
Abstract
Community-based participatory research (CBPR) offers effective, flexible approaches well suited to conduct health research with underrepresented populations that can be tailored to unique social, cultural, and geographic contexts. For these reasons, CBPR offers the potential to address rural underrepresentation in dementia research. However, the diversity of rural America requires multi-scalar approaches to research that account for regional characteristics in the analysis of health data and the design of health system interventions. To address this issue, Memory Keepers Medical Discovery Team (MK-MDT) has developed a regional CBPR model for dementia research that incorporates multiple rural communities across northern Minnesota, which builds unique regional knowledge allowing for regional comparisons. Facilitated by numerous partnerships with community organizations, healthcare providers, and academics, the MK-MDT regional CBPR model offers a framework that is actionable and effective, especially for recruiting participants across rural regions for a range of projects. In this paper, we describe the components and approach to our regional CBPR model as well as three case studies of how this approach has been effectively applied across a variety of projects focused on dementia. Although applied to the upper Midwest, the MK-MDT regional CBPR model is applicable to other rural regions where networks of rural communities work together to address Alzheimer’s disease and Alzheimer’s disease related dementias (AD/ADRD) and care needs. This approach demonstrates the power in leveraging multiple communities in CBPR research that better reflects the inter-related ways in which rural people and places interact with each other to provide AD/ADRD care.
Keywords
Background and Objectives
The prevalence of Alzheimer’s dementia among adults aged 65 and older in the United States is expected to rise from 6.5 million to 12.7 million people by 2050 (Alzheimer’s Association, 2024). Reports also demonstrate that the burden of dementia is often higher in underrepresented and minority populations (Shiekh et al., 2021). Rural populations are no exception. Living in a rural community can exacerbate the risk of Alzheimer’s disease and related dementias (AD/ADRD) as rural residents face higher rates of multiple chronic conditions that act as risk factors (e.g., hypertension, diabetes, physical inactivity), are less likely to receive an accurate and timely diagnosis (Herd et al., 2021), and face significant barriers accessing AD/ADRD services, leading to suboptimal care (Bayly et al., 2020; Siconolfi et al., 2019). Despite this awareness, rural populations are underrepresented in health research in general, and clinical research in particular (Indorewalla et al., 2021; Tanner et al., 2015). More specifically, there is a dearth of research concerning aging and dementia in rural populations. The National Institute on Aging’s (NIA) Health Disparities Framework recognizes the need for greater inclusion of rural populations in AD/ADRD-specific research (Hill et al., 2015; National Institute on Aging, 2023; Wiese, Gibson, et al., 2023).
It is generally recognized that rural and remote communities have a greater burden of ill health across many diseases and, by nature, poorer access to healthcare. Based on age structure and general health status, it would be expected that most rural populations would demonstrate higher rates of dementia compared to urban counterparts (Glasgow & Brown, 2012; Jensen et al., 2020), however, recent research has demonstrated a high degree of heterogeneity in rates of AD/ADRD at the county level across and within rural regions (Dhana et al., 2023; Ho & Franco, 2022). In 2020, Minnesota had 101,900 people aged 65 and older living with Alzheimer’s disease, roughly 10.7% of the older adult population and an anticipated 221.4% increase in the Alzheimer’s disease care workforce to meet projected demand in 2050 (Alzheimer’s Association, 2024). Furthermore, rural communities in Minnesota are on average older than their urban counterparts, leading the state’s Department of Health to project a two-fold increase of rural residents aged 85 and older in the next 35 years (Minnesota Department of Health, 2021). An exploratory epidemiological study concluded that rural Minnesota had a 17.6% lower age-adjusted rate of dementia mortality than urban areas, but visits to emergency departments from people with dementia were 12.4% higher than the urban counterparts, suggesting that older people with dementia in rural areas underuse primary health care clinics and inpatient hospital services, overuse emergency department visits, and are likely underdiagnosed (Rhew et al., 2023). This finding shows that rural Minnesotans with dementia engaged with health systems differently than their urban counterparts, relying on unplanned emergency services over planned hospital stays with long-term service options.
Rural populations are hard-to-reach geographically and can be more socially and culturally disconnected from research institutes and universities (Thurman & Harrison, 2020). Additional barriers to participation may also include low health and research literacy, distrust of research entities, and a lack of best practices for rural recruitment and retention (Gilmore-Bykovskyi et al., 2019; Kim et al., 2014). These factors are among a myriad of reasons rural populations are usually ignored in clinical trials research, including trials commonly conducted through Alzheimer’s Disease and Related Dementias Research Centers (ADRCs) (Indorewalla et al., 2021). At the time of writing, only 2 of 33 ADRCs have an explicit rural focus that details specific outreach, engagement strategies, and mission statements stressing the importance of including rural populations as a collective underrepresented population.
