
Abstract
Many key groups of people (e.g., older people, disabled people and minoritised people) are at risk of being excluded from research, which will affect the generalisability, quality, relevance, and integrity of the research findings and conclusions. However, ways of making research more inclusive have not been adequately explored. Appropriate strategies to maximise the participation of marginalised populations with diverse viewpoints, expertise, and experience are needed to enable them to make meaningful contributions. In this article, we draw lessons from four case studies that used Group Concept Mapping (a type of participatory, consensus research to generate agreement around a topic of interest within a group, community or society). We reflect on how our research was adapted to engage people with diverse needs (e.g., older/frail people, disabled people, people with language barriers, bilingual participants, and people lacking digital skills) in research. This paper highlights the importance of participatory, time and resources, ethical, and intersectionality considerations to enable marginalised populations to be heard and make significant contributions to research.
Introduction
In the UK, as part of the political reform, patient and public involvement and engagement has been made a strategic priority for more than a decade (INVOLVE, 2012). The UK standards for public involvement set up a benchmark for researchers to improve how the public is involved in research, acknowledging lay people’s experience, skills and expertise (Partnership UPISD, 2019). The National Institute for Health Research (NIHR, 2024) launched a set of new “Guiding principles for community engagement and involvement in global health research” on 6th August 2024, highlighting that research should be shaped by people of diverse backgrounds and communities. In addition to political pressures for inclusive research, health and social care service-receivers and members of the public also demand that they should play a key role in the research process (Moorley et al., 2023; Northway, 2010a).
However, evidence shows that many key groups of people (e.g., racialised communities, people with disabilities or impairments, and older people) are under-represented and marginalised in research (Moorley et al., 2023; Rios et al., 2016; Thake & Lowry, 2017; Yu et al., 2023a). Reasons for excluding these groups are multi-factorial and complex. For example, factors that prevent people in racialised communities from participating in research often include language barriers, mistrust, limited understanding of research and the research process, socio-cultural barriers, costs associated with translation and interpreters, and the perception of being ‘hard to reach’ (Bruton et al., 2020; Farooqi et al., 2022; Wallace et al., 2024; Yu et al., 2023a). Spencer et al. (2024) highlighted the range of language barriers experienced by minority language users in health and social care research, such as not recognising ethnic minorities in the recruitment process, not providing relevant information in people’s preferred language, and the lack of appropriate interpretation services.
In a review of barriers to recruiting disabled people to clinical trials, five broad factors were identified, including risk verse benefit assessment, design and management of recruitment protocol, balancing internal and external validity considerations, consent and ethics, and systemic factors, while the lack of adoption of person-centred, inclusive approaches to consent fails to empower disabled people to exercise their right to make informed choice in research participation (Shariq et al., 2023). Heinze and Jones (2024) argue that visual impairment has a great negative impact on social functioning, such as social isolation and social participation. Major barriers to involving people with sign and/or hearing loss in research often include the lack of accessible information in appropriate formats that address individual communication and accessibility needs, the lack of awareness of room layout and physical space requirements for data collection, and the lack of access to communication and emotional support (Skilton et al., 2018).
Older age is often associated with included vulnerability due to declining health, reduced mobility, experience of social isolation and loneliness, and great unmet health needs (Skilton et al., 2018). Factors that impact on the inclusion of older people in research are diverse, often including a range of individual (e.g., personal characteristics, beliefs, and attitudes), interpersonal (e.g., relationships and networks), organisational (e.g., organisation characteristics), community (e.g., relationships between organisations, such as needs-led services), and policy barriers (e.g., local, national and international policies and law) (Goodwin et al., 2023). Nocivelli et al. (2023) identified seven broad barriers and facilitators to the inclusion of UK care homes residents in research, including issues of research design, understanding of beliefs about research, rapport, eligibility criteria, preference-based decisions, and care home staff and environment. Most of these factors are out of older people’s control, such as research design, communication, and rapport.
While the exclusion of these groups may be unintentional, it has detrimental effects on the generalisability, quality, relevance, and integrity of the research findings and conclusions (Moorley et al., 2023). It is essential to address such under-representation so that effective interventions can be developed for the whole population and people from marginalised groups are provided with the equal opportunities to benefit from evidence-based care (NIHR, 2021). Regardless of various government policy and initiatives, the issue of under-representation of marginalised groups in research remains (Government Social Research Profession, 2022; NIHR, 2020; Varma et al., 2023). Researchers still face many challenges in planning, conducting, and disseminating research in an inclusive manner (Moorley et al., 2023; Yu et al., 2023a). In this paper, drawing lessons from four case studies, we demonstrate how Group Concept Mapping (GCM) can be adapted to engage people with diverse needs and consider recurring issues raised within the case studies through the lens of participatory research.
