
Abstract

Background
According to the World Health Organization (WHO), stroke is a rapidly progressive local or pervasive neurological disorder originating in cerebral vessels that lasts for more than 24 hours or leads to death (Sacco et al., 2013). Clinically, stroke is an acute focal neurological defect attributed to vascular damage (infarction, bleeding) of the central nervous system. It is the second leading cause of death and the third leading cause of disability worldwide. Most strokes (85%) are ischemic, mainly caused by small atherosclerosis and embolism of large arteries. These are especially important in young patients (under 50) (Bani Ardalan et al., 2022; Murphy & Werring, 2020). The incidence and mortality of stroke varies between countries, geographical regions and ethnicities (Katan & Luft, 2018). In all European Union (EU) countries, stroke is the main cause of adult disability, affecting 1.1 million residents of Europe annually and causing 440,000 deaths a year. The number of people living with strokes is estimated to increase to 27% in the EU between 2017 and 2047 (Wafa et al., 2020). In the United States (US), stroke is also at the forefront of major neurological disorders in terms of the number of absolute years lost due to disease (Feigin et al., 2021). In Asia, which accounts for more than 60% of the world’s population and most of its countries are “developing”, the disease is a serious problem (Venketasubramanian et al., 2017). The overall burden of stroke in Iran is also increasing among the middle-aged population (50 to 69 years-old) (Fallahzadeh et al., 2022).
Many survivors of stroke attacks are dealing with at least one surviving complication of the disease upon discharge from treatment centers. These patients and their families experience a heavy burden of physical and psychological symptoms that are frequently left unaddressed (Jafari-Golestan, 2024; Schutz & Creutzfeldt, 2023). Additionally, stroke survivors face social and cultural challenges that arise from their dependence on others because of mobility issues, reduced sensory perception, and decreased activity levels. These challenges significantly impact their daily lives, especially routine activities like bathing, getting dressed, and using the restroom (Alhalabi & Bani Hani, 2023; Cowey et al., 2021; Ndiok et al., 2020).
Families and caregivers of stroke survivors face many challenges. In the acute phase of the illness, they witness the rapid and unexpected decline of a loved one. They are also responsible for making decisions on behalf of the patient, especially in situations requiring immediate choices (Schutz & Creutzfeldt, 2023). Stroke survivors and their families often feel unprepared to transition into the post-stroke phase. They constantly seek help to manage symptoms, adapt to new strategies, and navigate medical decisions (Kendall et al., 2018).
The uncertain prognosis of stroke and its prolonged recovery period complicate the requirements of patients and their families. This may lead to a range of difficulties for survivors and their families regarding psychological, social, spiritual, financial, and physical needs that are frequently neglected in practice. At this stage, adopting a palliative approach can be helpful. Palliative care (PC) has been implemented and recognized as suitable for all patients with severe illnesses, including stroke (Schutz & Creutzfeldt, 2023).
In 2016, the American Stroke Association released a statement on PC and stroke. Since that time, texts on PC have become more prevalent in relation to stroke (Cowey et al., 2021). The PC model was offered by WHO. WHO characterizes PC as a means to enhance the Quality of Life (QoL) for patients facing incurable and life-threatening illnesses, along with their families, focusing on the period from diagnosis to post-mortem (Hökkä et al., 2021). According to the WHO, while 40 million individuals require PC each year due to life-limiting conditions, merely 14% of these individuals have access to and benefit from PC (Namasivayam et al., 2022).
According to the conventional model of PC, this type of care is solely associated with the final days of life and is conducted for patients suffering from cancer, while the updated perspective of PC is the science and art of enhancing the quality of life for every patient, which does not respond to routine healthcare. This care ought to be offered not just in the final phases of life, but also from the onset of diagnosis to assist in managing the symptoms of the illness throughout the extended years of living with a chronic condition (Scheerens et al., 2020; Yang-Huang et al., 2022).