Indorewalla and colleagues (2021) call for the advancement of precision research engagement for recruitment of underrepresented populations into AD/ADRD research that is theoretically grounded, testable, modifiable and replicable. It is noteworthy that many of the components and approaches they suggest to improve participation are normally incorporated into community-based participatory research (CBPR) models; for example, developing rapport through in-person interactions, raising awareness, using community spaces, engaging trusted community members/organizations to gain trust and disseminate information, using existing community networks for ongoing recruitment, and employing community outreach coordinators who share characteristics and lived experience with the recruitment population. The authors assert that purposeful action is needed to improve recruitment efforts, or else researchers are at risk of exacerbating health inequities (Indorewalla et al., 2021).
Community-based participatory research has been employed for decades to address the health needs of marginalized people and communities. Grounded in theories developed by Kurt Lewin (Lewin, 1946) and Paulo Freire in 1968 (Freire, 2018), participatory methods, when used appropriately, promote empowerment and social equity through the disruption of power imbalances, including when knowledge is being used as a means of social control (Reyes et al., 2023). More recently, interest in and use of the approach to improve participation in AD/ADRD research has risen, prompting a scoping review on the topic (Reyes et al., 2023). However, the notion of adopting CBPR to address disparities in AD/ADRD recruitment is not new. In 2014, Grill and Galvin suggested several strategies to enhance participation in AD/ADRD trials—for example, outreach, registries, and satellite clinics—but they noted that CBPR specifically can create innovative and sustained approaches to the benefit of older adults. CBPR has also been a method used for decades by qualitative researchers to conduct AD/ADRD research with disparity populations (Blind et al., 2023; Brush et al., 2020; Wiese, Lingler, et al., 2023) and in the development of rural and remote clinical interventions (Hicks et al., 2020; Morgan et al., 2014, 2019; Salisbury et al., 2023). As reviewed by Reyes et al. (2023), the key benefits of a CBPR approach to AD/ADRD research includes increased participation (Grill & Galvin, 2014), a focus on health equity as an outcome (Gilmore-Bykovskyi et al., 2019), improved study design and applicability of findings, and opportunities to center the voices of those living with dementia (Reuben et al., 2020).
The CBPR literature is vast. Many researchers using CBPR or its many allied or derivative approaches such as Participatory Action Research, Community-Academic Partnerships, or Patient-Oriented Research, share an interest in breaking down barriers between university-based researchers and the wider community and in conducting research that leads to positive and transformative change in the community (Geary et al., 2021; Ortiz et al., 2020). The literature varies on what are included as the basic principles of CBPR; however, the following principles show the most consistency over time: building on community strengths, recognizing and embedding local knowledge, equitably partnering throughout the life of the project, growing relationships that are reciprocal, building local capacity for research, contributing to empowerment and self-determination, and co-creating knowledge for action and social change with the goal of improving community health and eliminating disparities (Israel et al., 2017; Unertl et al., 2016). Reyes and colleagues (2023) echo Indorewalla et al.’s (2021) comments (i.e., theoretical mechanisms that are testable, modifiable, and transferable) in noting that if we hope to apply CBPR approaches to AD/ADRD recruitment and research with underrepresented populations, there is a need for greater transparency in study design, including description of how the participatory principles were enacted, who is participating (excluding study subjects), why the participatory approach was appropriate, and overall, more thorough descriptions of study design. For our purposes, we view CBPR as “an applied collaborative approach that enables community residents to more actively participate in the full spectrum of research with the goal of influencing change in community health, systems, programs, or policies (Jacklin et al., 2023).
Given the gaps in the literature and the many identified barriers to conducting rural CBPR, and AD/ADRD focused research, this paper will describe our application of CBPR in a rural regional context to facilitate the study of AD/ADRD in northern Minnesota. We also offer three case study examples to further describe our approach when dealing with different project needs and designs, as well as the effectiveness of the approach in these different settings.
Research Design and Methods
Building CBPR Partnerships to Address AD/ADRD in Rural Minnesota
Memory Keepers Medical Discovery Team (MK-MDT) was established in 2016 at the University of Minnesota (UMN) Medical School in collaboration with a State Legislature initiative designed to improve health outcomes for Minnesotans. This commitment provides core funding to the MK-MDT which has supported community outreach, advisory groups, and researchers that act as infrastructure to obtain pilot data to support additional grant funding for specific research projects. MK-MDT focuses on brain health equity in rural and Indigenous populations in Minnesota and beyond. Research with Indigenous populations was initiated in 2017, and in 2020, investigators (KJ, WW) began to develop a plan to address rural AD/ADRD disparities more broadly by developing a program of research called Community Engaged Rural Dementia and Alzheimer’s Research (CERDAR). Drawing on decades of experience with CBPR in Indigenous populations, CERDAR was designed to mirror principles and approaches that have proven successful in engaging with Indigenous populations, including a firm grounding in and commitment to health equity.
