
Abstract
Introduction: Only about half of the patients treated with Cognitive Behavioural Therapy (CBT) for depression are in remission after treatment. Progress monitoring during therapy, supplemented with clinical support tools, has shown promising results with regard to improving outcome, but results for group psychotherapy are less favourable. Therefore, we propose supplementary individual therapy as a possible solution to lack of progress in group CBT. The current study seeks to develop a brief add-on course of personalized individual therapy for patients showing lack of improvement during CBT group therapy. Methods and analysis: We aim to develop an intervention that includes progress monitoring, clinical support tools and a selection of patient-centred add-on interventions. An initial multiple case study will involve patients treated for depression in group CBT. The patients will perform progress monitoring every week, and therapists will receive alerts when a patient is not improving. Analyses will integrate qualitative data on the experiences of therapists and patients, quantitative tracking data, and initial clinical assessments. Based on these analyses, the proposed add-on interventions will be further developed and offered to the patients who are persistently not improving (pNOT) in three new CBT groups, which will be monitored as described above. Interviews will be performed with patients and therapists to explore their experiences of the new interventions. Qualitative data will be analysed through thematic analysis, and Single Case Experimental Design analyses will be made based on daily tracking of WHO-5.
Introduction
Background and Rationale
Despite the existence of numerous well-established psychotherapeutic treatments, research shows that only about 50% of patients suffering from depression recover after psychotherapeutic treatment (Cuijpers et al., 2014) and up to 10% of cases actually deteriorate (Cuijpers et al., 2018). This is also seen following evidence-based cognitive behaviour therapy (CBT) delivered in groups as currently done in Danish Mental Health Service (Reinholt et al., 2021). Since treatment failure might result in patients’ continuing suffering and societal costs of prolonged psychiatric service and lost productivity, it is critical to (a) identify patients at risk of treatment failure and (b) tailor appropriate interventions for these patients.
With regard to the identification of potential treatment failures, research shows that clinicians are not good at predicting which patients will end unremitted (Hannan et al., 2005; Shimokawa et al., 2010). Accordingly, it has been proposed to routinely monitor the patients’ symptom status from session to session in order to ensure that the patients improve continuously.
Several treatment approaches incorporate progress monitoring in order to detect when the patient is Not On Track (NOT) (Boswell et al., 2015; Connolly Gibbons et al., 2015; Lambert et al., 2005; Lambert et al., 2018; Lutz et al., 2015; Moltu et al., 2018). The term NOT is typically used within the feedback tradition where therapists are alerted if the patient, according to preset algorithms, deteriorates or stays unchanged (De Jong et al., 2014). A majority of progress monitoring studies demonstrate superior effect specifically for the subgroup of NOT patients in RCTs comparing progress monitoring versus treatment as usual (Shimokawa et al., 2010). However, other studies indicate less promising results and no effect in psychiatric settings (Østergård et al., 2020). Moltu et al. (2018) studied perspectives of therapists and patients to explore how progress monitoring can be helpful and acceptable to them. Patients experienced that progress monitoring has the potential of demonstrating to the patient that positive change has actually happened, which can give hope. Also, therapists and patients expressed that progress monitoring can aid in making the therapy goal oriented. However, other qualitative studies pointed to some challenging issues, like lack of meaning for the patients (Solstad et al., 2019), or lack of engagement from the therapists (Lucock et al., 2015), or even discouragement among therapists (Errázuriz & Zilcha-Mano, 2018). Studies of progress monitoring in group therapy have showed mixed results, probably due to the difficulty of adapting the group format to the individual needs of the patients (Davidsen et al., 2017; Koementas-de Vos et al., 2018; Marmarosh, 2018; Tasca et al., 2019).
All in all, progress monitoring may not be sufficient in itself to lead to substantial differences in treatment and to change outcome (Koementas-de Vos et al., 2018), perhaps because therapists are not necessarily able to identify the clinical challenges to progress and implement adequate changes in the therapeutic course. For this reason, many studies provide therapists with a Clinical Support Tool (CST) for NOT cases containing clinical advice for a range of scenarios. The CST can also be based on supplementary questionnaires and an algorithm determined recommendation based on the patients’ responses to these (Koementas-de Vos et al., 2018). However, in some cases, providing therapists with CST is not helping the patient get ‘back on track’ in therapy (Connolly Gibbons et al., 2015; Koementas-de Vos et al., 2018). If this is the case, the patient can be defined as persistently NOT (pNOT).