Currently, there is no cohesive approach to PC in the treatment of stroke survivors that allows for an appropriate time to initiate PC (Steigleder et al., 2019). The literature review suggests that although PC is an essential element of treatment in stroke units, the phrase “palliative care” is often misunderstood by stroke professionals, survivors, and their families as equivalent to end-of-life care or the termination of treatment. As a result, there are few referrals of stroke patients to specialized palliative care services, typically happening only at the time of death. For example, research conducted by Amber et al. indicated that a considerable number of stroke patients did not receive PC, even among those who passed away in the hospital. These results underscore the missed chances for PC to ease suffering following a severe stroke. The distinctive progression of the illness after an acute stroke demands a more profound understanding of how PC can be effectively employed for this patient group (Comer et al., 2022).
Literature indicates that many healthcare providers are unaware of the importance of addressing the social, emotional, and spiritual needs of patients. This represents a significant clinical deficit. A treatment team responsible for caring for survivors after a stroke should be able to recognize patients and families who could benefit from receiving PC interventions and develop the necessary plans (Govind et al., 2023). Given the lack of a standardized framework for PC in the treatment of stroke survivors, especially regarding the optimal timing for initiating such care, and the tendency to limit its use to end-of-life stages, there is a need for research that explores the concept, characteristics, antecedents, and consequences of PC for stroke survivors. Additionally, creating a tool tailored to the specific aspects of PC for this population, while taking into account the cultural context, is vital. Proper and timely implementation of PC can improve the QoL for patients and their families, decrease hospital readmission rates, and subsequently lower healthcare expenses. Consequently, this study is designed with the purpose of tackling these important issues.
Objectives
The overall goal of this proposed study is to explore the concept, characteristics, antecedents, and consequences of PC and develop a tool for stroke survivors. The specific objectives are as follows: (a) exploring the concept of PC in stroke survivors; (b) designing a specific PC questionnaire for stroke survivors; (c) determining the constituent items, dimensions, and subscales of the specific PC questionnaire for stroke survivors; (d) determining the face validity; the content validity, and the construct validity of the specific PC questionnaire for stroke survivors; (e) determining the internal consistency , and the stability (reliability) of the specific PC questionnaire for stroke survivors.
Methodology and Method
This research is sequential mixed-method exploratory analysis. It will focus on the concept of PC, its characteristics, antecedents, and consequences for stroke survivors, in addition to the creation and psychometric evaluation of a specific PC questionnaire for these individuals. It includes two phases: qualitative phase (exploring the concept of PC in acute stroke survivors using the hybrid concept analysis technique), and quantitative phase (creation of items for a special PC questionnaire for acute stroke survivors and evaluation of its validity and reliability).
The study will investigate and elucidate the concept of palliative care in patients who have survived acute strokes via a qualitative method (hybrid concept analysis). Subsequently, throughout the quantitative phase of the research, the outcomes from the qualitative stage will be used to develop and confirm the instrument. In the quantitative phase, the psychometric research approach will be utilized to finalize and validate the questionnaire. Following the initial qualitative data, the quantitative phase will then be conducted. To address the inquiry of the first phase of this research, which is qualitative, the researcher will adopt a constructivist approach to develop themes. To address the inquiry of the second phase, which is quantitative, they will transition from a constructivist to a positivist perspective to analyze the themes generated using a quantitative approach. There are several theories regarding the construction of instruments, such as Item Response Theory (IRT) and Classical Test Theory (CTT). Numerous measurement tools currently employed in health research are founded on the principles and techniques of classical test theory (CTT) (DeVellis, 2006). Given that CTT has been utilized to create many of the instruments in nursing research, this theory will also be implemented in the quantitative phase of this study to develop the instrument. Classical Test Theory states that the steps involved in creating an instrument are: (1) Defining the concept using analysis and ultimately determining its indicators. (2) Designing the instrument according to the Likert rating scale or meaning differentiation (3) Reviewing the questions by experts and specialists in terms of accuracy, suitability for the test specifications, identifying technical flaws in question construction, writing, and readability (4) Testing preliminary questions on a limited number of research units that represent the research community (5) Conduct a field test and implement all questions in their final outline form in a large sample representative of the target population of the research. (6) Conduct question analysis with the aim of identifying questions with a high internal consistency scale. (7) Select and retain questions with higher coefficients. (8) Conduct studies on the validity of the instrument. (9) Assess the reliability of the instrument. (10) Collect instrument norms. (11) Publish the results of the instrument preparation (Grove et al., 2014).