Membership and Characteristics of the Rural, Regional CBPR Team
MK-MDT’s approach bridges the divide between academic researchers and communities by developing meaningful relationships with communities that involve them throughout the research process, in project design, data collection, analysis, and the dissemination of results back to community members, setting the stage for the long-term, sustainable collaborations needed to support dementia research in rural communities. Central to our CBPR framework is an advisory structure that supports a regional Community Advisory Group (CAG), a Rural Research Advisory Group (RRAG), and a Rural Advisor in Residence. The Rural Advisor in Residence is a family physician who has worked with older adult patients in northern rural Minnesota for over 30 years, and who provides context and interpretive abilities to data collection and analysis. These individuals and groups are frequently consulted throughout the research process to identify emerging trends grounded in their lived experiences. (Figure 1). CERDAR CBPR Process.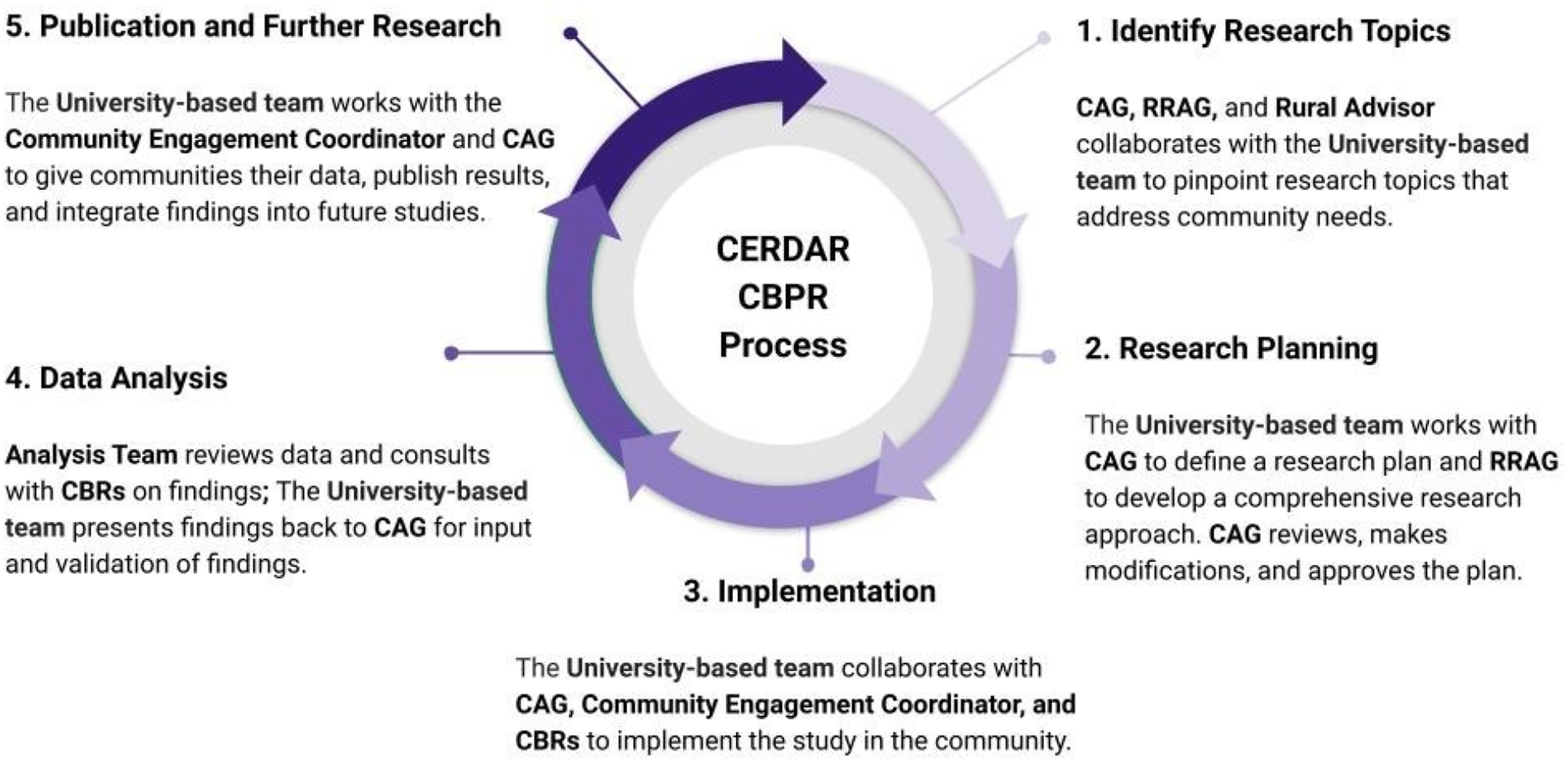
The CAG currently has 10 members from northern rural Minnesota and operates on the principle of consensus decision making, where the group works together iteratively to arrive at a decision agreed upon by all (Pérez et al., 2018). Advisory group members are selected according to knowledge, expertise, experience with dementia and interest in rural health, the health of older adults, and dementia care and services. CAG members have a range of backgrounds, including service planners, older adult program developers, a retired nurse, a psychologist, health coordinators, an older adult outreach advocate, a retired adult day care provider, and a person living with dementia. The CAG is involved with developing the vision for our program of research, responding to questions about community expectations around research, recruiting participants, analyzing research findings, and participating in dissemination efforts. They provide input for research strategies and questions as well as oversight of specific project objectives and timelines. The CAG meets with the university staff and investigators at least quarterly through a mixture of virtual and hybrid gatherings facilitated by a university-based community-engagement coordinator. During times of data analysis, more frequent meetings are needed. In between meetings, members are provided with monthly email communications including updates on research progress and activities, requests for information from the university research team, and notice of significant issues or developments. The CAG’s composition ensures diverse perspectives in dementia care are represented, and including a person living with dementia helps ensure their voices directly inform the research process through active participation in quarterly meetings.
