
Abstract
Vulnerability has typically been addressed in the context of research ethics from the point of view of participants, with a focus on how to prevent the potential or exacerbation of existing harm caused by the power and role asymmetries between researchers and participants. However, more recent approaches to research ethics question whether researchers are, by definition, located in a privileged position during the research process and safe from any kind of vulnerability. In line with this, we reflect on the dimensions of researcher vulnerability specific to studies using a qualitative methodology in health research. Our argument is that participants and researchers should be on the receiving end of efforts to implement ethical procedures and protection from harm. Based on the autoethnographic analysis of our experiences as qualitative health researchers, this paper aims to identify dimensions of researcher vulnerability, and draw out relevant recommendations for practice. The reflections upon which this paper is based emerged during a spring school focusing on research ethics in qualitative health research, during which we discussed situations from our own research experience which left us feeling vulnerable. We identify four dimensions related to the experience of vulnerability (reciprocity; emotional labor; application of ethical standards; reversed power asymmetries) and five crosscutting aspects relating to these dimensions (researching sensitive topics; researching in contexts of vulnerability, poverty and structural violence; being a novice; lacking adequate support; insufficient time and space for ethical reflexivity). Our recommendations address particular challenges for these dimensions, and center on the role of reflexivity, as one of the cornerstones for enabling ethical qualitative research practice, requiring us to acknowledge and address our own vulnerability and positionality. Autoethnographic exercises are particularly useful for zooming in on ethically important moments in research related to researcher vulnerability and fruitful for identifying resources to respond to such challenges in the future.
Introduction
One of the recurrent concerns in the research ethics literature has been to protect research participants from potential harm (Hammersley, 2018). As research imposes a predetermined role and power asymmetry between researcher and participants, a key concern is to conceive and manage researcher–participant relationships in a way that prevents exacerbating participants’ vulnerability than the one they might already be experiencing. This can be accomplished by minimizing the distance and separateness between research participants and researchers, committing to a power redistribution, and encouraging mutual disclosure and authenticity (Bell et al., 2014; Bracken-Roche et al., 2017; Karnieli-Miller et al., 2009).
Without diminishing the due importance of considering vulnerability, recent approaches to research ethics claim that the notion would gain from a more rich understanding instead of being mobilized as a rigid, fixed label (Luna, 2009, 2019). For example, Luna highlights the need to consider vulnerability as a phenomenon that arises in the context of certain relations between persons and circumstances including economic, social and political exclusion, and that it should not be considered as a permanent and categorical condition assigned to a particular subpopulation (Luna, 2009, 2019). Luna argues for a revised, contextual concept of vulnerability to be understood as “layers”, composed of multiple and different strata that may or may not be operating at any particular time for a given person, rather than being a solid and unique “label” (Luna, 2009). For example, Luna describes how being a women does not in itself constitute a vulnerability, but a women living in a country with low reproductive rights, a women who is illiterate, and/or living in poverty aquires (overlapping) layer(s) of vulnerability, which another women living in different circumstances will not have (Luna, 2019). Such reflexions about what constitutes vulnerability and who might be considered to be vulnerable in a given context also introduce the question of whether researchers are, indeed, by definition, located in a privileged position during the research process (Bashir, 2020; Råheim et al., 2016). Recent, critical approaches to research ethics argue that the rise of bioethics and of the “doctrine of vulnerability” (van den Hoonaard, 2018, p. 307) happened in health research in the particular institutional and sociopolitical context of the 20th century, in which individuals had been subjected, against their will or knowledge, to experimental treatments. This led to a focus on aspects related to asymmetrical power relationships and situations in which participants were not able to provide informed consent to research (van den Hoonaard, 2018).
However, one also needs to recognize and address the fact that researchers might be subjected to harm and considered as vulnerable in particular research configurations. In this approach, vulnerability is only not linked with the (in)capacity of giving consent to participating in research, but should be considered as a potential impact of research, thus, concerning both participants and researchers. Studies show that the exploratory, spontaneous and fluid nature of qualitative research places researchers in unexpected situations over which they often have little control (Dickson-Swift et al., 2008; Miller et al., 2012). As Sampson and Thomas (2003) argue, additional contextual specificities, such as hazardous occupational settings, and even gender identities (e.g., being a female researcher in a male-dominated setting) give way to situational risks that can endanger the health and safety of qualitative researchers. In particular, research focusing on sensitive and stigmatized topics, such as death, disability, poverty or other types of suffering, was shown to be delicate for researchers. For example, the grounded analysis performed by Dickson-Swift and collegues (2007) on the experience of qualitative researchers doing research on sensitive topics identified several challenges that they faced, including the obligation to develop rapport, the importance of researcher self-disclosure, listening to untold stories, developing feelings of guilt and vulnerability, difficulties of leaving the research relationship, and researcher exhaustion. As Clark and Sousa (2018, p. 1) rightfully note, the mental health of qualitative researchers is “precious yet precarious,” with particular risks corresponding to almost all phases of the research (data collection, analysis, publishing, grant applications, etc.).
In light of the growing recognition of the need to further investigate the challenges of qualitative research, scholars have been increasingly engaging in introspective discussions to show how research experiences of these sensitive topics can generate intense moral distress and emotional exhaustion (Howard & Hammond, 2019; Johnson & Clarke, 2003; Malacrida, 2007; Nkosi et al., 2022; Sikic Micanovic et al., 2019; Woodby et al., 2011), and even lead to the abandonment of research careers (Malacrida, 2007). In response to these concerns about researcher vulnerability, guidelines and codes of practice are being written and adopted to be better address the various dimensions of researcher vulnerability. The Social Research Association in the United Kingdom, for example, developed a “Code of Practice for the Safety of Social Researchers” as early as 2001 (Social Research Association, 2001).