Participatory Research
Participatory research is not a research design or a research method per se, but an equitable, collaborative research approach where researchers and those affected by the research are in partnership in the research process (Cornwall & Jewkes, 1995; Israel et al., 2005; Marrone et al., 2022). As an umbrella term for various approaches for co-producing knowledge, participatory research can be presented on a continuum based on levels of participant involvement, including ‘public and patient involvement and engagement’, ‘participatory action research’, and ‘community-based participatory research’ (McTaggart, 1991; Salma & Giri, 2021). Israel et al. (1998) identified eight key principles of participatory research, including: 1) Community as a unit of identity, 2) Building on existing community strengths and resources, 3) Collaborative partnerships in all phases of the research, 4) Mutual benefits for all partners 5) Co-learning and empowering process that addresses social inequalities through capacity building 6) Repeatable and iterative process 7) Addresses health from positive and ecological perspectives 8) Disseminates results to all partners
Originating from the disciplines of social sciences, psychology and education, participatory research challenges the assumptions that research should be conducted in a neutral, objective and value-free manner as highlighted in conventional research methodology, such as experiments, case control studies, and observation (Marrone et al., 2022; Rosas, 2012). Participatory research has been widely applied to engage marginalised groups in research, such as older people from immigrant and racialised communities (Salma & Giri, 2021), racial and ethnic minorities with disabilities (Oden et al., 2010), people living with dementia (Hogger et al., 2023), family/informal carers (Bowness et al., 2024), and people with hearing loss (Marrone et al., 2022) or visual impairment (Williams, 2009). Northway (2010b) highlighted five key areas that should be considered by researchers both before and during participatory research, including participatory, ethical, financial, time, and personal considerations. GCM provides a complementary approach (Kane & Trochim, 2007), which helps address some of the key challenges to participatory research, such as ensuring rigour and scientific credibility of the approach and appropriate presentation of all perspectives within a group with equal weight (Allen et al., 2015; Rosas, 2012).
Group Concept Mapping Methodology
GCM is an integrated mixed-methods, consensus-building approach, defined as “a structured methodology for organizing ideas of a group or organization, to bring together diverse groups of stakeholders and help them rapidly form a common framework that can be used for planning, evaluation, or both” (Kane & Trochim, 2007, p. 1). Speciality software (GroupWisdomTM) is used to systematically transform qualitative components into quantitative data as an integral process to gain consensus on a given topic of interest or concept within a group, community or society. Some key features of GCM make it particularly suitable for participatory research, such as the integration of diverse views of individuals with differing knowledge, expertise, interests and experience and a high level of participant inclusion in terms of idea generation, data collection, data analysis and data interpretation (Allen et al., 2015; Kane & Trochim, 2007; Rosas, 2012).
A GCM study can be carried out face-to-face in a workshop format or independently online using Group WisdomTM software, involving a six-step process (Figure 1) (Kane & Trochim, 2007): • Step 1: preparing for concept mapping, including developing focus prompt, sampling and participant recruitment • Step 2: generating the ideas or statements (Brainstorming) • Step 3: structuring the statements (Sorting and Rating) • Step 4: concept mapping analysis (multidimensional scaling analysis and hierarchical cluster analysis) • Step 5: interpreting the maps • Step 6: utilising the maps for action, measurement and evaluation. Flowchart of the Group Concept Mapping Process.
