
Abstract
Chronic illnesses are a leading cause of global disease burden among older people worldwide. For many, death from serious chronic illness in older age is preceded by an extended period of fluctuations in health and well-being, and these end-of-life trajectories can be complex and difficult to predict. Most research on end-of-life trajectories is quantitative, based on structured measurements and focused on creating groups or categories of trajectories. At the same time, there is little research that attempts to gain a deeper understanding of how older people perceive, interpret, and explain the changes in and influences on their health and well-being as they near the end of life, and how these experiences differ. This longitudinal narrative study aims to understand the commonalities, differences, and changes over time in older people’s narratives of their health and well-being towards the end of life. Thirty-six older people (≥70 years old) who are diagnosed with one or several serious chronic illnesses and in deteriorating health will be invited to complete narrative interviews every two months over the course of twelve months. The interviews will be analysed following Riessman’s approach to narrative analysis, studying the content, structure, and performance aspects of the narratives. This study will establish a novel perspective on end-of-life trajectories, uncovering what is shared and what is individually specific in how older people perceive, interpret and explain their changing health and well-being. The study findings will form an important evidence base for strengthening person-centered care in a way that reflects older people’s priorities and experiences in the final stages of life.
Keywords
Background and Rationale
Traditional conceptualisations of end-of-life trajectories in the field of palliative care have assumed three distinct patterns of physical or functional decline based on cause of death, corresponding to a cancer, organ failure, and dementia/frailty trajectory (Murray et al., 2005). Since then, empirical work has added important nuance, showing that end-of-life trajectories are highly diverse, and that underlying pathology alone is a poor predictor of how a trajectory will evolve. Quantitative research using structured longitudinal assessments has found several distinct groups of end-of-life trajectories in the physical domain that were not clearly linked to an underlying disease (Gill et al., 2010). Qualitative research, usually involving interviews with people nearing the end of life, has also pointed to fluctuations in well-being being linked to changes in circumstances or personal capacity to adapt to evolving situations rather than physical pathology alone (Lloyd et al., 2016).
Chronic illnesses are a leading cause of global disease burden in older populations (Vos et al., 2020) and an important factor driving the increase in the number of deaths in old age worldwide (Mathers & Loncar, 2006). For many people, death from serious chronic illness is preceded by an extended period of fluctuations in health, ranging from weeks to years. The end-of-life trajectories of older people are frequently described as profoundly different from those in earlier phases of life, and as complex and difficult to predict (Goodman et al., 2015; Van Vliet et al., 2015). This is in part because multimorbidity, that is the simultaneous presence of several chronic illnesses, is highly prevalent among older people (Fortin et al., 2012) and because older age is an important risk factor for complicating circumstances, such as frailty, social isolation, and financial difficulties (Xue, 2011).
Crucial gaps remain in our understanding of older people’s end-of-life trajectories. First, existing research on end-of-life trajectories tends to focus primarily on the physical and functional aspects of decline (Cohen-Mansfield et al., 2017; Lunney et al., 2003). It pays very little attention to psychosocial and existential domains of well-being, despite the latter being essential to people’s experiences and of equal importance to physical changes in health (Murray et al., 2005). Second, both quantitative and qualitative research have primarily sought to create groups or categories of end-of-life trajectories, or to uncover common aspects of decline across groups. These ‘generalising’ approaches run the risk of masking important inter-individual variation and prompting inaccurate conclusions about individuals based on aggregated trajectory patterns or common themes drawn from people’s accounts of their health and illness (Lloyd et al., 2016; Murray et al., 2005; Szabó et al., 2021), thereby neglecting individual uniqueness and personal stories of meaning-making. Third, while both quantitative and qualitative research have contributed to the evidence base on end-of-life trajectories, most existing studies stem from quantitative research, where researchers map out trajectories based on structured measurements. While this research has provided important insights, it does not allow a deeper understanding of how older people perceive, interpret, and explain the fluctuations in their health (Calman et al., 2013).