The community engagement coordinator and community-based researchers also frequently visit the members in their respective communities, and all reside in rural communities outside of Duluth, Minnesota. The community-based researchers have backgrounds in health or social work, including one dietician and one social worker with experience working with Areas Agencies of Aging and home and community-based services.
A smaller, six-member RRAG is comprised of national and international academic advisors with diverse experience in rural health and aging policy and practice, along with the leads of two key Area Agencies on Aging that demarcate the health service areas for older adults in northern Minnesota. The purpose of the RRAG is to advise the investigators on key issues, research priorities, and regional, state, national, and international rural health priorities related to rural dementia research. The RRAG meets virtually, in person, or hybrid twice a year. This structure is supported by email updates and contact directly by the investigators when needed.
Many of the members of the CAG and the RRAG have direct experience with informal or formal caregiving, life-experience with family members or friends who have lived with dementia or are themselves living with dementia. The main difference between the advisory committees is that the RRAG advises on national and state level priorities while the CAG refines research projects and approaches to ensure relevance to their community, gathers community input regarding research questions and directions, and provides feedback to study plans and analysis of results. Information and advice from both groups set the overall strategic aims for our program of research. For example, the RRAG discussed the potential for our program of research to expand across the entire state, but after exploring this with the CAG, the final consensus reached by both groups was that due to current capacity at MK-MDT the focus should remain on northern Minnesota where the needs are the greatest. Northern Minnesota has a higher incidence of AD/ADRD, an older population with increased “remoteness” (i.e., frontier areas lacking broadband connectivity), and a history of being excluded from university research.
Our research is designed as a program-project approach with specialized units supporting the CBPR process, data management and analysis, and administrative oversight (Figure 2). Our pilot projects involve a range of mixed methods studies, including the use of ethnographic methods to explore rural perceptions and experiences with dementia and caregiving, a remote exercise intervention for people with subjective cognitive decline that can take place in the home (Salisbury et al., 2023), and an epidemiological study comparing rural and urban dementia and health services data (Rhew et al., 2023). The long-term goal of CERDAR is to increase dementia care access, improve diagnosis, and provide culturally appropriate dementia education for AD/ADRD by revealing the unique facilitators and barriers that exist in rural communities. Project Structure.