Objectives
In this paper, we reflect on the dimensions of researcher vulnerability specific to qualitative health research. Our argument is that both participants and researchers should be on the receiving end of efforts to implement ethical procedures and protection from harm. Based on an autoethnographic analysis of our own experiences of vulnerability in this domain, this paper aims to identify a number of possible dimensions related to researcher vulnerability and draws out relevant recommendations for practice. While the paper does not seek to represent the full range of dimensions of researcher vulnerability possible, it aims to exemplify a methodology (autoethnography) which other researchers can utilize to reflect on dimensions of vulnerability that are unique, as well as more widely shared across context and places.
Methods and Process
The reflections upon which this paper is based emerged during a spring school focusing on Research ethics in qualitative health research, organized by the Ruhr University Bochum, Germany, in March 2022. During one of the workshops, the participants identified and discussed interesting topics in the field of research ethics in qualitative research, one of which was “researcher vulnerability.” In response to these discussions, a group of six workshop participants (the authors of this manuscript) came together to engage in several autoethnographic exercises to reflect on and describe specific situations from their qualitative health research experience which left them feeling vulnerable.
Autoethnographic writing has become popular in a wide range of disciplines, including social sciences and clinical work (Johnson & Clarke, 2003; Karnieli-Miller et al., 2009; Malacrida, 2007). It is defined as a research approach in which personal experience (“auto”) is described and analyzed systematically (“graphy”) in order to understand socio-cultural experiences (“ethno”) (Adams et al., 2018). It is therefore a mix of self-observation and reflexivity in relation to doing research fieldwork and analysis. As Ellis et al. point out, “autoethnography is one of the approaches that acknowledges and accommodates subjectivity, emotionality, and the researcher’s influence on research, rather than hiding from these matters or assuming they don’t exist.” (Ellis et al., 2011, p. 274). When applied to reflections on ethical issues, autoethnographic writing tends to produce transgressive accounts that can “trouble the ethical relations of self and other, break through the dominant representations of professional practice, creating new knowledge” (Denshire, 2014, p. 844). As such, this methodological approach was deemed to be particularly useful to address our topic.
The group of participants engaging in the autoethnographic exercise come from academic backgrounds in sociology, social anthropology, psychology, global health and pharmacy; four hold a PhD on a health-related topic using a qualitative approach. Five authors come from high-income countries in Europe, with two of these conducting their research or parts of their research in low- and middle-income countries in Asia, and the sixth author originating from and conducting research in a lower-middle income country in sub-Saharan Africa. As social constructivists, the participants also recognize that the insights gained in research are cognitive constructions that do not accurately reflect social reality but that this reality is generated in an interactive process (Pörksen, 2011). In this respect, the personal experiences of the researchers involved have influenced the interactions in the research process, as has been highlighted by other autoethnographers (Ellis et al., 2011).
The process of autoethnographic reflection was conducted in several stages over a series of online meetings between the authors (i.e., the “participants” of the autoethnographic exercise). Each participant was initially invited to reflect on and then orally share recollections of particular difficult moments in their research career in which they felt vulnerable. Each participant then chose one “ethically important moment” (Guillemin & Gillam, 2004) from their own experience which they considered important and proceeded to write down their recollections in the form of a case vignette. In making the selection among the case vignettes, the participants ensured that different “ethically important moments” were chosen, as several similar experiences were reported. The participants then paired up to exchange and discuss the written vignettes in a subsequent bilateral meeting, during which they were encouraged to use inquiry and active listening techniques to draw out further ethically salient reflections and perspectives from one another’s vignettes. Following this exchange in pairs, each vignette was then read and presented to the group during a subsequent meeting of all authors. The group members were then paired together again to identify which aspects within the vignettes seemed to lead to experiences of vulnerability. These aspects were subsequently discussed within the wider group and jointly categorized in overarching dimensions and crosscutting aspects that encompass all dimensions. After identifying several dimensions of researcher vulnerability specific to qualitative health research, the group reflected on recommendations that could prevent or alleviate these types of vulnerability. This reflection was based on participants’ own experiences and a review of relevant literature.
Findings
We present here the four dimensions that were identified as being related to the experience of vulnerability for researchers in healthcare (reciprocity; emotional labor; application of ethical standards; and reversed power asymmetries), each illustrated by a vignette drawn from our research careers, and the five crosscutting aspects that underpin these four dimensions (doing research on sensitive topics; doing research in contexts of vulnerability, poverty and structural violence; being a novice; lacking adequate support; and doing research with insufficient time and space for ethical reflexivity).
