
Abstract
Background
The amount of people on sickness absence due to common mental disorders (CMDs), including depression, anxiety and stress-related disorders, is a concern from societal and individual perspectives. Among the working population in the OECD member states, the point prevalence of having a mental health condition is almost one in five, most of which are CMDs. The lifetime prevalence of CMDs is 50% (Fisker et al., 2022; OECD, 2021). The total costs for mental health conditions including health care expenditures and loss of productivity are estimated to be approximately 4% of gross domestic product in the European Union member states (OECD/European Union, 2022). From the perspective of the individual and in addition to the direct symptoms, CMDs can be associated with reduced capacity to work, sickness absence and/or unemployment. Sickness absence and unemployment can, depending on social security regulations, have negative effects on private economy (Bryan et al., 2021). In Sweden, psychiatric conditions, including CMDs, account for approximately half of all diagnoses in ongoing sickness absence cases. The highest risk of being granted sickness benefits due to CMDs occurs between the ages of 29 and 45 years, thus contrasting to somatic diagnoses in which the risk increases with increased age. In addition, sickness absences with CMDs usually last longer and recur more often than somatic diagnoses (Försäkringskassan, 2020). Hence, supporting people with CMDs on sickness absence to go back to work in a sustainable manner is a key priority for individuals, work organizations and society (OECD/EU, 2018).
The Added Value of a Feasibility Study
Swedish primary care is the first line of psychiatric care for people with CMDs (Sundquist et al., 2017); only around 60% of the working population has access to occupational health services (Arbetsmiljöverket, 2022). Irrespective of the context, general practitioners are responsible for assessing work ability and issuing medical certificates with recommendations to the Social Insurance Agency on the need for sickness absence. Swedish health care has legal responsibility to provide coordination services to patients at risk of becoming sick-listed and those on sickness absence (“The Act (2019, p. 1297) on Coordination Interventions for Patients on Sick Leave,” 2019). The coordination service should consist of personal support for patients, managing internal collaboration within the health care services, and external collaboration with, for example, the patient’s employer, the Public Employment Service, and the Social Insurance Agency (Svärd et al., 2023). The coordination service is not further specified regarding, for example, how to carry out the personal support or which measures to use for collaboration with the patient’s employer. Each Swedish region has to decide on these matters (Björk Brämberg, Holmgren, et al., 2018). In contrast to occupational health services, primary care in Sweden is not primarily organized or staffed to support workplace involvement. This probably affects how clinicians (e.g., GPs, psychologists, occupational therapists) perceive the need to engage in work-directed efforts and how equipped they are to support such measures. The introduction of new ways of providing rehabilitation measures, such as introducing work-directed interventions in primary care, involves societal needs and preferences, clinician skills and resources, and the context in which the measures and policies are implemented. For example, professionals’ use of work-directed interventions is facilitated by their motivation and trust in the intervention (Björk Brämberg, Jensen, et al., 2018). Thus, workplace interventions go beyond the traditional care provided by primary care professionals to sick-listed patients (Finnes et al., 2019).
Work-Directed Interventions
Interventions involving the workplace are commonly suggested measures to reduce the duration of sickness absence spells and improve return-to-work (RTW) (cf. Björk Brämberg et al., 2024; Gabbay et al., 2011; OECD, 2021). Several systematic reviews and meta-analyses have evaluated the effectiveness of work-directed interventions, targeting or involving the workplace, work organization, work conditions and/or occupational case management. These reviews included studies based on specific psychiatric diagnoses (e.g, depression, adjustment disorders) or a collective term for several psychiatric diagnoses (e.g, CMDs or mental health disorders). The interventions were commonly based on the principles of cognitive behavioral therapy (CBT), problem-solving, or adjustment of the workplace (cf. Nieuwenhuijsen et al., 2020) and explored diverse outcomes, for example, sickness absences rates, duration or recurrent sickness absence, or RTW rates (Arends et al., 2012; Axén et al., 2020; Björk Brämberg et al., 2024; Dewa et al., 2015; Joyce et al., 2016; Mikkelsen et al., 2018; Nieuwenhuijsen et al., 2020; Nigatu et al., 2016). The original studies included in the reviews mainly originated from the Netherlands, Norway, Denmark, and Sweden and thus reflect country-specific regulations regarding for example, sickness certification (Axén et al., 2020; Finnes et al., 2019).
