
Abstract
There is little understanding of challenges encountered when recruiting people who frequently use urgent and emergency care (UEC) services to qualitative research. This is despite considerable evidence that people who frequently use healthcare services are a heterogenous group, who are under-served in qualitative research with voices that are seldom heard. This is particularly problematic when their use of healthcare services is often associated with unmet complex health or social care issues, chronic health conditions, and factors such as lower socioeconomic status; also associated with lack of involvement in health research and challenges to health status. This paper provides insight into recruiting this under-served and seldom-heard population to qualitative research studies and suggests how identified challenges could be overcome in future research. Using Rolfe et al.’s Reflective Framework (2001), we examine processes and outcomes of five studies with differing methodological recruitment approaches to identify common challenges and facilitators of recruitment success. All studies aimed to recruit people who frequently used one or more UEC service. In comparing approaches, we identified two key stages of the research process that most contributed to difficulties and successes in recruitment of service users, and thus are deemed to be critical junctures: (1) Research Planning and Design, and (2) Research Delivery. The first contained themes around systems factors and study design factors, whilst the second included relational factors and personal factors. Recruitment was challenging across all studies due to unpredictable interplay of these four factors, indicating that there is no ‘one size fits all’ approach for future research. This reflects the heterogeneous nature of the group, and suggests that multiple, targeted approaches to recruitment need to be co-designed with multiple service users from the outset. We make further recommendations that may also be transferred to other under-served and seldom-heard populations.
Whilst people who frequently use health and social care services are characterised based on their relatively high levels of service use due to their unmet health or social care needs, their voices and experiences are under-served in research contexts with little qualitative research regarding recruitment experiences of researchers in this context. People whose views are not often heard have been viewed as ‘hard to reach’ or ‘hard to engage,’ however, this creates a discourse of blame for their lack of engagement in research. While current literature discusses recruitment challenges, this does not address the unique factors in recruitment of this heterogeneous population. Therefore, we use the term ‘under-served’ in research to describe this population’s proximity to healthcare, while remaining unheard in terms of research. This paper addresses the unique challenge of recruiting participants who frequently use urgent and emergency care services, and as such are well known to some healthcare providers but remain under-served in research. By reflecting on research challenges that contributed to difficulties and successes in recruitment to qualitative research, this paper discusses various factors for consideration when planning and designing research studies with under-served populations. These factors are directly applicable to research in urgent and emergency care settings and are potentially transferable to other settings where people are under-served in research.What is Already Known
What this Paper Adds
Introduction
Qualitative healthcare research helps to inform our understanding of the lived experience of patients, their motivations for contacting and using health services, and their interactions with service providers (Holloway & Galvin, 2023). Qualitative research is key to informing advances in policy and practice, fundamentally shaping understanding and approaches across a wide range of disciplines (Borgeault et al., 2010). Furthermore, research is vital for continual evolution in evidence-based practice and decision making, ensuring that professionals, and both formal and informal services are adapting as the knowledge available to them expands (gov.uk, 2021; NHS, 2023a).
Many groups seldom have their voices heard in research, with reasons for this being multifaceted and complex (Ellard-Gray et al., 2015; Stevenson et al., 2018). Evidence suggests that those who are not represented in research are more likely to be living with chronic health conditions, from lower socioeconomic backgrounds, be from a minority ethnic group and experience significant health and social inequalities and disparities (Argarwal et al., 2019; Prinjha et al., 2020; Scott et al., 2023). Their inclusion in research is vital to ensure a diverse representation of the population and ensure rigour and validity of findings to strengthen transferability (Coe et al., 2023). Recruitment is one of the most important aspects of a research project and can impact the validity of the data, the timescales for completion, and even the viability of the whole study (Negrin et al., 2022). Bonisteel et al. (2021) highlight four phases to recruitment processes; planning, implementation, post-study engagement and assessment of recruitment activities for lessons learned, during all of which difficulties can occur.
Where people’s voices are not heard, they are often referred to as ‘hard to reach’ or ‘hard to engage’ (Adley et al., 2023). However, these terms can facilitate a ‘discourse of blame’ towards potential participants, rather than being an accurate representation of the potential participants not engaging with research (Drewett & O’Reilly, 2023). Further, this term conveys a stigma of difference to this cohort and dissuades further engagement in research (Duvnjak & Fraser, 2013). The term ‘seldom heard’ has been championed by researchers to remove the perceived blame from potential participants, and reduce any associated stigma, reframing this as a challenge for researchers and the methodological approaches employed in recruitment (Prinjha et al., 2020).
In this paper we focus specifically on qualitative research with people who use urgent and emergency care (UEC) services frequently. Seldom-heard groups in qualitative healthcare research are often equated with a low usage of healthcare services, such as avoidance of seeking care for cancer (Hall et al., 2015; Whitaker et al., 2016) and of healthcare treatment in people who use injectable substances (Wright et al., 2020). In contrast, people who frequently use services are known to, and are often engaged with, service providers. However, they can be as hard to recruit into research as more hidden groups (Plishka et al., 2023), and therefore, we refer to this group as ‘under-served in research’, in line with National Institute for Health and Care Research (NIHR) guidance (2022), rather than seldom heard. In doing so, we recognise that being under-served in research frames recruitment challenges as a problem for researchers.