A key element of our approach is involving community-based researchers (CBRs) employed by UMN who live in rural Minnesota. The CBRs help engage, recruit, and retain participants in research, and they assist in conducting qualitative research while living and working remotely from their home communities/regions. They are connected to one another regularly and serve as a liaison between researchers, community members, partners, and organizations. They provide critical support throughout the research process by tailoring methodological approaches to be more effective in the community setting, collecting data, recruiting, and providing deep contextual information for analysis. They are supported by institutionally based staff including senior research associates who help with project coordination, implementation, data analysis, and dissemination, and a community engagement coordinator. Currently, due to the level of funding available, our regional model allows for one community researcher in the northwestern portion of the state and another in the northeast region of the state, providing spatial coverage for northern Minnesota. To date, our approach to hiring CBRs has been to identify individuals who live in rural areas and, if possible, have experience with dementia and rural health care. We offer both onsite and remote training in CBPR approaches, as well as in qualitative and quantitative research methods and practices. Our long-term strategy is to secure additional funding through external grants to increase the number of community researchers to provide greater regional geographic focus and reduce travel demands for these positions.
While our inclusion of rural community researchers in our CBPR model is not novel, the extent to which our CBRs are involved in the research process is unique. We hire the CBRs as full-time employees of the UMN under the MK-MDT staff umbrella, and they are involved in all staff MK-MDT activities. Their understanding of local rural context and how that is incorporated is a strength of our approach. These individuals have a dual role comprised of research (recruitment, interviewing, member checking, data analysis, and dissemination) and community engagement activities which include participation in local health events. The CBRs are trusted and known to our community partners and offer existing relationships with non-profit organizations and social service agencies. Importantly, they provide a familiar face on a sensitive topic (both AD/ADRD and research) and help the MK-MDT demonstrate, at this incipient stage in its development, our commitment to building research capacity in rural areas.
Regional CBPR
Our CBPR approach is best characterized as regional. Research is tailored to cover the unique contexts of different communities while simultaneously being able to aggregate these findings for regional insights to better understand AD/ADRD care and experiences and inform future interventions. Northern Minnesota is a broad and vast geographic region characterized by low population densities and dispersed rural communities across different subregions, such as the Red River Valley, the Iron Range, and Greater Arrowhead, that are shaped by topography, social organization, and local economies. Commodity demands, job schedules, and health organizational practices all potentially affect the times rural residents are available to participate in research. Each of these features also influence how rural people live and interact. Understanding how to navigate local and regional difference is important for recruitment and community engagement efforts. For example, rural communities organized around agriculture in the western part of the state may be less available during planting and harvest seasons, whereas towns organized around recreation and tourism in the north-central part of the state may be busier during the summer months.
To ensure geographic representation of the communities in northern Minnesota, CERDAR geo-referenced data from our projects. Our use of rural mapping allows us to develop sustainable practices for ongoing research by ensuring representation from all rural communities (Figure 3). As we discover underrepresented areas for our research, CERDAR utilizes the CAGs, community researchers, and collaborating organizations to target outreach and recruitment efforts in those areas. This unique approach is well suited to rural regions, where iterative processes for participation recruitment and research—such as rural mapping and advisory board collaboration—ensure geographic representation of regional and community strengths, weaknesses, and needs relating to AD/ADRD care. The following three case studies describe separate but interrelated projects conducted by MK-MDT investigators and illustrate the application and effectiveness of our CBPR approach. Project Participants as of May 2024.
Results
Case Study #1: CBPR to Develop a Research Registry: The CERDAR Community
The aim of this project is to develop a rural AD/ADRD research registry for people living in northern Minnesota to bring together researchers and adults in rural communities to improve our understanding of the risk, resilience, and experience of memory problems or caring for people with dementia that are specific to rural life. The CERDAR Community, found on our website (ruralmemory.com), disseminates research opportunities and quarterly CERDAR newsletters that highlight recent activities and accomplishments, with options to opt out at any time. The CERDAR Community is used to identify potential participants and contact them about specific research projects that are applicable to their experience and position. Beyond information dissemination, the goal of this project is to create a pool of rural residents interested in participating in research related to AD/ADRD now and in the future. Our community engagement and research team actively seek rural adults to engage with the CERDAR Community through in-person recruitment efforts and the dissemination of recruitment materials at regional fairs, health conferences, community forums, and community events. Flyers to join the CERDAR Community have been delivered across libraries, bulletin boards, and with our collaborating partners in the Area Agencies on Aging and Senior LinkAge Line, as well as being regularly posted on social media and shared by these same partners.
Several adjustments have been made to the CERDAR Community since its inception to improve engagement. Initially called a research “registry,” the name was modified, based on feedback from our community advisory group, to the “CERDAR Community” to avoid any negative connotations with registries that may exist for rural people (e.g., national gun registry, sex offender registry, government-controlled registry). CERDAR Community members can control their degree of participation and indicate if they want to receive updates electronically or have physical copies mailed to their address. The initial enrollment of community members encompassed 39 members. Over the period of 41 months between November 2021 and April 2025, there has been an average of 2.31 individuals added to the CERDAR Community per month. There are 97 individuals currently part of the CERDAR Community. Our efforts to grow the community continue and we anticipate will accelerate with future grant support.