Reciprocity
A key ethical question arising in qualitative research evolves around researcher’s responsibility towards research participants and the need for “giving back” to participants (Tubaro, 2021). Depending on the context and setting in which research takes place, there may be many ways to “give back” (e.g., monetary compensation vs. nonmonetary, such as goods and services); time frames in which something is returned to participants (immediate vs. short- vs. long-term); and different levels at which reciprocal actions can be aimed: the micro (individual), meso (community) or macro (societal, political and structural) level (Bronfenbrenner, 1979). While a number of international ethical guidelines provide an overall normative framework for conducting global health research (Calman, 2002; Council for International Organizations of Medical Sciences [CIOMS], 2016, World Medical Association [WMA], 2013), questions about what is owed to participants, when and to whom have been widely debated in the research ethics literature (Lairumbi et al., 2011, 2012). However, the majority of this literature focuses on clinical rather than qualitative research (Grady, 2005), thus, often leaving qualitative researchers uncertain about what constitutes ethical reciprocity in qualitative health research and resulting in moral dilemmas and emotional burdens among fieldworkers (Nkosi et al., 2022; Tubaro, 2021). In the following autoethnographic field reflection, a researcher describes the distress she experienced as a result of feeling unable to sufficiently “give back” to her research participants following an interview study conducted in a lower-middle income country during her PhD:
Fieldnote #1. Reciprocity and the desire to leave participants “better off” One ethically challenging situation arose in deciding how to compensate participants for taking part in a research interview. I felt that money would have been most helpful to our participants. However, when discussing this with the local research partners, they expressed concern about setting up a precedent which they would not be able to uphold in future interactions with the community. We therefore decided against financial compensation. Each day, we travelled to interview participants in their homes in the rural areas. Many lived in severe poverty, and some were in really poor health. It was apparent that these families lacked everything – food, water, clothing, adequate shelter. One interviewee revealed that they were struggling with severe depression, which resulted in them not being able to care properly for the children in their household. Another participant described being regularly beaten up by a relative. There was no referral service I could suggest to my participants that would provide tangible, immediate protection or support. These encounters always left me feeling very sad and uncomfortable when leaving participants’ homes: I had a sinking feeling that I was not doing enough to help them. After each interview, we handed each participant a small giftbag containing useful items such as soap, water, snacks, pens and such things. But this felt inadequate. I was gaining a PhD from this research, but how were my participants benefitting? I wished to leave them ‘better off’ in some way. I felt indebted to my participants and was often left feeling guilty for not having been able to do more to help. Part of this feeling stemmed from a sense of personal moral obligation to help a fellow human in the face of suffering. But it was also greater than that: as a researcher coming from a ‘Global North’ institution doing research in the ‘Global South,’ I felt the weight of larger forces of current and past inequalities and exploitation, such as capitalism and colonialism, on my shoulders.
Field researchers may experience a heightened sense of needing to “give back” to their participants in research projects which operate against a backdrop of chronic poverty, social inequalities and structural violence (Farmer, 2004), and equally, a heightened sense of guilt and moral distress if this need is not met (Kingori, 2015).
This raises important ethical questions about the role and responsibility of field researchers and research institutions in reducing the suffering that they seek to understand. As researchers, it is our duty to conduct high-quality research to provide evidence for change, and make this knowledge available and accessible in order to advocate for change. Researchers seeking to implement changes and solutions should engage closely with community actors and employ participatory and action-based research methods whenever possible (Pratt et al., 2020; Reynolds & Sariola, 2018), acknowledging that “fostering reciprocity and mutual learning requires long-term engagement and therefore a break with the project logic of current funding mechanisms” (Heath & Mormina, 2022, p. 1709).
At the same time, researchers need to be aware of the limits of their role and capacity, recognizing the responsibility of local political institutions, nongovernmental organizations and community actors to implement structural and long-term changes at the community level. This may mean that, in many situations, researchers will be left with feelings of guilt and frustration about being unable to practice sufficient reciprocity—a situation which may never feel fully resolved but can be helped by anticipating and preparing for the moral distress of such research encounters. Furthermore, developing an understanding of the roles and responsibilities of different actors in a given research ecosystem is an important process of planning a research project which may help researchers to better understand their own roles and obligations, as well as the limits of their roles. Supervisors of junior researchers should pay particular attention to discussing these roles with their students from the outset and jointly reflect on questions of reciprocity, including how to identify locally existent support structures.
Emotional Labor
Emotion work theory provides a useful framework for understanding the experiences and challenges that qualitative researchers have during the research process. The reflection was initiated by Hochschild (1983) in her work on emotional labor, that is, how certain professionals would involve a display of their emotions as part of their daily jobs. Health professionals who are in contact with patients are often required to invest in such emotional labor (Riley & Weiss, 2016; Vinson & Underman, 2020), as are researchers (Bergman Blix & Wettergren, 2015; Hoffmann, 2007; Williams & Kolb, 2021). In the following field note, a researcher is reporting on an interview situation she encountered with a palliative interview partner during her PhD:
Fieldnote #2. Emotion labour and “the weigh of having to provide companionship” I conducted an interview with a woman living with cancer and nearing the end of life. I had been informed that she suffered from a severe facial disfigurement. Having anticipated that this might be challenging to handle, I prepared myself in order to ensure that my reaction would not hurt her nor prejudice the interview – though ultimately dealing with her disfigurement did not turn out to be a challenge. After the interview, she mentioned her weaving hobby and invited me to see some of her works. Even though I didn’t have a real interest, I found it hard to refuse, wanting her to feel appreciated. She mentioned her loneliness several times and how much she appreciated my interest, and it was hard for me to disengage. When I did, she expressed her hope of seeing me again. This situation made me experience severe distress and left me wondering what conduct would have been appropriate. I felt that I had faked an interest, while at the same time my concern with showing appreciation to her was genuine. I felt sad that the interview partner was alone, but also frustrated to feel the weight of having to provide companionship. It was obvious to me that such an engagement could not be asked of me professionally. Later, I received the message that she had passed away. I felt guilty but also relieved. Reflecting on this situation left me with a feeling of not being able to meet my own personal moral demands, I felt insecure because I tried my best to prepare for this interview and realized that I had not been able to anticipate the challenges.