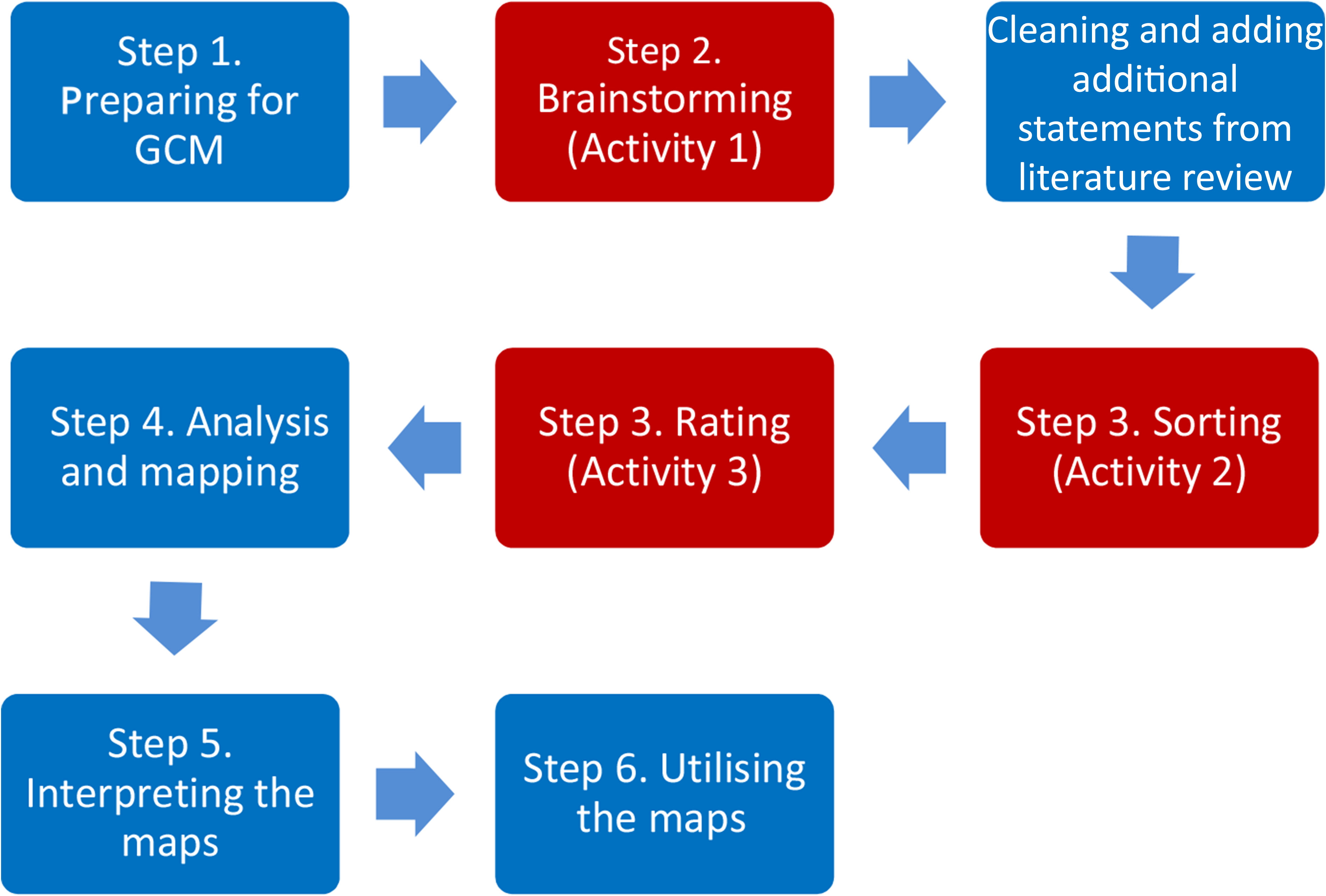
There are three facilitator-led activities. Participants take part in any or all these activities depending on when they are recruited and their willingness to participate (Kane & Trochim, 2007).
Activity 1: Brainstorming (Step 2)
The Focus Prompts and Rating Scales Used in Four Case Studies.

Activity 2: Sorting (Step 3)
Once a set of statements describing the concept for the given topic are agreed upon, participants complete two ‘structuring’ activities (Sorting and Rating). Participants individually arrange or sort the set of ideas/statements into preferred piles/clusters based on perceived similarity. For example, in Case study 1, participants were instructed to group the statements into piles/themes “in a way that make sense to them” to capture their perspectives on what constitutes compassionate care. Participants may generate as many piles/themes as they like, as there is no pre-determined number of piles that participants are expected to sort the statements into. Participants then label the piles by giving each pile of sorted statements a name.
Activity 3: Rating (Step 3)
Participants rate each statement against two or three Likert scales designed to address the purpose of a study (Table 1). For examples, in Case study 1, participants rated statements for importance and experience (i.e., How important do you think this item/statement is to compassionate care?).
Data generated from these three activities (Brainstorming, Sorting, and Rating) are then analysed using GroupWisdomTM software. Results are presented visually as a series of related concept maps, Go-zone reports and pattern matching reports (Kane & Trochim, 2007). For example, Figure 2 shows an example from Case study 4. The map illustrates seven clusters/themes of perceived broad areas that would help people participate in breast screening programmes (Yu et al., 2023a). 7-Cluster Map With Labels (Yu et al., 2023a).
GCM differs from conventional consensus approaches (e.g., Delphi and Nominal group techniques). For example, the Delphi technique is an iterative method that relies on a geographically dispersed expert panel to foster consensus on a given topic through several rounds of anonymous questionnaires and feedback (Chalmers & Armour, 2019). Anonymity, iterative feedback, group response, and consulting experts’ opinions are four key important characteristics of this technique. Participants often feel more comfortable to express their opinions openly without worrying about consequences and peer pressure as the answers are anonymous. A strong group consensus may be reached, but the process is very time-consuming as several rounds of consultation and analysis are required, there is no live group discussions, and there is a risk of not coming to a consensus. Similarly, in a GCM study, individuals complete Sorting and Rating independently or with support from researchers, so that they are free from peer pressure (Kane & Rosas, 2018). However, a GCM study only requires one-round of data structuring, making it quicker to gain group consensus compared to the Delphi technique.
The Nominal group technique is also a structured method for consensus building, involving five basic steps: introduction; brainstorming (silent idea generation); round-robin recording of ideas; discussion and clarification of ideas; voting or ranking (Olsen et al., 2019). The method is time effective due to real-time interaction and can be adopted in a virtual environment, and participants have equal opportunity to contribute (Khurshid et al., 2023; Olsen et al., 2019). However, this technique is often limited to smaller group size and there is a risk of groupthink where participants feel pressured to conform to group opinions or are uncomfortable sharing differing opinions in a group, thus reducing diversity of opinions (Olsen et al., 2019). On contrast, in a GCM study, participants complete the activities independently and anonymously, minimising groupthink risk or peer pressure (Kane & Rosas, 2018). In addition, unlike the Nominal group technique a GCM study can engage a larger number of participants.