Case Study #2: CBPR Recruitment Strategies: Sociocultural Factors in Rural AD/ADRD Care Experiences
The aim of this study was to analyze rural dementia illness experiences from the perspectives of formal and informal caregivers, those with subjective cognitive impairment, mild cognitive impairment or diagnosed with early – mid stage dementia, and key informants. We also included a subset of older adults without impairment to better understand pre-clinical perceptions and service use. Key informants included healthcare professionals, health leaders, and social workers. Research design included ethnographic qualitative methods to understand the lived experience of dementia and the facilitators and barriers to AD/ADRD care and quality of life. Participants are asked to join the CERDAR Community for research updates and opportunities to participate in upcoming research projects.
The MK-MDT utilized several CBPR approaches to recruit participants for this project. First, the CERDAR Community was used to identify potential participants who indicated an interest in participating in research related to AD/ADRD. Second, recruitment flyers were distributed across northern rural Minnesota at various libraries, clinics, and community bulletin boards with assistance from community advisory group members and home and community-based organizations that are part of the aging network of service providers in the region. The third and most successful method was personal outreach by the CBR using their respective formal and informal community-based social networks. The CBRs identified key contacts in each county (24 counties in the region) to visit, call and email, asking them to share information with professionals, older adults and family caregivers, and make referrals. Fourth, MK-MDT’s rural advisor identified rural physicians for recruitment, which was critical due to the inaugural rural advisor’s role in the UMN Medical School and the Rural Physician Associate Program responsible for placing newly graduated physicians in rural communities. Part of this outreach included sending messages to professional email addresses and making contact with mailed letters. Finally, participant locations were mapped to identify communities without representation in our dataset, and less represented geographies were intentionally recruited from using the steps identified above.
CERDAR faculty and on-site staff worked with the CBRs to analyze transcript data, and with the CAG for collaborative consensus building for community reports, publications, and presentations. The CBRs and CAG members offer a rural perspective that helps to inform the analytic process from inception to completion. The CBRs provide feedback derived from individual interviews, field notes and insights from their respective regional communities to help with the coding process and theme development. Advisory group members help with the triangulation of data by informing whether or not findings are reflective of their community and if there is additional information missing from the data. Data are discussed with the CAG through ongoing presentations virtually and in-person where findings are confirmed, challenged, and additional feedback is collected to contextualized findings across communities. Each CAG meeting includes university staff asking several questions to address confusing statements and contradicting information found in the data. To date, there have been 94 interviews conducted and member-checked for data analysis, while ongoing recruitment is still occurring to improve geographic representation.
Case Study #3: CBPR in a Rural Intervention Study: Feasibility of Community Based Exercise Rehabilitation in Rural Minnesota in Persons with Subjective Memory Complaints (MN RIDE)
The aim of this study, a single-group pre-post design, was to pilot test the feasibility of a remotely delivered exercise intervention into rural communities using a CBPR approach. As part of this project, participants had a stationary exercise bike delivered to their home for a 12-week exercise program and had their fitness and memory assessed at two different times. Sessions were supervised remotely via smart devices and Zoom. The aerobic exercise program was classified as moderate intensity stationary cycling with intensity increasing over time. Moderate intensity was defined as achieving an exercise heart rate of 64%–76% of age predicted maximum heart rate. The feasibility and safety were assessed by tracking session attendance, intensity adherence, presence of adverse events, and participant satisfaction.
The long-term objective of this project is to develop a rural dementia prevention program to reduce cardiovascular risk factors associated with the development of dementia-related illness. The CBRs played a crucial role throughout this pilot study. They leveraged existing professional and social networks to disseminate information about the program, recruit participants, determine eligibility, and enroll rural participants. CBRs conducted phone screenings and performed pre- and post-intervention fitness assessments at the participants’ homes to eliminate barriers to participation. Additionally, the researchers managed the necessary equipment, addressed questions and concerns, followed up on referrals, and conducted baseline and follow-up assessments. They also were able to assist participants in assembling the bikes when needed. Each participant was required to obtain physician clearance prior to enrolling in the study, ensuring that exercise participation was safe for them. Nine participants were recruited and were retained throughout the duration of the pilot study. Findings demonstrate the feasibility of a hybrid community-based and remotely delivered exercise intervention program (Salisbury et al., 2023) and associations with improvements in cognition and fitness (Salisbury et al., 2023). This pilot data will be used to move the MN RIDE program into a stage 1 intervention.