Collecting data requires some kind of personal relationship, and boundaries are often a matter of personal sensitivity, difficult to foresee and establish in advance. Particularly in situations in which research participants go to extra lengths to contribute to interviews, researchers may feel the need to display reciprocity (similarly to the reflections addressed in Fieldnote #1, yet on an emotional level). This exposes them even further to vicarious trauma—secondary trauma transposed from an original person to a second one who only witnesses its report (Smith et al., 2023). Building rapport with particularly vulnerable participants might also disarm the professional veneer of the researcher and lead them to experience emotional vulnerability, which may be hard to reconcile with as healthcare researchers.
Emotional labor is anchored in a deep cognitive process, which requires the person to identify with the emotions they want to display, to the point where those emotions are a consequence of cognitive activities (Lazarus, 1991). People who feel they “fake” emotions as part of their emotional labor feel guilty because they are not being sincere (Hochschild, 1983). Such a blatant discordance between experienced and displayed emotional states can lead to poor health and impact performance (Mesmer-Magnus et al., 2012). Strategies exist to prevent or limit the effect of emotional dissonance during emotional labor, such as deep acting (changing one’s internal feelings to align with expectations; Hochschild, 1983; Mesmer-Magnus et al., 2012), but rely on a complex cognitive process that requires experience and preparedness, and might not be easy to accomplish at the start of one’s career. This means considering such emotions not as “fake” but as performative, a façade that the researcher can engage and leading to greater participant or community access. On the other hand, researchers can also find something positive in their own emotions, when it comes to data analysis. Hoffmann (2007), with reference to Kleinman and Copp (1993), understands emotional labor itself as important data, which should not be omitted from the analytical material. To ignore the researcher´s own emotions would make it more difficult to understand those the researcher is studying. Therefore, understanding emotional labor is essential for high-quality data analysis (Hoffmann, 2007).
In certain situations, the life stories shared by participants might also make researchers vulnerable to the reemergence of their own painful emotions associated with their life story. Research methodology textbooks call for establishing critical distance with participants and the stories that they share (Woodthorpe, 2011). Suppressing negative feelings in order to filter only appropriate emotions are also an important part of emotional labor (Grandey, 2000). However, it is difficult to accomplish such distancing when the study touches on very personal experiences. In the following autoethnographic field note, a postdoc researcher reflects on an interview situation with a terminally ill woman, which triggered painful memories for the researcher:
Fieldnote #3. Emotion labour and “compassion” One difficult moment was when the participant talked about moving from her residence, where she lived with her husband, to an apartment where she would benefit from palliative care services but live by herself. I felt my tears welling up, because I imagined that she would be isolated from her husband. I realized afterwards that my emotions resulted from being reminded of my dying mother, who was also often alone towards the end of her life and received little care from my father. But during the interview, I was not aware of this analogy. I felt compassion because she seemed to know exactly what was coming her way and was very calm and rational. And this was also what I experienced with my mother. I managed not to cry, but when I left her after the interview, I felt strong emotions, because I knew that she was going to die and that next year would be marked by a constant physical decline. When I reflected on this situation, I thought about my motivation to control my emotions. I thought that had I not controlled my emotions, the participant might have felt a need to support me, which would have left little room to express her own emotions. It is possible that the participant would have wanted to withhold further details of her suffering, so as not to cause harm. I was concerned that my surfacing emotions could have led to a termination of the interview, leaving us both with an unpleasant feeling. These reflections left me wondering whether I was the right person to conduct interviews with those who are terminally ill.
Qualitative data have been described as an “affective process” leading to reflections about “an ethic and ontology of vulnerability” (Rooke, 2016, p. 31). Emotional and intellectual detachment in such settings is hard to reach. As a protective measure, researchers are still strongly advised to look for topics beyond their geographical, sociopolitical and medical proximity (Alvesson, 2009). However, the reliving of traumatic memories due to the researcher’s own life and family history is a situation that can often arise unexpectedly (Tanner, 2009). But how can we deny emotions and their expression from the content of our interaction and, at the same time, maintain the authenticity of the relationship? How can researchers handle such situations in a way that is respectful to themselves and the participants? Such situations highlight the paradoxes of emotional labor in research.
Application of Ethical Standards
Research ethics articulate core principles of ethical conduct in empirical research practice, and the role of research ethics committees (RECs) is to pre-evaluate ethical appropriateness of a study. RECs must base their ethical assessment of applications on three main evaluation perspectives. These are (1) the scientific quality, (2) the ethical justifiability and (3) the legal admissibility of the study (CIOMS, 2016, WMA, 2013). Following Guillemin and Gillam (2004), we refer to this approval and review process by RECs as “procedural ethics.”
While procedural ethics is essential to prevent harm to participants, it can also pose problems of transference into practice since it cannot prevent all ethically difficult situations which inevitably arise in practice (Israel, 2015; Øye et al., 2016; Mackworth-Young et al., 2019; Thompson & Russo, 2012). In the following field note, a researcher narrates the moral distress she experienced during her PhD in conducting focus group discussions about the experience of coercion among patients involuntary admitted to psychiatric hospitals in Nigeria. This study was pre-reviewed and positively approved by a REC.
