understandings but their interpretations of how best to address these needs differ? Examination of triangulation categories A and B begins to provide an answer.
For example, convergent data points (A) revealed that both TGD youth and healthcare professionals consistently identified bureaucratic challenges as a significant factor impeding access to care and overall wellbeing. These barriers included excessively complicated administrative, governmental, and legal procedures that limited timely access to care. However, divergences (B) were identified in terms of how these different stakeholder groups perceived and experienced these barriers.
Professionals largely focused on systemic-level issues, such as long waitlists and widespread discrimination. In contrast, TGD youth highlighted the psychological burden of repeatedly navigating healthcare systems. TGD youth described how the continual need to manage intricate processes such as correctly completing forms, meeting stringent eligibility criteria, and facing repeated gatekeeping at different stages resulted in feelings of frustration, helplessness, and diminished agency. Thus, unlike the professionals, TGD youth perceived the challenges they experienced as extending beyond the initial point of referral. Indeed, the recurrent process of learning how to ‘correctly’ navigate complex systems was deemed to be more psychologically challenging than long waitlists themselves (see Staras et al., in preparation). As a result, policies aimed at solely reducing waitlists or improving resource allocation may fall short of addressing the barriers impacting TGD youth’s healthcare access.
Triangulation was thus useful in highlighting the possibility that professionals may not fully understand the underlying factors that are exacerbating TGD youth’s negative health outcomes. Further, exploring A and B triangulation categories together highlights the nuances of the groups’ convergences and divergences. Practically speaking, this allows TGD healthcare professionals and policy makers to identify aspects of, and priorities in, healthcare delivery policy that fail to address the healthcare issues experienced by TGD youth, and to alter these policies accordingly. Specifically, our data suggest that adaptations to service delivery need to focus on simplifying GIC processes in ways that are transparent and easily comprehensible to young TGD people.
Intra-Group Conflict: A Case Study of Triangulation Category C
As discussed above, triangulation categories A and B allow researchers to identify where there is agreement and disagreement between two or more stakeholder groups. This information is key for hypothesising reasons why changes made by one group (e.g., professionals and policy makers) may not be perceived/received as expected by another group (e.g., service users). However, divergence in understanding health and social needs are not just observed across groups, but also within groups. Thus, even among young TGD people, there may be discrepancies and disagreements.
Within qualitative research, despite its interpretivist epistemology, the preference for presenting convergent findings to ensure results are reflective of the group’s general experiences can mask such intragroup discrepancies (Hanson, 2006). This can often lead to positivism creep (Braun & Clarke, 2022), the result of which is insufficiently processed themes that are generic and descriptive rather than meaningful and insightful (Finlay, 2021). Given that TGD young people are not monoliths, masking intragroup discrepancies through only documenting convergent findings and claiming this meaningfully captures the nuanced experiences of all group members is unrealistic. This leads us to question how we can go about fruitfully capturing intragroup differences, whilst still ensuring that the claims made are grounded in evidence. Triangulation category C can help us achieve this.
Triangulation category C reflects data which are partially present across both stakeholder groups whilst not being consistently mentioned within either group. The inconsistent mention of these data within groups suggests ingroup members have different experiences. One example of this was discrepancies between social experiences of binary and non-binary trans individuals. Specifically, the latter (compared to the former) expressed social support as being more important for their health/wellbeing. This was for two reasons: (1) social support was often described as being the primary form of affiliation and validation for non-binary individuals who are not seeking medical transition; and (2) because non-binary individuals are subject to more pervasive discrimination and exclusion than binary individuals, even within TGD-specific spaces, thus leading non-binary individuals to particularly value social support (e.g., McCormick & Barthelemy, 2020; also see Staras et al., in preparation).
The fact that this broader topic of non-binary exclusion within the wider TGD community fell into triangulation category C suggests that neither young TGD participants nor professionals considered it to be a particularly significant issue. However, making this assumption would mask the fact that the profound impact of intragroup discrimination was frequently discussed by non-binary TGD young people, and by some professionals (Staras et al., in preparation; McCormick & Barthelemy, 2020). Further, given that the issue of non-binary exclusion crossed group boundaries (i.e., it was mentioned by both stakeholder groups), it suggests that its occurrence is not arbitrary (Liddell & DeDeo, 2022). Based on this possibility, we begun to consider whether, rather than being perceived as an unimportant issue, the partial silence within both groups regarding non-binary exclusion indicated some individuals’ reluctance to discuss it.
Drawing on our strategies to interrogate divergent data (e.g., are there different perspectives and understanding within and across stakeholder groups?; is one group unwilling to talk about something?), and viewing non-binary exclusion as an ‘incomplete’ data point (i.e., because non-binary exclusion appeared to be common knowledge based on its presence across both groups, yet was not discussed by many members of each group; also see Farmer et al., 2006), we considered reasons for reluctance by some individuals to discuss non-binary exclusion.