The systematic reviews exploring diagnosis-specific interventions reveal that a combination of a clinical and a work-directed intervention can probably reduce the number of sickness absence days among patients with depression (Nieuwenhuijsen et al., 2020). However, combined interventions aimed at facilitating RTW among patients with adjustment disorders did not result in a significant reduction until partial or full RTW, whereas problem-solving therapy significantly enhanced partial RTW at 1-year follow-up compared with non-guideline-based care (Arends et al., 2012). Neither of these reviews reported effects on sickness absence or RTW outcomes ≥12 months (Arends et al., 2012; Nieuwenhuijsen et al., 2020).
Systematic reviews evaluating CBT-based or problem-focused RTW programs including exposure components revealed improved symptoms, decreased sickness absence, and increased RTW up to 12 months for people with CMDs compared with usual care or a wait-list control group (Björk Brämberg et al., 2024; Joyce et al., 2016). Another review revealed that CBT with problem-solving and focus on work did not improve the number of individuals returning to work, but the intervention significantly reduced the number of sickness absence days among people with CMDs compared with usual care (Nigatu et al., 2016). When work-focused CBT and problem-solving skills were provided by occupational health services to people with CMDs the time to first RTW was reduced in comparison with care-as-usual. However, the effect on return to full-time work was not consistent, and CMD symptoms were not improved (Axén et al., 2020). Among patients with mental disorders, work-focused problem-solving interventions delivered by occupational physicians or psychologists had a significant effect on enhancing RTW rates compared with a control group. Although the results were promising, the authors concluded that there is limited evidence that combinations of interventions with work-related problem-solving skills are effective in RTW outcomes (Dewa et al., 2015).
A Problem-Solving Intervention With Workplace Involvement
Recently, two cluster-randomized controlled trials of a problem-solving intervention with workplace involvement have been conducted (PSI-WPI) in primary care (Karlsson, Frantz, et al., 2024), and occupational health services (Keus van de Poll, Nybergh, et al., 2020) among employees on sickness absence with CMDs.
The PSI-WPI contained the following components: inventory and prioritization of the patient’s problems, brainstorming about options and solutions, formulation of an action plan, evaluation, follow-up and relapse prevention conducted by the patient, their first-line manager and a health care professional (Björk Brämberg, Holmgren et al., 2018; Keus van de Poll, Nybergh, et al., 2020). Further, the PSI-WPI applied a participatory approach as defined by Kraaijeveld and colleagues (Kraaijeveld et al., 2013) as a three-part meeting involving the patient, their manager and a health care professional (Björk Brämberg, Jensen, et al., 2018; Keus van de Poll, Nybergh, et al., 2020).
Findings from the primary care trial showed that the intervention was perceived by the health care professionals as a structured method for supporting RTW. Further, the three-part meetings involving the patient, their first-line manager and the health care professional were experienced as supportive in the knowledge transfer although time-consuming (Karlsson et al., 2023). The PSI-WPI had some ethical challenges; the most prominent was the sharing of health- and work-related information at the three-part meeting where meeting the patient had limited control over information sharing (Karlsson, Sandman, et al., 2024).
Regarding the intervention’s effectiveness, a significant reduction in sickness absence was found when delivered by the occupational health services (Keus van de Poll, Nybergh, et al., 2020) and the PSI-WPI was also cost-effective (Keus Van De Poll, Bergström, et al., 2020). However, no significant effect on sickness absence days was found when the intervention was delivered in primary care (Karlsson, Frantz, et al., 2024). Hence, the same intervention yielded different results in different contexts.