Recruitment and Participant Selection
This study will be divided into two primary phases: qualitative and quantitative. The phases of the research are outlined in detail below.
Phase 1: Qualitative Analysis
The initial phase of this research, grounded in Classical Test Theory, is the qualitative phase, which will be conducted through concept analysis utilizing a hybrid approach. A hybrid method for concept analysis has been advocated by Schwartz-Barcott and Kim. The hybrid model relies on developing concepts through a qualitative analysis of phenomena in their actual locations. Concept development through a hybrid model integrates both inductive and deductive approaches, allowing for a form of synthesis; thus, it can enhance concepts that have diverse applications. This framework includes three stages: (a) theoretical (deductive approaches); (b) fieldwork and investigation (inductive approaches), and (c) analytical (Schwart-Barcott & Kim, 2000). (a) Theoretical stage: during this stage a literature review on the topic of PC for stroke survivors will be conducted using international database including Google Scholar, ScienceDirect, Ovid, PubMed, ProQuest, Scopus, Web of Science, and Persian national database and the country’s medical research information portal including SID, Magiran, IronDoc. The steps involved in conducting the literature review for this research are: (1) Defining the research question: in this step research questions related to the concept of PC will be defined. (2) Identifying relevant studies, 3. Selecting articles: At these steps, databases search will be start. The search will be conducted using Medical Subject Headings (MESH) or keywords in databases following the guidelines specific to each database with no limits on time or language. The keywords based on MESH are as follows: “Cerebrovascular Accident, Cerebral Stroke, Cerebrovascular Apoplexy, Brain Vascular Accident, Cerebrovascular Stroke, Apoplexy, CVA (Cerebrovascular Accident), Acute Stroke, Acute Cerebrovascular Accident, Palliative Care, Supportive Care, Palliative Supportive Care, Palliative Treatment, Palliative Therapy, Palliative Surgery”. (4) Collecting data and producing charts based on the collected information, and 5. Organizing and presenting the results (Arksey and O'Malley, 2005): At these steps, articles focusing on definitions and conceptual importance, characteristics, predictors, and outcomes will be selected, and the similarities and differences between them will be examined. Data analysis will occur in the theoretical stage through text content analysis. (b) Fieldwork stage: The second stage of the hybrid concept analysis, which will take place alongside the first stage, is the fieldwork stage, aimed at exploring the concept of PC in individuals recovering from acute strokes. In this regard, the most effective method for exploring, understanding, and discovering the realities of the phenomenon under investigation is to apply the qualitative research methodology. The sampling approach during this phase is purposeful and includes nurses from the intensive care unit, neurology and stroke departments, as well as neurologists, critical care professionals, family members of stroke survivors, and stroke survivors who are able to communicate. The inclusion criteria will comprise: having a minimum of one year of professional experience and at least six months of relevant unit experience for nurses, and the ability to communicate verbally or in writing for stroke survivors. If necessary, based on the interview process, other individuals may also be included in the qualitative phase of the research. The exclusion criteria for the study are as follows: stroke survivors who were able to communicate verbally and in writing at the beginning of the research but are no longer able to communicate due to disease progression will be excluded. Interviews will be conducted in the setting and at the time preferred by participants. During this stage, the interviews will initiate as unstructured and then shift to a semi-structured format that includes some broad, entirely open-ended questions. Interviews will start with general questions and then progress according to the interviewees' answers by probing questions.