Discussion and Implications
We have presented a regional CBPR model for the study of AD/ADRD in rural populations and provided examples of its implementation. Defining the organizational capacity required to make this model successful is a characteristic that has seldom been described in the literature (Salimi et al., 2012). Central to this model are strong partnerships among the university, communities, and community organizations operating across northern Minnesota throughout the research process. Our CBPR approach shares common elements with the few others who have conducted CBPR research on AD/ADRD. Thoughtful integration of community-based researchers (Horowitz et al., 2009) and a community advisory group (Ta Park et al., 2023) allows for the equitable inclusion of rural perspectives and experiences with AD/ADRD care from trusted individuals. Further, implementing a research registry (Grill & Galvin, 2014) and partnering with local organizations, regional agencies (e.g., the Area Agencies of Aging), and caregiver support groups has facilitated recruitment for this underrepresented population in a range of research projects (Grill & Galvin, 2014; Indorewalla et al., 2021; Reyes et al., 2023). However, a regional CBPR approach has not previously been described in US AD/ADRD research. In fact, only the Rural Dementia Action Research (RaDAR) program of research in Canada has applied a regional structure in this context, albeit with a very different on-the-ground approach to community engagement (Morgan et al., 2014, 2019). How our model differs is in the addition of having a robust structure to support the approach including the community-engagement coordinators and CBRs on the team and working with an Advisory committee that extends beyond service-based membership to include community champions. Significantly, in our model the research happens on the ground in the communities who are interacting with other members of their community to do research. Researchers may consider a regional approach to CBPR when communities are unbounded and span large geographic distances, which is very often the case in rural research. This approach recognizes the diversity of rural communities that is important to capture in research and ultimately intervention design.
Achieving equitable and sustainable community-research relationships requires years of trust building and community outreach (Brush et al., 2020; Van Gelderen et al., 2018). This difficult process is further complicated by university expectations and policies as well as grant constraints on resources, reporting processes, and the long-term sustainability of CBPR-initiated projects (Brush et al., 2020; Chandanabhumma et al., 2023). Grant requirements for measurable outcomes and their time-limited resources often pressure investigators to practice rapid research. This compromises the ideal of the CBPR process which recognizes the sometimes unpredictable, iterative, dialectical, and reflexive vagaries of collaboration between community participants and the research team (Amauchi et al., 2022). Time, money, university policies, and IRB boards unfamiliar with CBPR processes are reported to be the largest barriers to CBPR (Brush et al., 2020; Cross et al., 2015; Hoeft et al., 2014; Stoecker, 2008).
Given their prior experience, the founding investigators of the MK-MDT (KJ, WW) recognized and confronted these challenges. With University investments, they ensured our model was supported by building university and community-based infrastructure to position community engagement as a central tenet of our research. With this investment, we have been able to rapidly establish and maintain a community advisory group, hire and train community-based researchers, and build relationships and trust with rural organizations and community members in northern Minnesota. With an additional investment from the UMN Medical School Academic Investment Research Plan, we have been able to define our collaborative research scope with a network of new faculty collaborators and community partners. Additionally, we have gathered pilot data to inform future grant applications to grow our community-based research infrastructure and improve the quality of life for rural Minnesotans impacted by AD/ADRD. The University’s role must not be underestimated. To operate effectively, the CAGs and CBRs require University staff and investigators to provide administrative support and methodological and subject matter expertise.
Together, the CAGs and CBRs are the strongest force in our approach to ensuring the inclusion of rural voice, and is a well-documented way to ensure the presence of patient, family, and community perspectives in health research (Salimi et al., 2012; Sharma et al., 2017). Membership composition has been described as a crucial step to consider in the formation of CAGs, and the composition of our CAGs was no different (Newman et al., 2011). It is crucial that multiple community voices are included, and members have some connection with the illness. Research experience was not an essential characteristic of the CAG members. Including persons living with dementia and people who are or have cared for someone with dementia grounded our approach to the research and analysis in the lived experience. These individuals have had to navigate rural health infrastructures, and their insights provide practical knowledge that informs the direction of our inquiry and interpretation of the results. Likewise, including members from local health organizations provides linkages to already established knowledge translation networks and helps establish legitimacy and trust at the local level.