Furthermore, unlike the Delphi and the Nominal group technique, in a GCM study, responses from each participant are accounted for in the analysis to produce more robust results, so that the findings reflect both individual and group perspectives on a given topic (Kane & Trochim, 2007; Rosas, 2012). This makes GCM method more inclusive than conventional consensus methods (Kane & Trochim, 2007).
GCM is increasingly popular in health and social care research for exploring topics such as the concept of wellbeing (Babal et al., 2024; Elliott et al., 2022), barriers to accessing dental care during pregnancy (Winckler et al., 2023), family resilience (Wallace et al., 2018), social prescriber role (Roberts et al., 2022), and consensus on occupational therapy interventions for people with palliative care needs (Wæhrens et al., 2023). Cook and Bergeron (2019) argue that GCM can be helpful in engaging marginalised or hard-to-reach populations by removing traditional power imbalances in research. However, there is little discussion about the challenges of applying GCM and how relevant strategies can be used to address them, despite GCM’s growing popularity and the advantages of its use to engage diverse populations. We draw on evidence from four case studies as examples to address this deficit and discuss how GCM can be adapted innovatively to promote its inclusivity.
Four Case Studies
Each case study highlights issues that arose and were addressed in different contexts. Ethical approval for the four studies was obtained from the Faculty of Life Sciences and Education Research Ethics Committee at the University of South Wales (18JY1001HR For case study 1; 200607LR for case study 2; 200402LR for case study 3; 201204HR for case study 4), HRA/Health Care Research Wales (18/HCRW/0029 for case study 1), and the Central Bristol Research and Ethics Committee (21/SW/0028 for case study 4). Written informed consent was gained from all participants in these four case studies.
Case Study 1: Using GCM With Older People, Carers and Service Providers
A GCM study was conducted exploring the concept of compassionate care in health and social care services from the perspectives of older people, carers, and service providers (Curtis et al., 2020). Nineteen older people, 14 carers, and 11 health and social care service providers were recruited through local authority, third sector organisations, community groups, and relevant professional networks. Using GCM to engage older people receiving residential, nursing, or domiciliary care was a considerable challenge especially with people who were very old and frail or who had reduced mobility or other impairments. The following strategies were applied to enhance participation.
Firstly, two options were offered to older participants for completing Brainstorming. These included face-to-face workshops facilitated by the research team and in-depth face-to-face interviews for participants who had difficulty attending a workshop. Of the six interviewees, one was aged 99, one had hearing loss, one had speech impairments, and one died 1 week after the interview. The participant with hearing loss was given additional written information, and the partner of the participant with speech impairments was present at the interview. Such adaption of the data collection method maximised the contribution of people who were very old, had physical impairments, or were at the end of life.
Secondly, offline and online participation was offered to address the needs of different participant groups. For older people, their access to digital devices and digital skills were considered. They were offered offline participation with an interview option for Brainstorming and a face-to-face workshop option for all three activities. For carers, considering they might not possess essential digital skills, the options of both online and offline participation were provided. For service providers, considering the difficulty of taking time off from work for workshop attendance and the flexibility of online participation, they were invited to take part online only. Adapting both online and offline participation made this research more inclusive.
Thirdly, individualised support was provided in face-to-face workshops. For participants who had difficulty in reading, writing or physically sorting statements, the research team provided one-to-one support by reading aloud focus prompts (for Brainstorming), each statement (for Sorting) or each rating question (for Rating) and recorded the participants’ responses. During Sorting, participants were also asked to think of a pertinent category until all statements were sorted into categories/piles that made sense to them. Statements in each category were then read back to participants to confirm their choices.
Case Study 2: Using GCM With a Visually Impaired Participant
Elliott et al. (2022) carried out a GCM study during the Covid-19 pandemic exploring the concept of social wellbeing. Participants were recruited from academia, social prescribing practitioners, healthcare professionals and members of the public. A sample of 93 participants aged 19–90 living in geographically diverse areas were recruited. Data collection took place June-September 2020, coinciding with UK Covid-19 pandemic restrictions on movement and face-to-face social interaction (Carroll et al., 2020). Consequently, the study was conducted solely online. Three 90-year-old participants took part online without needing any support, but online participation created challenges for some participants. For example, one individual registered an interest at the Sorting stage, but could not engage with the GroupWisdomTM software due to visual impairment. In response, the facilitator called the participant to explain the study and gained verbal informed consent. The telephone conversation was recorded. Two separate telephone calls were made to assist the participant to complete Sorting and Rating.
The telephone call for Sorting lasted approximately 45 min. The facilitator explained the activity and process involved and then worked through each of the 125 statements generated from Brainstorming. Each statement was read out. The participant identified several general themes/categories based on perceived similarity. Each statement was then placed in a relevant specific theme. Once all statements were sorted, the facilitator read out the title of each theme and the participant confirmed whether it should be merged, separated or amended. Where there was uncertainty, the statements within a theme were read out for the participant to gain clarity on the content and to confirm that the theme label was correct.