To illustrate, a few participants explained that one of the reasons that non-binary individuals are subjected to discrimination (even within TGD communities) is deep-rooted cisnormativity. This is because norms relating to congruent gender identity and expression, even for those who are TGD, can influence perceptions of what is deemed to be an (in)authentic identity (Staras et al., in preparation). Simply put, cisnormative discourse can lead to the discreditation of non-binary identities because, unlike binary trans identities, they do not align with traditional binary notions of gender. Evidencing this, some binary trans participants discussed how cisnormative discourse prompted them to view binary trans identities as more valid than non-binary individuals, despite also reflecting on the discomfort of these internalised norms (also see Bockting et al., 2020; Scandurra et al., 2018). Thus, silence on this issue does thus not necessarily imply unimportance, but rather an unwillingness by some binary trans people to acknowledge their internalisation of the very same traditional notions of gender that marginalised them. The QTF was thus able to provide a systematic strategy for questioning why not all participants within each group converged on this data-point, despite the topic being common knowledge across both groups. Without the QTF, non-binary exclusion could have easily been overlooked as a present, but insignificant, issue.
Embellishment or Irrelevant Data? A Case Study of Triangulation Category D
In our efforts to capture a nuanced understanding of TGD health and social engagement experiences, the coding process was iterative and extensive (see Staras et al., in preparation for further details). Resultantly, some codes were only relevant to very specific, individual circumstances, often denoted as triangulation category D (e.g., childcare being a barrier to social engagement). Whilst relevant to the individual, not all data points provide grounds for purposeful discussion and inclusion within the final thematic structure. However, as demonstrated in the above discussion of triangulation category C, only through questioning these points can we decipher what is significant or not. Thus, whilst not all triangulation category D data points were incorporated into the final thematic structure, either because they were not of key importance or we did not yet have enough data on the topic to make actionable recommendations regarding them, some category D data points embellished the key themes that were discussed (see Staras et al., in preparation for discussion of these themes).
One example of this is the code “cis[normative] het[erosexual] spaces are cognitively and emotionally exhausting”, a data point categorised as D due to its presence in only a handful of TGD young people’s interviews. This data point outlined how the psychological strain caused by entering social spaces populated by people who did not share their experiences of gender and sexuality led to participants’ avoiding such spaces. The negative health/wellbeing-related impacts of entering non-TGD spaces that this data point highlights shows that it is not just a preference for TGD youth to engage with similar others (i.e., other TGD youth) but a psychological need. This reinforces the need for TGD-specific spaces, since without them, loneliness, exclusion, and poor health/wellbeing are often inevitable.
Exemplar Divergences and Their Implications for Thematic Findings and Practice

Discussion
Within this study, we wanted to extend the literature on the utility of data triangulation for understanding discrepancies within and across qualitative data sets. We adapted existing triangulation systems used within political sciences (Campbell et al., 2020; Farmer et al., 2006; Sands & Roer-Steir, 2006) to achieve this, culminating in the development of the QTF. We demonstrate how interrogation of divergent data can shed light on why research-based ‘improvements’ to healthcare systems and/or policy may not lead to benefits being observed within evidence-based practice. TGD youth served as an illustrative example of this to showcase the QTF’s potential to address healthcare marginalisation. These findings underscore the importance of moving beyond surface-level consensus to interrogate the underlying factors driving divergent experiences and perspectives.
Understanding Divergence and Its Implications for TGD Youth and Their Healthcare
Understanding divergence within our data through utilisation of the QTF had several implications. We overview here how QTF’s ability to offer insight into stakeholder tensions permitted us a more nuanced understanding of the challenges within TGD healthcare, and the impact of this on future TGD healthcare provision.
Firstly, divergence between professionals and TGD youth regarding bureaucratic challenges illustrates a fundamental gap in understanding. While professionals often conceptualise these challenges as logistic hurdles that can be addressed through systemic changes, TGD youth emphasise the emotional and psychological toll of navigating these systems. This mismatch has significant implications for policy and practice, as interventions targeting structural barriers (e.g., long waitlists) may fail to alleviate the cumulative stress experienced by TGD youth. Effective reforms must therefore address both the systemic and emotional/psychological dimensions of care delivery.
Intragroup dynamics also emerged as a critical area of concern, particularly the exclusion of non-binary individuals within TGD communities. The partial silence from binary trans participants on this issue highlights the need for research methodologies, such as triangulation, that can identify overlooked or under-discussed tensions. Recognising and addressing these intra-community dynamics is essential for creating truly inclusive spaces and interventions.