UEC services include frontline organisations such as ambulance services, emergency departments, urgent treatment centres and community pharmacy. Each healthcare organisation has its own definition of how they define frequent use, which differ depending on the service provided and even varies across the same types of services within a single health system. For example, there is considerable variation in definitions of frequent use in both the Emergency Department (ED) (Soril et al., 2016) and Emergency Medical Systems (EMS), (Scott et al., 2014, 2023). Efforts have been made to standardise these within the same services and there is now a generally accepted definition of frequent callers to ambulance services within the UK (e.g. Scott et al., 2023), however how each ambulance service manages this differs (Edwards et al., 2015). It has been suggested that frequent attendance at emergency departments be defined as use as five or more times in a 12-month period which has been adopted by the Royal College of Emergency Medicine (RCEM, 2024)). However, the National Health Service (NHS) England guidance for high intensity use suggests focusing on the top fifty people with the most frequent visits to the emergency department (NHS England, n.d). Frequent contact with services may be undesirable for both service providers (placing additional strain on already strained services) and for patients (their needs may not be met appropriately), and this patient group is increasingly coming to the attention of policy makers (Kreuter et al., 2021; NHS, 2022). Reasons for frequent use can be complex and diverse, stemming from unmet social needs, adverse mental health, socio-economic factors, substance use or chronic medical conditions (Agarwal et al., 2019; Hudon, 2016; Scott et al., 2021). This can often lead to a stigmatisation of the person and receipt of low-quality care and thus can be detrimental to the person whilst not addressing the underlying reasons for frequent contact (Brodeur et al., 2020).
Frequent use can be considered problematic and, depending on the organisation, strategies to manage this can range from proactive management and support, through to punitive measures (Hudon et al., 2016). Research which adds to knowledge of how best to support both the person who frequently contacts or uses services and the service itself is imperative to better address the needs of the individual and reduce strain on overburdened services (Scott et al., 2021). In particular there is a need for further qualitative research into the lived experience of those who make frequent contact with providers, to understand their needs, motivations, and experience of contact with services.
This paper aims to offer insight into recruiting this under-served and consequently, seldom-heard population to qualitative research studies, as well as suggesting how identified challenges could be overcome in future research. We aim to do so by describing and critically reflecting on recruitment approaches used in five research studies that included qualitative components, led by multiple different research teams, exploring frequent use of UEC services. In doing so we aimed to identify themes in relation to both barriers and facilitators to recruitment and make recommendations for future methodological recruitment considerations with people who use UEC services frequently that could have transferability to other settings where people are seldom heard in research.
Methods
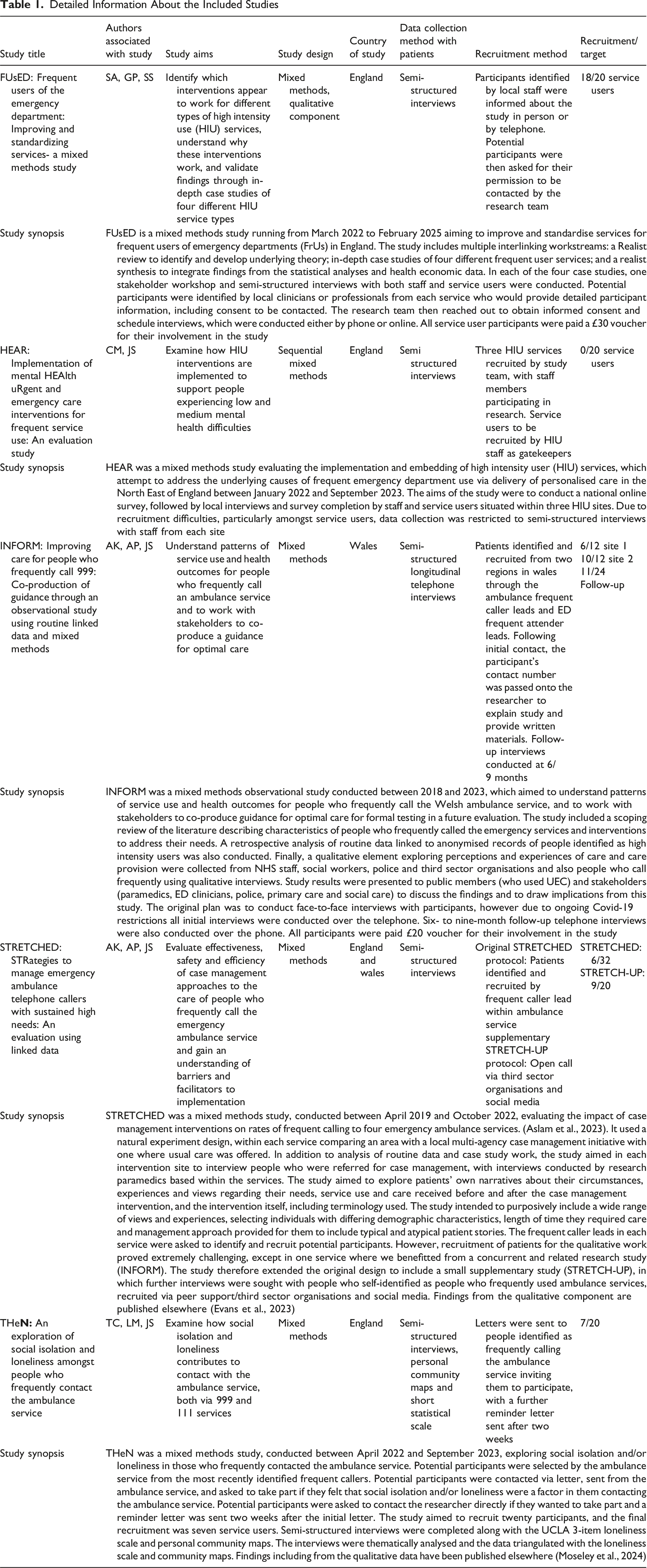
Selection and Description of Studies
Detailed Information About the Included Studies
Positionality
All authors, consisting of a mix of genders, were based in universities in England and Wales and ranged from early career pre-doctoral researchers through to senior academics, all with experience of conducting applied health services research in pre-hospital emergency care. Authors have experience of working in and contributing to healthcare (NHS), local authority (drug and alcohol services), and community and voluntary sector (charities).