Fieldnote #4. Application of ethical standards and “the audacity of hope” Given that our study objective was to study coercion, it was of the essence that participation to the study was voluntary and informed. We trained social workers from a different service to conduct the interviews; informed consent forms were explained. However, I felt that some patients had chosen to participate on the basis of false expectations. Some seemed to hope that by participating, they would show that they had regained ‘insight,’ which would lead to them being discharged. Most felt that the focus group discussion was done to facilitate change in the hospitals. Although we clarified that this was not the case, it was impossible to completely diminish the audacity of hope and unrealistic expectations. The audio recordings revealed extreme violations of human rights, such as the use of restraints and flogging with chains. My collaborators were well aware of these violations and could do little or nothing about them. It was a systemic problem: the psychiatric hospitals were underfunded and short staffed, and workers had not been trained; they had few humane devices for restraint. This made me feel like I was investigating a hopeless situation. I felt guilty for making them share these difficult experiences, and to be arousing “false hopes” that the study might change things for them. If their perception of the broader aim of the research was that it was meant to facilitate change, I could imagine their disappointment when they continued to experience those violations.
Power dynamics between researchers and participants is a well-studied phenomenon (Karnieli-Miller et al., 2009). The researcher is usually perceived to have more power in their capacity as the seeker of knowledge and methodological expertise. This power gradient can be exaggerated in different contexts, such as when research is carried out among participants diagnosed with a mental health condition. As studies show, participation in research can be motivated by altruism (McCann et al., 2010) and this is a resource of persuasive communication for researchers trying to convince participants to take part (Williams et al., 2008). One strategy that can be employed when research is to be conducted on situations that are known to give rise to significant ethical dilemmas may be to conduct a preliminary study in which feasibility is addressed and different ways of engaging with participants are explored. For example, when conducting research on the meaning that intimate partners of female rape victims attached to their lived experiences after the rape, Van Wijk and Harrison (2013) initially did a pilot study to identify and circumvent possible risk factors in the proposed recruitment and data collection methods. Yet needless to say, even when specific measures are put in place to clarify the risks and benefits of research, unanticipated events (such as finding out that participation was influenced by false expectations) may still lead to moral distress for the researcher.
In other cases, standardized ethical requirements can generate ethically difficult moments when they fail to address the context-specific needs that participants face and the researcher’s sensitivity to these needs. Researchers are sometimes forced to apply overly restrictive exclusion criteria that resort to conceptual shortcuts. A blatant example is how the notion of vulnerability is conceptualized. As Hurst (2008) argues, reaching an overarching definition of vulnerability must be grounded in the sociohistorical context. Yet, few research ethics policies consider vulnerability in all its complexity (Bell et al., 2014; Bracken-Roche et al., 2017). Article 19 of the Declaration of Helsinki states that vulnerable groups and individuals “may have an increased likelihood of being wronged or of incurring additional harm” and, therefore, “should receive specifically considered protection” (WMA, 2013). Although the clarificatory guidelines of the CIOMS seek to “avoid considering members of entire classes of individuals as vulnerable” (CIOMS, 2016, p. 57), RECs often assume that prospective research participants with mental disorders are intrinsically vulnerable (Bell et al., 2014). Similarly, even if the Council for International Organizations of Medical Sciences guidelines recognize that “vulnerability involves not only the ability to provide initial consent to participate in research, but also aspects of the ongoing participation in research studies” (CIOMS, 2016, p. 57), a predefined notion of vulnerability based on implicit assumptions about risks is often required by RECs (Haggerty, 2004; Holland, 2007; Peter & Friedland, 2017).
In the following autoethnographic field reflection, a postdoc researcher presents the moral distress she experienced when applying a REC’s participant exclusion requirement based on a presumption of risk that she did not judge to be appropriate in the specific research context:
Fieldnote #5. Applying ethical standards and “inappropriate exclusion criteria” During this research project, I conducted interviews with people who experienced coercion in psychiatry and their relatives. In one case, both a daughter who had experienced coercion in psychiatry and her mother wanted to take part in the study. However, based on the requirements of our research ethics committee, I was not allowed to conduct interviews with dyads because of the assumed risk of internal influence. After a discussion with my colleagues, who agreed that no derogation to the exclusion criteria was possible, I had to tell the mother and daughter that only one could take part in the study and that they should decide who that was (finally, the mother did). Later, I had a new appointment for another interview with a man who knew the mother and the daughter. Some days before the appointment the man contacted me to ask whether his partner could be present during the interview. I explained that the interview would be about his experiences but that his partner could be present. When I met him, I saw his partner sitting on a chair, and recognized her as the daughter who had initially wanted to take part in our study. I felt uncomfortable that I had to exclude her from participation the first time, based on requirements of the research ethics committee that I didn’t find appropriate for the particular research context. I considered that the exclusion criteria applied initially had been inappropriate, since both mother and daughter wanted to take part in the study and knew about each other’s intention.
It is questionable whether such a protective exclusion of individuals who are considered vulnerable is desirable (Bracken-Roche et al., 2017; Carlsson et al., 2017; Øye et al., 2007, 2016). What underlies the special protections for these research participants is a strong focus on the risks of research participation. Justified as a careful consideration of risks may be, a focus on risks becomes problematic when benefits to participants are underestimated or overlooked (Carlsson et al., 2017; Cox & McDonald, 2013; Graham et al., 2007; Lewis & Graham, 2007; Witham et al., 2015). Individual benefits in qualitative health research may include things such as feeling heard and seen, and having the opportunity to state one’s opinion. Furthermore, studies have shown that research participants often see a benefit in participating in research even if there is no individual outcome, for example, because they value having the opportunity to contribute to improving healthcare services (Cox & McDonald, 2013). Protective exclusion from qualitative health research based on an overestimation of risks and underestimation of benefits can, thus, be ethically problematic.