When chronic illness disrupts life, the stories people tell about their health reveal their subjective experiences and associated meanings (Bury, 1982; Charmaz, 1999). Rooted in interpretivist/constructivist epistemology (Guba, 1981), narrative research uncovers how experiences are (re-)constructed and interpreted within an individual context without seeking an objectively ‘true’ rendition of reality (McKibben & Breheny, 2023). People’s illness narratives also offer a means of exploring their experiences of chronic illness by connecting past, present, and future beyond the restrictions of chronological time (Tripathi et al., 2024). While narrative research has explored chronic illness at the end of life (e.g. Florijn et al., 2019; Frank, 2013; Riessman, 2003; Roulston et al., 2018), most studies rely on single interviews or specific populations (based on healthcare settings or diagnoses), thus neglecting changes over time and the variety of experiences across different populations. This study contributes to the limited qualitative longitudinal research on end-of-life trajectories, gathering the illness narratives of older people as they evolve over time, uncovering inter-individual differences in how seemingly similar circumstances (e.g. the same diagnosis) can shape different experiences of health and well-being, and the meanings and processes people assign to these experiences.
Aims
This article describes the study protocol of a longitudinal narrative study aiming to understand the commonalities, differences, and changes over time in older people’s narratives of their health and well-being towards the end of life.
Methods
Study Design
We will conduct a longitudinal narrative interview study. Older people living with serious chronic illness (see eligibility criteria below) will be invited to complete narrative interviews covering their health and well-being at baseline and every two months, over 12 months or until death if they die before. There is no universally accepted definition of what period constitutes the end of life. In this study, the end of life is not restricted to the terminal phase, but extends beyond it to include the last year of life.
The study is part of a larger mixed-methods, inter-disciplinary project named TRAJECT that seeks to develop a novel framework for identifying commonalities and differences in the end-of-life trajectories of older people living with serious chronic illness (Tripathi et al., 2024). It consists of a quantitative longitudinal survey study (protocol submitted as separate publication), a longitudinal narrative interview study (described here) and a mixed-methods integration of both studies. This protocol follows the ObsQual checklist for reporting qualitative study designs (Low et al., 2024).
Sampling and Sample Size