Reflection and Analysis Process
To generate data, each team reviewed and reflected on their recruitment processes using Rolfe et al.’s Reflective Framework (2001), which consisted of three key questions; (1) ‘What?’, (2) ‘So what?’ and (3) ‘Now what?’. Rolfe et al. offer a revised version of the framework (Rolfe et al., 2011), however the earlier version offered a pragmatic framework for reflection across studies. Following independent reflection on recruitment processes by each study team, data were analysed collectively by two authors (CM and LM) to identify commonalities and differences across the three key questions. These were then inductively grouped into initial themes, which were then further analysed to develop explanatory themes that included how themes had operated as barriers and facilitators to recruitment (‘So what?’) and how these could be overcome (‘Now what?’). Between each stage of analysis, meetings were held with representatives from each team (all co-authors) to offer additional insights and reflections on recruitment processes through sharing of experiences, shaping ongoing analysis, and ensuring each study was fully and accurately represented in the findings. The final themes were shared and discussed with all authors for final agreement.
During the studies, and of importance to our analysis, was the use of gatekeepers to support various research processes. We therefore considered our use of the term gatekeeper within this article. Lie et al. (2022) champion the term ‘gateways’ to describe the person who facilitates a relationship between researcher and community of interest. Other descriptors such as community connectors, research champions, and community advocates are also recognised as less stigmatising language, however they mainly refer to formal roles with these titles (Burn et al., 2020; Stahl & Shdaimah, 2008; Wallace et al., 2019). We settled on the term gatekeeper as it is traditionally recognised by research ethics committees (NIHR, 2020), and the included studies took place in healthcare settings where gatekeeper accurately describes the role and function of people who were intermediaries in research recruitment. Complexities regarding the gatekeeper role are beyond the scope of this paper, and are documented elsewhere (Clark, 2010; Gřundělová et al., 2024; Sanghera & Thapar-Björkert, 2008).
Findings
We present reflective findings grouped according to two key stages in the research process: Research Planning and Design and Research Delivery, representing critical junctures relevant to recruitment of participants. Within Research Planning and Design, the Study Design and the Healthcare and Research Governance Systems within which the research took place were key contributory factors. In the Research Delivery theme, recruitment was impacted by both Personal and Relational factors. Whilst we have presented these factors individually, the challenges often influenced one-another, highlighting the complexity of recruiting a heterogeneous group of people who may have complex health and social care needs. Together, the themes, which were developed using Rolfe et al. reflective framework (2001), highlight the need to consider multiple factors starting with study conception and design, through to the conduct of studies that account for both relational and personal factors, through to system-level issues that exist in both the governance of research and delivery of services. Figure 1 shows a thematic map of the findings. Thematic Map of the Critical Junctures and Themes Associated With Recruiting People Who Frequently Use Urgent and Emergency Care Services
Research Planning and Design
Research Planning and Design was a key element which impacted recruitment. Within this theme, both the Study Design and the Healthcare and Research Governance Systems, within which research is undertaken, were identified to influence recruitment.
Study Design
Flexible and Modifiable
Being flexible in research approaches and allowing for ad-hoc modifications to study design were seen to be crucial to recruiting patients. Feedback was obtained in the form of complaints from five people who were invited but declined to participate in the THeN study, who indicated that it was inappropriate to receive an invitation letter as they felt it accused them of misusing the ambulance service. The original letters sent by the THeN team, produced with input from a patient and public representative (see Co-production theme), took care not to mention people who contacted the ambulance service frequently, did not imply any misuse, and was worded to avoid stigmatisation. However, based on this experience, the letter was amended with further input from a patient and public involvement representative to make the purpose of the study clearer. This revised letter was sent to the same number of people (100) and received only one complaint. A need for flexibility was also identified in the STRETCHED study; the original plan was to recruit from four ambulance services, but there were significant challenges in three areas, so participants were recruited only from one, where the research team were able to combine data collection processes with the parallel INFORM study. In addition, the STRETCH-UP sub-study was added, with the aim of recruiting participants directly via social media. This process added extra time to the project and required additional university ethical approval. FUsED had an ethics amendment to widen recruitment of service users beyond the four case sites by asking organisations to share a flyer about the study. On reflection, the HEAR study, which was hindered in its recruitment of patients by high staff turnover in all participating organisations (see Healthcare and Research Governance Systems theme), would have benefited from a continuation of work, though this flexibility was not possible due to finite research funding.