Regarding the lack of effective interventions in primary care settings on how to support patients in their RTW processes or how these interventions can be integrated into primary care, researchers and clinicians are referred to the results from qualitative (e.g, Andersen et al., 2012; Joosen et al., 2022) or observational studies (e.g., Lidwall et al., 2018; Spronken et al., 2020; Toropova et al., 2024). These studies provided important knowledge regarding, for example, the motivational benefits for patients when they had a coordinator supporting them in the RTW-process (Saxvik et al., 2022). Although interesting and valuable, these studies did not address the cause – effect relationship and did therefore not inform policy makers or professionals in primary care with knowledge on how to support the target group.
A rigorous feasibility study conducted in primary care settings is needed before conducting another full-scale trial of a complex intervention (cf. Skivington et al., 2021). Such a study could identify potential barriers to and facilitators of work-directed interventions, specifically the PSI-WPI, assess the practicality, and determine necessary modifications in primary care. This protocol describes a feasibility study, in which we will explore how a problem-solving intervention with workplace involvement, should be designed to better fit within the primary care setting.
Aims
The overall aim is to evaluate the feasibility of work-directed interventions delivered in primary care settings, with a focus on a problem-solving intervention with workplace involvement among patients on sickness absence due to CMDs.
Specifically, the study covers two phases. The aims of the first phase are to; (1) explore how coordinators and general practitioners perceive how contextual factors influence their use of work-directed interventions in primary care, (2) explore how coordinators, general practitioners and employer representatives perceive the design, accessibility, usability, and acceptability of a PSI-WPI aimed at reducing sickness absence, and their needs of implementation support.
In the second phase, a problem-solving intervention will be further developed based on the first phase with the aim to; (3) evaluate the feasibility (i.e., recruitment, reach, fidelity, dose delivered, dose received, satisfaction and context) of a problem-solving intervention in the primary care setting with workplace involvement, and its preliminary effects post-intervention on RTW, self-efficacy, and symptoms among patients on sickness absence due to CMDs.
An overview of the study is shown in Figure 1. Overview of the Study’s Phases and Aims
Method
The CONSORT 2010 statement with an extension for randomized pilot and feasibility trials was used to describe the design, methods, and outcomes of the present study (Eldridge et al., 2016).
Study Design
Overview of the Study’s Phases, Aims, Design, Study Participants and Data Collection

The feasibility study’s theoretical framework departs from the Consolidated Framework for Implementation Research (CFIR) (Damschroder et al., 2022) with regard to the development phase, and the framework developed by Linnan and Steckler (Linnan et al., 2002) for the evaluation phase.
CFIR is a determinant framework with a descriptive purpose focusing on factors believed or found to influence the implementation or use of an intervention. The CFIR builds on several implementation frameworks and contains five domains: innovation, outer setting, inner setting, individuals, and the implementation process domain. The innovation domain refers to the program or intervention being implemented. The outer setting refers to the regions and communities in which the inner setting exists. The inner setting reflects the context in which the intervention is implemented. The individuals’ domain contains the roles and characteristics of the individuals taking part (either providing or receiving) in the intervention. The process domain refers to the activities and strategies used to implement the innovation. The CFIR will be applied for a systematic assessment of contextual factors and innovation design (Damschroder et al., 2022). The framework developed by Linnan and Steckler will be used (Linnan et al., 2002) to evaluate process measures about recruitment, reach, fidelity, dose delivered and received, satisfaction and context regarding the third aim.
Setting
The study is conducted in three Swedish health care regions, that is, region Stockholm, region Uppsala and region Västra Götaland. These regions, comprising approximately 4.5 million inhabitants in urban and rural areas, have been purposefully recruited to the current study. The regions comprise approximately 480 primary care centers providing health care to people of all ages. The primary care centers are publicly or privately driven but contracted with and reimbursed by each region.