The telephone call for Rating lasted 30 min. The facilitator read each statement aloud in a neutral manner to minimise any influence on participant decisions. The participant rated the statements against three rating scales - importance, access, and enjoyment (Table 1). Regular breaks were offered, so as the opportunity to complete Sorting or Rating in a following-up telephone call. The participant completed Sorting and Rating without a break in one individual telephone call respectively. She regarded her experience of participation very positively and expressed an interest in taking part in future research on social wellbeing.
Case Study 3: Using GCM in a Multi-Lingual Context
In Wales, 29.7% (906,800) of the population speak the Welsh language (Welsh Government, 2023a). The Welsh Language (Wales) Measure 2011 made Welsh an official language in Wales and Welsh ‘must be treated no less favourably than English’ when conducting public business (Welsh Government, 2011). This means that GCM studies involving voluntary organisations/charities in Wales must offer a bilingual option.
In 2020 during the Covid-19 pandemic, a research team were commissioned by the Wales Council for Voluntary Action (funded via Welsh Government European Transition Fund) to undertake a GCM study entitled ‘Future Wellbeing of Wales: Transforming Health and Social Care Services Close to Home’ (Wallace & Llewellyn, 2020). Fifty participants were recruited. The research team ensured participants could take part using their language of choice by: 1. Providing all information on the project website in Welsh and English (Welsh first so it is treated not less favourably than English), 2. Providing the participant information sheet and consent form in both languages, and 3. Conversing through email or by telephone with participants through either Welsh or English.
The study was facilitated by a bilingual researcher. The GCM project settings did not have a full description in English and Welsh. GroupWisdomTM software only accommodates direct translation of six languages (English, Spanish, German, French, French Canadian and Danish), and some settings had limited characters to accommodate both languages. Bilingual instructions were emailed to all participants to overcome this issue. Participants responded to the focus prompt in either Welsh or English during Brainstorming. Only 3/110 statements generated were provided in Welsh. The final statement set was provided in both languages to enable inclusion of all statements in Sorting and Rating regardless of which language the statements were provided.
One demographic question was about the use of language in practice. The majority of participants provided support or services in both Welsh and English (56%), followed by English only (28%) and a combination of other languages (6%). No participants provided support or services through the Welsh language only (Wallace & Llewellyn, 2020). Although many participants did use the Welsh language in their everyday practice, most participants participated in this study using the English language.
Case Study 4: Using GCM in a Multi-Cultural Context
Yu et al. (2022) explored support mechanisms to facilitate cancer screening to address low screening uptake in Newport, Wales. Newport is a multicultural city with the largest ethnic minority population in Wales (14.8%) (Welsh Government, 2023b) and is among the most deprived areas in the country (Welsh Government, 2022).
Three GCM studies addressing breast screening, bowel screening, and cervical screening were carried out simultaneously. Engaging people in research who usually decline cancer screening is crucial but presents an extreme challenge (Yu et al., 2023b). Recruitment took place July-September 2021 when Covid-19 related measures regarding social distancing and mass gathering were in place, which compounded challenges.
Recruitment information was distributed via email and social media (Twitter, Facebook, and WhatsApp) and was displayed via organisations, networks, community groups, local libraries, and primary care practices. One hundred and thirty-one participants were recruited across the three studies. They were from 10 ethnic groups, of which 81 were from minoritised ethnic groups. Thirteen languages were spoken (Arabic, Bengali, English, Farsi, Italian, Kurdish, Patwa Creole, Punjabi, Romanian, Spanish, Somali, Urdu, and Yemeni). In this case study, key issues around language barriers and digital skills were raised.
Language barriers were related to inability to speak English and low literacy/health literacy skills, which was the case for 40 participants. Initial recruits were white and well educated, and therefore, the researchers engaged five female participants from ethnic minority communities in the target area and trained them as lay researchers to reach members in their respective communities. In addition to English, lay researchers spoke Bengali, Punjabi, Hindi, Urdu, Somali, Arabic, or Yemeni. This helped reach people less likely to participate in cancer screening or research, i.e., those who do not speak/read English or read their own languages. A standard version and an easy-read version of participant information sheets and consent forms were prepared (Bennett et al., 2021). Residents in our target area and members of the Learning Disability Advisory Group at the University of South Wales were consulted to ensure all information was culturally sensitive and easy to read/understand (Yu et al., 2023b). Both versions were distributed to interested individuals.
The initial plan was to collect data solely online via GroupWisdomTM due to Covid-19 related restrictions. This was challenging or impossible for some people to take part, particularly older people and people speaking little or no English. Offline participation was adapted accordingly to address digital exclusion, while ensuring the same information was collected. More than half the data were collected offline via participants completing required paperwork. This approach helped the researchers include people who would otherwise be digitally excluded from research despite the increased workload.
Discussion
To the best of our knowledge, this is the first paper that explores how GCM can be used innovatively to engage participants with diverse needs (e.g., people who are very old/frail, have hearing/visual/speech impairment, are bilingual, have language barriers, and have limited digital skills). Four key issues that need to be addressed before and during research are discussed below.