Co-Production
Critical reflection highlighted the reliance of partnerships between existing services and Patient and Public Involvement (PPI) in research to facilitate recruitment and sense-check materials and procedures. Studies benefited from involving staff and PPI representatives in their design. THeN had strong staff input including in deciding the topic (via FreCaNN) and with a staff co-applicant. The team initially attempted to identify and recruit a past patient with experience of frequently using the ambulance service but were unable to, due to not having any pre-existing contacts. Without success, THeN researchers instead identified someone with experience of isolation and loneliness who helped to re-design recruitment letters (see Flexible and modifiable theme) through existing research networks and via PPI in pre-registration programmes at the host university. The HEAR study did not have PPI input until the later stages, in which a patient forum read over the information sheet and consent form to ensure language use was appropriate and inclusive. Minor changes were recommended, and were made before these materials were distributed. FUsED involved PPI representatives from the early stages of the research programme design, who played a crucial role in reviewing the interview topic guide for service users and participated in pilot interviews with qualitative researchers, which helped refine the approach to engaging participants. The group also provided valuable feedback on improving our recruitment processes. Based on the PPI input, FUsED submitted an amendment to the research ethics committee and Health Research Authority (HRA) to allow advertising of the study in non-NHS sites, such as patient and family associations, to enhance direct recruitment efforts. INFORM has support from two public members with lived experience of frequent calling. They were involved from initial study inception, design, and delivery. They were also members of the Research Advisory Group. Both PPI members were also involved as research co-applicants on the STRETCHED study, as and subsequently became active members of the multi-disciplinary Research Management Group, also contributing to analysis and interpretation. The STRETCHED team also established a Lived Experience Advisory Panel of eight public contributors with relevant lived experience, chaired by one of the public co-applicants, which met at key stages of the study to provide in-depth input to study design, interpretation, and dissemination.
Method of Participation
There are multiple ways in which people can take part in research, and where studies were underway at the outset of the Covid-19 pandemic, this often consisted of a shift to collecting data remotely, either via telephone or digital online approaches. Conducting interviews remotely brings new challenges, but in some cases can be more convenient for all involved, due to the lack of travel time or costs (Self, 2021). The FUsED team, which collected data after restrictions related to the Covid-19 pandemic had ended, highlighted digital exclusion (where people are excluded from research due to lacking digital means of participation) as both a consideration by gatekeepers and as a barrier to taking part in research for potential participants. However, some sites had close relationships with service-users and (following an ethics amendment) a supported participation model was implemented, in which staff were able to provide support regarding facilities and technology. During analysis of the studies, we observed that having the skills to use digital technology and/or access to resources required to participate interacted with wider determinants of health, including the social conditions that contribute to increased use of services and may further exclude people from participating.
It became apparent that the use of multiple methods, such as telephone and digital methods, may also aid in recruitment. For example, during interviews for THeN participants were given a choice of participating either via phone, online call, or face-to-face interview. Of the seven participants, four chose to meet the researcher face-to-face and three opted to be interviewed via telephone; none opted for an online interview. FUsED participants were offered online video calls or telephone calls and of the fifteen participants, eleven chose to be interviewed by telephone. The INFORM study took place during the Covid-19 pandemic. The original study design intended to use ‘Books of Experience’ to encourage patient centred interviews (Khanom et al., 2015). Participants were to be given a scrapbook to record their experience of care and reasons for calling. The books would then be used to conduct face-to-face interviews, however, pandemic restrictions necessitated that this was changed to telephone interviews without face-to-face contact to provide the scrap books (see Flexible and modifiable theme). Several scrapbooks were posted to participants, but only one person returned the book. The INFORM study has the highest level of recruitment of the studies discussed. As such, use of the Rolfe et al. (2001) reflective framework showed that whilst technological exclusion may be a concern for some potential participants and some may prefer a face-to-face interview, it is more important to offer flexibility and a range of options for participants.
Renumeration
Offering participants remuneration was another consideration when designing studies. INFORM and STRETCHED (via the STRETCH-UP sub study) offered a £20 voucher for participation and had the highest recruitment levels. Whilst there is no data available to consider whether this voucher contributed to the higher recruitment levels, it is a factor for consideration given the recruitment challenges faced by other studies. The FUsED team offered a £30 voucher and recruited almost to their target level. The teams reflected on the need to find a balance between recognising that participants are providing their time, including amongst people who are experiencing social conditions including deprivation, and the potential biases that research incentivisation may introduce (Head, 2009; Zutlevics, 2016). However, the ability to offer remuneration is often outside of the researchers control and the THeN and HEAR studies were limited by the research funding provided, which had not costed in payment to participants in the funding application.
Research Governance Systems
Ethics processes
During critical reflection on the studies, it became apparent that it is common for ethical processes to impact on the recruitment process. In three studies, ethical approval was delayed due to the infrequency of ethical panels for qualitative research. Further, THeN was delayed by an unfavourable decision from the ethics panel, due to concerns that the clinical team approaching people was coercive, yet a similar strategy was approved for other studies. A further example of inconsistency was found, as the HEAR study were told by the ethics panel that they could not send reminder letters to potential participants despite this being approved for THeN. Despite rigorous ethical approval processes, there were still sometimes concerns amongst staff members when identifying participants (see Participant selection theme). In the INFORM study, this was overcome by reinforcing that there was a robust strategy to ensure participants were fully informed of the research and the development of a process (see Flexible and modifiable theme) that ensured safeguarding issues or safety concerns arising during data collection would be passed on to staff from the recruiting organisation.