The Examples of questions that will be asked in the interview include: (1) Questions related to the medical staff (doctors and nurses) will be: - What is your experience with palliative care, especially in stroke survivors? - When you hear the term palliative care, what thoughts come to mind? - Have you previously cared for stroke survivors in need of palliative care? If so, how was the experience and what treatments were provided? - How is palliative care provided at the hospital where you are employed? Who is responsible for determining the need for palliative care and when it should be initiated? - Based on your experiences, what are the factors that influence and the barriers that hinder the
Implementation of palliative care in your hospital? (2) Questions related to the patients and their family members will be: - How long has it been since you or your loved one had a stroke? - What were your initial feelings and challenges when you received the stroke diagnosis? - How were you or your loved one cared for following the stroke diagnosis? - Were you directed to a specific facility or department for palliative care? If so, which facility or department was it and what services were provided there?
Audio will be recorded, and transcribed verbatim.
The sampling will continue until data saturation. The length of each interview will vary depending on the individual interviewed. Data analysis during this stage will employ qualitative content analysis.
The steps of qualitative content analysis include: specifying the research problem, formulating questions and objectives, defining and specifying variables, sampling and selecting units of analysis, coding and categorization, analyzing and inferring results, and reporting (MomeniRad, 2014).
© Conceptual Analysis or Synthesis Stage
A combined approach will be used for the final stage of concept analysis, in which a comprehensive assessment of how well the first two stages were integrated will be carried out. A comprehensive definition that includes all of the characteristics mentioned in the previous stages will be produced at this stage by combining the definitions and concepts gathered from the first two stages. Qualitative data will be analyzed inductively. The software MAXQDA version 21 will facilitate data management and content analysis; quantitative data will be analyzed by using SPSS version 21.
Phase 2: Quantitative Analysis
Based on the results of the qualitative phase, a decision will be made on which aspect of the palliative care concept to implement. In other words, the design and development of the questionnaire will be based on concept explained in the qualitative phase. This questionnaire will be developed through various stages of development and psychometric evaluation of a questionnaire, which will involve producing items, determining face validity, content validity, construct validity, and reliability. These stages will be explained in detail in the following sections:
Producing the Items of the Questionnaire
The categories, subcategories, and item pool related to the concept under investigation in this study will be extracted based on the findings of the first phase of the study, which includes the qualitative phase (consisting of three steps: theoretical, fieldwork, and analytical). After extracting the items, the response rate for each item or question will be determined. Questions or phrases will be written in a logical order and similar items will be placed in a group.
Face Validity
Face validity will be conducted using both quantitative and qualitative methods. To conduct qualitative face validity, interviews will be held with several individuals from the target group. These participants will be asked to read the items and explain their understanding of the items to the researcher, a process known as “think aloud.” They are also questioned about the difficulty level, consistency, and ambiguity of the items, as well as whether any items should be removed or kept in the instrument. The items will be revised based on the feedback from this group. This iterative process will continue until the items are easily understood by the individuals and no further changes are recommended (Almanasreh et al., 2019; Taghizadeh et al., 2017).
Quantitative face validity will be measured by calculating the item impact score. To measure it, a number of expert panel and participants will be asked to evaluate the items in terms of their importance and give each item a score from 1 to 5, depending on the level of importance. A score of 1 indicates the lowest and a score of 5 indicates the highest level of importance. The impact score for each item will be calculated as the product of the importance of an item and its number of repetitions. An impact score greater than 1.5 will be considered appropriate (Allen et al., 2023; Taghizadeh et al., 2017; Taherdoost, 2016).
Content Validity
Content validity will be conducted using both quantitative and qualitative methods. To determine content validity in a qualitative manner, a group of professionals in the field of stroke survivor care and treatment, including neurologists, nurses, and critical care specialists, will be asked to provide their written opinions as part of the qualitative content validity study. It will be emphasized that grammar, wording, item allocation, scaling, and completion time should all be considered when evaluating the qualitative content validity. Once expert opinions are collected, necessary modifications to the instrument will be made.