In Sweden, the mainly tax- and fee-funded social insurance system provides economic compensation and rehabilitative measures to people with reduced work capacity due to disease or injury. People with gainful employment receive economic compensation during the first 14 days of sickness absence (except for one qualification day) from their employer. From day 15, the costs of the benefits are covered by the public and universal Sickness Insurance. A sickness certificate issued by a physician is needed from day 8. Decisions on entitlement to sickness benefits from day 15 are made by the Social Insurance Agency.
Phase 1: Development
Study Participants
A strategic sampling procedure will be applied to obtain a range of opinions and experiences. With regard to the first and second aim, eligible study participants (coordinators, general practitioners and employer representatives) should have participated in a work-directed intervention (either as part of routine care, or part of a study), defined as an intervention targeting or involving the workplace; for example receiving support from a coordinator in a patient’s RTW-process, a coordinator or general practitioner having contact with the patient’s workplace, or collaboration between a coordinator and a general practitioner aimed at supporting RTW.
Recruitment
Eligible study participants are recruited from each of the participating regions and the research group’s networks. Information about the study will be provided by the principal investigator (PI EBB) at meetings with the regions’ representatives, primary care managers, coordinators, and general practitioners. Further, the PI and the research group will provide oral and written information. Those expressing interest in participation will receive written information and will be followed-up by email or telephone contact.
Coordinators and general practitioners recruited to focus groups regarding the first aim will also participate in the second aim.
Data Collection
Data will be collected by focus group interviews because of the interactive and explorative character of this form of data collection. The focus group setting will provide the study participants with opportunities to identify and discuss their perceptions about work-directed interventions, their views of organizational and individual level factors that hinder or facilitate their use of work-directed interventions, and more specifically, the development and usability of the problem-solving intervention with workplace involvement (Kitzinger, 1995).
An interview guide will be developed to explore how the study participants perceive the contextual factors influencing their use of work-directed interventions (aim 1), starting with the CFIR domains: the outer and inner settings, individual’s domain, and the implementation process. The CFIR domain innovation design will be applied to explore the study participants’ perceptions about the design, accessibility, usability, and acceptability of a problem-solving intervention with workplace involvement (aim 2) (Damschroder et al., 2022).
In addition, the interview guide will be further developed based on previously used interview guides adjusted to the clinical context, the contextual knowledge related to CMDs, and work-directed interventions (cf. Holmlund et al., 2020; Holmlund et al., 2022). The interview guide will start with demographic questions (profession, basic education and training, work experience in years), followed by organizational and individual level challenges. Examples of organizational level challenges are the interaction between the primary care context and the intervention (how does the intervention fit within routine primary care?), and organizational requirements for delivering the intervention (resources, guidelines, insurance medicine decision aid). Examples of individual-level challenges are the participants’ attitudes to the intervention, interprofessional collaboration, competence, training and support needed to provide the intervention (cf. Nielsen et al., 2018). The guide will also include questions regarding suggestions for improved usability of the problem-solving intervention.
Overview of the Problem-Solving Intervention With Workplace Involvement, With Suggested Modules, Content, Assignments and Patient, First-Line Manager, Primary Care Professional Involvement

Each focus group will be moderated by an experienced focus group leader and a co-moderator and will be recorded and transcribed verbatim. The coordinators, general practitioners and employer representatives will participate in separate groups to avoid a power imbalance in the groups. About three focus groups (i.e., one group from each region) with coordinators, general practitioners, and employer representatives will be conducted, with approximately 5–7 participants in each group.
Data Analysis
Qualitative, thematic analysis are used for interpretation of the data (Braun et al., 2006). The initial steps of the analysis will be data driven: (a) familiarization with the data; (b) generating initial codes, and (c) searching for themes. Then, the CFIR framework will be applied to further elaborate on the preliminary themes (Damschroder et al., 2022).