Bridging procedural ethics and ethics in practice allows one to ensure that research is developed and led based on ethical criteria that are adapted to each particular study context. In this light, it seems important to give weight to both the external assessment of ethical principles and the situational interpretation of these principles (Peter & Friedland, 2017). This requires RECs to grant researchers a certain degree of flexibility and decision-making power while carrying out their research, and encourage them to practice ethical reflexivity to increase their sensitivity to ethical challenges that arise during the data collection process (Allen & Israel, 2018).
Reversed Power Asymmetries
Qualitative inquiry, by its approach, tends to reduce the impression that the researcher is the ultimate source of authority (Karnielli-Miller et al., 2009). Power relations between researcher and participants have essentially been considered from the point of view of protecting participants in reflections on qualitative research. However, at times, power asymmetries can play out in the opposite direction, with the researcher being the one in a detrimental and disempowered role (Råheim et al., 2016). This is due to the essence of qualitative research itself that requires a thorough immersion alongside a population of which researchers have only little or theoretical knowledge. Dynamics that exist within communities cannot be contained within their environment when an external observer arrives. Instead, the external observer is pulled into these dynamics. Participants might also challenge the researcher to prove they have the higher ground in a desire to affirm the ownership that they hold over their experience and knowledge. Just like a rite of passage, the researcher submits to a hazing that identifies them as a newcomer but also allows their entry and recognition within the new setting. In the following fieldnote, a researcher remembers one of the most difficult moments experienced at the beginning of her PhD:
Fieldnote #6. Reversed power asymmetries At the beginning of my PhD, I had to shadow hospital porters, an event which had been arranged by their chief and my supervisor. Early on my first day, I was informed of our first assignment: to transport the body of a deceased person from a unit to the morgue. While I accompanied them to the unit, I felt a rising anxiety at the thought of being near a dead body and of showing my anxiety. I had hoped that they would tell me not to come with them, but they just asked “Are you interested in joining?,” to which I felt obliged to say, “Yes.” I felt unnerved because this seemed very far from my study objective and I was being needlessly exposed to anxiety and ridicule. When we got to the room, they jokingly said that I should wait outside because the patient had died with tuberculosis and it might be infectious after death, yet I couldn’t understand whether it was a joke or not (and how). In the elevator, we were pretty crammed and I found this spatial promiscuity very bothering; the three porters cynically asked me if I found all this “interesting.” My head started spinning as I was taking in the reality of being near an unknown dead body. The stress and the space restrictions made me more aware of our gender differences (myself a woman and all them male). Arriving at the morgue, they jokingly told me that I could wait somewhere else if I was “unwell.” I felt they had a very dismissive way of talking to me. I felt like leaving would have been a breach of my job and that I would have irremediably lost face. I followed them into the morgue, where they had to check several fridges that were occupied (with other bodies). I had the impression they did this only to tease me. My head started spinning and I finally said that I would wait for them outside.
The power asymmetry in this case is not one deliberately caused by the study participants, though it might have been knowingly indulged by them. It showed the researcher that something as innocuous as observing the work of porters in a hospital is actually more complicated because the activity in itself is all but banal (as one might expect). This challenge is often experienced by researchers doing their fieldwork in domains of knowledge over which they have little to no expertise (Råheim et al., 2016) and its complexity is dependent on the type of research and design (Karnieli-Miller et al., 2019). Indeed, it quickly became an issue of being a witness to death and participating in mortuary preparations. The researcher was faced with the need to “play along,” all the while wondering or feeling that the situation could have been prevented had the participants been more “benevolent.”
Gender stereotypes can also impact on the relationship created between researcher and participants, and be conducive to asymmetries that tilt the situation in the favor of participants (Gurney, 1985). For example, some participants might find it easier to confide in woman researchers (Padfield & Procter, 1996); however, in situations in which the information shared is off topic, this can be experienced as emotionally draining for the researcher (Sampson & Thomas, 2003). Doing field research in settings that are highly gender-segregated can be experienced as challenging for researchers of the opposite gender, who can be faced with a hostile reception expressed through sexism, verbal harassment and physical intimidation. The female researchers Sampson and Thomas (2003, p.180) note on their experience of research on-board cargo vessels, feeling that they were tested by the male participants in order to “pass the test,” feeling the need to reflect on how they could minimize the impact of their gender on the situational risk encountered. Similar compensation mechanisms may be necessary with regard to the age and generation of researchers (Underwood et al., 2010).
Crosscutting Aspects Related to Vulnerability
Based on the autoethnographic reflections presented above, we identified five crosscutting aspects that can increase vulnerable situations for researchers.