To quantitatively determine content validity, the Content Validity Ratio will be used to ensure that the most crucial and accurate content (question necessity) has been selected. Subsequently, the content validity index will be used to ensure that the instrument’s questions are effectively constructed to measure the content. In order to evaluate the questionnaire’s content validity, a group of medical and nursing specialists will be contacted to rate each question as “necessary,” “useful but not necessary,” or “not necessary.” The answers will be calculated using the CVR formula and compared to the Lawshe table (30). The CVI will be assessed using the Waltz and Basel content validity index (31), following the determination and calculation of the CVR. The questionnaire will be given to the same experts again to calculate the CVI. They will be asked to rate each question on a four-point Likert scale based on relevance, simplicity, and clarity (e.g., 0: irrelevant, 1: somewhat relevant, 2: relevant, 3: completely relevant). A CVI score above 0.79 will indicate acceptance of the items (29) (32). The Content Validity Ratio will then be used to quantitatively assess the validity of the content and ensure that the most crucial and accurate content (question necessity) has been selected. Subsequently, the content validity index will be used to ensure that the instrument’s questions are effectively constructed to measure the content. In order to evaluate the questionnaire’s content validity, a group of medical and nursing specialists will be contacted to rate each question as “necessary,” “useful but not necessary,” or “not necessary.” The answers will be calculated using the CVR formula and compared to the Lawshe table (Lawshe, 1975). The CVI will be assessed using the Waltz and Basel content validity index, following the determination and calculation of the CVR. The questionnaire will be given to the same experts again to calculate the CVI. They will be asked to rate each question on a four-point Likert scale based on relevance, simplicity, and clarity (e.g., 0: irrelevant, 1: somewhat relevant, 2: relevant, 3: completely relevant). A CVI score above 0.79 will indicate acceptance of the items (Taherdoost, 2016).
Construct Validity
Construct validity is a measure of how well the outcomes of using measures align with the theories that the test is based on. It also shows how well the measurement captures the idea according to relevant theories. Instead of being restricted to a single indicator or set of observable traits, a construct comprises a collection of related variables. Important steps in researching construct validity include developing hypotheses regarding the concepts being studied, testing these hypotheses, and determining how well the results correlate with the original measurement. High construct validity is indicated by a high correlation coefficient, and vice versa. Therefore, the degree to which the prepared questionnaire’s items are grouped around a theoretical construct and are either correlated (internal consistency) or different should be ascertained. If the items on the test have a relationship with one another, then the test is construct valid. Otherwise, there is no construct validity in the questionnaire (Taherdoost, 2016). Different methods for determining construct validity include: hypothesis testing, convergent validity, divergent validity, known groups, discriminant validity, factor analysis (Arabkhani et al., 2023).
In this study, exploratory factor analysis (EFA) using the Principal Component Analysis (PCA) method will be employed, because little information is available about the construct under study. In fact, Factor analysis summarizes and classifies a large number of variables or items by analyzing their internal correlations and grouping them into a small number of factors. The goal is to identify basic patterns of relationships between the variables. In the PCA method, the researcher aims to determine the number of factors that can account for the highest variance in the data related to the topic being measured. This process helps reduce the number of variables and identifies key elements that form a factor and ultimately a construct. As a result, it aids in the organized grouping of elements and the development of factors to evaluate a topic. This method is particularly suitable for variables assessed using a Likert scale. To conduct factor analysis, the sampling adequacy test (KMO) will be initially calculated to ensure the sample size is sufficient. Then, Bartlett’s sphericity test will be used to confirm that there is a non-zero correlation among the variables, as this correlation forms the basis of factor analysis. The number of factors will be determined based on eigenvalues and the scree plot diagram. Components with absolute loading values of 0.4 or higher will be considered, while those below this threshold will be eliminated (Floyd & Widaman, 1995). EFA will be performed using SPSS version 21 software.