Thirty-six older people will be invited to participate in the narrative interviews. This sample size considers an attrition of 15% for causes other than death, to achieve a final sample of 30 participants, which was shown to be large enough to obtain meaningful conclusions in previous narrative research (Bennett et al., 2020; Willig, 2015). The sample for the narrative study will be drawn from the larger sample of the quantitative longitudinal survey study of the TRAJECT project (N = 280) through purposive sampling (following recommendations by Palinkas et al., 2015). We will strive to obtain maximum variation in age (70–85 vs. >85), main diagnoses of chronic illnesses, and gender. The samples of the two studies are intended to partly overlap so that the mixed-methods findings can later be integrated at the individual and aggregated level. However, if a participant in our study drops out of the quantitative study, this will not impact their participation in the narrative study (if they still wish to be involved).
In longitudinal studies with people nearing the end of life, study termination due to death is by definition not considered a drop-out nor a threat to feasibility. However, we expect that some participants will drop out for reasons other than death (e.g. being too ill). All participants’ narratives, regardless of the length of their follow-up, will be retained for our analyses.
Population and Eligibility Criteria
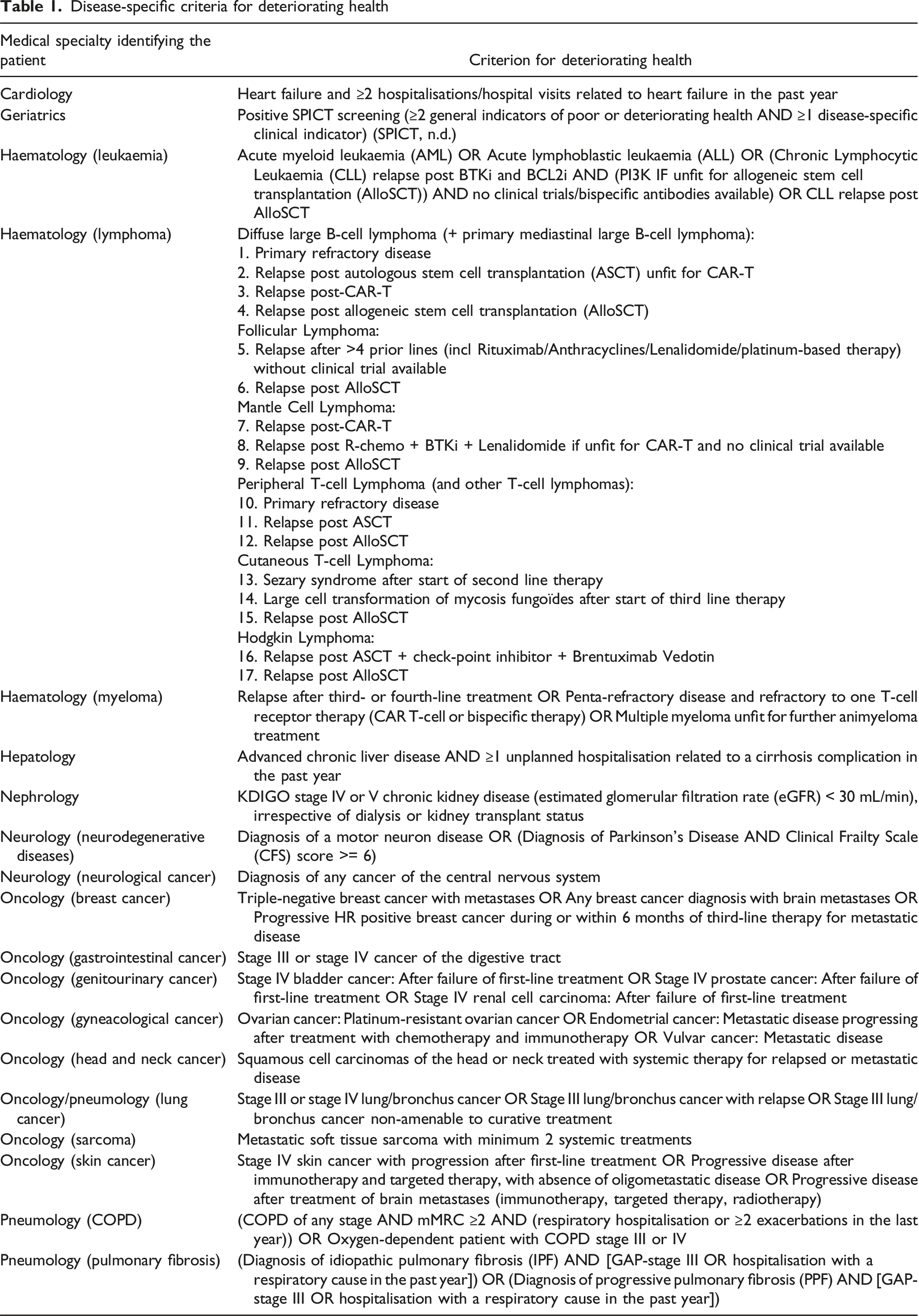
We will include participants aged 70 years or older who are diagnosed with a serious chronic illness, whose health is deteriorating, and who can participate in the study in either French or Dutch—the two most widely spoken languages in Belgium. We will exclude patients whose physician indicates that they are in the terminal phase of life (i.e. the last days of life) and patients who are unable to give informed consent to research participation according to their treating physician (e.g. due to cognitive decline).
Disease-specific criteria for deteriorating health
Method of Approach
Study participants will be identified at two university hospitals in Belgium (Universitair Ziekenhuis Brussel and Universitair Ziekenhuis Gent) at different clinical departments (i.e. geriatrics, medical oncology, pneumology, cardiology, gastro-enterology, nephrology, neurology, and haematology). In Belgium, hospitals are deemed appropriate settings to identify the population for this study because care for older people with a deteriorating serious chronic illness typically runs through the hospital at some point in the last year of life, either because they are hospitalised or because follow-up of their condition is done during outpatient visits (e.g. as in a cancer or chronic kidney disease trajectory) (DGGS - Gezondheidszorg: Dienst data- en beleidsinformatie, 2023).
Potentially eligible participants will be identified and approached by their treating physician with brief information about the study. The physician will ask for their permission to be contacted by the research team. Those who agree will then be contacted and visited by a researcher at a location of their choice. The researcher will provide the full study information and obtain written informed consent, contact details for a contact person (i.e. close family member or friend), if available, and conduct the first narrative interview. We will record reasons for refusal if the approached person is willing to provide one.