In accordance with the call for ‘personalized’ psychotherapy, a way to improve outcome of treatment for depression would be to individualize treatment for patients at risk of poor outcome (Cuijpers et al., 2016). Understanding more about factors associated with response to therapy may eventually enable clinicians to tailor therapy to the individual from the onset of therapy (Carter et al., 2018), but until then, we can attempt to optimize treatment depending on the individual’s response during the course of therapy (Lambert et al., 2018; Tasca et al., 2019). In the case that a patient is pNOT in therapy, an alternative treatment strategy based on the patients’ preferences might be helpful (Moeller et al., 2021).
In the present project, we propose a routine monitoring procedure tracking the symptom level before each session, thereby allowing the detection of patients who do not improve sufficiently during treatment. Furthermore, we pursue the development of add-on interventions to the standard CBT offered in Danish mental health services that can be applied concurrently with the course of group CBT in cases where a patient is pNOT.
The research question we will follow is: How do patients and therapists experience lack of improvement in group CBT for depression, and which interventions will be associated with increased rates of improvement?
Objectives
The main objective of the project is the development and initial test of a set of individual person-centred add-on interventions to group CBT to be delivered in case of observed lack of progress or deterioration. The project comprises two sub-studies:
Research Objectives Substudy 1 – Discovery:
• To understand how therapists and patients experience and explain patients’ lack of improvement during group CBT for depression. • To create knowledge about the needs and preferences of patients and therapists when a patient is not improving in group CBT, and how they would accommodate these in the treatment. • To develop add-on interventions relevant for NOT patients.
Research Objectives Substudy 2 – Initial Feasibility:
• To create knowledge about how pNOT patients experience individual personalized add-on interventions to group CBT for depression. • To learn if personalized add-on interventions are associated with a positive outcome for patients who are pNOT in group CBT for depression.
Hypotheses
Within both sub-studies we have embedded a small-n Single Case Experimental Design (SCED), see below.
• After introduction of CST, 50% of NOT patients will achieve a mean increase of 10 WHO-5 points, compared to their own pre-CST scores.
• At the end of the individual add-on interventions, 50% of pNOT patients will achieve a mean increase of 10 WHO-5 points, compared to their own pre-add-on intervention scores.
Methods
Study Design
The overall project follows the phase structure suggested by Gitlin (Gitlin, 2013) and accordingly it is divided into phases consisting of different methodologies. Presently, we aim to conduct the discovery phase (substudy 1) and a phase where the feasibility of our intervention will be tested (substudy 2), see Figure 1. Timeframe for the two DIPNOT Sub-Studies.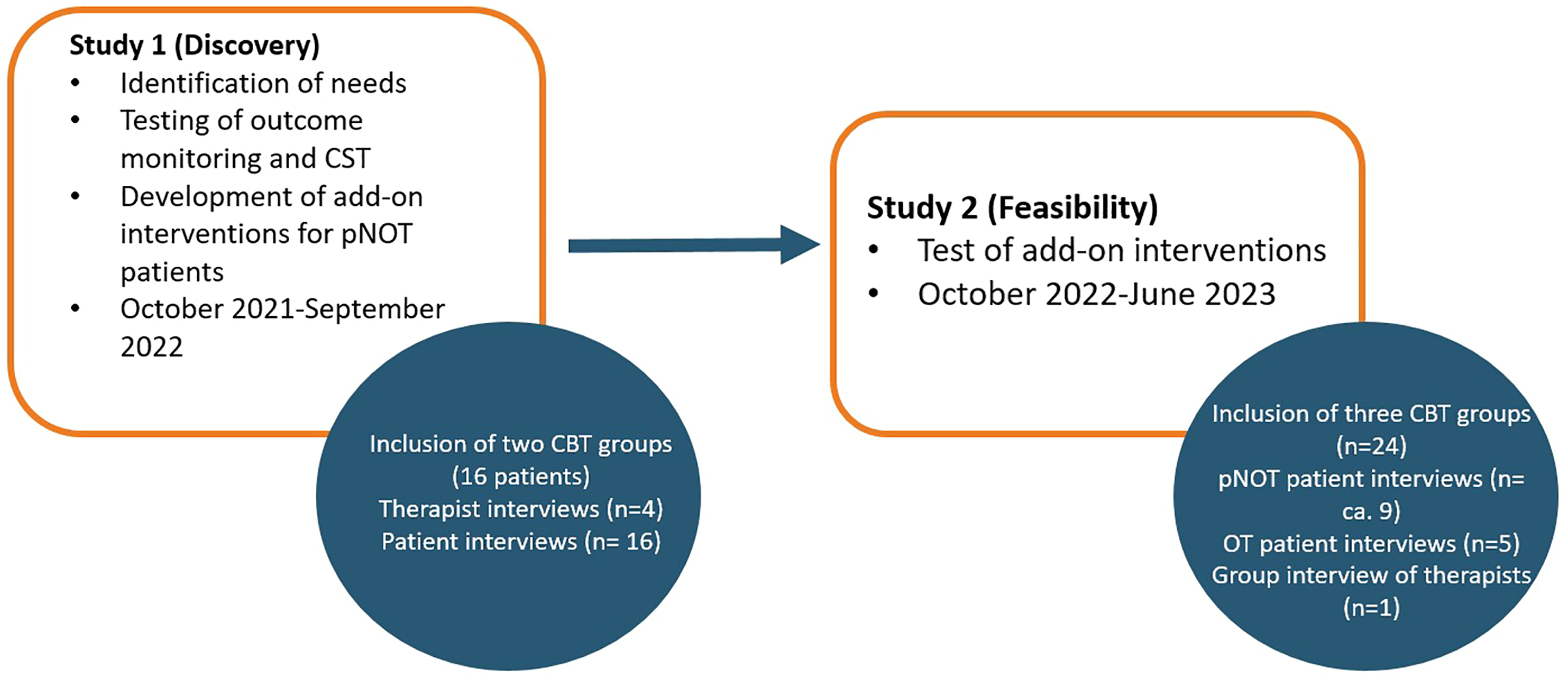