Reliability With Internal Consistency and Consistency Methods
A questionnaire’s reliability indicates how well the measurement tool yields consistent results under the same circumstances. One of the qualities of a measurement tool, such as a questionnaire, interview, or other social science test, is reliability. The reliability coefficient typically ranges from 0 (no correlation) to +1 (complete correlation). The reliability coefficient shows how well the measuring device captures the subject’s variable and transient traits, as well as their stable traits. It should be mentioned that a test’s reliability can differ depending on the circumstance and the group. Methods such as re-administration (test-retest method), parallel method (peer), classification method (split in half), Koder-Richardson method, and Cronbach’s alpha method are used to determine a measuring instrument’s reliability coefficient (Ahmed and Ishtiaq, 2021).
Reliability Assessment
We will assess reliability once before conducting factor analysis and once after. Depending on the scale of the instrument we design, we will use either the internal consistency method (Cronbach’s alpha) or the test-retest method.
Assessing Internal Consistency (With Cronbach’s Alpha)
Cronbach’s alpha is one of the most widely used techniques for assessing internal consistency. Internal consistency addresses the question of whether the items in an instrument are conceptually compatible with each other. The alpha coefficient is the most popular statistical technique for proving internal consistency, as it is the only sample-dependent reliability indicator that only needs to be administered once. For example, an alpha value of 0.9 or higher is considered excellent, 0.7 to 0.9 is good, 0.5 to 0.7 is fair, and less than 0.5 is unacceptable (47).
Assessing the Questionnaire’s Stability Through the Test-Retest Method
The designed questionnaire will be distributed to multiple participants at 2-week intervals as part of the retest method. The intraclass correlation index will then be used to compare the scores earned over the course of these two weeks. The intraclass correlation should be at least 0.4 (Ahmed & Ishtiaq, 2021).
Project Chronogram

Sample Size
In the quantitative phase, which focuses on measuring validity and reliability, the size and number of samples will be determined after the qualitative phase and in consideration of the items in the designed instrument. However, as a general guideline, the recommended sample sizes for different stages of the quantitative phase are as follows: Face validity: 10 to 15 individuals, Content validity: 10 to 15 individuals, Construct validity: 5 to 10 individuals per item included in the questionnaire, Calculation of Cronbach’s alpha for Construct validity: at least 20 individuals, Reliability assessment using the internal consistency method (Cronbach’s alpha): the same sample size used for Construct validity.
Data Analysis
Data Analysis in Each Stage of the Study
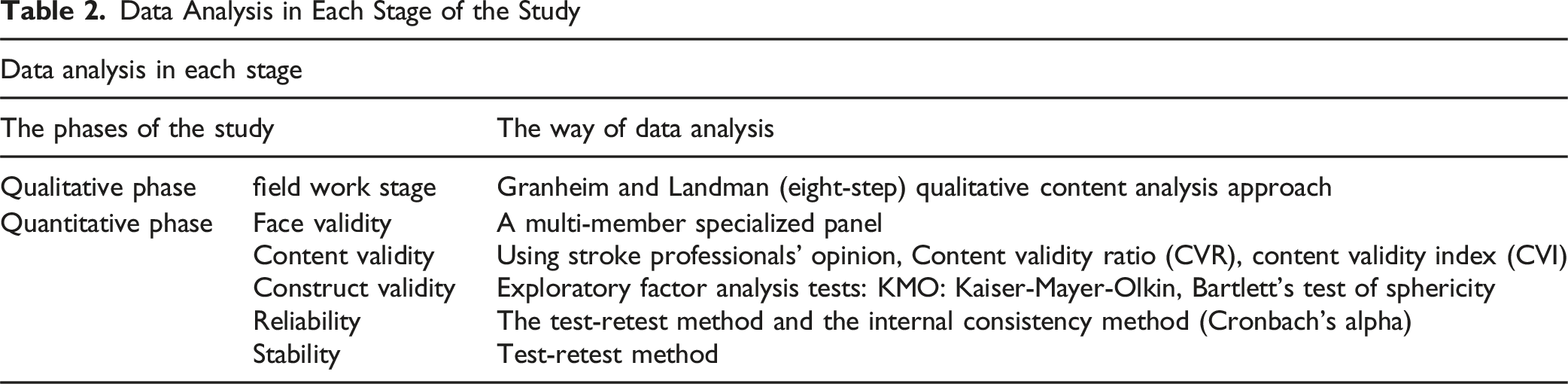
At the Field Work Stage of the First Phase
Qualitative Content Analysis Steps

Ethics
The researchers will adhere to ethical principles throughout all phases of the research. All researchers and collaborators commit to adhering rigorously to the Declaration of Helsinki. All interviews will be gathered anonymously, and after creating the tool for collecting quantitative data, anonymous surveys will be formulated and given to the participants. The research participants will also be informed that taking part in this study is entirely voluntary and that they are free to exit the research setting at any point during the study if they choose not to continue responding to the questions. Ethics Approval for the study has been obtained from the Research Ethics Committees of the School of Nursing and Midwifery & Rehabilitation - Tehran University of Medical Sciences (IR.TUMS.FNM.REC.1403.100). Informed written consent will be obtained from all participants.