Participant Timeline
Narrative interviews will be conducted at baseline (upon inclusion), and follow-up interviews will be done every two months, over 12 months or until death if the participant dies before. For those participants who also take part in the TRAJECT project’s longitudinal survey study, the narrative interviews will be scheduled within two weeks of the quantitative data collection, to avoid the data collection becoming too burdensome for participants.
Collection of Narratives
The narrative interviews will preferably be conducted face-to-face (to facilitate direct interaction and observations of non-verbal cues by the interviewer) at a location chosen by the participant, typically their home. They can also be held online if preferred by the participant. Each interview will be audio-recorded and transcribed verbatim with the help of a transcription software. We expect that interviews will last approximately one hour, although participants can take the lead in continuing or ending an interview. Participants may also choose to have a family member, friend, or another close person present during the interview. All interviews will be conducted in French or Dutch by a researcher who is a native speaker, depending on the participant’s preference.
The interview guide for the first interview (forward-translated to English for readers’ information, see Supplemental Materials) begins with a broad, open-ended question inspired by an introductory question suggested by Anderson and Kirkpatrick (2016): “Could you tell me about when you first got sick, and what has happened since?” This question encourages participants to narrate the story of their chronic illness, allowing them to highlight what they feel is important and how they experienced the evolution of their illness. The phrase “when you first got sick” provides a starting point for the narrative, while leaving room for the participant’s interpretation of when their illness began. “What has happened since” prompts them to continue their story from that point to the present. The response to this question will form the main narrative of the interview, during which the researcher will minimally interrupt, offering only non-verbal encouragement. We anticipate that the initial interviews will reflect the exploratory nature of this study through broad and in-depth conversations about participants’ varied experiences with aging and chronic illness, as well as the meanings they attribute to these experiences.
In follow-up interviews, similar open-ended first questions will be used to encourage storytelling (e.g. “Could you tell me about what has happened since our last conversation, about two months ago?”). These interviews will be treated as opportunities to uncover changes in narratives occurring over time and gain a deeper understanding of the stories previously told. We will extensively prepare follow-up interviews by studying the transcripts of previous interviews and reflexive notes made by the interviewing researcher. These extensive reflexive notes made by the researcher before, during, and after each interview will describe the interview context in terms of atmospheres, impressions, underlying emotions or non-verbal cues which traditionally are not recorded in transcripts (Lear et al., 2018).
Aside from the above-mentioned first questions, the interview guide contains a list of open-ended questions that serve as suggestions meant to inspire the researcher and remind them of potentially relevant topics. Narrative interviews are inherently unstructured (Hsu & McCormack, 2010), which means the researcher is encouraged to let the conversation unfold according to the participant’s narrative. The researcher relinquishes control over the conversation and allows the participant to lead, even into unexpected topics (Riessman, 2008). With a trusting relationship established over the course of the interviews, participants should feel comfortable sharing their thoughts freely (Charmaz, 2009).
Narrative Analysis
To analyse participants’ narratives, we will follow Catherine Riessman’s suggestion to study both the content of the narratives as well as the act of narration (Riessman, 2008). While the content consists of tangible and observable elements that can be analysed for their nature and sequence, the act of narration is equally significant, as it highlights the context and settings in which the narrative is produced, performed, and subsequently interpreted. We will use thematic, structural, and performance analysis to examine what was said, how it was said, and why it was said in that way, respectively (Riessman, 2008). Subsequently, we will integrate the insights obtained through these three analysis methods. We will examine these aspects of the narrative while preserving the continuity of the story within its original context. Systematic integration of the three kinds of analysis methods will make the process an in-depth interpretative one to reveal the different layers of meanings embedded in the narratives, ultimately improving the quality of our findings (Meraz et al., 2019). We outline the three kinds of analysis that we will apply below.
Content: Thematic Analysis
This first step in narrative analysis will focus on the content of the narratives told by participants, following the six steps of reflexive thematic analysis as outlined by Braun et al. (2022). We will start by reading interview transcripts as wholes to gain familiarity with the stories told. We will then code the interview transcripts based on what is said by the participant, assigning codes to fragments of narratives that seem relevant to the research question. We will maintain larger narrative sequences (ranging in length from two sentences to whole paragraphs) as is commonly done in narrative analysis, rather than fraction the narratives into smaller word groups (Bergien et al., 2023). As codes are developed based on the narratives, we will form overarching themes within individual participants’ narratives and across them. We will revise, adapt, and enhance these overarching themes using a variety of techniques (e.g. reading the entire dataset again or attempting to tell a re-constructed story through the themes and evaluating this re-constructed story’s nearness to the initial narratives), before defining and naming the finalised themes. When presenting our findings, we will use narrative sequences to illustrate themes.