The discovery phase encompasses a mixed-method, exploratory multiple case study where each case is analysed both qualitatively and quantitatively. The case material will be analysed with a particular focus on identifying key possible interventions that could have improved the outcome of therapy. Relevant new add-on interventions will be detailed in collaboration with therapists and the user panel and appropriate training work shops will be carried out for substudy 2 therapists. A priori, we have three suggested add-on interventions, but these will be subject to modification, depending on the results of substudy 1 (see supplementary material).
In substudy 2, we determine acceptability, feasibility and safety of the resulting interventions (Gitlin, 2013). Here, we again apply a case study design on pNOT cases, and add post-treatment group interviews with each CBT group and the therapists to access their experiences of the treatment, and their suggestions for improvement.
Both sub-studies will additionally involve a quantitative Single Case Experimental Design (SCED). The design is popular when investigating psychotherapy before engaging in larger research projects as RCT’s (Renner et al., 2016; Withiel et al., 2020). SCEDs cannot inform about the representativeness of the results in a greater population. However, SCED has good external validity and the effectiveness of the add-on interventions within participants can be evaluated (Moeyaert et al., 2014).
Setting
The interventions will be conducted in public, free-of-charge outpatient mental health clinics in the mental health services in Denmark. The mental health services’ target population is patients with depression that have not remitted following two attempts of pharmacological or psychotherapeutical treatment in the primary sector or cannot maintain improvement. Outpatient treatment for moderate to severe depression is standardized in accordance with the Danish Health Authority guidelines (Danske-Regioner, 2017). This implies that most patients with depression are offered 12–14 sessions in group CBT.
Participants and Recruitment
Substudy 1 will include 16 patients and four therapists and substudy 2 will include 24 patients and six therapists. In study 1, all patients and therapists will be interviewed individually. In study 2, pNOT patients and eight On Track (OT) patients will be interviewed individually, while all therapists are interviewed in a group. All patients will be assessed at inclusion and will carry out progress monitoring.
Patients are eligible if they (1) have a clinically established primary diagnosis of depression (Unipolar Depression or Recurrent Depression), (2) are offered group CBT in mental health services, (3) have a smartphone and (4) have given informed consent. Eligibility will not be determined by presence or type of medical treatment, but stability of dose should be achieved at onset of the baseline period (i.e. the consultant has deemed the antidepressant type and dosage to be optimal, and dosage has been unchanged for 3 weeks).