Participatory Considerations
Inclusion is defined as “being included – being embedded and actively involved in what is going on” (Atcheson, 2021, p. 16). Achieving inclusion in the context of research requires a participatory and collaborative approach that emphasises actively engaging people or communities whose lives are affected by the issues being studied (Vaughn & Jacquez, 2020). The nature of GCM is in line with the participatory approach, where participants actively engage with the research process including data analysis and interpretation, and the results incorporate responses from all individual participants (Kane & Trochim, 2007). In traditional research, there is imbalance of power between the researchers and the researched, where the researchers are assigned the role of a knowledgeable expert, while the participants play a passive role (Northway, 2010a). Research information provided by an ‘expert’ is often not accessible to participants, presenting a barrier to participation. For example, standard participant information sheets are lengthy, containing required ethnical and governance information, which may be daunting and inaccessible to many people, such as those with learning disabilities or limited literacy skills (Bennett et al., 2021; Northway, 2010; Yu et al., 2023b). To address this issue and mitigate exclusion, providing pictorial and easy-read information is essential as demonstrated in Case study 4, where participants were provided with an easy-read version (using plain language and photo-symbols) and a standard version of the participant information sheet and consent form. Community members in the target area and members of a Learning Disability Advisory Group were consulted to ensure the content was easy to read/understand and the language and pictures were culturally appropriate (Yu et al., 2023b). Similarly, the provision of pictorial and easy-read information is considered highly important as shown in research with people with learning disabilities (Northway et al., 2024; Oloidi et al., 2022). For example, in a study where a health communication tool was developed to support people with learning disabilities in accessing healthcare, Northway et al. (2024) translated the 40 pieces of information used in an online survey with families, carers and health professionals into an easy-read format for participants with learning disabilities. Appropriate pictures were used to illustrate the information and each piece of information was placed on a card. In addition, the provision of research information via multimedia (e.g., audio, video, and slideshows) to address the communication and accessibility needs of different participant groups has been increasingly highlighted (Ditai et al., 2018; Knapp et al., 2023; NIHR, 2025). In our ongoing research projects with people from under-represented communities, a video version of the participant information sheet is also provided as an alternative in addition to written information (Rossouw et al., 2024; Yu et al., 2024).
Furthermore, traditional methods of data collection may create barriers to inclusion. Recent advances in digital technologies have significantly transformed every aspect of people’s life, such as how information is shared, how people interact with each other, how services are provided, and how research is conducted (Sun et al., 2020). Since the Covid-19 pandemic, online research participation has accelerated dramatically (Keeley & Bernasconi, 2023). Online-based research has many advantages, such as reach to wider population including hidden groups, removing geographic barriers, increased convenience, and saved time/costs (Oliveri et al., 2021). However, if all research materials are computer-based, many marginalised groups (e.g., older/frail people, people with visual impairment, and people with limited English proficiency) are likely to be excluded from research due to multiple layers of barriers to digital skills and access (Mubarak & Suomi, 2022; Yu et al., 2023b). Conducting a GCM study online is a flexible, valuable alternative to a face-to-face workshop-based approach (Kane & Rosas, 2018). Engaging people in a GCM study who are at risk of being excluded requires researchers to be creative and innovatively adapt their approaches so that anyone who is interested may take part. Our case studies demonstrate the value of providing the option of offline participation (e.g., workshops, face-to-face interviews, telephone interviews, and self-completion of hard copies) to include people who lacked access to digital devices, and/or information technology skills, or had visual or hearing impairment (Curtis et al., 2020; Elliott et al., 2022; Yu et al., 2023a, 2023b). Similarly, Northway et al. (2024) applied different modes of data collection for different participant groups when developing a health communication tool for people with learning disabilities, where an online survey was conducted to sought views from families, carers, and health professionals, while focus groups were carried out with participants with learning disabilities. Furthermore, Heath et al. (2018) demonstrated the values of offering a qualitative interview by telephone, email, Skype, and face-to-face to facilitate participation in research exploring parents’ experiences following the burn-injury of their children.
Time and Resources Considerations
It is well acknowledged that actively involving people who are usually marginalised from society and research is very time consuming, as is often the case with GCM studies when researchers need to adapt their approaches to promote inclusion (Northway, 2010; Yu et al., 2023b). Thus, researchers, participants and funders need to be aware of the required time and resources in research of this nature.
First, as shown in our case studies, additional time was required for face-to-face interviews, workshops, and telephone conversations. Study materials were read out to participants or orally translated in situ as people were not necessarily able to write/read the language they spoke. Additional time was also needed to prepare physical copies of required documents, deliver relevant paperwork, and manually entre data. The number of statements for Sorting (e.g., 89 statements in Case study 1; 125 in Case study 2) should also be considered. This can be overwhelming for some participants, especially those needing extra support. Yu et al. (2023b) reported approximately 3 hr spent supporting a participant who spoke little English to complete Sorting and Rating. Researchers need to help participants choose their level of involvement based on their physical and mental capabilities to reduce overburdening participants and lay researchers. Researchers have frequently highlighted that participatory research is time-consuming and labour-intensive as sufficient time and effort is required from all team members for communication, collaboration, trust-building, and data collection (Hitchen & Williamson, 2015; Scheffelaar et al., 2020).