Based on the data analysis and the results from the first and second aims, the problem-solving intervention will be further developed by the research group and adjusted to the primary care context or specific patient groups.
Phase 2: Evaluation
Recruitment and Study Participants
Coordinators and/or General Practitioners
Recruitment takes place in primary care centers in each region. Information about the study will be provided by the PI in meetings with primary care managers, coordinators and general practitioners.
Coordinators and general practitioners will be eligible if they work ≥50% at a primary care center and have ≥1 year of work experience in their basic profession. Exclusion criteria: upcoming leave of absence (e.g., pregnancy leave, sabbatical) or retirement.
Study participants will take part in a 2-day training course on the problem-solving intervention. The training is provided by the research group. The study participants will complete a questionnaire about the quality of the training course and their problem-solving skills before and after the course. The study participants will be supported by a manual and work-sheets developed by the research group based on research into CMDs, the problem-solving intervention, and coordination of RTW.
Patients with Employment on Sickness Absence
The current feasibility study will include up to 40 patients with employment who are on sickness absence and recruited from primary care centers in three Swedish regions by primary care professionals (e.g., general practitioners and coordinators). Patients who fulfill the inclusion criteria will be invited to participate in the study by email. Eligible participants will receive written information about the study, and how to contact the PI (EBB) for additional questions before providing written consent to participate.
Those eligible will be included if they meet the following inclusion criteria: patients aged 25–60 years, ongoing sickness absence (at risk of long-term sickness absence with a maximum of 26 weeks) due to mild to moderate depression (F32.0, F 32.1), anxiety (F41.1, F41.2, F41.3), adjustment disorder (F43.2) or reactions to severe stress including exhaustion disorder and other non-specified reactions to severe stress (F43.8, F 43.9) as the primary diagnosis for sickness absence diagnosed by a physician according to the Swedish version of the International Statistical Classification of Diseases and Related Health Problems, Tenth Revision (ICD-10); understand written and spoken Swedish.