Discussion
This study aims to explain the concept of palliative care in stroke survivors. The literature review indicates that while palliative care is a crucial component of treatment in stroke units, the term “palliative care” is frequently misinterpreted by stroke professionals, survivors, and their families as synonymous with end-of-life care or the cessation of treatment. Consequently, there are limited referrals of stroke patients to specialized palliative care services, typically occurring only at the time of death (Comer et al., 2022). Literature shows that many healthcare providers lack awareness of the importance of addressing the social, emotional, and spiritual needs of patients, which signifies a substantial clinical gap.
Therefore, the current study aims to offer a more thorough understanding of palliative care after stroke by utilizing a mixed-methods approach that integrates qualitative and quantitative research techniques.
Transferability, Applicability and Opportunity of the Proposal
The findings of this study may be generalizable to all stroke patients and their families, and may also provide valuable insights for nurses—particularly those working in emergency departments, neurology wards, and intensive care units (ICUs) throughout Iran.
At the Healthcare Level
The findings may assist in comprehending the accurate concept of palliative care in stroke patients and result in the integration of palliative care nurses and physicians as part of the treatment team for this patient group.
At the Educational Level
The findings may result in the design of educational packages and related educational software for patients and their families to support the care of stroke patients. Additionally, the results may lead to the establishment of essential minimum training requirements in the area of palliative care following a stroke for treatment teams.
On a Policy Level
Our findings probably suggest that we need to give significant focus to the matter of palliative care in stroke patients and should not restrict this form of care to just terminally ill and end-of-life patients.
Alongside scientific publications and conferences, we intend to share the findings with various professional, patient, and public organizations, as well as through press statements, the media, and policy documents. Ultimately, the methods and outcomes could provide a foundation for upcoming studies, as they illustrate the preliminary circumstances.
Footnotes
Ethical Approval
Ethics Approval for the study has been obtained from the Research Ethics Committees of the School of Nursing and Midwifery & Rehabilitation - Tehran University of Medical Sciences (IR.TUMS.FNM.REC.1403.100).
Informed Consent
Informed written consent will be obtained from all participants.
Author Contributions
Zakiyeh Jafaryparvar: made a significant contribution to the concept, design, acquisition, analysis or interpretation of data. Writing – Original Draft. Approved the final version of the article for publication. Fatemeh Bahramnezhad: made a contribution to the concept and design of the study. Review & editing the article critically for important intellectual content. Approved the final version of the article for publication. Fatemeh Hajibabaee: made a contribution to the concept and design of the study. Review & editing the article critically for important intellectual content. Approved the final version of the article for publication. Mahdi Shafiee Sabet: made a contribution to the concept and design of the study. Review & editing the article critically for important intellectual content. Approved the final version of the article for publication. Nahid Dehghan Nayeri: made a significant contribution to the concept, design, acquisition, analysis or interpretation of data. Writing – Review & Editing the article critically for important intellectual content. Approved the final version of the article for publication.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data from this study are available by contacting the corresponding author, subject to a reasonable request.