Second, a trusting relationship between the researchers and the people or communities is essential to foster participation and engagement (Ison et al., 2024; Northway, 2010b; Scheffelaar et al., 2020). Building and maintaining trust is an ongoing process requiring considerable time, resources and efforts from several parties (Christopher et al., 2008). Historical and extant social injustices and inequalities to vulnerable populations, such as people with learning disabilities, mental health problems, very older people, ethnic minorities, and the socially deprived, exacerbate their mistrust to the research community (Ison et al., 2024; Moorely et al., 2023). Health and social care researchers are required to show evidence of Patient and Public Involvement and Engagement when securing funding (NIHR, 2024). Some support is available to help researchers involving the public in research (Health Care Research Wales, n.d.). However, the time spent on developing trust is often not costed but relies on the goodwill of the researchers and community members, making it challenging to sustain a trusting relationship (Northway, 2010b). Furthermore, it would be inappropriate to start to develop a trusting relationship with the target groups once a project is funded due to the usual tight timeline and the missed opportunity to engage the public at the onset of research. In recognising the importance of establishing trust and a lasting partnership with communities to promote inclusivity in research, the Ethnic Minority Research Advisory Group was set up in the authors’ organisation (University of South Wales) in 2022 to actively engage ethnic minority communities in research. It is essential that researchers plan early and build in sufficient time and necessary resources required to engage with under-represented populations in all stages of the research process, to avoid tokenism and value lay people’s contributions.
Ethical Considerations
GCM adaptation to include marginalised participants may raise ethical implications on power dynamics, informed consent, and the potential for bias in data collection.
As discussed earlier, there is power imbalance between the researchers and the researched in conventional research where participants have little control over the research process and outcomes. Involving and engaging patients and the public throughout the whole research process can have a positive effect on the power dynamics (INVOLVE, 2012; NIHR, 2024). However, evidence still shows that the involvement of marginalised groups (e.g., ethnic minority groups) is most occurred in research design, but least in data analysis/interpretation (Dawson et al., 2018). A trusting relationship, an enduring, equal partnership, and feeling of being heard, valued and respected are key to help gain trust, balance the power relationship, and promote meaningful participation. As in our case studies, the researchers spent time with participants to establish rapport, listened to and respected their views, and provided required support accordingly. Recently, the lead author of Case study 4 has secured a small fund for a community capacity building programme to train members from marginalised communities (asylum seekers and refugees, people with learning disabilities, ethnic minorities, and substance users) to become research ambassadors and lay researchers (Yu et al., 2024). It is hoped that this newly funded project will increase research engagement in the future by empowering under-represented communities, addressing power imbalance, sustaining trust, and making marginalised communities become research ‘ready’.
The issue of consent should be recognised and addressed. In conventional research, consent is often provided in a written format, where participants sign a paper copy of the consent form. When research is conducted online, consent is usually provided in a digital format, where participants sign a consent form on a virtual platform or return the signed consent form via email. In our case studies, written, digital, and verbal consent were received. It is essential that appropriate options were given to remove barriers to inclusion at the consent stage. For example, in Case study 4, some people who were interested to take part were unable to open or fill in the consent form which was initially provided as a Word document. In this case, a hard copy of the form was given if possible or information on the consent form was provided as email content rather than as an email attachment. In Case study 2, verbal consent was sought via a telephone call from a participant with visual impairment, which was audio recorded. In addition, to facilitate informed consent, sufficient information should be provided in a format that is accessible to potential participants. Case study 4 has shown the value of offering an easy-read version of the participant information sheet and consent form. As stated earlier, a standard version was also provided with detailed ethical and governance information as required. This strategy has been frequently applied when conducting research with people with learning disabilities (Caton et al., 2024; Hatton et al., 2021). However, it is essential that potential participants can always contact the research team during the consent stage and throughout a study. In Case study 4, five participants from ethnic minority communities were recruited and trained to gain consent and collect data from the participants they recruited in their respective communities. The value of involving community members as lay researchers in health and social research has been increasingly highlighted (Jones et al., 2021; Mockford et al., 2016; Nöstlinger & Loos, 2016), As this approach may have ethical implications on consent, appropriate training on recruitment and gaining consent should be always provided to ensure that lay researchers understand the key principles of informed consent. Furthermore, timely support from the research team for lay researchers should always be available.
The potential for bias in data collection is another issue when researchers adapt GCM to include marginalised populations. When participating in a GCM study online, participants have limited contact with researchers and complete the required activities independently without being influenced by other participants or the researchers. However, as in other research where data collection is undertaken via interviews, workshops, or telephone conversations, researchers may be intensely involved in data collection. Thus, researchers need to be aware that this may result in biased responses, highlighting the importance of transparency and reflexivity. It is hoped that the rapport developed with participants and our adoption of a neutral stance may have minimised researchers’ influence on participants. Researchers should critically self-reflect about their own preconceptions, relationship dynamics, and analytic focus during the processes of collecting, analysing, and presenting data (Polit & Beck, 2017).