Overall, the QTF allowed us to develop themes that were reflective of the nuances both within and across stakeholder groups. For example, ‘Identity Loss During Transition’ became ‘The Ambivalent Nature of Transition-Related Identity Loss’, which allowed us to capture differential experiences and perspectives of familial support. Moreover, ‘Non-Binary Exclusion’ was extended to ‘Non-Binary Exclusion: Perceived Violation of Binary Ingroup Norms’ to better capture the processes that lead to non-binary exclusion. This meant we could develop suggestions for TGD healthcare that were (1) more diverse and personalised, and (2) that better reflected the reasons behind negative health outcomes in order to more effectively address them. Comprehensively, then, the QTF provides a compelling framework for not only understanding divergence within qualitative data, but also for developing more actionable recommendations than those which could be achieved without this in-depth exploration of the data.
Wider Implications
Relevance to Other Minoritised Populations
Whilst the present paper has explored the utility of the QTF for research with TGD populations, this is not its only purpose. As outlined in the introduction, there are multiple minoritised groups who would benefit from research approaches that value both divergence and convergence. This would allow minoritised voices, which are often overlooked or undervalued (Han et al., 2021; Horton, 2024; Pratt, 2019), to be better acknowledged and thus to make a more meaningful contribution in the research process. Thus, the QTF, demonstrated to be effective for TGD research, presents itself as a promising tool for research with other minoritised groups.
By way of illustration, individuals with chronic illness (Doherty et al., 2022; Natafgi et al., 2022), ethnic minorities (Gaya-Sancho et al., 2021), and broader LGBTQ + communities (Damery et al., 2025; Hascher et al., 2024) all report similar challenges to TGD youth in relation to the perceived lack of benefits they experience after the implementation of healthcare policy ‘improvements’. Resultantly, future research would benefit from adopting the QTF as a tool for developing actionable insights that address these challenges. For instance, the QTF could be applied to explore disparities in mental health services for ethnic minority communities (Thomeer et al., 2022). This could be achieved by using the QTF to examine differing perceptions about mental health held by ethnic minorities and by the healthcare professionals who care for them, thereby highlighting what ethnic minority service users prioritise as essential for addressing their mental health needs, and how this compares to the priorities of professionals. Similarly, misalignments between chronically ill people and their care providers can complicate care management. For example, service users may prioritise quality of life and symptom management, whereas providers may emphasise adherence to clinical guidelines. The QTF could systematically identify these misalignments, leading to recommendations for shared decision-making models that better align with service user priorities.
Further to these examples, several other populations may also experience differential understandings of their healthcare needs, yet these may not be reported in literature given the predominantly convergent and positivist nature of research designs (e.g., positivism creep; Braun & Clarke, 2022). Thus, data triangulation and questioning of divergent data, particularly when conducting research with groups that experience both inter- and intra-group discrimination, can facilitate the unpacking of these experiences. Altogether, the present findings underscore the value of the QTF for acknowledging and uplifting minoritised voices within research.
Extending the QTF: Data Sets in Tension
While the present study has focused on the application of the QTF for amplifying minoritised voices, particularly within TGD healthcare research, its utility extends beyond research with minoritised populations and healthcare settings. Any qualitative research that involves multiple stakeholder groups, competing perspectives, or divergent interpretations can benefit from an approach that systematically interrogates both convergence and divergence. For example, in fields such as public policy, organisational studies, and interdisciplinary health research, tensions frequently emerge between different groups who may not be minoritised but hold conflicting perspectives (Abelson et al., 2013). This can be due to different institutional roles, disciplinary boundaries, and lived experiences (Abelson et al., 2013). For instance, in public health policy, researchers and policy makers often interpret healthcare needs differently from frontline practitioners and service users (Abelson et al., 2013; Holman et al., 2021). Similarly, within organisational change, executives might highlight the increased productivity and cost savings of implementing new technology systems. However, frontline employees might express frustration over inadequate training, unrealistic performance expectations, and increased stress (e.g., Wijethilake et al., 2021).
By applying the QTF to these contexts, researchers can uncover the reasons why different stakeholder groups interpret the same issues in contrasting ways. Rather than viewing divergence as a barrier to consensus, the QTF allows for a more productive interrogation of why disagreements exist and how they might be resolved. This approach ensures that research findings are not oversimplified into a singular narrative but instead reflect the complexities of real-world decision making. Ultimately, the broader application of the QTF demonstrates its potential as a methodological tool for any research that seeks to navigate conflicting perspectives within and across qualitative data sets. By moving beyond a sole focus of minoritised voices, the QTF contributes to a richer, more nuanced understanding of stakeholder dynamics across diverse fields of research and practice.