Organisational Infrastructure
Challenges were identified across all studies relating to the structure of participating NHS organisations to support research. Interest in supporting research often consisted of involvement at an individual rather than organisational level, meaning that those supporting the research did so because of their interest and passion in the topic, but this was subsequently hindered by high levels of staff turnover, which then impacted on relationships with potential participants (see Relational factors > Communication theme). Within the HEAR study, management staff who had buy-in and engagement and who were acting as gatekeepers moved on to other roles during the recruitment period and were replaced with other staff. On reflection, whilst the new staff members engaged with the study, not being involved from the outset likely impacted their motivation to support recruitment, in part due to unfamiliarity with the research. Further, staff had little capacity due to time constraints caused by clinical pressure, itself exacerbated by staff changing roles. THeN had a service provider as a co-researcher and therefore found that the level of commitment to recruitment was consistent and supportive throughout (see Co-production theme). Initially, FUsED worked with organisations that had close case-worker relationships with service-users and easily met recruitment targets. However, in services that did not foster close relationships with service users (e.g. NHS case-management approaches) establishing contact with potential respondents was highly problematic. This led to a substantial imbalance of under-representation, depending on the type of services provided.
Research Delivery
In reflecting on Research Delivery, two key themes were identified: Relational factors and Personal factors. While separate from Research Planning and Design, they remain interlinked as these factors were both influenced by, and influenced, the study designs and the systems within which the research took place.
Relational Factors
Gatekeeping and Communication
On critical reflection, communication between the research team and providers was a key element across all the studies which impacted on recruitment, reflecting the wider organisational contexts in which the studies were conducted (Rolfe et al., 2011). All five studies recruited via gatekeepers working in relevant organisations. Whilst two studies included staff as co-researchers (see Co-production theme) when obtaining the funding, only one study (THeN) included the person that was acting as gatekeeper. The gatekeeper, regardless of study, was a key role that underpinned recruitment success, though in some cases was also a barrier, due to reasons such as staff turnover and lack of buy-in (see Organisational infrastructure theme). The HEAR study had regular meetings with gatekeepers who were accessible and supported the project, however the study team were unable to define whether gatekeepers were approaching patients for recruitment and any barriers to participation. To support recruitment, the STRETCHED study team held a training day for paramedics as researchers, however they were not able to use these skills due to lack of participants recruited, resulting in frustrations for all involved. THeN recruited via letters sent out by the service provider. While this approach did recruit participants, it may have also hindered some potential participants. For example, the researcher received a phone call from one letter recipient who explained he was unable to read the letter and had phoned to enquire regarding the nature of the letter. While this individual did agree to participate after a conversation with the researcher, it is possible that others with limited literacy may have also received letters and subsequently discarded them. In the INFORM study, the Research Fellow attended monthly multi-sector case management meetings led by the Emergency Department Frequent Attender leads six months prior to recruitment of participants. This approach enabled the researcher to build rapport with a range of staff and had a high chance of potentially fulfilling the study recruitment quota, however the onset of Covid-19 led to delays and staff turnover.
Participant Identification and Selection
Selection processes for recruitment of participants was a key factor found in all studies upon critical reflection. People who frequently use UEC services account for a small percentage of the population, therefore, there is a relatively small cohort of potential participants from which to recruit. This can be further impacted dependent on the scope of the research; for example, STRETCHED participants also had to have experienced case management intervention, whilst THeN only recruited people who self-identified as experiencing social isolation and/or loneliness. STRETCHED experienced far lower recruitment than anticipated, in part due to the gatekeeper excluding people after screening due to the service user being deemed at risk of distress or too challenging to take part. This led to a re-evaluation of study scope and an additional sub-study being added (see Flexible and modifiable theme). HEAR encountered similar reticence from staff who had joined the organisation partway through the study (see Organisational infrastructure theme), however this was in part due to unfamiliarity with the research process and the requirements of gatekeeping. FUsED experienced variable levels of caution from gatekeepers who screened potential participants regarding the perceived appropriateness of participation for individuals. THeN benefited from being a collaborative study with the service provider who had been involved from study conception including study design (see Co-production theme), though still encountered difficulties due to concerns by an ethics committee regarding coercion (see Ethics processes theme), highlighting tensions that researchers need to overcome when working closely with gatekeepers.
Participatory Care
Much consideration was given by the research teams, using Rolfe et al. reflective model, to Participatory care, which we define as service users (as participants) and researchers collaborating to support the individual’s care and support needs. Whilst some consideration for this was given in the production of recruitment materials, such as signposting people to relevant support services, participatory care particularly took place after recruitment. All the studies involved vulnerable people who were experiencing difficulties related to their physical, mental and/or social care needs which led them to access healthcare services frequently. Difficulty navigating health and social care services meant that researchers were often asked questions about the participant’s care, and study teams reflected on how being prepared for this allowed them to provide support. An example of this was during the INFORM study where the researcher supported a participant to access required equipment after several years of frustrations for the participant trying unsuccessfully to get this themselves. Furthermore, during THeN, the researcher was able to provide extensive advice and signposting to a participant around local services due to the researcher’s previous professional practice background.