Intersectionality Considerations
The impact of intersectionality on health and research involvement and participation has increasingly been highlighted in recent years (Merz et al., 2023; Mooreley et al., 2023). Intersectionality is viewed as the ‘overlapping and connected nature of personal characterises’, and compounded inequalities experienced by individuals due to multiple protected characteristics (e.g., age, gender, ethnicity, race, and socio-economic backgrounds) (Atcheson, 2021; Scottish Government, 2022). The intersection between these characteristics contribute to social and health inequalities and injustices, affecting every aspect of people’s daily life (Hassiotis, 2020). Our case studies have shown the intersection effect of age, ethnicity, language, and physical impairments on participation. For example, in our case studies, a participant could be an older female, identify as black, belong to a lower socio-economic group, and have hearing or visual impairment. Researchers need to take intersectional approaches by viewing individuals as a unique whole and recognise that different characteristics contribute to them as individuals (Moorley et al., 2023). Such approaches focus on power dynamics and structural causes that determine such dynamics, which helps understand the reasons for people to or not to engage with research (Merz et al., 2023). Thus, appropriate strategies can be developed accordingly to involve people belonging to intersectionally marginalised communities in research. For example, in Case study 1, offline participation in the form of interviews or workshops was offered to participants who were very old, frail, and had hearing/visual impairment. In Case study 2, telephone calls were offered to collect data from a female participant in her 90s and had visual impairment. In Case study 4, offline participation was offered to participants who were old, had limited digital skills, and had language barriers. In addition, five participants were trained as lay researchers who recruited and collected data from people who identified as ethnic minorities, belonged to a socially deprived group, spoke no/little English, and had low literacy skills. On the other hand, researchers also need to be aware of any potential unconscious bias about the interplay of these protected characteristics. For example, some 90-year-old participants in Case study 2 took part online without needing any support (Elliott et al., 2022). Researchers need to consider diversity within a group and between groups to avoid stereotyping (Moorley et al., 2023). Adopting a person-centred approach where all participants are respected, and their needs are individually assessed and addressed accordingly may alleviate participation barriers.
Implications
Our exploration on how GCM can be adapted to engage marginalised people in research has the potential to influence inclusive research practices. The underlying challenges (e.g., lack of trust, reduced mental capacities and language barriers) of engaging under-represented groups in research are common across disciplines and countries. A better understanding of complexities of various issues that researchers and marginalised people may face is crucial to make research more inclusive.
Based on four case studies, our exploration of research involvement and engagement has highlighted the importance of four key areas that should be addressed in future research: participatory, time and resources, ethical, and intersectionality considerations. First, researchers should make research information accessible to participants and adapt data collection modes that suit participants. Second, researchers and funding bodies need to acknowledge the time and resources that are required to build a trusting relationship with marginalised people and engage them in research. It is essential that appropriate funding and support is in place for trust building and compensating for participants’ involvement and contributions. Third, issues of power dynamics, informed consent and response bias should be considered and addressed. A trusting relationship and a long-term partnership between the research community and marginalised communities may help mitigate these issues, highlighting the importance of ongoing engagement to avoid tokenism in research participation. Lastly, a person-centred participatory approach should be adopted when engaging marginalised people in research, considering the complex intersection between multiple protected personal characteristics.
Conclusion
This paper has originality by building upon the existing work of participatory research and is the first account of a methodological debate about how individuals from marginalised populations characterised by age, disability, language barriers, and digital skills may be supported to take part in GCM studies. The paper is significant by having the potential to help researchers in multiple disciplines adapt GCM and other participatory research methods to promote research inclusivity, so that people who are previously under-represented from society and research can be heard and make significant contributions to knowledge. Active involvement and engagement with marginalised communities in research is challenging but can also be very rewarding. It is hoped that the discussion presented in this paper will help researchers within and outside health and social care settings in the UK and overseas to take an inclusive research agenda forward.
Footnotes
Acknowledgements
We thank all participants who took part in all four case studies presented in this article and people who helped us during the fieldwork.
Statements and Declarations
Author Contributions
Juping Yu: Conceptulisation, Writing - original draft, review and editing; Megan Elliott: Conceptulisation, Writing - original draft, review and editing; Molly Curtis: Writing - draft of case study 1, review and editing; David Pontin: Conceptulisation, Writing - review and editing; Sarah Wallace: Writing - review and editing; Carolyn Wallace: Writing - draft of case study 3, review and editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Case study 1: Funded by KESS II in Partnership With Torfaen County Borough Council; Grant number: 21087. Case study 2: Funded by the Welsh School of Social Prescribing Research; Grant number: 21793. Case study 3: Funded by the Wales Council for Voluntary Action; Grant number: WCVA Request for Quote - Issued 9 January 2020. Case study 4: Funded by Aneurin Bevan University Health Board; Grant number: ABU-STA-124307.
Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.