Firstly, independently of the researcher’s resilience, doing research on sensitive topics is difficult in itself (Johnson & Clarke, 2003; Malacrida, 2007). Secondly, and relatedly, conducting research with participants in particular vulnerable situations, such as when researching in contexts of poverty and structural violence, where participants lack any adequate support post study, is likely to lead to moral distress among researchers. Thirdly, literature shows that novice researchers are particularly exposed to emotional challenges, especially in the context of conducting research on sensitive health issues (Johnson & Clarke, 2003). Indeed, our autoethnographic vignettes date from the authors’ early days of carrying out research, or being confronted for the first time with a particular setting or with a qualitative methodology. Fourth, we identified the fact of being (or feeling) “alone,” that is, without the support of a supervisor, peers with whom to have formal or informal conversations about difficult situations and conduct, or share responsibility, as being a common underpinning experience of researcher vulnerability. Finally, projects that are deployed at a fast pace and oriented towards short-term outcomes can cause vulnerable situations for researchers as they do not allow sufficient time and space to reflect on potential ethical challenges that might be encountered.
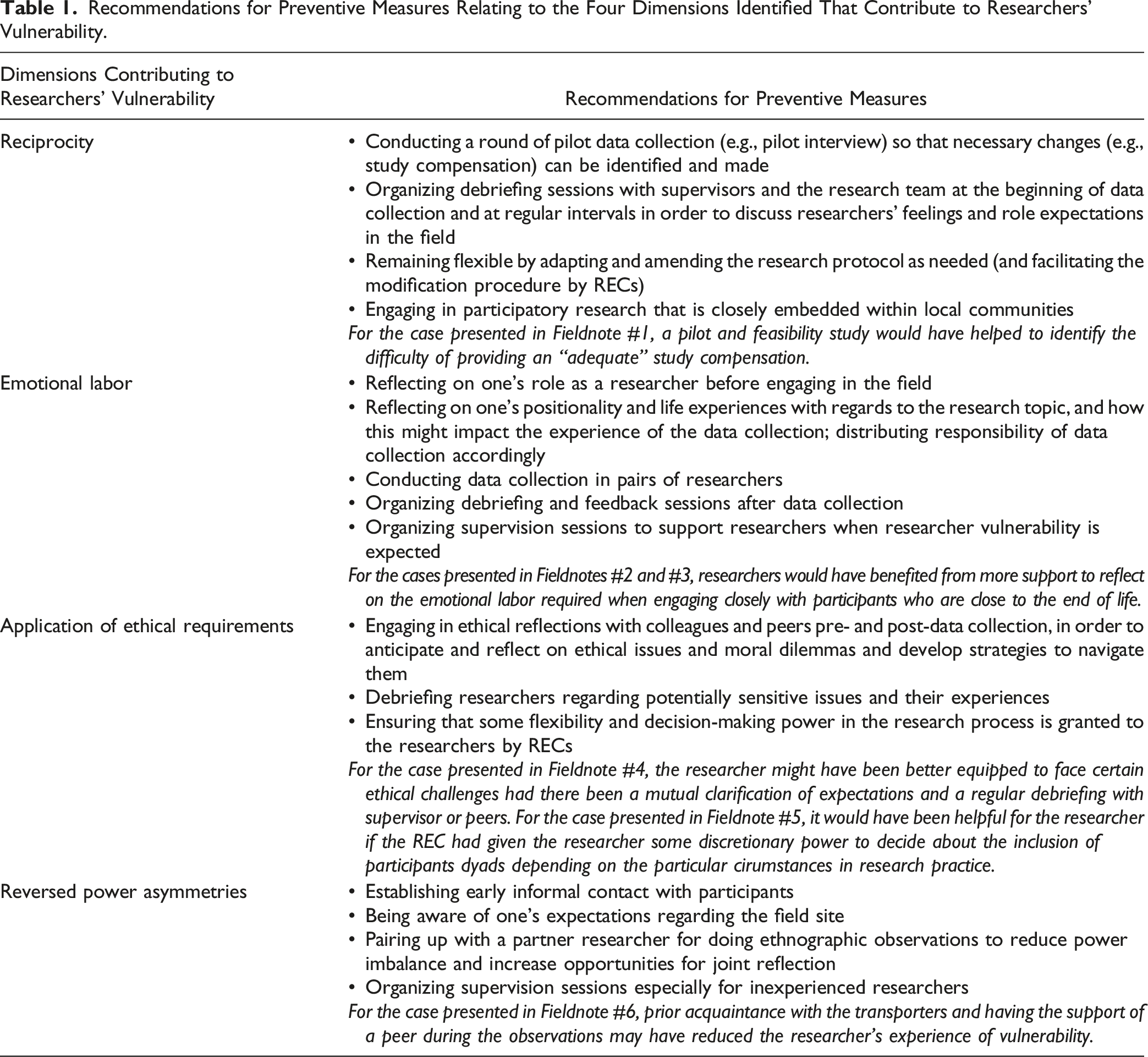
Recommendations
Recommendations for Preventive Measures Relating to the Four Dimensions Identified That Contribute to Researchers’ Vulnerability.
Discussion
This paper presents findings from a reflexive autoethnographic exercise conducted among six qualitative health researchers, showing that qualitative health researchers experience vulnerability in a wide range of circumstances. Firstly, researching disadvantaged and vulnerable populations often leads to an overwhelming desire and felt moral duty among researchers to help their participants (see Fieldnote #1). This may leave researchers feeling morally distressed if they are unable to adequately reciprocate or address participant’s needs in research, which often reflect broader structural and social inequalities. Yet just as reciprocity does not necessarily only focus on pratical aspects, emotional labor is another important component of qualitative research (the second dimension that we identified). Researchers need to mobilize emotional display to build rapport and establish trust. And yet, as shown in Fieldnote #2, needing to display empathy in professional settings can be experienced as a burden. When personal history comes into play and research brings forth one’s own painful experiences, emotional dissonance may be heightened (see Fieldnote #3).