Exclusion criteria: patients with severe depression, other severe mental disorders (psychotic or bipolar disorders, or referral to a psychiatrist), pregnancy.
Outcomes
Overview of Outcomes Measured at Baseline, During and Post-Intervention
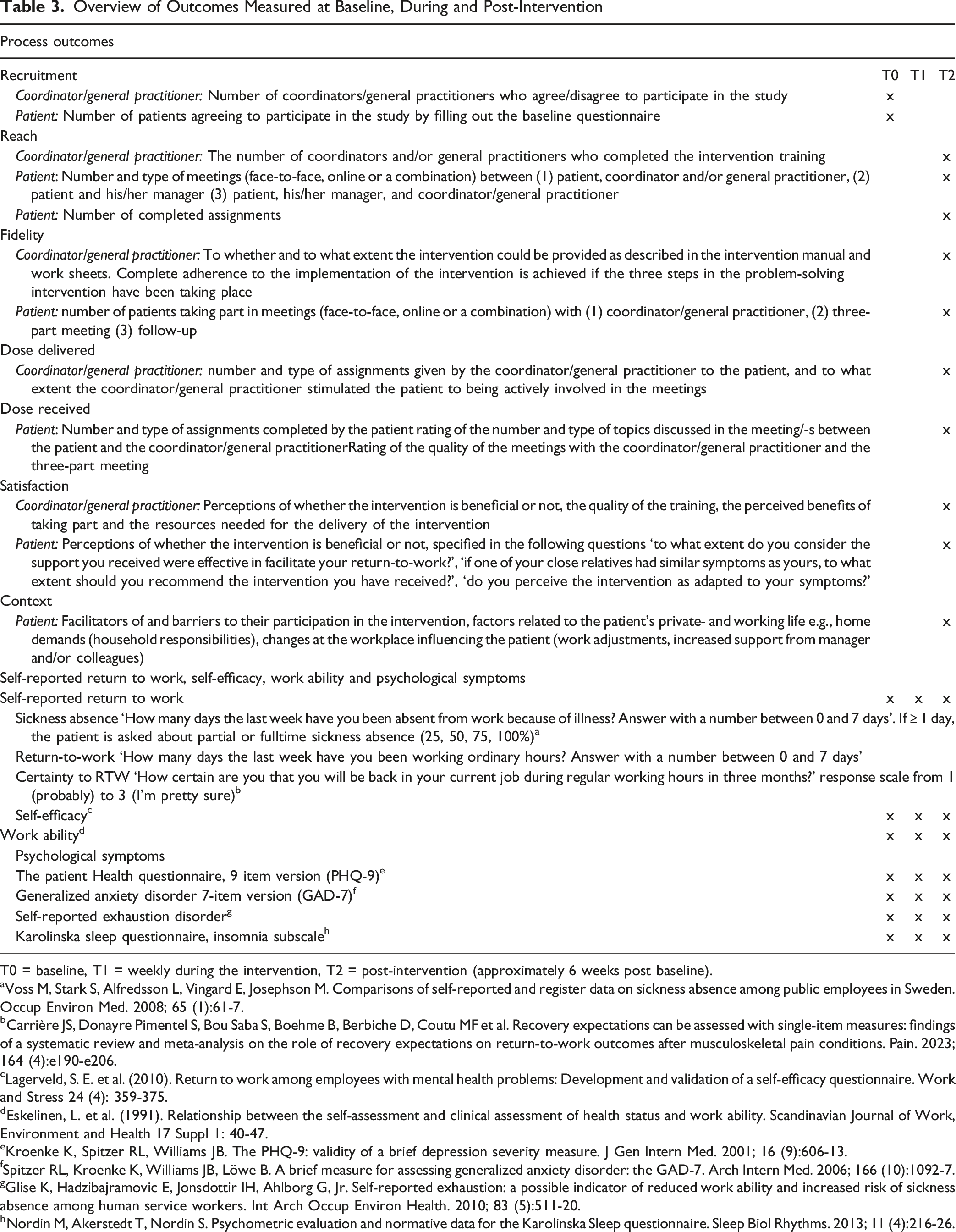
T0 = baseline, T1 = weekly during the intervention, T2 = post-intervention (approximately 6 weeks post baseline).
aVoss M, Stark S, Alfredsson L, Vingard E, Josephson M. Comparisons of self-reported and register data on sickness absence among public employees in Sweden. Occup Environ Med. 2008; 65 (1):61-7.
bCarrière JS, Donayre Pimentel S, Bou Saba S, Boehme B, Berbiche D, Coutu MF et al. Recovery expectations can be assessed with single-item measures: findings of a systematic review and meta-analysis on the role of recovery expectations on return-to-work outcomes after musculoskeletal pain conditions. Pain. 2023; 164 (4):e190-e206.
cLagerveld, S. E. et al. (2010). Return to work among employees with mental health problems: Development and validation of a self-efficacy questionnaire. Work and Stress 24 (4): 359-375.
dEskelinen, L. et al. (1991). Relationship between the self-assessment and clinical assessment of health status and work ability. Scandinavian Journal of Work, Environment and Health 17 Suppl 1: 40-47.
eKroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001; 16 (9):606-13.
fSpitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006; 166 (10):1092-7.
gGlise K, Hadzibajramovic E, Jonsdottir IH, Ahlborg G, Jr. Self-reported exhaustion: a possible indicator of reduced work ability and increased risk of sickness absence among human service workers. Int Arch Occup Environ Health. 2010; 83 (5):511-20.
hNordin M, Akerstedt T, Nordin S. Psychometric evaluation and normative data for the Karolinska Sleep questionnaire. Sleep Biol Rhythms. 2013; 11 (4):216-26.