Strengths and Limitations
To the authors’ knowledge, this is the first documented approach of qualitative data triangulation used within the social sciences. Whilst qualitative data triangulation has been utilised when combining interview data with documentary analysis (e.g., Campbell et al., 2020; Farmer et al., 2006), the same has not been replicated for the synthesis of two primary qualitative data sets within the data analysis stage. Similarly, whilst SAGA (Reicher & Sani, 1998) presents a type of triangulation, it does not integrate multiple data sets. Rather, it only explores arguments present within a single data set. Thus, the QTF presents a novel extension of existing triangulation work.
It is relatively common to see integration of quantitative and qualitative data in mixed-methods designs, where qualitative research is helpful for illuminating the underlying psychological processes of an observed change within quantitative outcomes (Ahmad et al., 2019). However, by design, this methodology tends to place emphasis on converging data. This desire for convergence, in part, stems from a response to the quantitative/qualitative divide within research, where neat, actionable qualitative findings that reflect broad groups are suggested to be comparable to quantitative work (Hanson, 2006; also see Braun & Clarke, 2022 on positivism creep). However, considering that this divide is often more political than intellectual (Hanson, 2006), and as suggested by the aforementioned case studies, convergent findings are not always the most useful for inspiring practical action. Instead, the reality for social sciences and healthcare research is that there are a multitude of social, political, and economic factors that impact lived experiences across multiple domains; complexity that is often filtered out through convergent research designs, and therefore is often ignored within the practical recommendations that emerge from such research (Mathison, 1988).
Having said that, it is not our intention here to discredit prior triangulation work, particularly where this has paved the way for coalescing quantitative and qualitative research to produce grounded mixed-methods research designs (Greene et al., 2001; Valencia, 2022). Rather, we envisage a new way for conceptualising qualitative research findings using the QTF; one that highlights sources of tension between stakeholder groups that, if overlooked, can have negative implications for policy and practice (as demonstrated in the analysis of triangulation categories A and B). Crucially, it is only through the comparison of two or more sets of qualitative data that we can begin to understand the ‘whys’. Why do these groups understand the same experience differently? Why do we not always see practical benefits when healthcare practices are ‘improved’? Why do minoritised communities still feel marginalised? Discerning these differences can help researchers and policymakers to move forward effectively.
Finally, while this paper provides valuable insights, it is not without limitations. The QTF, while effective, has not been rigorously tested across diverse data sets. Rather, it has been novelly applied to two new data sets to strengthen the actionability of our analytical claims. Nonetheless, it is anticipated that the present paper’s worked examples of data point examination highlight the applicability of the QTF for enhancing data analysis. Moving forward, adoption of the QTF when conducting research with minoritised populations and stakeholders in tension would benefit researchers whilst simultaneously establishing an evidence base for the QTF.
Conclusion
This study underscores the critical role of qualitative data triangulation as a methodological tool in research. Specifically, development of the QTF demonstrated how systematic categorisation and interrogation of data can move beyond surface-level findings to uncover the dynamics that shape stakeholder experiences. Traditional research methods often prioritise positivism and convergence to validate findings, yet this study highlights the power of divergence and interpretivism in capturing the complexity of marginalised experiences. By examining discrepancies, such as differing interpretations of systemic barriers or intra-community dynamics, the QTF offers a framework to generate richer, more actionable insights that conventional methods may overlook. Whilst we demonstrate the effectiveness of the QTF for TGD populations, the methodological contributions of this study extend beyond minoritise populations and healthcare settings. Triangulation provides a replicable process for integrating multiple perspectives, promoting inclusivity, and addressing overlooked tensions in research with other marginalised populations and stakeholder groups in disagreement. This demonstrates that adopting innovative approaches can not only amplify diverse voices but also enhance the depth and impact of research in multiple settings.
Footnotes
Ethical Considerations
Ethical approval for the original data set was obtained from Nottingham Trent University’s BLSS Research Ethics Committee (Application ID: 1741695) on October 24th, 2023.
Consent to Participate
Participants gave written and verbal consent before interviews commenced. Identifiable information was anonymised.
Consent for Publication
Written and verbal informed consent, including consent for publication, was obtained prior to research participation.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a fully funded PhD studentship from Nottingham Trent University.
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets analysed during the current study are not publicly available due to disclosure risks. However, with consent from participants and the removal of identifiable information, data may be shared for two purposes: (1) for the purposes of independent scrutiny, and (2) for the purposes of reproduction and/or research in a direction consistent with this research (i.e. to be of benefit to TGD communities in ways that affirm their identities). In these cases, permission to access anonymised transcripts will be granted on a case-to-case basis.