Content: Structural Analysis
In analysing structure, we will explore the added value of identifying discursive structures in narratives using a simplified version of socio-linguist William Labov’s methods of analysis (Labov, 1977). We will pay particular attention to Labov’s notion of evaluation (1977). Evaluative clauses, which can be spread throughout a narrative, indicate the participant’s answer to an unspoken question: “Why does the participant think this particular story is worth telling?” Paying attention to structural features of discourse such as evaluative clauses can help researchers identify subjective temporality in a narrative, highlight what drives action in the story (i.e. motivations), and illuminate the role of external influences in the end-of-life trajectory (Meraz et al., 2019). A narrator might for instance signal what they consider crucial about their story by placing it at the end of their narrative sequence and awaiting reaction from the listener. By analysing a narrative in this manner, we hope to identify the purpose it serves for the narrator. For example, a narrator could present relationships between events as causal to bring a sense of order to an illness trajectory often experienced as jumbled (Williams, 1984).
Narration: Performance Analysis
The co-construction of narrative happens within a shared space between the researcher and participant, and entails a performance of identities (Riessman, 2008) which means dynamics of trust, power, and control that shape the narrative must be taken into account (McKibben & Breheny, 2023). The ‘self’ in a narrative is (re-)constructed and performed with or for the audience (Riessman, 2003). In this study, the performance analysis of narratives will unveil how the participants “do illness in vastly different ways” (Riessman, 2003, p. 20). The performance within an interview space is inherently symbiotic, with the researcher’s presence shaping the dynamics. The interviewing researcher will take extensive field notes before, during, and right after interviews, documenting such dynamics and processes (McKibben & Breheny, 2023; Muylaert et al., 2014). When analysing performance in a narrative, the researchers will be guided by the question: “Why does the participant tell this story in this particular way and to me?” Further questions leading the reflexive process regarding performance include “What are our mutual assumptions about each other as narrator and listener?” “What identities are at stake in the telling of the story?” and “How does [the story] tend to larger discourses at play?” (Sahlstein Parcell & Baker, 2017). These questions will be answered through a constant reflexive exercise by the researcher in collaboration with other researchers, based on the field notes taken to understand the interpersonal factors at play, through multiple readings of the transcripts, and to recognise any blind spots in relation to the researcher-participant dynamics.
Longitudinal Narrative Analysis
We will examine the longitudinal series of narratives for each participant, searching for underlying narrative threads, changes in narrative occurring over time, and the role of external influences in shaping those changes. Subsequently, we will identify commonalities and differences across the different participants’ narratives by placing series of individuals’ evolving narratives in juxtaposition to each other. Figure 1 is a schematic representation of how the whole process of analysis will be organised. We will refine our analytical approach by drawing on established qualitative longitudinal analysis methods, ensuring a structured and rigorous process. We will document and report our methodological choices and adaptations transparently in later stages of the research. Schematic representation of the longitudinal narrative analysis in three steps
Ethics
This project was approved by the Commission for Medical Ethics of the Universitair Ziekenhuis Brussel (Brussels University Hospital, 1432024000122, approval obtained on the 3rd of July, 2024) and the Commission for Medical Ethics of the Universitair Ziekenhuis Gent (Ghent University Hospital, B6702024000297, approval obtained on the 2nd of September, 2024).
Data Management and Monitoring
The processing of personal data is subject to free and fully informed consent and will be conducted in accordance with applicable international, EU and national law (in particular, the GDPR, national data protection laws and other relevant legislation). The researchers have drafted a Data Management Plan (DMP) according to European Research Council guidelines and a Data Protection Impact Assessment (DPIA) regarding the collecting, processing, and archiving of personal data.
Pilot Study
A pilot study has been conducted with six older people who were invited to participate in narrative interviews twice; once at baseline and once after two months. Two participants died before the second interview could be conducted. The pilot study aimed to test the feasibility and acceptability of the study methods, and helped the researchers finalise the interview guide and anticipate challenges in the data collection strategies.