The third dimension relating to researcher vulnerabilility in healthcare research that we identified is related to the application of ethical standards. Due to the diversity and unpredictability of social research, applying a rulebook mentality to ethical regulations is insufficient when it comes to qualitative methods. As such, needing to apply inadequate or insufficient ethical requirements of a REC can also be felt as challenging (as illustrated in Fieldnotes #4 and #5). The realities of research as experienced by field researchers are also often different from those imagined by lead investigators and RECs.
In reality, power is rarely balanced and oscillates from one side to the other. At any time, participants may challenge having the higher ground, and affirm an authority they hold over the researcher (the fourth dimension). Last but not least, as exemplified in Fieldnote #6, personal and contextual conditions can also induce vulnerability in any research situation.
Aspects such as working on particularly sensitive topics, being a novice to research, working in small teams with insufficient support schemes, and in fast-paced projects focused on competitiveness may heighten the vulnerability of researchers. Researchers are required to be sensitive to all dimensions of research that might harm their participants. Participant vulnerability can be managed and minimized through designated procedures and ethical codes of conduct. From a social sciences perspective, vulnerability is a more relational and dynamic concept (Bracken-Roche et al., 2017; Luna, 2009). It is not an imaginary label drawn from shallow, biased, stereotypical understandings of our environment, but a concept rooted in the participants’ understanding and reality, which does not necessarily meet that of RECs (Haggerty, 2004; Holland, 2007). As we argue in this paper, vulnerability is not a static, predetermined, unidirectional process, but concerns both participants and researchers. We argue here that in order to ensure the ethical conduct of research, it is important to also focus on the protection of researchers and better understand the dimensions of researcher vulnerability.
In our reflection on dimensions of researcher vulnerability, we were interested in identifying resources that aided or might have aided us in dealing with the challenges experienced, in order to establish recommendations that we address not only to researchers but also to those accountable for protecting them from such situations: supervisors, research institutions and RECs. We acknowledge, in particular, the role of reflexivity, as one of the cornerstones for achieving ethical qualitative research practice, as it requires us to acknowledge and address our own vulnerability. Like each setting, each researcher is a unique individual with their own sets of lived experience that inform their expectations and positionality. Autoethnographic exercises, such as the one presented here, are particularly useful for zooming in on “ethically important moments” (Guillemin & Gillam, 2004) and aspects related to researcher vulnerability, and are fruitful for identifying resources to better deal with such challenges in the future. While we encourage researchers of all stages to practice reflexivity in relation to their research, we equally highlight the importance of them receiving support and training to do so, especially from their supervisors (Clark & Sousa, 2018) and more experienced peers, and the necessity of flexibility from RECs that allows this reflexivity to be put into practice.
In light of this, Allen and Israel argue that a relevant approach would be for ethics arrangements to “have as a primary objective resourcing the reflective practice of research” (2018, p. 276), meaning that research institutions should focus on nurturing ethical conduct by initiating, encouraging and supporting researchers of all levels to engage in reflective practice and imagination. In this model, research ethics becomes the responsibility of everyone involved in research, recognizing every individual’s unique contribution and challenges. Allen and Israel (2018) identify several resources through which this objective can be achieved: developing collaborative networks; appointing people with skills in qualitative research to chair RECs; developing resources for ethical reflection; teaching social research ethics; and making ethics regulations open to change. Just as the practice of ethics should be democratized to include researchers, so should the notion of “protection from harm” and the conception of vulnerability be extended to include not only participants but also researchers alike.
Limitations
We recognize that an important limitation of this paper is that it mainly focuses on the experiences of the authors and their reflections on the topic. While this approach has been used by many other authors (Gurney, 1985; Øye et al., 2017; Råheim et al., 2016; Rooke, 2016; Sikic et al., 2019; Smith et al., 2023; Tanner, 2009) and is valuable in identifying dimensions of researcher vulnerability, it might not capture the full range of challenges and experiences that researchers in this field encounter. Future research should incorporate more diverse perspectives and experiences, including from different context, disciplines and geographic locations, to provide a more comprehensive understanding of additional dimensions of researcher vulnerability in qualitative health research. We equally acknowledge the need for future research to focus more attention on developing resources aimed at supporting researchers’ ethical reflexivity and reducing researcher vulnerability in practice, including on how to practice reflexivity and to how to improve the ethical requirement of RECs. Recommendations should be further tested and refined to specific research situations. Lastly, we acknowledge that future discussions on the potential benefits of vulnerability, such as fostering reflexivity, empathy and trust with the participants, will make an important contribution to this field.
Conclusion
Qualitative health research often gives way to an exploration of vulnerability, frailty or suffering, which can bear a heavy burden on researchers conducting this research. In this paper, we have presented reflections on different dimensions of researcher vulnerability, guided by our own experiences as qualitative health researchers which revolve around two incremental needs: firstly, that of recognizing the potential detrimental situation in which researchers may find themselves and acknowledging their needs to be protected, and secondly, that of supporting and encouraging self-reflexivity as an essential resource in protecting researchers from harm.
Footnotes
Acknowledgments
We acknowledge the support of the international spring school “Research Ethics in Qualitative Health Research” held at the Institute for Medical Ethics and History of Medicine at Ruhr University Bochum, Germany, as well as the support received from various reviewers.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this paper: The authors declare that this scientific work was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this paper: This work was supported by the German Federal Ministry of Education and Research (no. 01GP2191).