Personal factors
Fear and Stigma
Critical reflection by the study teams highlighted the considerable issue of potential fear and stigma felt by potential participants when invited to take part in research. The teams were conscious that potential participants may have perceived that they were under scrutiny or being blamed for excessive use of services, and that this may have contributed to a reluctance to participate. Furthermore, all five studies addressed sensitive topics, some of which were more specific than others (e.g. THeN which focused on the role of isolation and loneliness), which meant that participants may not have deemed the research relevant to their own situation. This is particularly challenging, as the people who frequently use healthcare services are recognised to be a very heterogeneous group with complex health and social care needs. Upon consideration, potential participants may have been suspicious of researchers’ motives, and a possible unfamiliarity with or lack of trust of research may have added to people’s fears. As the studies were examining people’s experiences related to frequent use of healthcare services, those who fit study criteria may have perceived stigma when invited to take part in the studies. Some people invited to the study did not consider their use of healthcare services to differ from the norm and were resentful of the implication – whether unintentionally implied or not – that it may not be appropriate. Care was taken to ensure that language used in participant information leaflets was non stigmatising and neutral, with all studies asking a PPI group to check that materials were suitable (see Co-production theme). This highlights that even co-produced study materials alone is not sufficient to address service users’ fears and perceived stigmas.
Personal Circumstances
The personal circumstances of potential participants were considered, and how they may have impacted on their decision on whether to take part in the research. People who frequently use UEC services likely have some form of unmet physical health and/or social care needs, including those related to physical health, mental health and compounding social factors such as loneliness, financial insecurity and unstable housing. In relation to the HEAR study, gatekeepers felt that some of these factors would inhibit participation, and they did not have the resources to offer necessary extra support to participate. Study teams reflected that the complexity of these factors were likely to influence potential participation in numerous ways such as participants not feeling well enough to participate, concerns about discussing their use of UEC would have on their mental health, not having a private space to participate in the research or digital exclusion (see Method of participation theme). Analysis of reflections on possible personal circumstances reinforced the importance of conducting research with, not on, people who use services frequently (see Co-production theme) to better understand their personal experiences and situations, and to ensure that research is designed with consideration for their needs and concerns. In THeN personal circumstances both helped and hindered recruitment. For the people who did choose to take part, they all commented that this was an opportunity to tell their story, and four of seven participants commented outside of data collection that it was nice to have something to do and/or someone to talk to. Given that these participants self-identified as socially isolated and/or lonely, the opportunity to partake in research gave them some contact. However, people also contacted the researcher to decline to take part for reasons including feeling their current health problems meant participation would be too difficult, or that their social isolation and/or loneliness detracted from the medical needs that they had. The INFORM study was able to follow-up on eleven out of sixteen respondents to conduct follow-up interviews six to nine months later to check on health outcomes, calling behaviour and any change in circumstances.
Discussion
This paper discusses factors relating to recruitment to studies investigating the frequent use of UEC services, drawing from experiences and reflections of five study teams. In doing so, we identify two critical junctures in the qualitative health research process that contribute to recruitment of people who have complex needs. They were identified by utilising the ’What’, ‘So What’ and ‘Now What’ cycle of analysis within the Rolfe et al. reflective framework; producing recommendations to overcome recruitment barriers which were developed during the ‘Now What’ stage of analysis. The first critical juncture is the research planning and design stage, where it is important to adopt flexible study designs that are co-produced with a diverse cohort of people with experience of frequently using services. Within this juncture, it is necessary to negotiate healthcare and research governance systems, which have the potential to hinder suitably flexible approaches. The second critical juncture, research delivery stage, requires consideration of the personal and relational factors, especially addressing fear and stigma and understanding that each service user is likely to have unique personal circumstances.
Through critical reflection, which contributed to the planning and design themes, we recognised links to well-known challenges in recruitment prior to a project beginning, which were dependent on how the research is designed and the potential participants who are sought to participate. This is often related to the researcher’s positionality and their prior knowledge of the group they plan to engage with (Sanghera & Thapar-Björkert, 2008; Wilson et al., 2022), however even if there is a strong plan for recruitment, obstacles will often persist. Daly et al. (2019) highlighted that in healthcare research, lack of adequate recruitment impacts study outcomes and often leads to a requirement for an extension. Further, our reflections in relation to research delivery are often recognised across other areas of qualitative research, where recruitment methods can pose challenges in accessing participants, leading to underrepresentation and poor inclusion in sampling (Tromp & Vathorst, 2015).