Rigor
The criteria for scientific quality relevant to this study’s methods are aligned with its interpretivist/constructivist approach. We will follow generally accepted guidelines that research should be ethical, important, using fitting and rigorous methods, and reported coherently and thoroughly (Cohen & Crabtree, 2008). We will strive to meet the criteria of confirmability, dependability, and credibility through several key strategies (Frankel, 1999). Specifically, we will consider researcher subjectivity as a resource rather than a problematic bias (Cohen & Crabtree, 2008), therefore encouraging researcher reflexivity using researcher triangulation and extensive reflexive notes. Disagreements on interpretations among researchers will be treated as opportunities for self-reflection and worked through until mutual understanding is reached. These processes will be documented in meeting reports. We will also provide rich qualitative data to support interpretive claims, reflecting our participants’ experiences. Finally, we will report our study results according to existing guidelines for qualitative research (Critical Appraisal Skills Programme, 2016; Tong et al., 2007).
Discussion
Strengths and Contributions
By collecting the narratives of health and well-being of older people living with serious chronic illness towards the end of life, we will gain insight into their subjective experiences and how they evolve over time. We will be able to compare experiences across end-of-life trajectories based on underlying pathologies, while also considering various other individual and contextual characteristics potentially shaping people’s experiences. By doing so, we will uncover the dynamics of experiences in end-of-life trajectories—where they differ, where they converge into shared experiences, and how they are shaped.
Narrative approaches offer a powerful way to enhance our current knowledge of end-of-life trajectories by revealing how individuals make sense of the world and their place within it. They provide valuable insights into how people give meaning to chronic illness and aging (Nicholson et al., 2013). Where quantitative research often represents individual uniqueness along a continuum of scores on measurement scales (e.g. to assess well-being), our narrative approach will allow for a deeper understanding of how older people living with serious chronic illness perceive and interpret fluctuations in their health as their illness progresses and the end of life nears (Bury, 1982; Charmaz, 1999).
Conducting narrative interviews at multiple points in the end-of-life trajectory is particularly valuable for capturing the evolving nature of experience and highlighting health and well-being as individually unique processes (McKibben & Breheny, 2023; Murtagh, 2015). Repeated narrative interviews also foster trust between researcher and participant, creating a safe and familiar space where participants can comfortably open up over time (Read, 2018). Furthermore, retelling a story across different points in time can reveal shifting perspectives, new insights, and variations in emphasis, bringing forward aspects of the illness experience that might otherwise go unspoken in a single interview (Charmaz, 2009).
Narrative research also creates space for participants to be recognised as reliable narrators and expert witnesses on their own lives (Rahman et al., 2024). This approach will offer deeply personal insights into what people consider significant in their end-of-life trajectories, an essential element in understanding the impact of chronic illness on identity and well-being towards the end of life. Thus, by giving older people living with serious chronic illness a space in which to freely express their experiences, this study can contribute to the development of more holistic and person-centered approaches in their end-of-life care.
Potential Challenges
The nature of longitudinal narrative interviews can present ethical challenges. While many older people benefit from participating in qualitative research on their experiences (Fudge et al., 2007; Leahy et al., 2005), discussing personal subjects such as the nature and progression of illness may elicit psychological discomfort. To minimise distress, we will maintain flexibility in data collection (Scantlebury & Adamson, 2022), adapting to participants’ needs and circumstances. A distress protocol (see Supplemental Materials) outlines steps to be undertaken if researchers notice psychological distress. Experienced researchers on the team and an international advisory board will provide supervision and support concerning potentially distressing situations for both participants and researchers.
Some participants may struggle to share their experiences, not necessarily due to distress but because they feel their experiences are irrelevant. This is an issue we noted in the pilot study. The interviewing researcher will thoroughly prepare follow-up interviews, identifying potential avenues for deeper engagement. Conversely, participants may share narratives that seem unrelated to their end-of-life trajectory. Rather than redirecting too quickly, the researcher will allow space for these accounts, as their relevance may emerge later. However, when needed, the interview guide includes strategies for gently refocusing the conversation.