Therapists will inform the researcher when patients meet inclusion criteria and have agreed that the researcher can contact them. The patients are invited to a meeting where the researcher provides information about the project and the patients sign an informed written consent form.
Assessment and Outcomes
Assessments, Questionnaires and Progress Monitoring.

Procedures
After giving informed written consent and completing the inclusion assessment, patients are instructed to begin to fill out progress monitoring on the Monsenso app (see Figures 1 and 2). When the baseline data collection period is finished, therapy will start following the standard Danish group CBT protocol for depression (Due-Madsen, 2008) and conducted by trained CBT therapists. One or two weeks after the therapy has ended, patients will participate in semi-structured interviews, where the visual graphs of tracking data will be included as an anchor point for the interview about the patient’s experience of the treatment. After the interviews with patients, interviews will be made with the patients’ therapists (see Figures 1 and 2). Study 1 and 2.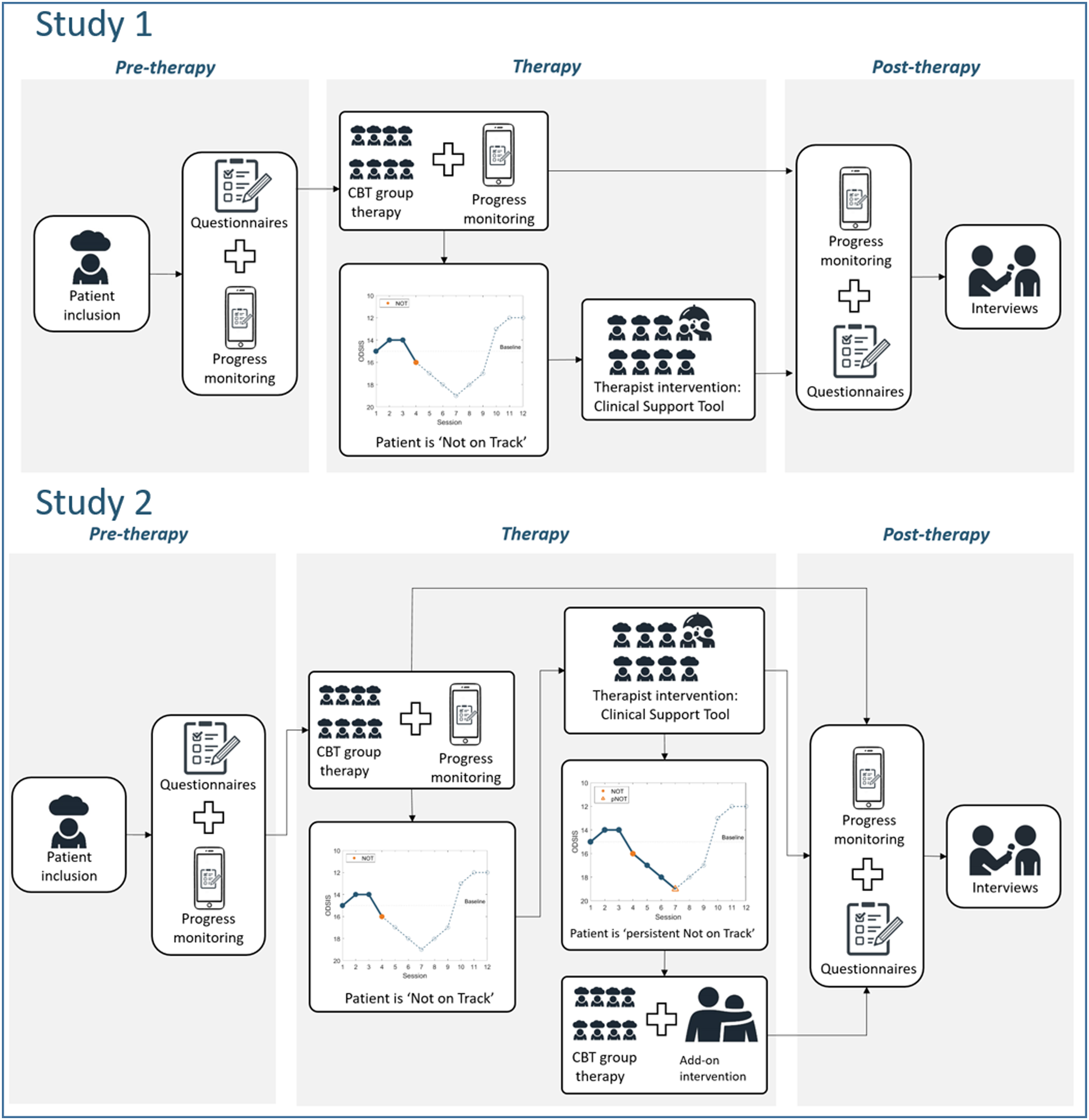
Progress Monitoring and Alert Definition
The progress monitoring will be depicted as a graph for the patients on their smartphone app, and for the therapist and researcher on the Monsenso© website for clinicians. The researcher, a clinical psychologist, will monitor the progress monitoring and alert the therapist if patients are NOT.