Undertaking research with this unique group of participants, who are well known to UEC services, yet under-served in research, requires careful planning (Oliver et al., 2019). The ability to be flexible in the research approach was instrumental in successes seen within the projects we examined. This included the methods in which participants could be involved, such as offering a choice of face-to-face, online or telephone interviews. A balance between delivering research to benefit and understand vulnerable populations, and ensuring psychological and emotional safety of participants was important to all teams (Alessi & Khan, 2022; Gordon, 2020). Benefits such as feeling heard, feeling helpful and contributing to wider knowledge were noted by McDonald et al. (2013) and Staphorst et al., 2017. However, thought must be given to inclusion/exclusion criteria and the capacity of the participant at the time of data collection, to allow ethical representation of a broad population (Finnegan & O’Donoghue, 2017). Additionally, we recommend detailed thought as to balancing the needs of the study and researcher capabilities, with the known challenge of limited involvement with the participants long term care (Garrels et al., 2022). The nature of the five studies meant that the opportunity for researchers to positively benefit participant care, or impact on difficulties participants were facing, was limited in most cases to signposting. This can cause frustrations for both the researcher and participant and led to considerations about whether the researchers should take a more active role in supporting participants. Interpretation of participant-researcher boundaries and how involved a researcher can be in someone’s care should be carefully considered. It may be outside of the research remit or boundaries to advocate for the individual; however, it is difficult for the researcher to ignore circumstances which they can influence (Eide & Kahn, 2008; Mitchell & Irvine, 2008). Given the often complex circumstances faced by people who frequently use UEC services, it may be of benefit to them if participating in research were to address some of their challenges (von Benzon & van Blerk, L, 2017). We recognise that this is difficult to achieve without unintentionally becoming an additional source of ongoing professional support, though broader developments in providing public health interventions, such as social prescribing, in UEC settings may help to provide suitable signposting opportunities for researchers and service providers alike (Cooper et al., 2024). Co-production of research with organisations and peer researchers can offer a different dynamic to that of traditional, hierarchical research; forming longer term alliances to address long term goals (Bandola-Gill et al., 2024; UKRI, 2024).
A further consideration of the study design is remuneration of participants’ time, as is good practice (NIHR, 2024). The authors recognise that this may not be possible for all studies due to research funding constraints, but remuneration can potentially have a positive impact on recruitment. Ballance and Ripley (2023) note the importance of ethical participant payments to reflect time cost and other expenses. Additionally, Largent et al. (2022) found that over half of participants were not influenced to take part in research by financial incentives. The use of remuneration is also not without ethical concern, particularly that it may unduly influence someone to take part, having a negative effect on the person. Różyńska (2022) presents a practical, ethical analysis of remuneration, drawing attention to four principles as an ethical anatomy of payment: social beneficence, respect for autonomy, individual beneficence and justice. Guidelines for offering remuneration can support decisions around this, for example noting that a payment may impact the participant’s benefit claim (Fox et al., 2024; NIHR, 2024). Discussion around remuneration and making the participant aware of factors such as impact on welfare claims are vital in the early stages of research planning.
Collaboration with PPI is considered to be best practice in research (UKRI, n.d). In healthcare settings, there is scope for further co-production, but this would likely necessitate culture change (Pain & Francis, 2003; Boaz, 2021). This being said, co-production can be achieved at a significant level in healthcare research. Kim et al. (2023) utilised patient-led research and found authentic partnership to be a key theme of successful recruitment and retention. Our key findings suggest that a co-production approach to research with people who frequently use UEC services would be of particular benefit in understanding, from those with lived experience, the best approach to research with this group. Incorporating this with a flexible design that allows multiple avenues of recruitment would further increase participation. Close and trusting relationships between service-users and staff within services can be key factors for successful recruitment, meaning that pockets of seldom-heard voices might persist within groups receiving services that do not prioritise building these strong personal relationships (Jordan et al., 2015; Sy et al., 2022).
One challenge which was highlighted during the reflective process is receiving ethical approval. Ethical approval in research is paramount to ensuring that research practice is sound and conforms to the overarching principle of ‘do no harm’. Research ethics evolved from the 1947 Nuremburg Code (Wynn, 2017) and adapted in response to various harms and documented unethical practices in research (Hammett et al., 2022). In 2005, in the UK, a number of research councils made it mandatory for any funded projects to undergo ethical review, at the same time that institutions tightened their own ethical procedures (McAreavey & Muir, 2011; Morris, 2015). Additionally, research taking place in NHS settings requires ethical approval from the HRA. While there is little disagreement on the basic principle of ethical approval (Hammett et al., 2022) there are numerous critiques about how ethical approval processes are administered, how qualitative research is viewed, bio-medical standards being routinely used for research in the social sciences, and ethical approval processes being increasingly bureaucratic risk management exercises rather than safeguarding against unethical practice (Hugman et al., 2011). The authors do not disagree with the importance of ethical approval in research, however, suggest that approval processes be reviewed and streamlined, as well as ensuring that the differing approaches to healthcare research are not all judged by the standards of medical trials. Hickey et al., (2021) offer an alternative critique of ethical processes, suggesting a reframing of ethical review which includes Deliberative communication, Engagement with researchers and the Distribution of responsibility. Whilst HRA have instigated a streamlined process for qualitative research with lower risk groups and staff participants via proportionate review, we have evidenced how existing processes can be a barrier for recruitment of higher risk patients. This is a particular challenge for those groups, such as people who frequently use UEC services, who are already under-served in terms of understanding of their lived experience. Our critical reflection echoes concerns that researchers often modify studies primarily to satisfy ethics panels, leading to increasingly bureaucratic governance. Such rigidity can hinder innovation, flexibility, and responsiveness, all of which are essential qualities when engaging with under-served participants (Allen & Israel, 2018; Ellard-Gray et al., 2015; Marcus & Lerman, 2018).