Beyond ethical considerations, this study will generate a substantial amount of longitudinal narrative data in two languages, making analysis particularly complex. To ensure that we meet the aims of the study, we will adhere to established methods of data analysis (Vandenbogaerde et al., 2024; Wanat et al., 2025) and involve researchers fluent in the interview languages. Reflexive field notes and meeting reports will enhance transparency on data analysis processes in future publications.
Prognostic uncertainty in chronic illness means that some participants will outlive the 12-month follow-up, while others may die before its completion. Those who die before will have provided valuable insights into their experiences in the last phase of life, while those who live longer will have shared experiences of declining health. Some participants who are in very poor health for a long period of time before death may be unable to participate in interviews despite their death occurring after the intended follow-up. As all these periods that are covered by our study are, broadly speaking, part of end-of-life trajectories, they remain relevant to the study aim and to our analysis.
Finally, participating in this study and speaking about one’s health and well-being might in itself impact how participants experience their end-of-life trajectories. We will critically reflect on this possibility in our analyses and reports, noting instances where participants express how they experienced study participation.
Conclusion
By studying the evolving narratives of older people living with serious chronic illness towards the end of life, this study will provide critical insights into their shared as well as individually specific experiences, and the context in which their end-of-life trajectories unfold. The study findings will deepen our understanding of how older people make sense of and give meaning to health and well-being, providing an important evidence base for strengthening person-centred care in a way that reflects older people’s priorities and experiences in the final stages of life.
The contributions of this study have the potential to lay the groundwork for a new research paradigm—understanding end-of-life trajectories and the circumstances that shape them through a study of people’s narratives. Embedded in the broader TRAJECT project, which recognises the equal epistemological value of qualitative and quantitative research paradigms, this study also exemplifies a deeply integrated mixed-methods approach aimed at understanding the complex and nuanced nature of end-of-life trajectories (Tripathi et al., 2024).
Supplemental Material
Supplemental Material - Older People Living With Serious Chronic Illness Towards the End of Life: Study Protocol for the Longitudinal Narrative Study of the TRAJECT Project
Supplemental Material for Older People Living With Serious Chronic Illness Towards the End of Life: Study Protocol for the Longitudinal Narrative Study of the TRAJECT Project by Emma Gobiet, Khyati Tripathi, Aline De Vleminck, Lieve Van den Block, Lore Decoster, Eline Naert, Nele Van Den Noortgate and Lara Pivodic in International Journal of Qualitative Methods
Supplemental Material
Supplemental Material - Older People Living With Serious Chronic Illness Towards the End of Life: Study Protocol for the Longitudinal Narrative Study of the TRAJECT Project
Supplemental Material for Older People Living With Serious Chronic Illness Towards the End of Life: Study Protocol for the Longitudinal Narrative Study of the TRAJECT Project by Emma Gobiet, Khyati Tripathi, Aline De Vleminck, Lieve Van den Block, Lore Decoster, Eline Naert, Nele Van Den Noortgate and Lara Pivodic in International Journal of Qualitative Methods
Footnotes
Acknowledgments
We would like to thank the participants of the pilot study for their interest in the project and for sharing their experiences with their ongoing chronic illness. We also acknowledge and thank all the clinicians for their cooperation in developing the disease-specific inclusion criteria, in setting up recruitment procedures, and for facilitating the identification of potential participants. Additionally, we are grateful to the TRAJECT advisory board members - Annemarie Samuels, Caroline Nicholson, and Sigrid Sterckx - for their continued support, input, and feedback throughout this project.
Ethical Considerations
This project was approved by the Commission for Medical Ethics of the Universitair Ziekenhuis Brussel (Brussels University Hospital, 1432024000122, approval obtained on the 3rd of July, 2024) and the Commission for Medical Ethics of the Universitair Ziekenhuis Gent (Ghent University Hospital, B6702024000297, approval obtained on the 2nd of September, 2024).
Consent to participate
Not applicable to this paper which describes a study protocol.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The TRAJECT project is funded by the European Research Council (ERC, Project No. 101077555). Views and opinions expressed are however those of the authors only and do not necessarily reflect those of the European Union or the European Research Council Executive Agency. Neither the European Union nor the granting authority can be held responsible for them. Aline De Vleminck is the recipient of a senior postdoctoral mandate from FWO, Grant No. 12ZY222N.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.