It is not straightforward to assess that patients are NOT. In recent validation papers on ODSIS, the diagnostic cut-off is reported quite dissimilarly (5, 8 and 11), while standard error is reported relatively uniformly 0.30–0.65 (Bentley et al., 2014; Ito et al., 2015; Mira et al., 2019). In study 1, patients will be considered NOT if they score 3 ODSIS points lower than their baseline at any point in their treatment (de Jong et al., 2012, 2012b), or if no change (i.e. < 2 ODSIS points) occurs for 3 sessions in a row (Koementas-de Vos et al., 2018). The choice of 3 sessions is pragmatic, providing time to observe stability of lack of progress, and yet not wasting too much time of the 14-week group course. For study 2, pNOT is defined by no change (i.e. <2 ODSIS points) or ODSIS points lower than baseline measurement (>3 ODSIS points) occurring for 3 sessions in a row after the first alert.
Interventions
Group Cognitive Behavioural Therapy
CBT is designated as the gold-standard treatment for depression (National Institute for Health Clinical Excellence, 2004). In the current study, the treatment is based on an adapted version of a Danish group CBT manual (Due Madsen, 2008). Traditional CBT suggests that there is a connection between thoughts, feelings and behaviour (Beck, 1979). This entails that, for example, by changing cognitive beliefs that cause psychological distress, we can change unhelpful behaviour (Beck, 1979).
Substudy 1: Clinical Support Tool (see Figure 2)
When a patient is NOT, the therapist will be alerted in order for the therapist to respond to the situation. The therapist will receive an overview of the patient’s results from the weekly questionnaires. She is encouraged to seek guidance from co-workers, team psychiatrist or supervisor. Furthermore, a CST based on Koementas-de Vos et al. (2018) will be applied. The suggested CST contains clinical recommendations concerning life events, group climate, group cohesion and working alliance. For example, if the questionnaire reveals that the patient experiences the therapeutic alliance as weak, an example of a recommendation could be that the therapist should help the patient express negative feelings about therapy and respond in an open or nondefensive manner, while accepting responsibility for own contribution to the interaction (Koementas-de Vos et al., 2018).
Substudy 2: Clinical Support Tool and add-on individual sessions (see Figure 2)
When a patient is NOT, the therapist will be alerted and given CST as described above. If a patient is pNOT (i.e. remains NOT after application of CST) she will be invited to an individual decision session with one of the group therapists, where different therapeutic options for a small series (5 sessions) of additional individual sessions will be presented for collaborative treatment planning.
Presently, these add-on interventions are conceptualized as a tentative framework for three types of personalized interventions, based on the presenting problem and patient preferences. The framework is a simplification of the causes of pNOT divided into three main elements and their possible therapeutic solutions: Unrecognized psychopathology of the patients – managed by therapeutic assessment and, potentially, supplementary pharmacological treatment; Problems in the patients’ environment and social life outside therapy – managed by network-based problem-solving; Therapy hindering psychological processes – managed by collaborative case-conceptualization (see supplementary material). However, the interventions will be adapted in accordance with the findings of substudy 1 to meet the most salient needs of the patient population in treatment.
Therapist Training
Group therapists in the participating CBT groups will receive training in the interventions of the study. This includes a workshop in progress monitoring and CST, and a three-day workshop in the content of the individual add-on interventions decided upon after substudy 2. The training in study two will be conducted by relevant experts within the field of each add-on intervention.