Important caveats to the model are that sustainability will require on-going external grants and any research that is more expansive than our pilot studies will require additional CBRs across rural Minnesota. In the current model there is one CAG for all of northern Minnesota (at the request of the members), however, as the program of research grows and is more regionally focused, the establishment of additional CAGs will be necessary. Yet, our model holds strong potential for replicability in other rural locations and can significantly support the recruitment of rural people into AD/ADRD clinical trials, which is a recognized need. The ability to effectively recruit rural residents into a range of dementia-related research—from exploratory interviews to intervention feasibility studies—demonstrates an actionable framework to implement a rural regional CBPR structure for rural dementia studies and address on-going challenges of underrepresentation. Implementing a rural-regional specific CBPR model can help increase the clinical representation of rural residents by allowing participants to work with trusted individuals in their community. Doing so allows research participants to engage more easily since researchers are able to attend to the unique needs and circumstances of rural people and places and may support sustainability and longevity of research partnerships (Newman et al., 2011). Furthermore, the creation of partnerships across communities and organizations has the potential to extend beyond existing funding cycles and produce ripple effects that continuously improve health outcomes across rural communities.
Limitations
There have been challenges in recruiting and adequately compensating rural community-based staff given the current economic climate where low unemployment rates make recruiting BA or MA qualified staff difficult. As we try to expand the numbers of community researchers and locate them in specific areas to develop our rural footprint, these human resource challenges will undoubtably continue and require a constant investment in recruitment and training.
Several seasonal challenges in northern rural Minnesota impact CERDAR’s CBPR efforts. First, the winters can be long and often involve subzero temperatures, high winds, and heavy snowfalls that make travel perilous. Second, late fall and winter schedules are full of holidays in western societies, and these periods of time can be difficult to work around for qualitative research and large meetings. Third, when the long winters pass, many northern rural residents take much-needed summer vacations and can be difficult to reach. Fourth, the seasonal nature of the economies related to agriculture and tourism affects the availability of participants at different times of the year.
There also exists the potential for funding instability which could hinder sustainability and growth of the model. Short-term, grant-funded research alone is insufficient to build the research infrastructure necessary to support a regional CBPR model. Grant funding is crucial to the sustainability and growth of established networks, but ongoing core funding from the University or foundations is needed to support university and community-based staff as they continuously build and maintain community relationships.
Conclusions
Our work addresses the pressing issue of underrepresentation of rural participants in AD/ADRD research by applying a regional CBPR approach to recruitment and research. Rural populations are considered hard-to-reach in health research for a number of factors: geographic isolation, socially disconnected from research institutes, low health literacy, and distrust of research entities and outsiders (Kim et al., 2014; Tanner et al., 2015; Thurman & Harrison, 2020). The MK-MDT utilizes a unique regional CBPR approach that draws upon mixed-methods and is suited for social and cultural contexts of rural people and communities in northern Minnesota. The model recognizes that the strengths and diverse perspectives of academic and community-based staff and advisors are necessary to ensure the incorporation of local knowledge with academic research. This research framework employs a reflexive approach to participant recruitment and advisory roles that promote geographic representation of the data collected. Community researchers ground the research approach in a cultural lens that is both familiar and trusting, and reflexive processes are built into meetings among investigators, research associates, data analysts, and two advisory boards as they discuss research processes and findings. There does not appear to be any CBPR health research center focused on rural AD/ADRD in the US; thus, the MK-MDT and CERDAR program fulfills a critical role in revealing the unique barriers and facilitators rural people face with AD/ADRD care. Ultimately, this method will contribute to a better understanding of the health disparities between urban and rural populations.
Sustainable community-research relationships must be culturally appropriate, adaptable, responsive, and adequately and continually resourced to address the specific needs and research questions that communities want addressed. Through the application of a regional CBPR approach, we have demonstrated the feasibility of conducting foundational AD/ADRD research with rural populations across vast geographies, including the creation of structures that allow for the flow and exchange of knowledge between the rural north of Minnesota and the University of Minnesota.
Footnotes
Acknowledgments
We would like to acknowledge our Community Advisory Group, Rural Research Advisory Group, and Rural Advisor Dr. Shawn McMahon for their continued effort and support of the MK-MDT CBPR framework. We also wish to acknowledge and thank the late Dr. Jim Boulger for his unwavering support for our rural research vision. Finally, thank you to Drs. Dana Ketcher and Amy Otto, and Margaret Noun, for their help and feedback on the manuscript.
Ethical Statement
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Memory Keepers Medical Discovery Team – Health Equity, University of Minnesota Medical School and a University of Minnesota Medical School Academic Investment Research Program (AIRP) Grant. The development of the model was also supported in part by The National Institute on Aging of the National Institutes of Health under award number R21AGO72566 “CareBand: A Collaborative Pilot Study to Optimize a Life-Space Performance Metric for Monitoring and Early Detection of Alzheimer's Disease and Related Dementias in Rural and Indigenous Communities.” The content is soley the responsibility of the authors and does not necessarily represent the offical views of the National Institutes of Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.