Data Collection
Data is collected by self-reported questionnaires and text messages. The baseline questionnaire includes questions on demographic information, job characteristics (job demands, resources, and opportunities for adjustments in their work situation), and which treatments for CMDs the participants have received (e.g., psychopharmacological treatment, psychotherapy).
Data Analysis
Feasibility measures will be reported with descriptive statistics (recruitment, reach) in the process evaluation. The effects of time on outcome measures self-reported RTW, self-efficacy, and work ability are analyzed with linear mixed models with random intercept and slope. Data on fidelity to the treatment protocol is included as a predictor in the models in order to analyze the dose-response relationship. Psychological symptoms and sleep quality are included as covariates in the models. The findings are integrated with the findings of the process evaluation.
Ethical Considerations
Ethical approval has been obtained from the Swedish Ethical Review Authority, reference number 2024-00932-01. All participants will receive written and oral information and provide written informed consent to their participation. The oral and written information stresses the voluntary nature of the participation and that the participant may withdraw their participation at any time without stating a reason. The involvement of the patient’s first-line manager might pose an ethical challenge in relation to the patient’s autonomy and privacy. This ethical challenge is handled by the written and oral information provided by the research group before consent to participation.
There are no stopping guidelines (Tyson et al., 2016) in this study. However, patients have regular meetings with health-care professionals during the intervention and are closely monitored during and after the intervention by the research group. Hence, this study is of low risk.
Discussion
This paper presents the design of a feasibility study, in which we aim to elaborate the feasibility of work-directed interventions in Swedish primary care with a specific focus on a problem-solving intervention with workplace involvement. The study will elaborate on whether, and to what extent, the intervention is received and accepted by those using and receiving it, and facilitators and barriers to the implementation.
The effectiveness of work-directed interventions aimed at reducing sickness absence or increasing RTW is incongruent. Research reported in gold-standard systematic reviews, meta-reviews and randomized controlled trials has failed to find effective measures (cf. Björk Brämberg et al., 2024; Nieuwenhuijsen et al., 2020). Most studies evaluate interventions at the individual patient level with positive effects on symptom assessment but not on outcomes such as sickness absence and RTW. Work-directed interventions usually combine individual measures with employer contacts. These work-directed interventions seem to have a slightly better effect on sickness absence and RTW. Thus, it is reasonable to continue that line of research. However, work-directed interventions are complex; that is, delivered and evaluated at different levels, including individual, organizational, and societal levels. It is difficult to identify effective or non-effective mechanisms. There are only a few feasibility studies that dig deeper into the experiences of the stakeholders involved, scrutinizing all levels of importance for the success of a complex clinical trial.
The study applies a feasibility design with qualitative and quantitative methods. The study’s rigor will be ensured and maintained during the research process by using high-quality research methodology in every step (e.g., sampling, data collection, analyses) by an interdisciplinary research group. Further, transparent reporting of the research process and findings will be done in accordance with the study protocol and reporting guidelines (Eldridge et al., 2016; Tong et al., 2007). The detailed descriptions of the study design presented in the current protocol will facilitate the judgement of transferability of the results (Williams et al., 2009).
Our research group has identified an urgent need to take stock before moving forward. Through a thorough analysis of the perspectives of professionals and employer representatives on delivering primary care based work-directed interventions in general, and more specifically, the problem-solving intervention with workplace involvement, this study will establish whether the use of these interventions is in line with the goals of primary care and contextual factors influencing the professionals’ use of such interventions when supporting their patients and employees in RTW.
Footnotes
Ethical Approval
Ethical approval has been obtained from the Swedish Ethical Review Authority (ref. No. 2024-00932-01). Eligible study participants will receive written and oral information regarding their participation. Written consent will be obtained from all study participants.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study is funded by The Swedish Research Council for Health, Working Life and Welfare (reference number 2023-01488). The funder has no role in the design of the study, data collection, analysis, or interpretation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data Availability Statement
The current article describes a study protocol, and therefore data sharing is not applicable as no datasets have yet been generated or analyzed.