Data Collection and Analysis
Psychotherapy is a complex and interactive process, where contextual conditions to the phenomenon under study and the boundaries between the phenomenon and context often are unclear (McLeod, 2010). Since case studies provide an efficient way of representing and analysing complexity these can be seen as an ideal opening approach for this project. Fishman (2012) argues for combining different case-study models and thereby enhancing the knowledge produced by each. The discovery phase of this project can be seen as a combination between a quantitative case analysis and a Narrative Experience Case Study, as the patient’s symptom level in each session is measured and depicted in a time-series graph. The Narrative Experience Case Study focuses on exploring the narrative experience and personal meaning of the therapy from both the client’s and therapist’s viewpoints (Fishman, 2012). In this manner, the analyses will comprise both quantitative baseline descriptives, course descriptives and qualitative data.
Interviews and Case Study Analysis
Interviews will be carried out after the end of the CBT groups. In case of premature drop-out or discharge they will be conducted as soon as possible. Interviews will be digitally recorded and transcribed verbatim. Interviews will centre around graphical displays of the patients’ progress monitoring. The interviews will take place in the psychiatric clinic or in the patients’ homes.
Substudy 1:
• Interviews with all the participating patients: After the end of treatment, the researcher will conduct interviews with each patient about experiences of progress, relapse, or being NOT. • Interviews with therapists: After interviewing the patients, interviews with the patients’ therapists will be conducted concerning the therapists’ experiences of the patients’ progress during therapy.
Substudy 2:
• Interviews with pNOT patients: After the end of treatment, the researcher will conduct interviews with the pNOT patients concerning their experiences of progress monitoring and the add-on interventions. • Interview with 8 OT patients: After treatment, patients who were OT will be interviewed about their experiences of progress monitoring and the intervention where some of the patients received add-on interventions and some did not. • Group interview with therapists: Therapists will be interviewed in a group concerning their experiences of the progress monitoring and add-on interventions.
The interviews will begin with open explorative questions and then continue with more specified theory-based questions investigating factors known to affect therapy outcome, as mentioned above, and psychological therapy-hindering issues such as those proposed by Constantino et al. (2013). The graphs discussed will include tracking of ODSIS, significant life events, personalized items, and therapeutic alliance, group climate and group cohesion as measured by the Group Questionnaire.
The interviews will be transcribed, anonymised and analysed in NVivo, version 12. A rich case record will be assembled for each patient, incorporating clinical features, tracking data, outcome measures and follow-up interviews with patients and therapists. The case materials will be analysed to identify key (un)helpful processes in the course of therapy. In substudy 1, the analyses will have an additional focus on possible interventions considered helpful, and in substudy 2, the analyses will have an additional focus on the patients’ experiences of the add-on interventions. The patient and therapist interviews will be analysed using thematic analysis (Braun & Clarke, 2006). Thematic analysis is a 6-phase process and aims to identify patterns within data. A cross-case text analysis, involving the full project group in discussions, will be used to highlight common themes and tendencies across the cases. The project group consists of both clinicians and researchers with experience in analysing qualitative data. In case of disagreements, we will try to reach consensus through discussions. Ultimately, we will expand the discussion group with external support. One researcher will be responsible for the analyses and will invite the project group to regular meetings while the analyses are being conducted.
Quantitative Data Collection and Analyses
SCED analyses will be based on daily app-based tracking of well-being applying the WHO Well-Being Index (WHO-5). WHO-5 is a self-report measure of positive mental health. Respondents rate five items on a 6-point scale from ‘all the time’ to ‘at no time’ concerning their well-being. WHO-5 has shown to have good internal consistency (Löwe et al., 2004; Newnham et al., 2010) and high convergent associations with other measures of well-being (Bech et al., 2003). Also, WHO-5 has shown good sensitivity and specificity when predicting major depression (Byrne et al., 2012).
The SCED encompasses three phases: baseline, first period of group therapy before add-on intervention (CST or add-on individual sessions) and second period of group therapy following these. During a three week baseline, frequent collection of WHO-5 averages out temporary deviations in the patients’ state and determine any cyclic fluctuations (McLeod, 2010). This makes it possible to analyse significant differences in WHO-5 mean and trend between phases (Kratochwill & Levin, 2014). For this study, all data will be subjected to a hierarchal linear modelling analysis (Kratochwill & Levin, 2014).