Organisational research culture is known to impact buy-in, as healthcare staff’s research understanding is influenced by both research culture within the organisation, and individual knowledge and experience (Harding et al., 2016). Key organisational challenges identified during the reflective process included training and upskilling staff in conducting research (Stewart et al., 2015), funding (Harding et al., 2016) and time constraints (Lamb et al., 2016). Luckson et al., (2018) suggest the use of a framework such as Cookes’ (2005) framework for research capacity building. Individual, team and organisational buy-in is necessary to support good organisational culture (Luckson et al., (2018). As evidenced by the THeN study, the service provider in a co-researcher role can improve motivation, contributing to recruitment. We recommend this as an important aspect of engaging this seldom heard group, as service providers are most likely to have significant and meaningful contact, being better placed to discuss the project with potential participants. However, it should also be noted that this may also reduce recruitment due to overprotection of participants, and staff not believing they have the skills to introduce the topic (Preston et al., 2016). Therefore, this links back to not only collaborating with an organisation to carry out research, but also to addressing the aforementioned challenges in research culture (Oliver et al., 2019), in addition to providing suitable research training for service providers and co -researchers. Peer support workers and peer research advisors can also support research co-design, coproduction and recruitment. When gatekeepers lead recruitment, personal relationships and trust building with participants is not accessible to researchers in the initial stages. The benefit of direct communication between researcher and participant was evident in recruitment for HEAR, as gatekeepers were under time and staffing pressures; however, it is to be noted that gatekeeping is essential to protect vulnerable people (Kay, 2019). Power imbalances between staff and patient must be considered when healthcare staff carry out recruitment, as informed and non-coercive consent is essential for ethical research projects (Ocloo & Matthews, 2016). Prout et al. (2022) found that embedding recruitment into a nursing service enhanced participant buy-in and motivation and added value to clinicians’ roles. The importance of developing partnerships between researcher and practitioner as gatekeeper was evident in the studies within this paper (Gelinas, 2016), as was the importance of partnership between organisations (Clark, 2011; Spacey et al., 2021). Literature regarding communication between researcher and practitioner aligned with our reflective findings; echoing the importance of open, clear communication and boundary setting, including focus on mutual understanding of each other’s positionality (Garland et al., 2006; Rycroft et al., 2015). Williams et al. (2020) state that the onus to build and maintain relationships is with the researcher, including knowledge translation and ensuring accessibility of language and materials. This is in line with our findings, and we recommend a focus on communication skills, alongside gaining an understanding of each organisation and individuals’ role and standpoint in the research.
Fear and perceived stigma can affect people’s willingness to participate in research (Sheridan et al., 2020). People who frequently use UEC may have experienced institutional stigma from services, and/or experience internalised stigma regarding their mental and physical health needs (Chronister et al., 2013; Nyblade et al., 2019). Sampling may therefore not be representative of the heterogeneous cohort, as voices of those experiencing fear or stigma may be lost in the recruitment process. Potential participants may not come forward for numerous reasons, including fear of being blamed, not understanding their role and the purpose of research and lack of social support to participate (Shé et al., 2019; Teodorowski et al., 2023). In addition to this, personal circumstances as detailed previously may impact ability to take part. Cvetanovska et al., (2023) found that factors such as personal characteristics and emotion or stress during healthcare interactions impacted relationships between clinician and patient, and this appeared to be transferable to recruitment via gatekeeping in the five studies reflected upon. To achieve future research impact, co-production of research creates learning and wider understanding of research processes by involving participants as co-researchers during the research process; beginning in the initial stages of a project in methodology discussions, data collection and analysis (Abma, 2018; Amann & Sleigh, 2022; Smith et al., 2022). Dissemination of findings and feedback in accessible, non-academic formats such as brief reports, blogs, infographics and posters potentially reduces feelings of stigma by increasing understanding and promotes future possibility of involvement (Knoepke et al., 2019; Kost et al., 2013). As co-production is not always possible for reasons of time and funding, participant engagement throughout the process, including periodic updates, is recommended. This method is not without flaws and may only support people who are interested in research but may appeal to others over time as a research base is established via consistent research collaboration with people in practice.
Conclusion
As a collaborative group of five study teams in the UK undertaking research in this area, we believe the implications of this paper may benefit researchers, clinicians, and participants by providing insights on how to best devise and carry out research to include people who are under-served in research ethically and practically. Creating flexible, co-produced study designs with a broad range of people who have various experiences of using UEC is essential, though this requires navigating research governance systems that are sometimes overly bureaucratic and may further silence seldom-heard voices. When delivering research, addressing personal and relational factors such as fear, stigma and the unique personal circumstances of people who frequently use UEC services is necessary. To conclude, our reflections highlight two critical junctures for the successful recruitment of people who frequently use UEC services to qualitative research: the research planning and design, and research delivery stages of the research project.
Footnotes
Acknowledgements
We are thankful for the time and effort of the internal and external project partners and the collaborative effort of all the research study teams involved. The THeN team would like to thank the steering group for all their input.
Ethical Consideration
FUsED: REC 23/WM/0055; HEAR: REC 22/SS/0051; InFORM: REC 19/WA/0083; STRETCHED: REC 19/WA/0216 and STRETCH-UP: REC 20222-0048; THeN: REC 23/YH/0003.
Consent to Participate
The authors declare that participants gave verbal/written informed consent to participate in all research studies.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by FUsED NIHR HS & DR Reference Number: NIHR132852. HEAR: NIHR ARC NENC Reference number: NIHR200173. InFORM: Health and Care Research Wales: Health Fellowship Award: HCRW HF-17-1420. THeN: NIHR CRN NENC Targeting Health Needs Award Reference: 179695242. STRETCHED and STRETCH-UP: NIHR HDSR Reference: NIHR180302.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.