In substudy 2, the main outcome at end of treatment will also be analysed in a repeated measures ANOVA, reporting simple pre-post effect-sizes, and the proportion of patients in remission, defined as BDI-II at end of therapy being less than 14 points, will be calculated.
User and Stakeholder Involvement
The project includes qualitative interviews with patients and in this way the project gives a voice to users of psychiatric treatment. Furthermore, between every phase of the project, results will be presented for a user panel to ensure comprehension and further application of the results. The user panel consists of people with personal experiences as patients in outpatient psychiatry.
Ethics
The protocol has been approved by the Regional Data Security Agency (approval number REG-044-2021). Participants of this study must sign an informed consent form. No negative effects are expected from the assessment or interviews, but we will argue that interviewing patients with no remission after ended therapy can potentially have ethical consequences. Therefore, patients in study 1 participating in post-treatment interviews and having a poor treatment outcome will be offered extra therapy sessions. Information concerning the included patients will be protected according to the Act on the Processing of Personal Data and the Patients’ Right Act. All data will be saved on a secure regional sharepoint.
Rigor
In order to enhance credibility of the analyses, the researchers will continuously be encouraged to relate to their own preconceptions and position as researchers. The project group will participate in regular meetings where analyses will be discussed, and we will make sure that everyone in the project group reads at least three transcripts of the interviews individually before discussing the content. Two researchers will have read all transcripts before the meetings in order to enhance intersubjective reliability (Brinkmann & Kvale, 2008). One researcher will make sure that all decisions will be written down in details. She will stay reflexive of her own position and write down personal thoughts and hypotheses concerning the topic prior to data collection.
The analyses will be conducted under the supervision of experienced qualitative researchers and will be presented to a user panel where people who themselves have participated in group therapy for depression will give feedback. We will furthermore make sure that the participants’ own words are presented in future papers and presentations. By including demographics, results from clinical assessments and curves from progress monitoring as well as information about outpatient psychiatry in Denmark and the specific clinics in the multiple case studies, we aim to provide a thick description of each participant. In this way, we seek to enable the reader to evaluate if the findings can be applied in other contexts (Willig, 2013).
Discussion
This study will contribute to existing research concerning psychotherapy for depression and will provide important new knowledge about lack of progress in group therapy through a multiple case study approach that has rarely been applied within this field of study (McLeod, 2010). Furthermore, unexpected findings, yielded through the explorative design applied in the present study, allow for spin off-projects examining, for example, mechanisms of change.
Since the studies in the project build on each other, there is a risk that findings from study 1 will not give sufficient information to start study 2. Study 2 will therefore also be based on existing literature concerning lack of progress in psychotherapy and application of progress monitoring. Current findings of progress monitoring demonstrate that the implementation process is critical for a successful result (de Jong et al., 2012, 2021). Therapists and patients should therefore be included in the implementation processes. For this reason, we have already held user panels and therapists workshops. Among other things, the therapists expressed a worry about how they can make time to reflect on the patients’ progress monitoring in a strictly scheduled working day, where supervision is not offered weekly. A solution could be that in addition to supervision, the therapists arrange mutual meetings where they take time to present their cases and reflect on these together.
Using a qualitative approach within the progress monitoring context is not new within individual therapy, however, at the moment we find no qualitative studies of implementation of progress monitoring within group therapy. For this reason, one of the strengths of this study is that it will provide necessary new knowledge of how progress monitoring can be applied in group therapy.
Supplemental Material
sj-pdf-1-ijq-10.1177_16094069221084786 – Supplemental Material for Development of Individual Add-On Interventions for Patients With Depression Who are Persistently Not on Track in Group Cognitive Behavioural Therapy: A Protocol for a Treatment Development and Feasibility Study
Supplemental Material, sj-pdf-1-ijq-10.1177_16094069221084786 for Development of Individual Add-On Interventions for Patients With Depression Who are Persistently Not on Track in Group Cognitive Behavioural Therapy: A Protocol for a Treatment Development and Feasibility Study by Jasmin Rejaye Gryesten, Stig Poulsen and Sidse Marie Arnfred in International Journal of Qualitative Methods
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Trygfonden, grant number: 150579
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.